
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Over the last several years, the morbidity, mortality, and high costs associated with lung volume reduction (LVR) surgery has fuelled the development of different methods for bronchoscopic LVR (BLVR) in patients with emphysema. In this meta-analysis, we sought to study and compare the efficacy of most of these methods.
Methods
Eligible studies were retrieved from PubMed and Embase for the following BLVR methods: one-way valves, sealants (BioLVR), LVR coils, airway bypass stents, and bronchial thermal vapor ablation. Primary study outcomes included the mean change post-intervention in the lung function tests, the 6-minute walk distance, and the St George’s Respiratory Questionnaire. Secondary outcomes included treatment-related complications.
Results
Except for the airway bypass stents, all other methods of BLVR showed efficacy in primary outcomes. However, in comparison, the BioLVR method showed the most significant findings and was the least associated with major treatment-related complications. For the BioLVR method, the mean change in forced expiratory volume (in first second) was 0.18 L (95% confidence interval [CI]: 0.09 to 0.26; P<0.001); in 6-minute walk distance was 23.98 m (95% CI: 12.08 to 35.88; P<0.01); and in St George’s Respiratory Questionnaire was -8.88 points (95% CI: −12.12 to −5.64; P<0.001).
Conclusion
The preliminary findings of our meta-analysis signify the importance of most methods of BLVR. The magnitude of the effect on selected primary outcomes shows noninfe-riority, if not equivalence, when compared to what is known for surgical LVR.
Introduction
Chronic obstructive pulmonary disease (COPD) is now the third leading cause of death in the United States.Citation1 In 2007, the economic burden of COPD in the US was $42.6 billion in health care costs and lost productivity.Citation2 Although different pharmacological treatments have shown improvement in lung functions in general COPD patients, the predominantly emphysema phenotypes with poor lung functions are often considered for additional surgical procedures. These include the bullectomy,Citation3 single and double lung transplantation,Citation4 and, more recently, lung volume reduction (LVR) surgery (LVRS).Citation5 The latter is based on the concept that targeted resection of the damaged tissue that causes hyperinflation allows more space for the residual lung, which results in improvement of chest wall mechanics and transpulmonary recoil pressures. This and other factors appear to contribute to the physiological and symptomatic improvements that follow LVRS. The National Emphysema Treatment Trial (NETT) showed that the patients who benefited the most from LVRS in terms of survival and functional improvement were those who had predominantly upper lobe emphysema and poor exercise capacity.Citation5,Citation6 However, significant short-term morbidity and mortality have been associated with LVRS.Citation7 Furthermore, the associated costs of LVRS are almost prohibitive and make this a less attractive option for LVR.Citation8
Different methods of bronchoscopic LVR (BLVR) have been studied, and more alternatives to LVRS are being studied in clinical trials. Most of the evidence in literature exists for one-way valves, sealants/hydrogels (from here on, collectively referred to as BioLVR), coil implants (LVR coils [LVRCs]), airway bypass stents, and bronchial thermal vapor ablation (BTVA) therapy. The valves work by preventing inspired air from entering target airways and allow exit of trapped air from distal airways. BioLVR therapy involves administration of a fibrinogen suspension and thrombin solution into the airways separately. Once in contact, these products polymerize into a hydrogel in situ. A localized inflammatory reaction ensues, causing atelectasis and remodeling, as well as a volume reduction over a 4- to 6-week period. BTVA uses heated water to produce thermal injury of the target tissue, which is followed by permanent fibrosis and atelectasis. Airway bypass stents have been used to create and maintain passages between the bronchi and emphysematous lobes. In the LVRC method, a coil is deployed into the target tissue. Once deployed, a coil conforms to its predetermined shape, by bending in the airway and causing compression of adjacent lung tissue, thereby creating local LVR. Since the advent of these new BLVR techniques, there has been no head-to-head comparison of one versus another. In this meta-analysis, we sought to analyze the comparative efficacy of each BLVR technique.
Methods
Search strategy and selection criteria
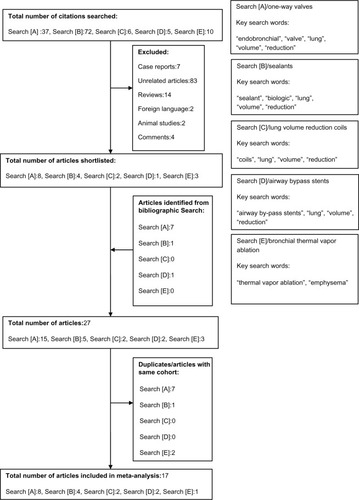
We searched PubMed and Embase databases from their inception to June 6, 2013. We used combinations of the following keywords: “endobronchial valves”, “one way valves”, “lung sealants”, “coils”, “lung volume reduction surgery”, “bronchial thermal vapor ablation”, and “emphysema”. Boolean operators (AND/OR) were used to pair key search words. The search from PubMed yielded all the studies included in this meta-analysis. To ensure a thorough search of the literature, we handsearched the reference lists of the included studies and previously published meta-analyses. For inclusion in our meta-analysis, we considered only those studies that reported the pre- and post-LVR data on lung functions (in specific, the forced expiratory volume in 1 second [FEV1], forced vital capacity [FVC], total lung capacity [TLC], residual volume [RV], and diffusion lung capacity of carbon monoxide [DLCO]), the 6-minute walk distance (6 MWD), and the St George’s Respiratory Questionnaire (SGRQ). Prospective nonrandomized and randomized controlled trials (RCTs) were included, provided pre- and post-intervention data (absolute numbers) or mean difference (between pre- and post-intervention) were available. We included prospective nonrandomized consecutive case series but excluded case reports. Prospectively conducted multicenter cohort studies with retrospective analyses were also considered eligible for inclusion. However, retrospective cohort studies, as well as studies that reported data in median and interquartile range, were excluded. One investigator (IHI) independently searched the studies and performed the final screening. There were no disagreements between investigators on the inclusion or exclusion of a study. summarizes the results of the selection process. As a general rule, for multiple publications of the same trials, we intended to include only the most recent one. A total of seven studiesCitation9–Citation15 from the subgroup of one-way valves, one from BioLVR,Citation16 and two from BTVACitation17,Citation18 were affected by this rule (see “Supplementary material” for details).
Figure 1 Flow diagram of articles identified and evaluated during the study selection process.
Study outcomes
Our primary outcomes included assessments of lung function (FEV1 and FVC) measured in liters, lung volumes (TLC and RV) measured in liters, diffusion capacity (DLCO) measured in mL/min/mmHg, assessment of exercise capacity (6 MWD) measured in meters, and assessment of the health-related quality of life with the SGRQ.
Analyses of secondary outcomes were related to the safety of a particular device or procedure. As the complications associated with each procedure were distinct from each other, we were not able to pool the data for a common outcome across different subgroups. For one-way valves, we included the incidence rates of pneumonia distal to valve, pneumothorax lasting more than 7 days, and migration of valves. For the BioLVR, we included the incidence rate of pneumonia and COPD exacerbations. For the LVRCs, we only included the incidence rate of COPD exacerbations. Data from the studies on airway bypass stents and BTVA were not sufficient enough to analyze.
Data abstraction
Data were extracted on a prespecified worksheet. This included first author’s name, year of publication, number of study participants, their age and sex distribution, presence of comorbidities besides COPD, type of BLVR, country of origin, and study design. For the analysis, we recorded the mean of pre- and post-BLVR FEV1, DLCO, 6 MWD, and SGRQ with standard deviations (SDs), and, where necessary, the mean difference with SD or 95% confidence intervals (CIs). For any included study, where such information was not complete for a particular outcome of interest, this information was not included. In any included study, if outcomes were assessed at different time points, we obtained the data available for the longest follow-up. Where DLCO was available in mmol/min/kPa units, we used the conversion factor of 0.335 to obtain data in mL/min/mmHg.Citation19 6 MWD reported in feet was converted into meters using the following formula:
Standard errors (SES) were converted into SDs using the following formula:
For RCTs, comparing a BLVR with either control or an active comparator, we extracted data only for the cohort that received BLVR (see “Supplementary material” for details).
Quantitative data synthesis
The mean changes in the outcomes from BLVR along with their 95% CIs were estimated by pooling the available data using Comprehensive Meta-Analysis software (v 2.2.064, Biostat, Englewood, NJ, USA). We separately analyzed the pooled changes in primary and secondary outcomes for each type of BLVR. Forest plots were constructed to analyze the results. Fixed effects methods were used to account for variance within the studies. Random effects methods were used to account for variance between and within the studies.Citation20 Statistical heterogeneity was assessed with the I2 statistic.Citation21 An I2>60% indicated significant heterogeneity. Where moderate-to-high heterogeneity was noticed, we reported the results in random effects model. For our analysis of safety data, we used total number of events and person years to calculate the incidence rate for a particular safety outcome. Person years were calculated by multiplying the number of study participants at risk with the mean duration of follow-up (in years). If the number of cases was zero, a correction factor of 0.5 was added to both the events and person years.Citation22 Data were pooled, and the results are displayed in the form of forest plots. To check for publication bias, we constructed funnel plots of effect size and standard errorCitation20,Citation23 and also analyzed results by using the Begg and Mazumdar rank correlation test.Citation24
Results
Study characteristics
A total of 17 studiesCitation19,Citation25–Citation40 qualified for inclusion in the meta-analysis. The total number of study participants was 998. There were eight studies for one-way valves,Citation26,Citation29,Citation30,Citation33–Citation35,Citation38,Citation39 four for BioLVR,Citation19,Citation27,Citation31,Citation32 two for LVRC,Citation28,Citation37 two for airway bypass stents,Citation25,Citation36 and one for BTVA.Citation40 outlines the baseline characteristics of the study population. On average, study participants were >58 years old. The duration of follow-up lasted between 1 and 12 months. There were a total of four RCTs.
Table 1 Baseline characteristics of studies
Effect on primary outcomes
For the studies using the BioLVR method, the pooled mean change in FEV1 was 0.18 L (95% CI: 0.09 to 0.26; P<0.001 (), in 6 MWD was 23.98 m (95% CI: 12.08 to 35.88; P<0.01) (), and in SGRQ was −8.88 points (95% CI: −12.12 to −5.64; P<0.001) ().
Figure 2 Change in FEV1.
Notes: The diamond reflects the 95% CIs of the pooled estimate of mean difference. “BioLVR” indicates studies using sealants/hydrogels. “BTVA” indicates studies that used BTVA. “Stents” indicates studies using airway bypass stents. “Valves” indicates the subgroup of studies that used one-way valves. “GOLD” indicates stage of severity of chronic obstructive pulmonary disease.
Abbreviations: BTVA, bronchial thermal vapor ablation; CI, confidence interval; CV−, collateral ventilation absent; CV+, collateral ventilation present; FEV1, forced expiratory volume in the first second in liters; GOLD, Global initiative for chronic Obstructive Lung Disease; LVR, lung volume reduction.
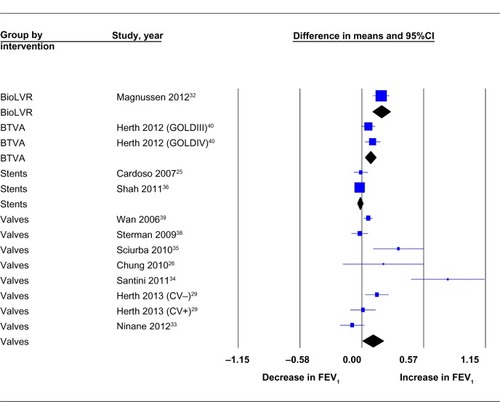
Figure 3 Change in 6 MWD.
Notes: The diamond reflects the 95% CIs of the pooled estimate of mean difference. “BioLVR” indicates studies using sealants/hydrogels. “BTVA” indicates studies that used BTVA. “LVRC” indicates studies using LVRCs. “Stents” indicates studies using airway bypass stents. “Valves” indicates the subgroup of studies that used one-way valves. “GOLD” indicates stage of severity of chronic obstructive pulmonary disease. The 6 MWD test was measured in meters.
Abbreviations: 6 MWD, 6-minute walk distance; BTVA, bronchial thermal vapor ablation; CI, confidence interval; CV−, collateral ventilation absent; CV+, collateral ventilation present; GOLD, Global initiative for chronic Obstructive Lung Disease; LVRCs, lung volume reduction coils.
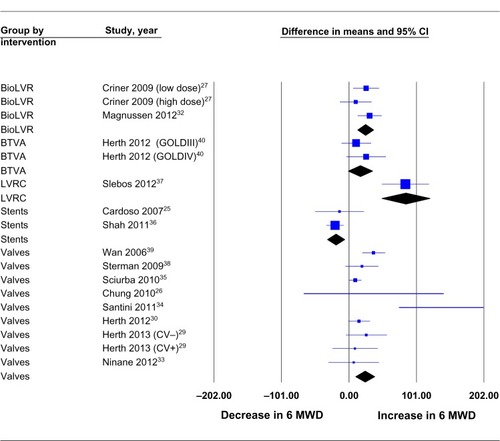
Figure 4 Change in SGRQ.
Abbreviations: BTVA, bronchial thermal vapor ablation; CI, confidence interval; CV−, collateral ventilation absent; CV+, collateral ventilation present; GOLD, Global initiative for chronic Obstructive Lung Disease; LVRCs, lung volume reduction coils; SGRQ, St George’s Respiratory Questionnaire.
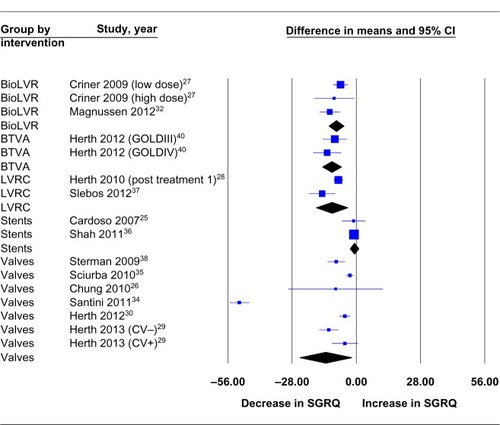
The studies that used one-way valves showed a pooled mean change in FEV1 of 0.10 L (95% CI: 0.00 to 0.19; P=0.04) (), in 6 MWD of 23.27 m (9.06 to 37.48; P=0.001) (), and in SGRQ of −13.53 points (−24.38 to −2.23; P=0.01) ().
Studies on BTVA showed a pooled mean change in FEV1 of 0.07 L (95% CI: 0.02 to 0.12; P<0.01) (), in 6 MWD of 16.24 m (95% CI: −1.92 to 34.41; P=0.08) (), and in SGRQ of −10.82 points (95% CI: −14.95 to −6.70; P<0.001) ().
Only 6 MWD and SGRQ data were analyzed for LVRC studies, which showed a pooled mean change of 84.4 m (95% CI: 48.43 to 120.36; P<0.001) () and −10.79 points (95% CI: −17.66 to −3.92; P<0.01) (), respectively.
and Figures S1–S4 summarize the results of all other primary outcomes, including FVC, TLC, RV, and DLCO.
Table 2 Effect on primary outcomes
Effect on secondary outcomes
The effects on secondary outcomes, defined a priori, are shown in Supplementary material. One-way valves were associated with an increased incidence of pneumonia distal to the valves (incidence rate of 0.05; P<0.001), pneumothorax >7 days (incidence rate of 0.06; P<0.001), and with valve migration (incidence rate of 0.01; P=0.03). Results are shown in the form of forest plots in Figures S5–S7. BioLVR and LVRCs had a unique association with treatment-related COPD exacerbations with an incidence rate of 0.07 (P=0.04) and 1.30 (P=0.01), respectively (Figures S8 and S9). BioLVR was also associated with an increase in treatment-related pneumonias (Figure S10).
Assessment of publication bias
The Begg and Mazumdar rank correlation testsCitation24 did not show evidence of publication bias for the data on primary outcomes (see Tables S1 and S2).
Post hoc analyses
We separately analyzed studies from the subgroups of one-way valves, BioLVR, and LVRCs that studied participants for a minimum of 6 months. Results are reported in and discussed below.
Table 3 Post hoc analysis of studies with duration 6–12 months
Discussion
To the best of our knowledge, this is the first meta-analysis that has systematically analyzed the effects of different forms of BLVR. Although our meta-analysis was designed to compare different methods used for BLVR, most of the studies included in our meta-analysis studied one-way valves. Consequently, this subgroup had the largest number of study participants compared to the other methods (BioLVR, LVRCs, airway bypass stents, and BTVA). Overall, the findings of our meta-analysis favor BioLVR as the most efficacious method of BLVR. This is because not only did this subgroup show a statistically significant difference in the assessment of lung functions (FEV1, FVC, TLC, RV, and DLCO), but also showed the most increase in exercise capacity (as assessed by the 6 MWD). Airway bypass stents seemed to lag behind in almost all of the primary outcomes. It also seemed paradoxical that this subgroup, in fact, showed a decrease in the FEV1. Direct comparison of the different BLVR methods for our secondary outcomes was not possible, since each method had a unique and different side effect profile. However, there did seem to be more procedure-/device-related complications associated with the one-way valves than with the LVRCs or BioLVR.
Data from the NETT research groupCitation5 indicate that, at 6 months post-LVRS, the change in FEV1 was 8.1%±9.3% predicted at 6 months and 6.0%±8.9% predicted at 12 months. This corresponds to an improvement of approximately 30% from baseline at 6 months and 22% from baseline at 12 months. The dominant finding of the NETT was an increase in the exercise capacity (defined as an increase in the maximal workload by more than 10 watts from baseline) and health-related quality of life, as measured by SGRQ, in those with predominantly upper lobe emphysema, in the surgical group versus the group that received medical therapy.Citation5 The pre- to post-surgery data from the same study indicated that the change in 6 MWD at 6 months and 12 months was 47.3±232.7 m and 14.4±275.1 m, respectively.Citation5 This corresponds to an improvement of 3.88% and 1.18%, respectively, compared to baseline. This study also showed that 68% of the 508 study participants randomized to surgery achieved an overall reduction in SGRQ scores. Most of the studies included in our meta-analysis had a shorter duration of follow-up and a much lower number of study participants compared to the NETT. However, results of our post hoc analysis correspond to an improvement in FEV1 of 43% and 31.2% in the subgroups of one-way valves and BioLVR, respectively. Similarly, for 6 MWD, results of our post hoc analysis correspond to an approximate 13.14% improvement in the subgroup of one-way valves and 5.34% in the subgroup of BioLVR. Thus, a comparison of our findings, in particular for FEV1, 6 MWD, and SGRQ, with the data from NETT, at the same duration of follow-up (6–12 months), suggests noninferiority, if not equivalence, for BLVR. Indeed, the long-term follow-up data of 5 years from the NETT showed an overall survival advantage in the LVRS group compared to medical treatment.Citation6 This data also showed significant improvements in exercise capacity and health-related quality of life (as measured by SGRQ) at 3 and 4 years post-surgery, respectively. While similar long-term data do not exist for most methods of BLVR, more recent data report that the 5-year survival rates in patients treated with one-way valves exceeded 80%.Citation12 However, in terms of the overall safety profile, if LVRS is associated with approximately 5.5% (5.5% in NETT and between 5% and 20% in others) 90-day mortality, then, in comparison, current published literature shows that one-way valve therapy is associated with 1%, airway bypass stents with 3%, and BioLVR with 0% 90-day mortality.Citation15,Citation25,Citation27,Citation41
The mechanism of LVR differs between one-way valves, BioLVR, LVRCs, airway bypass stents, and BTVA. From a historical perspective, the methods have evolved. The first in line were the proximal obstructing devices.Citation42,Citation43 However, because of their failure in producing effective LVR and the high incidence of procedural pneumothoraces, these devices soon fell out of favor. It was thought that flow from the extensive collateral ventilation (CV) pathways between and within the emphysematous lobes paradoxically led to hyperinflation distal to the occlusion. The one-way valves, because of their design, are less likely to be associated with the problem of “paradoxical hyperinflation”. However, as was the case with one-way obstructing devices, certain factors such as CV and fissure integrity have a bearing on the long-term success of procedures with one-way valves.Citation30,Citation35 In the post hoc analyses of both the US and European Endobronchial Valve for Emphysema Palliation Trial (VENT) studies, factors such as fissure integrity on computed tomography lung scans and lobar occlusion were associated with significant LVR, and patients who exhibited these signs on computed tomography had significantly improved clinical outcomes.Citation30 Most importantly, these results were sustained at 12 months post-procedure. Recently, Herth et al validated the use of a method to assess CV for predicting efficacy of one-way valves.Citation29 Their results showed an accuracy of 75%. It is likely that current ongoing research trials with one-way valves using this approach would show better outcomes compared to the earlier studies. In contrast to the one-way valves, the effect of BioLVR for LVR is not dependent on interlobar fissure integrity.Citation32 The effects seem dose dependent, with the best effect produced by high-dose (20 mL/sub-segment) versus low-dose (10 mL/sub-segment) sealant.Citation27 Aside from some short-term complications, including treatment-related pneumonia (Figure S10) and COPD exacerbations (Figure S8), overall, as noted above, this method has been found to be very safe with no procedural mortality reported in studies.Citation19,Citation27,Citation31 This is in contrast with the frequent procedure-related complications observed with one-way valves, such as pneumonia distal to valve implantation, valve- or procedure-related pneumothorax, and valve migration, as shown in Figures S5–S7.
Our meta-analysis has several strengths. It incorporated a total of 998 study participants from 17 different studies. We separately analyzed studies that followed participants for a minimum of 6 months to a maximum of 12 months. Study participants belonged to different countries and continents. This allows for some degree of generalizability of our findings. No evidence of publication bias was observed by statistical tests in our primary outcomes.
Our meta-analysis has several limitations. First, moderate-to-high heterogeneity was observed in most of the analyses. This could be because of the differences in the baseline characteristics of the study participants, procedural techniques, assessment of outcomes, and the geographic locations in which the studies were conducted. However, in order to account for the between-study variance, we used random effects model to report our results. Second, excluding the subgroup of one-way valves, most of the other subgroups did not have a sufficient number of studies, hence assessment of publication bias in these subgroups was not possible. Nevertheless, we believe that our search for studies was thorough and extensive. Third, most of the studies included in our meta-analysis were single-arm prospective trials and not RCTs and a few were pilot studies, which, as standalone studies, cannot be considered powered enough to draw strong conclusions from.
Despite these limitations, we believe our findings are significant, as this meta-analysis provides some form of comparability between the different methods of BLVR. We believe that future studies can benefit from the estimates of effect sizes provided in our meta-analysis.
Conclusion
These preliminary findings show that, excluding airway bypass stents, most of the methods of BLVR show efficacy in improving lung functions and exercise capacity. Moreover, these methods could likely be noninferior, if not equivalent, to LVRS. However, it is likely that, in clinical practice, the efficacy observed for most BLVR methods would be tempered with considerations of the technical peculiarities of each procedure (such as the absence or presence of CV in the case of one-way valves) and their associated complications. LVRS may still be considered first-line for patients with predominantly upper lobe emphysema and poor exercise capacity, and only a select number of patients could be considered for BLVR. This is because, firstly, there is no trial that directly compares LVRS and BLVR and, secondly, none of the bronchoscopic methods are approved by the US Food and Drug Administration. Given the preliminary nature of our findings, we believe that more trials are needed that are designed with a comparative effectiveness research model, involve a larger number of participants, with a much longer duration of follow-up, and with different markers of improvement than the ones traditionally used in earlier studies.
Disclosure
IHI and FRM report no potential conflicts of interest with any companies/organizations whose products or services may be discussed in this article. AIM was/is an investigator on the Spiration pivotal study (co-principal investigator), Aeris trial (principal investigator), EASE trial (principal investigator), and PneumRx trial (principal investigator). None of the authors report any funding source for this work.
References
- Copd (chronic obstructive pulmonary disease) [webpage on the Internet]National Heart, Lung, and Blood Institute2012 Available from: https://www.nhlbi.nih.gov/about/factbook/chapter4.htmAccessed September 24, 2013
- 2007 nhlbi morbidity and mortality chart book. [webpage on the Internet] Available from: http://www.nhlbi.nih.gov/resources/docs/07-chtbk.pdfAccessed September 24, 2013
- De GiacomoTRendinaEAVenutaFBullectomy is comparable to lung volume reduction in patients with end-stage emphysemaEur J Cardiothorac Surg20022235736212204723
- CassiviSDMeyersBFBattafaranoRJThirteen-year experience in lung transplantation for emphysemaAnn Thorac Surg20027416631669 discussion 1669–167012440627
- FishmanAMartinezFNaunheimKNational Emphysema Treatment Trial Research GroupA randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysemaN Engl J Med20033482059207312759479
- NaunheimKSWoodDEMohsenifarZNational Emphysema Treatment Trial Research GroupLong-term follow-up of patients receiving lung-volume-reduction surgery versus medical therapy for severe emphysema by the national emphysema treatment trial research groupAnn Thorac Surg20068243144316888872
- NaunheimKSWoodDEKrasnaMJNational Emphysema Treatment Trial Research GroupPredictors of operative mortality and cardiopulmonary morbidity in the national emphysema treatment trialJ Thorac Cardiovasc Surg2006131435316399293
- RamseySDBerryKEtzioniRKaplanRMSullivanSDWoodDENational Emphysema Treatment Trial Research GroupCost effectiveness of lung-volume-reduction surgery for patients with severe emphysemaN Engl J Med20033482092210212759480
- HopkinsonNSTomaTPHansellDMEffect of bronchoscopic lung volume reduction on dynamic hyperinflation and exercise in emphysemaAm J Respir Crit Care Med200517145346015579725
- SnellGIHolsworthLBorrillZLThe potential for bronchoscopic lung volume reduction using bronchial prostheses: a pilot studyChest20031241073108012970040
- TomaTPHopkinsonNSHillierJBronchoscopic volume reduction with valve implants in patients with severe emphysemaLancet200336193193312648974
- VenutaFAnileMDisoDLong-term follow-up after bronchoscopic lung volume reduction in patients with emphysemaEur Respir J2012391084108922005916
- VenutaFde GiacomoTRendinaEABronchoscopic lung-volume reduction with one-way valves in patients with heterogenous emphysemaAnn Thorac Surg200579411416 discussion 416–41715680805
- WoodDEMcKennaRJJrYusenRDA multicenter trial of an intrabronchial valve for treatment of severe emphysemaJ Thorac Cardiovasc Surg2007133657317198782
- YimAPHwongTMLeeTWEarly results of endoscopic lung volume reduction for emphysemaJ Thorac Cardiovasc Surg20041271564157315173708
- RefaelyYDransfieldMKramerMRBiologic lung volume reduction therapy for advanced homogeneous emphysemaEur Respir J201036202719926742
- GompelmannDHeusselCPEberhardtREfficacy of bronchoscopic thermal vapor ablation and lobar fissure completeness in patients with heterogeneous emphysemaRespiration20128340040622377613
- SnellGIHopkinsPWestallGHolsworthLCarleAWilliamsTJA feasibility and safety study of bronchoscopic thermal vapor ablation: a novel emphysema therapyAnn Thorac Surg2009881993199819932274
- HerthFJGompelmannDStanzelFTreatment of advanced emphysema with emphysematous lung sealant (AeriSeal®)Respiration201182364521228545
- SuttonAJAbramsKRJonesDRSheldonTASongFMethods for Meta-analysis in Medical Research: Wiley Series in Probability and StatisticsNew York, NYJohn Wiley and Sons Inc2000
- Huedo-MedinaTBSánchez-MecaJMarín-MartínezFBotellaJAssessing heterogeneity in meta-analysis: Q statistic or I2 index?Psychol Methods20061119320616784338
- SankeyS WLFineMKapoorWAn assessment of the use of the continuity correction for sparse data in meta-analysisCommun Stat – Simul C19962510311056
- SterneJAEggerMSmithGDSystematic reviews in health care: investigating and dealing with publication and other biases in meta-analysisBMJ200132310110511451790
- BeggCBMazumdarMOperating characteristics of a rank correlation test for publication biasBiometrics199450108811017786990
- CardosoPFSnellGIHopkinsPClinical application of airway bypass with paclitaxel-eluting stents: early resultsJ Thorac Cardiovasc Surg200713497498117903516
- ChungSCPetersMJChenSEmmettLIngAJEffect of unilateral endobronchial valve insertion on pulmonary ventilation and perfusion: a pilot studyRespirology2010151079108320636308
- CrinerGJPinto-PlataVStrangeCBiologic lung volume reduction in advanced upper lobe emphysema: phase 2 resultsAm J Respir Crit Care Med200917979179819179484
- HerthFJEberhardRGompelmannDSlebosDJErnstABronchoscopic lung volume reduction with a dedicated coil: a clinical pilot studyTher Adv Respir Dis2010422523120538661
- HerthFJEberhardtRGompelmannDRadiological and clinical outcomes of using Chartis™ to plan endobronchial valve treatmentEur Respir J20134130230822556025
- HerthFJNoppenMValipourAInternational VENT Study GroupEfficacy predictors of lung volume reduction with Zephyr valves in a European cohortEur Respir J2012391334134222282552
- KramerMRRefaelyYMaimonNRosengartenDFruchterOBilateral endoscopic sealant lung volume reduction therapy for advanced emphysemaChest20121421111111722722233
- MagnussenHKramerMRKirstenAMEffect of fissure integrity on lung volume reduction using a polymer sealant in advanced emphysemaThorax20126730230822374920
- NinaneVGeltnerCBezziMMulticentre European study for the treatment of advanced emphysema with bronchial valvesEur Respir J2012391319132522654006
- SantiniMFiorelliAVicidominiGDi CrescenzoVGMessinaGLaperutaPEndobronchial treatment of giant emphysematous bullae with one-way valves: a new approach for surgically unfit patientsEur J Cardiothorac Surg2011401425143121764325
- SciurbaFCErnstAHerthFJVENT Study GroupA randomized study of endobronchial valves for advanced emphysemaN Engl J Med20103631233124420860505
- ShahPLSlebosDJCardosoPFEASE trial study groupBronchoscopic lung-volume reduction with Exhale airway stents for emphysema (EASE trial): randomised, sham-controlled, multicentre trialLancet2011378997100521907863
- SlebosDJKloosterKErnstAHerthFJKerstjensHABronchoscopic lung volume reduction coil treatment of patients with severe heterogeneous emphysemaChest201214257458222116796
- StermanDHMehtaACWoodDEIBV Valve US Pilot Trial Research TeamA multicenter pilot study of a bronchial valve for the treatment of severe emphysemaRespiration20107922223319923790
- WanIYTomaTPGeddesDMBronchoscopic lung volume reduction for end-stage emphysema: report on the first 98 patientsChest200612951852616537847
- HerthFJErnstABakerKMCharacterization of outcomes 1 year after endoscopic thermal vapor ablation for patients with heterogeneous emphysemaInt J Chron Obstruct Pulmon Dis2012739740522927751
- CrinerGJSternbergALNational Emphysema Treatment Trial: the major outcomes of lung volume reduction surgery in severe emphysemaProc Am Thorac Soc2008539340518453345
- SabanathanSRichardsonJPieri-DaviesSBronchoscopic lung volume reductionJ Cardiovasc Surg (Torino)200344101108
- WatanabeSShimokawaSYotsumotoGSakasegawaKThe use of a Dumon stent for the treatment of a bronchopleural fistulaAnn Thorac Surg20017227627811465202