
Abstract
Background
We recently published that platelet-activating factor receptor (PAFr) is upregulated on the epithelium of the proximal airways of current smokers and also in bronchial epithelial cells exposed to cigarette smoke extract. These treated cells also showed upregulation of Streptococcus pneumoniae adhesion. Bacterial wall phosphorylcholine specifically binds to PAFr expressed on airway epithelium, thus facilitating adherence and tissue invasion, which may be relevant to chronic obstructive pulmonary disease (COPD). Moreover, the use of inhaled corticosteroids (ICS) in COPD patients is associated with an increased risk of invasive respiratory pneumococcal infections.
Objective
In this study, we have investigated whether PAFr expression is especially upregulated in airway epithelium in COPD patients and whether this expression may be modulated by ICS therapy.
Methods
We cross-sectionally evaluated PAFr expression in bronchial biopsies from 15 COPD patients who were current smokers (COPD-smokers) and 12 COPD-ex-smokers, and we compared these to biopsies from 16 smokers with normal lung function. We assessed immunostaining with anti-PAFr monoclonal antibody. We also used material from a previous double-blinded randomized placebo-controlled 6-month ICS intervention study in COPD patients to explore the effect of ICS on PAFr expression. We employed computer-aided image analysis to quantify the percentage of epithelium stained for PAFr.
Results
Markedly enhanced expression of PAFr was found in both COPD-smokers (P<0.005) and COPD-ex-smokers (P<0.002) compared to smokers with normal lung function. There was little evidence that PAFr expression was affected by ICS therapy over 6 months.
Conclusion
Epithelial PAFr expression is upregulated in smokers, especially in those with COPD, and is not obviously affected by ICS therapy.
Background
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease characterized by airflow limitation that is not fully reversible. It is a global health crisis with a substantial and increasing burden, which reduces quality of life, increases national economic burden, is a major cause of acute hospital admissions, and has significant mortality, especially during exacerbations.Citation1–Citation5
Emphasis has been laid on the importance of lower respiratory-tract bacterial colonization in the pathogenesis of, subsequent long-term progression of, and exacerbations in COPD, and so it is likely to be one of the important factors driving inflammatory processes in the airways.Citation6–Citation8 However, the mechanisms underlying the initial bacterial epithelial adherence and subsequent infection remain elusive. Haemophilus influenzae and Streptococcus pneumoniae are the most important pulmonary bacteria during both stable phase of disease and exacerbations of COPD.Citation9–Citation11 Moreover, complex interactions between the host, microbes (both bacteria and viruses), and environmental pollution are associated with exacerbations that are marked by substantial increases in inflammatory markers in the airways.Citation12,Citation13
Large intervention trials and follow-up pharmacoepidemiology studies have recommended the use of inhaled corticosteroids (ICS) to reduce frequency of exacerbations and improve quality of life in more severe COPD patients, and ICS has become an established therapy.Citation14 Although ICS therapy undoubtedly has some positive effects, it is accompanied by an increase in the risk of lower respiratory-tract bacterial infections in COPD patients, especially with S. pneumoniae, which increase in incidence over time.Citation15–Citation17
In an international collaborative study, we recently demonstrated increased platelet-activating factor receptor (PAFr) expression and PAFr-dependent S. pneumoniae adhesion to epithelial cells in culture exposed to cigarette smoke extract, and provided preliminary evidence of an increase in airway epithelial expression of PAFr in smokers.Citation18 PAFr is a G-protein-coupled epithelial cell membrane receptor that naturally binds the phosphorylcholine ligand on the eukaryotic proinflammatory chemokine PAF. Of all bacteria, S. pneumoniae (also Haemophilus and Pseudomonas) cell walls specifically express phosphorylcholine (ChoP), which out-competes PAF to bind to the PAFr. This initiates bacterial uptake by the host cell in a β-arrestin-dependent pathway.Citation19–Citation21
In addition, PAFr-deficient mice are less likely to develop invasive pneumococcal infections as compared to their wild-type counterparts.Citation22 PAFr-dependent pneumococcal adhesion is also upregulated by several other factors in addition to cigarette smoke, including acid, respiratory viral infection, interleukin-1α, and exposure to particulate matter.Citation23 This all fits with the pattern of infection and deterioration seen in COPD.
In this report, we have extended our previous cross-sectional observations to analyze the expression of airway epithelial PAFr in another batch of normal smoker tissue, but also in groups of COPD subjects (smokers and ex-smokers) not on ICS, and in COPD subjects who were involved in a trial of ICS therapy for 6 months.
Materials and methods
Study design
All subjects gave written informed consent prior to participation. The study was approved by the Human Research Ethics Committee (Tasmania) Network.
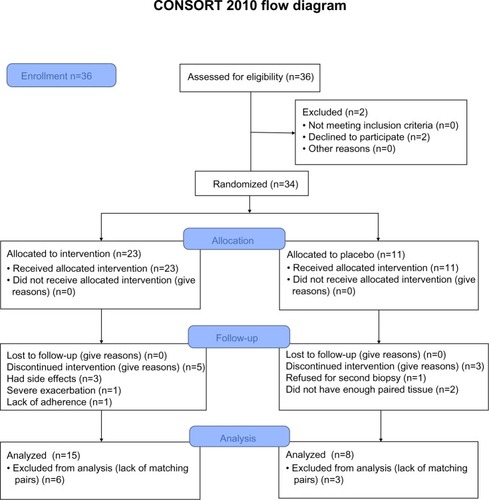
In the cross-sectional study, 17 current smokers with established COPD (COPD-smokers) and 15 ex-smokers with COPD (COPD-ex-smokers) were recruited by advertisement for bronchoscopy and airway biopsy (), and their tissue was compared with biopsies collected in a similar manner from 16 normal lung-function smokers (NLFS). Data from this group was presented in the previous study,Citation18 but this assessment was done de novo on new slides by a separate researcher.
Table 1 Demographic and lung function data for participants in the cross-sectional study
Here, we have also included residual airway biopsy tissue from a previous 6-month randomized control trial using inhaled fluticasoneCitation24 for a preliminary investigation of the effect of ICS on PAFr expression in COPD subjects. In this longitudinal study, a computer-generated random numbers table was used to assign COPD participants to fluticasone propionate (Accuhaler; GlaxoSmithKline plc, London, UK) 500 μg twice daily or placebo via identical multidose dry powder inhaler devices for 6 months (). Before and after treatment, lung function and bronchial biopsies were performed. Half of the participants were current smokers and the other half were ex-smokers. This trial was registered with the Australian New Zealand Clinical Trials Registry (Registry No ACTRN12612001111864). The details for the randomized control trial have been published previously.Citation25 For the current analysis, we had 15 pairs of biopsy tissue in the ICS arm, but only eight in the placebo arm, available for processing.
Figure 1 Study design.
Abbreviation: COPD, chronic obstructive pulmonary disease.
Subjects
The diagnosis of COPD was made according to the Global Initiative for Chronic Obstructive Lung Disease guidelinesCitation1 based on forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio, and was categorized into two groups on the basis of current versus ex-smoking history. For normal lung function current smokers, the inclusion criteria were: a minimum 10 pack-year history of cigarette smoking with spirometry within normal limits, ie, FEV1 >80% of predicted and FEV1/FVC >70%; and no scalloping out of the expiratory descending limb of the flow-volume curve to suggest small airway dysfunction. Normal healthy volunteers had no history of respiratory illness or smoking and had normal lung function.
Exclusion criteria
The exclusion criteria were:
subjects with a history suggestive of asthma, which includes symptoms in childhood, related atopic disorders, eczema or hay fever, substantial day-to-day variability, or prominent nocturnal symptoms;
or a history of wheeze rather than progressive breathlessness;
and any who had previously used ICS (oral or inhaled).
In our study population, there were no major comorbidities such as uncontrolled diabetes, angina, or cardiac failure, nor other coexisting respiratory disorders including pulmonary fibrosis, lung cancer, or bronchiectasis, and subjects were not on medication relating to previously mentioned conditions.
Subjects with an inability to give written informed consent were also excluded.
Inclusion criteria
The inclusion criteria were:
COPD-smokers: aged 40–70 years with a smoking history ≥15 pack-years; subsequently obtained bronchoalveolar lavage fluid had to be free of culturable bacteria; FEV1 40%–80% of predicted, with forced expiratory ratio (ratio of FEV1 to FVC) ≤70% post-bronchodilator and with definite scalloping out of the descending limb of flow-volume loop on spirometry;
COPD-ex-smokers: up to 6 months of smoking cessation.
Normal healthy never-smoking controls also underwent bronchoscopic examination and physiological evaluation. Subjects were at least 18 years old with FEV1/FVC ratio ≥70% and FEV1 ≥80% of predicted; they had no history of respiratory illness.
Bronchoscopy
Bronchoscopy was performed using standard techniques.Citation26 Briefly, subjects were premedicated with nebulized salbutamol (5 mg) 15–30 minutes before the procedure. Sedation was achieved with intravenous midazolam (3–10 mg) and fentanyl (25–100 μg). Lignocaine (4%) was used for topical anesthesia above the vocal cords and lignocaine (2%) was used to anesthetize the airways below the cords, in 2 mL aliquots as required, up to a maximum of 6 mL. Subjects were monitored by pulse oximetry throughout the procedure and oxygen was administered routinely. Eight biopsies from secondary carinae of segmental and subsegmental bronchi in the right lower lobe were obtained. There were no complications from the procedures. Bronchial biopsies were fixed in 4% neutral buffered formalin for 2 hours and subsequently processed into paraffin through graded alcohol and xylene using a Leica ASP 200S tissue processor (Leica Biosystems Nussloch GmbH, Nussloch, Germany).
Immunostaining
Sections were cut at 3 mm intervals from individual paraffin blocks, stained with hematoxylin and eosin, and morphologically assessed for quality and lack of damage.
Following removal of paraffin and rehydration, immunostaining for PAFr was done using an anti-PAFr monoclonal antibody (11A4, clone 21, Cayman Chemicals, Michigan, USA, Catalogue No 160600, 1/80 dilution, for 1 hour at 20°C with no heat retrieval). In each case, a negative control with the primary antibody replaced by a species-appropriate isotype-matched immunoglobulin G2 (X0931 clone DAK-GO1; Dako Denmark A/S, Glostrup, Denmark) was included. Tissue from previously resected lung was used as positive control. Endogenous peroxidase blocking was done with 3% hydrogen peroxide in Milli-RO water (EMD Millipore, Billerica, MA, USA) for 15 minutes at 20°C to eliminate nonspecific staining, but no serum block was necessary. Bound antibodies were elaborated using peroxidase-labeled Envision+ (catalogue number K4001; Dako Denmark A/S) and liquid DAB+ (catalogue number K3468; Dako Denmark A/S).
Biopsy section quantification
Computer-assisted image analysis was performed with a Leica DM 2500 microscope (Leica Microsystems, Wetzlar, Germany), Spot Insight-12 digital camera (Diagnostic Instruments, Inc., Sterling Heights, MI, USA), and Image Pro Plus 7.0 (Media Cybernetics, Inc., Rockville, MD, USA) software. Expression of PAFr was assessed on randomized and coded slides by an operator blinded to smoking and clinical status, and was expressed as the percentage of epithelium with PAFr expression. The cell distribution of staining was also noted qualitatively.
Statistical analysis
For cross-sectional data, the distributions were generally skewed, so results are presented as medians and ranges; non-parametric analyses of variance were performed (Kruskal–Wallis Test comparing medians across all the groups of interest) and specific group differences were then explored as appropriate according to prior hypotheses using the Mann–Whitney U test. To avoid multiple comparisons as much as possible, cross-sectional COPD groups were compared independently with the NLFS group and the results are presented as scatter plots. In the COPD groups, we performed regression analysis for PAFr expression against age, FEV1, and smoking history. For multiple comparisons (two COPD groups versus a single NLFS group), a Bonferroni correction was made (P<0.001).
For the longitudinal study, data were log-transformed because of skewness and the Student’s t-test was used for within group comparisons. The post-ICS group data has also been included in for the cross-sectional analysis, to give an overall perspective.
Statistical analyses were performed using SPSS 15.0 for Windows, 2003 (IBM Corporation, Armonk, NY, USA), with a two-tailed P-value ≤0.05 being considered statistically significant.
Results
Immunostaining was prominent only in the apical part of the bronchial epithelium of NLFS, but staining was darker and more generalized, apparently around the perimeter of cells, in the COPD groups. There was negligible PAFr staining in normal controls. These staining patterns are illustrated in .
Figure 2 PAFr expression in epithelium of bronchial biopsy.
Abbreviations: COPD, chronic obstructive pulmonary disease; PAFr, platelet-activating factor receptor.
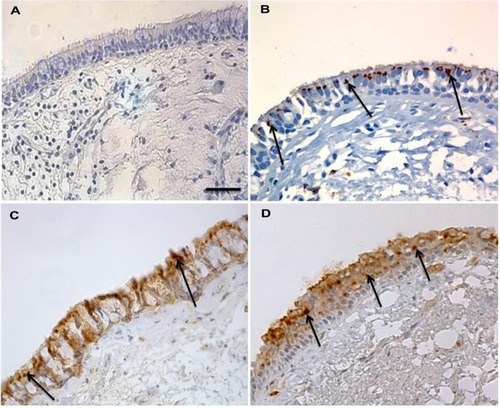
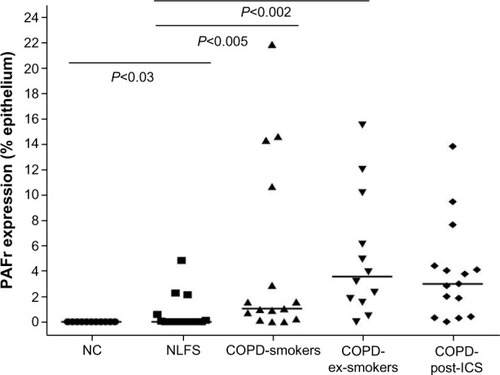
Image analysis confirmed that there was no difference in PAFr expression between the COPD-smokers and COPD-ex-smokers study groups (nonsignificant P-value), but the difference between the NLFS group and the COPD groups (median 0.0%, range 0%–4.9%), was significant (ie, COPD-smokers [P<0.005; median 1.03%, range 0%–21.8%], COPD-ex-smokers [P<0.002; median 3.6%, range 0%–15.5%]). The NLFS group also showed significantly higher PAFr when compared to normal controls (median 0.0%, range 0%–0%). PAFr expression in the ICS-treated group was very similar to the other COPD groups, so no formal statistical testing was done (). In the NLFS group, only seven of the 16 epithelia stained detectably, while, in the two COPD groups combined, 24 had detectable staining out of 27 (χ2; P<0.001); five samples from the COPD groups (two out of 17 COPD-smokers and three out of 15 COPD-ex-smokers) did not have enough tissue for analysis.
Figure 3 Percentage of epithelium showing PAFr expression in cross-sectional study.
Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids; NC, normal control; NLFS, normal lung-function smoker; PAFr, platelet-activating factor receptor.
PAFr expression in the placebo-controlled ICS intervention study
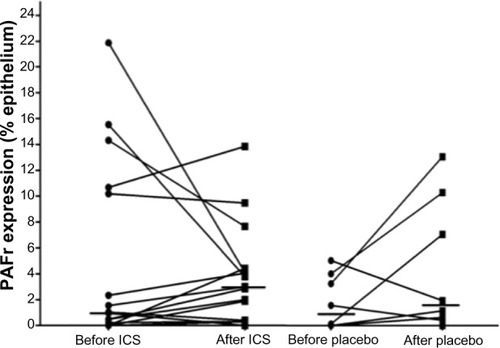
There was considerable variation in PAFr expression within the COPD groups both before and after the treatment phase. The median percent epithelial expression rose in both the groups, by approximately threefold in the ICS limb (P<0.15) but also by approximately twofold in the placebo group over time (). Although the final median level in the ICS groups was greater than in the placebo group, this was neither significant nor were the changes in expression over this time between the groups (P<0.4). It is possible, because of the small number of paired tissues that were available to us, that we saw a type-2 statistical error; thus, a power calculation using nontransformed data was undertaken for a potential real increase in epithelial PAFr expression with ICS, which indicated that, for these estimates of effect size, a bronchoscopic study of over 200 subjects per group would be needed to show a significant positive effect of ICS on PAFr expression.
Figure 4 Relative PAFr expression in the intervention study.
Abbreviations: ICS, inhaled corticosteroids; PAFr, platelet-activating factor receptor.
The regression analyses showed that age and FEV1 had no significant effects on PAFr expression (r=0.23 and 0.11, respectively). However, for pack-years of smoking in the COPD-ex-smokers group, there was quite a strong relationship (r=0.56; P<0.05), but this was not seen in the COPD-smokers subjects (r=0.09; P<0.81).
Discussion
In the present study, we found that in vivo expression of PAFr is significantly upregulated in COPD patients as compared to NLFS. Expression in COPD-smokers and -ex-smokers was similar but quite variable in both groups. This might suggest that smoking cessation may be ineffective in downregulation of PAFr once COPD has developed. Alternatively, it is possible that especially high expression of PAFr in some smokers is both a risk factor for COPD development in the first place, and its progression, even after smoking has ceased.
Overall, our data on the effects of ICS are negative, with at the very most only modest evidence that ICS upregulate PAFr expression – though they certainly do not decrease it – over 6 months, as suggested in earlier in vitro and animal models.Citation27 The present study may also have been relatively short to demonstrate an effect of ICS on PAFr expression, which could potentially elevate risk of pneumococcal disease in COPD patients. The incidence of pneumonia in patients on ICS escalates over years rather than weeks or months.Citation17 It is also possible that the effects of ICS could be more marked in peripheral airways or lung parenchymal epithelium where the clinical problem occurs, while our biopsies were taken only from relatively central airways. Pneumonia occurs at a rate of approximately 1% per year in severe COPD patients on ICS,Citation28 and it is not known whether there is some aberrant change in this small group of individuals or if some generic change occurs on ICS that manifests clinically only in a small percentage. This issue needs further work.
The relationship between cigarette smoking and infection/colonization with S. pneumoniae and H. influenzae has been well documented, and exposure to tobacco smoke is considered as a major risk factor for invasive pneumococcal disease.Citation29,Citation30 Persistence of chronic inflammation and continuous deterioration of lung function following smoking cessation may be attributed to chronic colonization and invasion of lung tissue by respiratory bacterial pathogens, again most commonly S. pneumoniae and H. influenzae.Citation30 Bacterial adherence to lung epithelium and subsequent tissue invasion is thought to be a crucial step in the pathogenesis of respiratory infections. The major respiratory bacterial pathogens are equipped with the surface ligand known as ChoP, which is capable of binding to epithelial PAFr. Especially virulent strains of S. pneumoniae have been shown to adhere to its bacterial cell surface ChoP more firmly with epithelial surface PAFr.Citation19,Citation21,Citation23 We suggest that our data on PAFr expression in the airway epithelium in COPD may be relevant to this as, out of an estimated 109 different bacterial species,Citation31 it is S. pneumoniae and H. influenzae especially (and also Pseudomonas aeruginosa, which is more relevant in cystic fibrosis) that express the ChoP ligand.
In a collaborative study with Grigg et al,Citation18 we recently described significant increases in PAFr-dependent pneumococcal adhesion, PAFr transcript level, and PAFr protein expression in epithelial cell cultures exposed to cigarette smoke extract. Moreover, a specific PAFr antagonist attenuated pneumococcal adhesion. In the same study, we showed enhanced airway epithelial PAFr expression in smokers’ airways for the first time. The present study takes this observation further and confirms much greater upregulation of PAFr expression in the COPD groups than in NLFS. In contrast, Suri et alCitation32 reported no difference in PAFr messenger RNA transcript levels between NLFS and COPD-smokers. However, they did not quantify the PAFr immunoreactivity on bronchial biopsies, and, ultimately, it is protein expression on the epithelial surface that will matter functionally.Citation32 Moreover, the micrograph provided by Suri et alCitation32 seemed to have more PAFr expression in their normal controls than we have found, but the most staining did appear to be in COPD, consistent with our finding. We now need ex vivo epithelial cultures from these patients to see if, functionally, there is greater bacterial adhesion in COPD airways in the group with the greatest PAFr expression.
The regression analysis in the two cross-sectional COPD groups produced interesting outcomes. There was no relationship between either age or severity of airflow obstruction and PAFr-expression, but pack-years of smoking was strongly related, at least in COPD-ex-smokers. The lack of this relationship in current smokers suggests that this long-term effect was confounded by the effect of current smoking. Thus, both current smoking and history of smoking seem important, but, since only a minority of smokers develop COPD, there must also be an additional individual susceptibility effect.
The role that ICS can play in COPD has been extensively studied in the recent past, and ICS are especially effective at reducing exacerbation rates.Citation14 Other described benefits are more tentative, such as reduction in rate of decline in lung function, decreased cancer rates,Citation33,Citation34 and decreased mortality.Citation14 However, a paradoxical effect is that ICS therapy also increases the risk of lower respiratory bacterial infections, especially with S. pneumonia,Citation14,Citation16 an effect that worsens over time.Citation17 An association between ICS and increased risk of hospitalizations due to pneumonia in elderly COPD patients with a high mortality rate, has also been reported.Citation15 Animal models also demonstrate a similar effect of elevated risk of pneumonia with administration of ICS.Citation35
On the basis of our current data, we cannot say that this increased infective risk of ICS is related to enhanced expression of respiratory epithelial PAFr, but it remains a possibility. A much larger clinical study would be needed to determine this, but such a large bronchoscopic investigation is rather unlikely to occur. A better approach may be to see if corticosteroids have any effect on human primary epithelial cell cultures in this regard. It is notable that PAFr expression seemed to increase in both ICS- and placebo-treated COPD subjects over 6 months. Patients are recruited into such studies when they are especially well and free from infection, and this apparently spontaneous change may be a regression back to their more usual status of increased vulnerability.
There were several limiting issues in the study, especially the small numbers of samples available in the ICS intervention study. Furthermore, only large airways were studied, but we are in the process of extending this work to small airway samples and alveolar epithelium obtained at lung resection. Strengths of the present investigation include fairly robust numbers in our cross-sectional study that followed on from the smoking effect we published previously with this tissue bank. The data for the NLFS were obtained de novo and by a separate operator, but are very similar to that published earlier.Citation18
Conclusion
In summary, airway epithelial PAFr expression is significantly upregulated in smokers, but is especially marked in COPD subjects, whether current smokers or not. The significance of this in the pathogenesis and evolution of COPD needs further study, but could be very important in the etiology of chronic and invasive infection with S. pneumoniae and H. influenzae. Whether the increased expression of PAFr is a contributing cause of COPD, or a result of it, needs further investigation.
Acknowledgments
Funding source: National Health and Medical Research Council (NHMRC), Australia (Grant No 490023). The sponsors had no role in the study design, in the collection, analysis, and interpretation of the data, or in the decision to submit the article for publication. Trial registration: Australian New Zealand Clinical Trials Registry (ACTRN12612001111864).
Disclosure
The authors report no conflicts of interest in this work.
References
- http://www.goldcopd.org [homepage on the Internet]Global initiative for Chronic Obstructive Pulmonary Disease2011 Available from: http://www.goldcopd.orgAccessed January 22, 2013
- MathersCDLoncarDProjections of global mortality and burden of disease from 2002 to 2030PLoS Med20063e44217132052
- PasqualeMKSunSXSongFHartnettHJStemkowskiSAImpact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare populationInt J Chron Obstruct Pulmon Dis2012775776423152680
- SuissaSDell’AnielloSErnstPLong-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortalityThorax20126795796322684094
- Soler-CataluñaJJ1Martínez-GarcíaMARomán SánchezPSalcedoENavarroMOchandoRSevere acute exacerbations and mortality in patients with chronic obstructive pulmonary diseaseThorax20056092593116055622
- CabelloHTorresACelisRBacterial colonization of distal airways in healthy subjects and chronic lung disease: a bronchoscopic studyEur Respir J199710113711449163659
- PatelISSeemungalTAWilksMLloyd-OwenSJDonaldsonGCWedzichaJARelationship between bacterial colonisation and the frequency, character, and severity of COPD exacerbationsThorax20025775976412200518
- ErkanLUzunOFindikSKatarDSanicAAticiAGRole of bacteria in acute exacerbations of chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis2008346346718990975
- BanerjeeDKhairOAHoneybourneDImpact of sputum bacteria on airway inflammation and health status in clinical stable COPDEur Respir J20042368569115176680
- SolerNEwigSTorresAFilellaXGonzalezJZaubetAAirway inflammation and bronchial microbial patterns in patients with stable chronic obstructive pulmonary diseaseEur Respir J1999141015102210596683
- MurphyTFBrauerALSchiffmacherATSethiSPersistent colonization by Haemophilus influenzae in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200417026627215117742
- SapeyEStockleyRACOPD exacerbations. 2: aetiologyThorax20066125025816517585
- HurstJRPereraWRWilkinsonTMDonaldsonGCWedzichaJASystemic and upper and lower airway inflammation at exacerbation of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2006173717816179639
- CalverleyPMAndersonJACelliBSalmeterol and fluticasone propionate and survival in chronic obstructive pulmonary diseaseN Engl J Med200735677578917314337
- ErnstPGonzalezAVBrassardPSuissaSInhaled corticosteroid use in chronic obstructive pulmonary disease and the risk of hospitalization for pneumoniaAm J Respir Crit Care Med200717616216617400730
- SinghSAminAVLokeYKLong-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysisArch Intern Med200916921922919204211
- CatesCInhaled corticosteroids in COPD: quantifying risks and benefitsThorax20136849950023242950
- GriggJWaltersHSohalSSCigarette smoke and platelet-activating factor receptor dependent adhesion of Streptococcus pneumoniae to lower airway cellsThorax20126790891322550083
- CundellDRGerardNPGerardCIdanpaan-HeikkilaITuomanenEIStreptococcus pneumoniae anchor to activated human cells by the receptor for platelet-activating factorNature19953774354387566121
- RadinJNOrihuelaCJMurtiGGuglielmoCMurrayPJTuomanenEIBeta-Arrestin 1 participates in platelet-activating factor receptor-mediated endocytosis of Streptococcus pneumoniaeInfect Immun2005737827783516299272
- SwordsWEBuscherBAVer Steeg IiKNon-typeable Haemophilus influenzae adhere to and invade human bronchial epithelial cells via an interaction of lipooligosaccharide with the PAF receptorMol Microbiol200037132710931302
- RijneveldAWWeijerSFlorquinSImproved host defense against pneumococcal pneumonia in platelet-activating factor receptor-deficient miceJ Infect Dis200418971171614767826
- GriggJThe platelet activating factor receptor: a new anti-infective target in respiratory disease?Thorax20126784084122802333
- ReidDWWenYJohnsDPWilliamsTJWardCWaltersEHBronchodilator reversibility, airway eosinophilia and anti-inflammatory effects of inhaled fluticasone in COPD are not relatedRespirology20081379980918811878
- SohalSSReidDSoltaniAChanges in airway histone deacetylase2 in smokers and COPD with inhaled corticosteroids: a randomized controlled trialPLoS One20138e6483323717666
- FeltisBNWignarajahDZhengLIncreased vascular endothelial growth factor and receptors: relationship to angiogenesis in asthmaAm J Respir Crit Care Med20061731201120716528018
- BarbierMAgustiAAlbertiSFluticasone propionate reduces bacterial airway epithelial invasionEur Respir J2008321283128818684852
- KewKMSeniukovichAInhaled steroids and risk of pneumonia for chronic obstructive pulmonary diseaseCochrane Database Syst Rev20143CD01011524615270
- NuortiJPButlerJCFarleyMMCigarette smoking and invasive pneumococcal disease. Active Bacterial Core Surveillance TeamN Engl J Med200034268168910706897
- ArcaviLBenowitzNLCigarette smoking and infectionArch Intern Med20041642206221615534156
- CurtisTPSloanWTScannellJWEstimating prokaryotic diversity and its limitsProc Natl Acad Sci U S A200299104941049912097644
- SuriRMalliaPMartinJEBronchial platelet-activating factor receptor in chronic obstructive pulmonary diseaseRespir Med201410889890424685340
- CelliBRThomasNEAndersonJAEffect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH studyAm J Respir Crit Care Med200817833233818511702
- ParimonTChienJWBrysonCLMcDonellMBUdrisEMAuDHInhaled corticosteroids and risk of lung cancer among patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200717571271917185647
- PattersonCMMorrisonRLD’SouzaATengXSHappelKIInhaled fluticasone propionate impairs pulmonary clearance of Klebsiella pneumoniae in miceRespir Res2012134022651370