
Abstract
Background
Acute exacerbations of chronic obstructive pulmonary disease (COPD) are often treated with antibiotics. Theoretically, to be maximally effective, the antibiotic concentration at sites of infection should exceed the minimum inhibitory concentration at which 90% of the growth of potential pathogens is inhibited (MIC90). A previous study showed that most hospitalized COPD patients had sputum amoxicillin concentrations <LMIC90 when treated with amoxicillin/clavulanic acid. Those with adequate sputum concentrations had better clinical outcomes. Low amoxicillin concentrations can be caused by beta-lactamase activity in the lungs. This study investigated whether patients with sputum amoxicillin concentrations <MIC90 had higher beta-lactamase activity in sputum than patients with a concentration ≥MIC90.
Methods
In total, 23 patients hospitalized for acute exacerbations of COPD and treated with amoxicillin/clavulanic acid were included. Sputum and serum samples were collected at day 3 of treatment to determine beta-lactamase activity in sputum and amoxicillin concentrations in both sputum and serum.
Results
We found no difference in beta-lactamase activity between patients with sputum amoxicillin concentrations <MIC90 and ≥MIC90 (P=0.79). Multivariate logistic regression analysis showed no significant relationship between beta-lactamase activity and sputum amoxicillin concentrations <MIC90 or ≥MIC90 (odds ratio 0.53; 95% confidence interval 0.23–1.2; P=0.13). Amoxicillin concentrations were <MIC90 in 78% of sputum samples and in 30% of serum samples.
Conclusion
In patients treated with amoxicillin/clavulanic acid for an acute exacerbation of COPD, sputum beta-lactamase activity did not differ between those with sputum amoxicillin concentrations <MIC90 or ≥MIC90. The finding that the majority of patients had sputum amoxicillin concentrations <MIC90 suggests that current treatment with antibiotics for acute exacerbations of COPD should be optimized.
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity and mortality throughout the world. The prevalence and burden of COPD are projected to increase in the coming decades due to continued exposure to COPD risk factors and the changing age structure of the world’s population, with COPD likely to become the third leading cause of death by 2020.Citation1 Morbidity and mortality among patients with COPD are in large part related to acute exacerbations (AECOPD), which impair respiratory, physical, social, and emotional functioning both acutely and longitudinally.Citation2–Citation4
The management of AECOPD is empirical and includes oral corticosteroids, often combined with antibiotics, although the need to prescribe these antibiotics is still not convincingly demonstrated.Citation5 Most placebo-controlled antibiotics trials that have been performed have important limitations and are difficult to compare because different definitions of COPD and AECOPD and different endpoints have been used.Citation6,Citation7 Further, these trials were conducted several decades ago, before systemic steroids were widely introduced for the treatment of AECOPD.Citation8–Citation11 In a more recent placebo-controlled study by Llor et al, treatment with amoxicillin/clavulanic acid did show a beneficial effect; however, only 17% of these patients received systemic steroids.Citation12 In a study by Daniels et al, in which the add-on effect of antibiotics was investigated, no difference in clinical outcome after 30 days was observed.Citation13
Theoretically, to be maximally effective, the antibiotic concentration at sites of infection should exceed the minimum inhibitory concentration at which 90% (MIC90) of the growth of potential COPD pathogens such as Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis is inhibited. Levels of antimicrobial agents in sputum, where as a representation of the site of infection many potential pathogenic microorganisms are located, may be a more relevant predictor of efficacy of antibiotics in treatment of an AECOPD than concentrations in serum.Citation14–Citation16 An antibiotic widely used in the treatment of AECOPD is amoxicillin/clavulanic acid.
In a former study by Brusse-Keizer et al, in which 33 COPD patients were treated with amoxicillin/clavulanic acid for AECOPD, sputum amoxicillin concentrations proved to be an important determinant of clinical outcome. Patients with sputum amoxicillin concentrations <MIC90 were hospitalized for 4 days longer than patients with an amoxicillin concentration in sputum ≥MIC90 (7 versus 11 days). Moreover, 67% of patients in this study had a sputum amoxicillin concentration <MIC90.Citation17
The sputum amoxicillin concentration may differ markedly from the concentrations in serum due to various factors, such as the diffusion of amoxicillin into the airways,Citation18 which could be both a host-related as well as a drug-related factor.
A well-known drug-related factor associated with amoxicillin is the susceptibility of amoxicillin to breakdown by beta-lactamase enzymes. In COPD, there are several potential pathogens (eg, H. influenza and M. catarrhalis) that produce these beta-lactamase enzymes.Citation19 The use of beta-lactamase inhibitors, such as clavulanic acid, allows inactivation of certain beta-lactamases.Citation20 An excessive beta-lactamase activity in sputum of COPD patients compared with the dosage of clavulanic acid could possibly be an explanation for the earlier observed low numbers of COPD patients in which an amoxicillin concentration above the MIC90 was reached.
We therefore conducted a study to investigate whether there was any difference in beta-lactamase activity between COPD patients with a sputum amoxicillin concentration <MIC90 and those with a concentration ≥MIC90.
Materials and methods
Patients
This study was part of the Cohort of Mortality and Inflammation in COPD (COMIC) study, a single-center prospective cohort study on the immune status of COPD patients as a determinant of survival. From December 2005 until April 2010, 795 patients were included in the cohort, with a follow-up period of 3 years. To be eligible for the cohort, patients had to meet the following criteria: a clinical diagnosis of COPD, as defined by the Global Initiative for Chronic Obstructive Lung Disease criteria;Citation21 current or former smoker; age 40 years or over; no medical condition compromising survival within the follow-up period or serious psychiatric morbidity; absence of any other active lung disease (eg, sarcoïdosis); no maintenance therapy with antibiotics; and ability to speak Dutch.
In this exploratory study, we had no data available on which we could base our power calculations. We therefore included all patients from the COMIC study when they were hospitalized for an AECOPD that was treated with amoxicillin/clavulanic acid between November 2009 and March 2010.
An AECOPD was defined as an acute event characterized by a worsening of the patient’s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication.Citation21,Citation22 Patients with pneumonia were not excluded, and pneumonia was defined as an acute respiratory infection combined with an infiltrate of the lungs, which was visible on an X-ray of the chest. The infiltrate had to be non-pre-existent, nor reasonably caused by another cause than pneumonia. Further, patients had to be able to produce a sputum sample.
The medical ethics committee of Medisch Specrtum Twente, Enschede, the Netherlands approved the COMIC study and the amendment for the current study, and all patients provided written informed consent for both the COMIC study itself and the amendment. All patients received usual care, which included oral corticosteroids and amoxicillin/clavulanic acid started on the day of admission. Amoxicillin/clavulanic acid was administered according to regular care, which was either orally (500/125 mg three or four times a day) or intravenously (1,000/200 mg four times a day). Some patients received oral and intravenous amoxicillin/clavulanic acid sequentially.
Outcome measures
On the first day of admission, C-reactive protein was measured in blood using the NyoCard® CRP Single Test (Clindia Diagnostics, Leusden, the Netherlands). On the third day of treatment with amoxicillin/clavulanic acid, sputum and serum samples were collected. Sample collection was performed on the third day of treatment because, theoretically, steady-state amoxicillin concentrations in both serum and sputum should be reached by then.Citation23 Serum samples were stored at −80°C. Sputum samples were stored at −80°C after a culture was performed.
Before measuring amoxicillin concentrations and beta-lactamase activity in sputum, sputum samples were thawed and homogenized using a MagNA lyser (3×60 seconds at 6,500 rpm; Roche Diagnostics, Indianapolis, IN, USA). Lysing of cells during the homogenization process was confirmed by microscopy. After homogenization, vials were centrifuged at 10,000 g for 5 minutes to separate cell debris. Amoxicillin concentrations in serum and homogenized sputum samples were determined using a high-performance liquid chromatography/tandem mass spectrometry method.
For amoxicillin, an a priori cut-off level of 2 mg/L was defined as an adequate concentration in both serum and sputum. This value corresponds to the MIC90 for amoxicillin/clavulanic acid. The MIC90 used in this study is derived from local susceptibility tests from the Regional Laboratory of Public Health and is comparable with data published by the European Committee On Susceptibility Testing.Citation24
Beta-lactamase activity was measured directly in homogenized sputum samples by measuring the turnover rate of nitrocefin (Calbiochem, San Diego, CA, USA). Nitrocefin is a beta-lactam with chromogenic properties; it changes color from yellow to red under the influence of beta-lactamase activity. Nitrocefin turnover was measured with spectrophotometry at λ=490 nm in a mixture of 50 μL of homogenized sputum and 50 μL of a 0.025% nitrocefin solution. Beta-lactamase activity was quantified by comparing the measured activity with the activity of a beta-lactamase positive lysate from a H. influenzae culture. Beta-lactamase activity was calculated as a percentage of the activity of the H. influenzae lysate.
Statistical analysis
Continuous variables are expressed as the mean (standard deviation [SD]) or as the median (interquartile range [IQR]). Categorical variables are displayed as numbers (percentages). The crude relationship between beta-lactamase activity and sputum amoxicillin concentrations (<MIC90 or ≥MIC90) was analyzed using the Mann–Whitney U test. To identify confounders in this relationship, first the association of a priori selected possible confounders with beta-lactamase activity was analyzed by Pearson correlation tests, independent samples t-tests, and analysis of variance for normally distributed (continuous/dichotomous/categorical) variables. For non-normally distributed variables, this was performed with, respectively, Spearman correlation tests, Mann–Whitney U tests, and Kruskal–Wallis tests. Variables associated with beta-lactamase activity with a significance of P<0.15 were tested for an association with sputum amoxicillin concentration (<MIC90 or ≥MIC90). For categorical variables, these associations were tested by chi-square tests or by Fisher’s Exact tests, and for continuous variables by independent samples t-tests or Mann–Whitney U tests. Variables that were also associated with sputum amoxicillin concentration with a significance of P<0.15 were considered as potential confounders in the relationship between beta-lactamase activity and sputum amoxicillin concentration and were entered in a multivariate logistic regression model. Subsequently, variables with the highest P-values were eliminated step by step, until the fit of the model decreased significantly, based on the −2 log likelihood. The statistical analyses were performed using Statistical Package for the Social Sciences version 15.0 software (SPSS Inc., Chicago, IL, USA).
Results
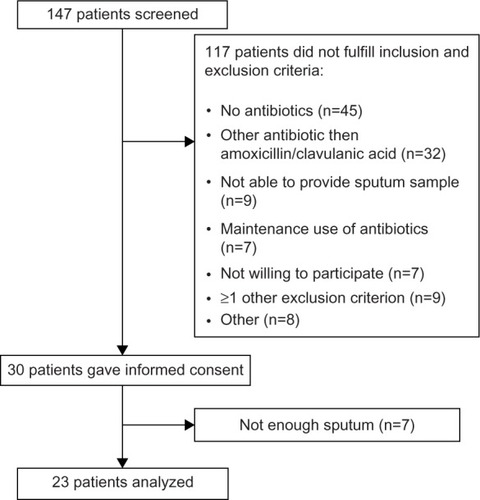
Between November 2009 and March 2010, 147 patients were screened for eligibility (). Of the 30 patients included, 23 provided a sufficient amount of sputum. shows the demographic and clinical characteristics of these 23 patients. The organisms isolated in all patients were confirmed to be susceptible to amoxicillin.
Table 1 Baseline patient demographic and clinical characteristics
Figure 1 Flowchart of study inclusion.
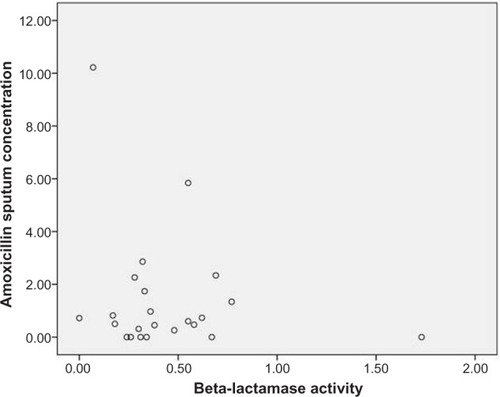
The univariate analysis showed no difference in beta-lactamase activity between patients with a sputum amoxicillin concentration <MIC90 and patients with a concentration ≥MIC90 with, respectively, a median beta-lactamase activity of 0.35 (IQR 0.26–0.59) and 0.32 (IQR 0.18–0.62; P=0.79). Also when individual data of beta-lactamase activity and sputum amoxicillin concentrations were plotted in a scatter diagram () no correlation could be observed (r=−0.06, P=0.80). In 18 of 23 sputum samples (78%), amoxicillin concentrations were below the MIC90. In six of those samples (26%), the amoxicillin concentration was undetectable. Seven of 23 serum samples (30%) had an amoxicillin concentration below the MIC90. All serum samples had detectable levels of amoxicillin.
Figure 2 Scatter diagram of amoxicillin sputum concentration and beta-lactamase activity.
Only route of administration, median daily clavulanic acid dose, and C-reactive protein concentration at admission were univariately associated with beta-lactamase activity (P<0.15; ) and were tested for an association with sputum amoxicillin concentration. All three were also significantly associated with sputum amoxicillin concentration <MIC90 or ≥MIC90 (). Multivariate logistic regression analysis showed no significant relationship between beta-lactamase activity and sputum amoxicillin concentrations <MIC90 versus ≥MIC90 (odds ratio 0.53 for a 0.1% increase in beta-lactamase activity; 95% confidence interval 0.23–1.2; P=0.13). The likelihood of reaching a sputum concentration ≥MIC90 was 80 times greater when amoxicillin/clavulanic acid was administered intravenously versus via the oral route (odds ratio 80.6; 95% confidence interval 1.6–4100; P=0.03).
Table 2 Potential confounders: association with beta-lactamase activity
Table 3 Potential confounders: association with <MIC90 or ≥MIC90
Discussion
No difference in beta-lactamase activity was found between patients with an amoxicillin concentration in sputum <MIC90 and patients with a concentration ≥MIC90 when treated with amoxicillin/clavulanic acid. Although we found that 78% of the patients had a low sputum concentration of amoxicillin (<MIC90), beta-lactamase activity does not seem to be the reason for this observation.
Beta-lactamase activity could not explain the low numbers of patients with an adequate amoxicillin concentration in sputum, so it seems that there should be other host-related or drug-related factors that influence the penetration across the blood-bronchus and alveolar-capillary barriers.
The most important host-related factor is the integrity of the anatomical barriers which may be damaged by inflammation and mechanical injury. In the presence of inflammation, the distribution of amoxicillin may be altered because of increased membrane permeability.Citation25,Citation26 As observed in this and our previous study a high level of C-reactive protein, a marker of systemic inflammation, was related to higher amoxicillin levels.Citation17 C-reactive protein levels could therefore possibly be used as a marker to determine COPD patients in whom adequate concentrations could be reached. However, this does not solve the problem of low concentrations in the majority of patients; this is a worrying feature, especially because our previous study showed that this is also associated with significantly worse clinical outcomes.Citation17 This warrants further investigation into more optimal treatment in these patients.
Since beta-lactam antibiotics such as amoxicillin do not cross membranes readily,Citation27 it might be interesting to look at other antibiotics for the treatment of AECOPD that have a better penetration in sputum.Citation28 Also, the possibility of individually tailored amoxicillin dosing could be investigated, since it has been shown that increased systemic dosing of amoxicillin is associated with increased levels in sputum. We observed that intravenous administration was associated with a higher probability of reaching a sputum amoxicillin concentration ≥MIC90 and led to higher serum concentrations (data not shown), but still 50% of patients had a concentration <MIC90. Further, due to the wide confidence interval that was observed with this probability and since we did not observe any differences in the numbers of patients who reached the MIC90 between intravenous and oral administration in our earlier study,Citation17 we cannot recommend a preference for use of either intravenous or oral administration to reach adequate amoxicillin sputum levels.
Alternative routes of administration such as inhalation of antibiotics could be considered. Aerosolized antibiotics have been proven to deliver high concentrations of antibiotics into the airways with low systemic bioavailability. Stockley et al treated patients with bronchiectasis with nebulized amoxicillin and observed significant reductions in sputum purulence and volume after failure with the same drug given orally.Citation29 It would therefore be interesting to administer amoxicillin/clavulanic acid via inhalation to reach the MIC90, and perhaps to improve the efficacy of antibiotic treatment, as seen in cystic fibrosis.Citation29,Citation30
The observed concentration of amoxicillin in serum is in the range of concentrations found in earlier published studies, which showed concentrations between 3.87 and 45.2 mg/L. Observed concentrations of amoxicillin in sputum ranged between 0.23 and 4.4 mg/L.Citation31–Citation36 However, these concentrations were measured in non-COPD patients and in healthy subjects.
Our study could have been influenced by selection bias, since we only included patients who were able to produce a sufficient amount of sputum on day 3. There might have been a difference in beta-lactamase activity and/or amoxicillin concentration between patients who were able to produce sputum and those who were not. Patients who were able to produce sputum may have had other characteristics in terms of presence/absence of bacteria or cause of exacerbation (eg, viral/bacterial infection). To overcome this issue, induction of sputum with hypertonic saline and the effects on possible dilution of amoxicillin concentration could be explored. Sputum induction has proven to be safe even during exacerbations in COPD patients.Citation37
Since the majority of patients had an amoxicillin concentration <MIC90, the beta-lactamaseactivity of these patients could be compared to the beta-lactamaseactivity of only a small group of patiets with a concentration ≥MIC90. Although there seems to be no difference in median beta-lactamase activity, this study cannot definitely conclude that no relationship exists, and further studies are still necessary.
Conclusion
We observed no relationship between beta-lactamase activity and sputum amoxicillin concentration (<MIC90 or ≥MIC90) in patients treated with amoxicillin/clavulanic acid for an acute exacerbation in COPD. More studies are necessary to confirm this finding. Further, we repeatedly observed that the majority of patients had low sputum concentrations of amoxicillin (<MIC90), suggesting that current treatment with antibiotics should be optimized.
Disclosure
The COMIC study was partly funded by GlaxoSmithKline, the Netherlands, through an unrestricted research grant. Otherwise, the authors report no conflicts of interest in this work.
References
- RabeKFHurdSAnzuetoAGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med200717653255517507545
- CelliBRBarnesPJExacerbations of chronic obstructive pulmonary diseaseEur Respir J2007291224123817540785
- SeemungalTADonaldsonGCPaulEABestallJCJeffriesDJWedzichaJAEffect of exacerbation on quality of life in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1998157141814229603117
- DonaldsonGCSeemungalTABhowmikAWedzichaJARelationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax20025784785212324669
- WilsonRBacterial infection and chronic obstructive pulmonary diseaseEur Respir J19991323323510065660
- HirschmannJVDo bacteria cause exacerbations of COPD?Chest200011819320310893379
- HirschmannJVBacteria and COPD exacerbations reduxChest200111966366711171760
- QuonBSGanWQSinDDContemporary management of acute exacerbations of COPD: a systematic review and metaanalysisChest200813375676618321904
- NiewoehnerDEErblandMLDeupreeRHEffect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study GroupN Engl J Med19993401941194710379017
- DaviesLAngusRMCalverleyPMOral corticosteroids in patients admitted to hospital with exacerbations of chronic obstructive pulmonary disease: a prospective randomised controlled trialLancet199935445646010465169
- MaltaisFOstinelliJBourbeauJComparison of nebulized budesonide and oral prednisolone with placebo in the treatment of acute exacerbations of chronic obstructive pulmonary disease: a randomized controlled trialAm J Respir Crit Care Med200216569870311874817
- LlorCMoragasAHernandezSBayonaCMiravitllesMEfficacy of antibiotic therapy for acute exacerbations of mild to moderate chronic obstructive pulmonary diseaseAm J Respir Crit Care Med201218671672322923662
- DanielsJMSnijdersDde GraaffCSVlaspolderFJansenHMBoersmaWGAntibiotics in addition to systemic corticosteroids for acute exacerbations of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med201018115015719875685
- BaldwinDRHoneybourneDWiseRPulmonary disposition of antimicrobial agents: methodological considerationsAntimicrob Agents Chemother199236117111751416816
- GouldIMHarveyGGolderDPenetration of amoxycillin/clavulanic acid into bronchial mucosa with different dosing regimensThorax19944999910017974318
- DaviesBMaesenFSerum and sputum antibiotic levels after ampicillin, amoxycillin and bacampicillin chronic bronchitis patientsInfection19797Suppl 5S465S468315930
- Brusse-KeizerMten BokumLMovigKRelation between amoxicillin concentration in sputum of COPD patients and length of hospitalizationCOPD20118667021495834
- PenningtonJEPenetration of antibiotics into respiratory secretionsRev Infect Dis1981367737013001
- SportelJHKoëterGHvan AltenaRLöwenbergABoersmaWGRelation between beta-lactamase producing bacteria and patient characteristics in chronic obstructive pulmonary disease (COPD)Thorax1995502492537660337
- BarcelonaLMarinMStamboulianDBetalactam antibiotics combined with bectalactamases inhibitors. Amoxicillin-sulbactamMedicina (B Aires)2008686574 Spanish18416324
- Global Initiative for Chronic Obstructive Lung DiseaseGlobal Strategy for the Diagnosis, Management and Prevention of COPD2011 Available from: http://www.goldcopd.org/Accessed October 9, 2014
- Rodriguez-RoisinRToward a consensus definition for COPD exacerbationsChest2000117398S401S10843984
- LoveringAMPycockCJHarveyJEReevesDSThe pharmacokinetics and sputum penetration of ampicillin and amoxycillin following simultaneous iv administrationJ Antimicrob Chemother1990253853922338417
- European Committee for Antimicrobial Susceptibility TestingMIC determination2014 Available from: http://www.eucast.org/antimicrobial_susceptibility_testing/qc_tablesAccessed December 1, 2014
- BraudeACCohenRDPennerJLPrestonMARebuckASPulmonary disposition of moxalactamChest1984868818836499551
- Bergogne-BerezinEPenetration of antibiotics into the respiratory treeJ Antimicrob Chemother198181711747287601
- HoneybourneDAntibiotic penetration into lung tissuesThorax1994491041068128396
- BaldwinDRHoneybourneDWiseRPulmonary disposition of antimicrobial agents: in vivo observations and clinical relevanceAntimicrob Agents Chemother201136117611801416817
- StockleyRAHillSLBurnettDNebulized amoxicillin in chronic purulent bronchiectasisClin Ther201175935994053147
- HillSLMorrisonHMBurnettDStockleyRAShort term response of patients with bronchiectasis to treatment with amoxycillin given in standard or high doses orally or by inhalationThorax1986415595653787536
- FraschiniFScaglioneFFalchiMPharmacokinetics and tissue distribution of amoxicillin plus clavulanic acid after oral administration in manJ Chemother199021711772199627
- MaesenFPDaviesBIBaurCAmoxycillin/clavulanate in acute purulent exacerbations of chronic bronchitisJ Antimicrob Chemother1987193733833494724
- HavardCWFernandoABrumfittWHamilton-MillerJMA pilot study of ‘Augmentin’ in lower respiratory tract infections: pharmacokinetic and clinical resultsBr J Dis Chest1982762552606751365
- IngoldASputum and serum levels of amoxycillin in chronic bronchial infectionsBr J Dis Chest1975692112161201187
- LoveringAMPycockCJHarveyJEReevesDSThe pharmacokinetics and sputum penetration of ampicillin and amoxycillin following simultaneous iv administrationJ Antimicrob Chemother1990253853922338417
- HillSLBurnettDLoveringALStockleyRAUse of an enzyme-linked immunosorbent assay to assess penetration of amoxicillin into lung secretionsAntimicrob Agents Chemother199236154515521510453
- BathoornELieskerJPostmaDKoëterGvan OosterhoutAJKerstjensHASafety of sputum induction during exacerbations of COPDChest200713143243817296644