
Abstract
Exercise tests are often used to evaluate the functional status of patients with COPD. However, to the best of our knowledge, a comprehensive systematic comparison of these tests has not been performed. We systematically reviewed studies reporting the repeatability and/or reproducibility of these tests, and studies comparing their sensitivity to therapeutic intervention. A systematic review identified primary manuscripts in English reporting relevant data on the following exercise tests: 6-minute walk test (6MWT) and 12-minute walk test, incremental and endurance shuttle walk tests (ISWT and ESWT, respectively), incremental and endurance cycle ergometer tests, and incremental and endurance treadmill tests. We identified 71 relevant studies. Good repeatability (for the 6MWT and ESWT) and reproducibility (for the 6MWT, 12-minute walk test, ISWT, ESWT, and incremental cycle ergometer test) were reported by most studies assessing these tests, providing patients were familiarized with them beforehand. The 6MWT, ISWT, and particularly the ESWT were reported to be sensitive to therapeutic intervention. Protocol variations (eg, track layout or supplemental oxygen use) affected performance significantly in several studies. This review shows that while the validity of several tests has been established, for others further study is required. Future work will assess the link between these tests, physiological mechanisms, and patient-reported measures.
Introduction
COPD is a leading cause of death worldwide, and the prevalence of the disease is projected to increase as the population ages and as exposure to risk factors, such as smoking, continues.Citation1–Citation3 COPD is characterized by symptoms of breathlessness and reduced exercise capacity.Citation4,Citation5 Decrements in exercise capacity can result in reduced ability to perform activities of daily living, and the resultant inactivity and sedentary lifestyle can further exacerbate exercise impairment (the COPD “vicious circle”).Citation6
In clinical practice, spirometry is recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) for the diagnosis of COPD.Citation5 However, the results of spirometry alone poorly predict disability and quality of life in patients with COPDCitation7 and correlate only weakly with dyspnea, exercise capacity, and health status.Citation8–Citation10 Recent guidelines on the diagnosis and treatment of COPD indicate that assessment of disease severity is improved by using additional functional criteria such as exercise capacity.Citation4,Citation5,Citation11 Quantification of the degree of functional impairment is therefore important for the assessment of response to treatment and as an outcome for clinical trials.
There are a number of laboratory- and field-based tests currently used for the assessment of exercise capacity, including the 6- and 12-minute walk tests (6MWT and 12MWT, respectively), the incremental and endurance shuttle walk tests (ISWT and ESWT, respectively), the incremental and endurance cycle ergometer tests (ICET and ECET, respectively), and the incremental and endurance treadmill tests (ITT and ETT, respectively). However, there is no consensus about which test is the most appropriate for use in patients with COPD. These tests have different primary outcomes (eg, endurance time, distance, oxygen consumption) that may reflect different physiological parameters. It is therefore difficult to compare results across studies, limiting interpretation of the published literature in this field. Furthermore, the relative merits of different tests have not been established.
The systematic review presented here therefore evaluated evidence of the “repeatability” (defined as consistency of results when multiple tests are conducted on the same day) and the “reproducibility” (consistency of results when tests are conducted on different days) of the tests. The review also assessed the relative properties of the eight commonly used exercise tests and their sensitivity to therapeutic intervention (such as rehabilitative, pharmacological, or surgical procedures). In addition, the effect of protocol variations within each test was assessed across studies. When possible, results were placed in the context of available minimal clinically important difference (MCID) values, which have thus far been ascertained for the 6MWT,Citation12 ISWT,Citation13 ESWT,Citation14 and ICET.Citation12 Investigation of these factors will be useful in guiding test selection in clinical practice and for outcome measures in clinical trials. As these tests are often also used as interventions, evaluation of exercise testing modalities in patients with COPD will also inform the clinical development of optimal exercise rehabilitation strategies.
Methods
Search strategy
Literature searches were conducted using Ovid® (Ovid Technologies Inc., New York, NY, USA), incorporating Ovid Medline® (US National Library of Medicine, Bethesda, MD, USA), for the period from 1948 to January 22, 2013, Ovid Embase™ (Elsevier Inc., Philadelphia, PA, USA) for 1974 to January 22, 2013, and The Cochrane Library (John Wiley and Sons Ltd, Hoboken, NJ, USA) for 1962 to January 22, 2013 (see Tables S1–S3). Search strings were constructed to identify studies reporting primary data on the outcomes of the following exercise tests in patients with COPD: the 6MWT, 12MWT, ISWT, ESWT, ICET, ECET, ITT, and ETT. The full search strings are presented in the “Supplementary materials” section.
Study selection
Study selection followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for performing a systematic literature review.Citation15 Review articles and studies not published in English were excluded using search-engine filters. Studies confounded by comorbidities (such as cancers, diabetes, and non-COPD respiratory-tract diseases) were excluded on review of title/abstract. The remaining studies were screened based on titles and abstracts, and full articles were reviewed when their relevance was unclear from the abstract. Screening was performed by a single author (GM) and records were initially reviewed by title/abstract; a full paper review was subsequently undertaken for publications that could not be excluded by title/abstract. Included records were verified by a second author (IF). A 30% random sample of excluded records was also reviewed by the second author (IF). Disagreements were settled by consultation with the remaining authors.
When reviewing abstracts or full papers, records were excluded if they were reviews, were not in the English language, studied patients with confounding comorbidities (eg, cancers or diabetes), did not use an exercise test as an outcome measure, or examined an intervention other than our interventions of interest (pulmonary rehabilitation, bronchodilator therapy, and lung-volume reduction surgery). Specific inclusion criteria included any definition of COPD (including emphysema- and bronchitis-specific studies); interventions were included only in our comparison of sensitivity and limited to pulmonary rehabilitation, bronchodilation, and lung-volume reduction surgery. Included test outcomes are outlined in the “Data abstraction” section. Following screening, studies were subsequently included for assessment if they reported data on:
repeatability (studies reporting data from two or more performances of the same test[s] on the same day under the same conditions)
reproducibility (studies reporting data from two or more performances of the same test[s] on different days under the same conditions)
comparisons of sensitivity (studies reporting responses of two or more tests to the following therapeutic interventions: pulmonary rehabilitation, bronchodilator therapy, or lung-volume reduction surgery)
protocol variations (studies reporting two or more performances of a test when protocol parameters have been modified).
Data abstraction
Data were primarily abstracted by a single author (GM) and reviewed by all co-authors. A randomly generated selection of 30% of all articles was reviewed by a second author (IF) for quality-control purposes.
The following outcomes of exercise tests were recorded: distance or stages achieved for the 6MWT, 12MWT, and ISWT; duration of exercise for the ESWT, ECET, and ETT; and the highest recorded volume of oxygen consumption (peak VO2) and/or maximum workload (Wmax) for the ICET and ITT. Articles merited inclusion in this review if they reported: outcomes of the specified tests when performed repeatedly under the same conditions, either on the same day (repeatability) or on different days (reproducibility); changes in response before and after therapeutic intervention (comparison of sensitivity); or effects of within-test variations in protocol (protocol variation).
Studies comparing the sensitivity of tests were also assessed for expression by the authors of preference for any specific test. When distances were reported in feet, values were converted to meters using standard conversion criteria stated by the International Bureau of Weights and Measures (0.3048 meters per foot). Within each publication, tests for which results are available are referred to as “test 1”, “test 2”, etc; occasions on which a test has been described by the authors, but results are not reported (such as for practice tests), are referred to as “familiarizations”.
Results
Overview of identified studies
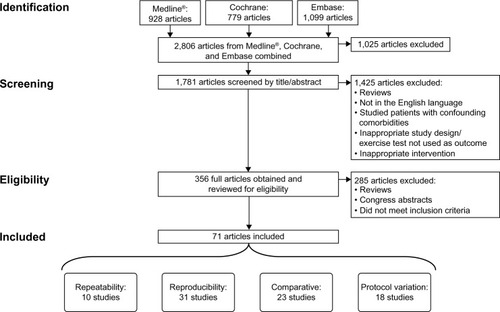
The search methodology used to identify relevant articles is summarized in . Of 1,781 unique articles screened, 71 were ultimately deemed eligible for inclusion in this review.
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram detailing the identification and inclusion process of the articles. Some studies are included in more than one analysis category; consequently, the aggregate number of studies in the repeatability, reproducibility, comparative, and protocol variation groups adds up to more than 71.
Studies assessing the repeatability and reproducibility of tests
Clinical practice is influenced by factors such as the repeatability and reproducibility of exercise tests in patients with COPD. These factors have been extensively assessed for the 6MWT and 12MWT; data are more limited for the ISWT, ESWT, ITT, and ETT (23 references for the 6/12MWT; 12 for the IWST, ESWT, ITT, and ETT; seven for the ICET and ECET; this made 37 references in total owing to overlap of these categories). summarizes the results of studies assessing the repeatability and reproducibility of the 6MWT and 12MWT; focuses on the ISWT, ESWT, ETT, and ITT; and presents data on the ICET and ECET.
Table 1 Repeatability and reproducibility of the 6- and 12-minute walk tests
Table 2 Repeatability and reproducibility of incremental shuttle walk test, endurance shuttle walk test, incremental treadmill test, and endurance treadmill test
Table 3 Repeatability and reproducibility of cycling tests
Six studies presented repeatability data for the 6MWT ().Citation16–Citation21 Of these, five reported a significant increase in 6MWT distance from the first to the second test;Citation16–Citation20 the remaining study found no differences between results, though patients had been previously familiarized with the tests.Citation21 The three studies clearly reporting the results of three 6MWTs performed on the same day found that there was no significant difference between the second and third tests.Citation18,Citation20,Citation21 The only study that presented intra-class correlation coefficients (ICCs) for repeated 6MWTs on the same day reported excellent repeatability (ICC =0.94), but also observed that the second test was significantly higher.Citation16 For the 12MWT, the distance achieved was reported to be repeatable in the only study in which patients were retested on the same day.Citation22 Equivocal results were reported for the repeatability of the ISWT by three studies;Citation18,Citation21,Citation23 one found that the distance was repeatable after familiarization,Citation18 but the other two reported poor repeatability even after familiarization ().Citation21,Citation23 For the ESWT, exercise duration was reported to be repeatable in the two studies in which patients were retested on the same day.Citation23,Citation24 One study reported that peak VO2 and Wmax were repeatable for the ICET ().Citation25 No repeatability data were found for the ECET, ITT, or ETT.
Reproducibility of the 6MWT was assessed in 12 studies,Citation17,Citation18,Citation26–Citation35 six of which reported that distances achieved in the 6MWT demonstrated good reproducibility between the first and second tests ().Citation17,Citation27,Citation28,Citation32,Citation35 Of two studies presenting reproducibility results from three 6MWTs,Citation18,Citation28 only one reported reproducibility between the second and third tests.Citation28 Two further studies reported results of tests after familiarization;Citation26,Citation30 only one found 6MWT results to be reproducible.Citation30 The only study presenting ICC data between the first and second 6MWT performance showed high reproducibility (ICC =0.88), but also that there was a significant increase in distance in the second 6MWT.Citation33 Reproducibility of the 12MWT was assessed in seven studies.Citation22,Citation36–Citation41 Five of these presented the results of three or more tests, and reported that the 12MWT distance increased significantly from the first to the second test;Citation36,Citation37,Citation39–Citation41 one of these studies reported that in a subset of patients who readily experienced exercise-induced hypoxia, the 12MWT distance did not significantly change from the first to the second to the third test.Citation36 Two additional studies, in which there had been prior familiarization with the test, reported no significant change in 12MWT distance between subsequent first and second tests.Citation22,Citation38 For the ISWT, five studies presented data assessing reproducibility: from the first to the second test with prior familiarization,Citation42,Citation43 from the first to the second test without prior familiarization,Citation44,Citation45 and from the second to the third test without prior familiarization ().Citation18 Two further studies evaluating the ESWT reported reproducibility (either from the first to the second test with prior familiarization,Citation46 or from the second to the third test without familiarization).Citation47 Good reproducibility of the ICET from the first to the second test was reported by four studies both withCitation30 and without prior familiarization ().Citation25,Citation48,Citation49 Two further studies reported an increase in ICET duration from the first to the second test with no familiarization,Citation41,Citation50 with one of these studies reporting progressive increases in ICET duration from the first through to the fourth test.Citation41 In the only study reporting data for the ECET, duration was found to have excellent reproducibility (ICC =0.85).Citation51 Reproducibility was also found to be excellent in the only study reporting such data for the ETT (no significant increases from the first to the second test, ICC =0.85),Citation52 but less so for the ITT (increased peak VO2 from the first to the second test, statistical test not reported).Citation50
Several studies were identified that compared the repeatability and/or reproducibility of two or more exercise tests. One study observed that repeatability for the 6MWT and the ISWT was comparable, but that the ISWT was more reproducible.Citation18 However, another study showed that the ISWT was more repeatable than the 6MWT.Citation21 One study reported that both the 6MWT and the ICET were reproducible.Citation30 The ESWT was reported to be more repeatable than the ISWT in one study, when measured in two sessions before and two sessions after pulmonary rehabilitation.Citation23 In another study, both 12MWT distance and ICET performance were found to increase significantly and progressively over four tests; the ICET was found to have no obvious advantages over the 12MWT when assessing exercise performance.Citation41 The final study to report reproducibility of more than one test reported that peak VO2 increased from test 1 to test 2 in both the ICET and the ITT; however, the authors did not report the statistical tests used.Citation50 Three studiesCitation18,Citation28,Citation30 were found that compared the reproducibility of two or more exercise tests. Of these, two reported that the 6MWT was found to have similar reproducibility to the ISWTCitation18 and the ICET.Citation30
Studies comparing responses to interventions among exercise tests
In total, 23 studies were identified that compared responses of two or more exercise tests after one of the following interventions: pulmonary rehabilitation (16 studies),Citation23,Citation47,Citation53–Citation66 administration of bronchodilators (six studies),Citation14,Citation18,Citation67–Citation70 and lung-volume reduction surgery (one study)Citation71 (). Of the 16 studies that assessed pulmonary rehabilitation in patients with COPD, the most commonly assessed test was the 6MWT, which was reported by eleven studies.Citation53–Citation55,Citation57–Citation59,Citation61,Citation63–Citation66
Table 4 Between-test comparisons of sensitivity to interventions
Two studies compared the response to the 6MWT and ITT after pulmonary rehabilitation; both reported significant increases in 6MWT distance and ITT performance (peak VO2Citation53 and work-level completed).Citation57 However, the latter study did not observe a significant response in peak VO2 during the ITT after pulmonary rehabilitation.Citation57 One further study assessed the 6MWT and ITT during nutritional supplementation and placebo, and reported that the 6MWT distance was sensitive to pulmonary rehabilitation (>MCID); but these authors did not present peak VO2 or Wmax data for the ITT.Citation54 Another study assessed the 6MWT, ETT, and ITT, and found that both the ETT and the ITT were sensitive to pulmonary rehabilitation, whereas the 6MWT was not (again, the authors did not report peak VO2 or Wmax data for the ITT).Citation58 Several further studies reported equivocal findings when comparing the 6MWT with the ICETCitation55,Citation63–Citation65 after pulmonary rehabilitation. All three studies comparing the ECET with the 6MWT found the ECET to be more responsive to pulmonary rehabilitation.Citation63,Citation65,Citation66 One study assessing responses to pulmonary rehabilitation reported similar sensitivities for the 6MWT and the ISWT, with both giving responses that exceeded the MCID.Citation61 All four studies assessing the sensitivity of the ISWT and the ESWT to pulmonary rehabilitation reported a significant improvement in performance for both tests;Citation23,Citation47,Citation60,Citation62 however, in all four studies the response of the ESWT was greater and in two the ISWT response did not reach the MCID.Citation23,Citation47 An additional study suggested that although both tests showed a significant response that was above the MCID, the ESWT was more responsive to pulmonary rehabilitation than the 6MWT.Citation59 Equivocal sensitivity was observed in response to pulmonary rehabilitation when using the 12MWT and the ICET.Citation56
Of the six studies comparing the responses of two or more exercise tests to bronchodilator therapy,Citation14,Citation18,Citation67–Citation70 one reported the 6MWT to be more responsive to pharmacological intervention than the 12MWTCitation67 and one reported the 6MWT to be more responsive to pharmacological intervention than the ISWT.Citation18 The standardized (percentage) increase in response to the ECET was higher than that of either the 6MWT or the ICET in one study,Citation68 and higher than that of the ETT in another.Citation70 One study reported the response of the ESWT to bronchodilation to be greater than that of the 6MWTCitation14 and one study reported the response of the ESWT to bronchodilation to be greater than that of the ECET.Citation69
Finally, one study assessed exercise test performance 1 year after lung-volume reduction surgery, and reported a 9.1% increase in 6MWT distance and a 15.4% increase in ICET Wmax, but noted that ICET peak VO2 did not increase significantly.Citation71
Minimal clinically important differences in responses to interventions
MCIDs have been thus far ascertained for the 6MWT (26 meters),Citation12 the ISWT (48 meters),Citation13 the ESWT (45 seconds–85 seconds or 60 meters–115 meters [MCID calculated after bronchodilatory intervention]),Citation72 and the ICET (4 watts).Citation12 Of the eleven studies assessing the 6MWT in response to pulmonary rehabilitation, nine reported an increase in excess of the recognized MCID,Citation53–Citation55,Citation57,Citation59,Citation61,Citation63,Citation65,Citation66 with another reporting a significant increase in distance of less than the MCIDCitation64 (the remaining study reported no significant change in 6MWT distance after pulmonary rehabilitationCitation58); these increases ranged in magnitude from 4.8% to 36.3%. Five studies reported a significant response of the ISWT to pulmonary rehabilitation ranging from 15.0% to 52.9%,Citation23,Citation47,Citation60–Citation62 with three finding that the distance observed reached the MCID.Citation60–Citation62 All five studies assessing the sensitivity of the ESWT to pulmonary rehabilitation reported that distance and/or duration increased in excess of the MCID (increases ranged from 88.0% to 205.4% when expressed as time [seconds];Citation23,Citation47,Citation59,Citation60,Citation62 and from 92.0% to 140.0% when expressed as distance [meters]).Citation47,Citation59,Citation62 Of five studies assessing the ICET before and after pulmonary rehabilitation,Citation55,Citation56,Citation63–Citation65 two reported Wmax responses in excess of the MCID,Citation56,Citation63 and another reported significant changes in Wmax that did not reach the MCIDCitation64 (the increased ICET performance observed across these studies ranged from 5.4% to 20.0% for peak VO2 and 8.6% to 18.0% for Wmax). The two remaining studies did not observe a significant change in ICET peak VO2 or Wmax after pulmonary rehabilitation.Citation55,Citation65 All three studies reporting the response of the ECET to pulmonary rehabilitation observed significant increases in duration (ranging from 73.5% to 166.0%).Citation63,Citation65,Citation66 Four studies assessed the ITT before and after pulmonary rehabilitation; two did not present data for either peak VO2 or Wmax.Citation54,Citation58 Of the remaining two studies, one reported a significant increase in peak VO2 of 14.3%,Citation53 while the other found no significant increase in peak VO2 after pulmonary rehabilitation.Citation58 The only study assessing the ETT before and after pulmonary rehabilitation reported significant increases in duration (27.4%) and distance (22.1%).Citation58
Of the four studies assessing the 6MWT before and after bronchodilator therapy, two reported improvements in distance that exceeded the MCID (one found an increase in 6MWT distance of 8.7%;Citation18 the other reported a higher absolute distance increase [53.6 meters], but did not present baseline values; therefore the percentage increase cannot be calculatedCitation67). The third study reported a small (1.2%) but significant increase in 6MWT distance,Citation68 while the remaining study found no significant difference in 6MWT distance.Citation14 One study found a significant increase in 12MWT distance after bronchodilation in excess of the MCID (59.9 meters), but did not provide baseline values.Citation67 One study reported a significant increase in ISWT performance after bronchodilators (30 meters) that did not reach the MCID.Citation18 Two studies reported significant increases in ESWT performance above the MCID, of 144 metersCitation14 and 164 seconds,Citation69 respectively. One study reported a small but significant improvement in ICET Wmax of 3.4% after bronchodilator therapy, but noted that peak VO2 did not increase significantly.Citation68 Three studies assessed ECET performance after bronchodilators; two found significant increases in duration of 18.0%Citation68 and 47.1%,Citation70 with the remaining study reporting no significant improvement in ECET duration.Citation69
In the only study assessing lung-volume reduction surgery, a 6MWT improvement in excess of the MCID was seen; however, ICET improvements (whether peak VO2 or Wmax) did not reach MCID.Citation71
Studies assessing within-test variations in protocol
Eighteen studies were identified that assessed minor variations in protocol within a specific exercise test ().Citation17,Citation20,Citation33,Citation46,Citation73–Citation86 Variations (such as track environment or layout and the type of encouragement provided by the investigators to the patient) affected test outcomes (and consequently, their repeatability and reproducibility).
Table 5 Protocol variations reported to affect performance of exercise capacity test
Discussion
A number of laboratory- and field-based exercise tests are used to assess the degree of functional impairment in patients with COPD. However, the choice of which test to use in clinical trials historically seems to have been made on a practical basis (tests such as the 6MWT and 12MWT require little time, organization, or equipment), or without necessarily taking into account how representative the exercise modality used is to activities of daily living for these patients (eg, cycling tests) or the likely impact of the intervention on the outcome of the test. Equally there are few data describing the relative merits of these tests employed simultaneously to evaluate interventions such as rehabilitation and bronchodilator therapy. Results from this systematic review indicate that there is an extensive body of published literature regarding the performance of the eight exercise tests that are widely used.
Repeatability data were found for only the 6MWT, 12MWT, ISWT, ESWT, and ICET. As could be anticipated, we did not identify studies assessing the repeatability of the ECET, ITT, or ETT; these studies test to exhaustion and would be impractical for patients with COPD to perform repeatedly on the same day. Of those reported, the 6MWT was by far the most thoroughly assessed. This may reflect its simplicity and relevance to daily life.Citation87 However, a substantial proportion of the reported data does not explicitly support 6MWT repeatability. Some studies suggested that the ISWT was more repeatableCitation21 and reproducibleCitation18 than the 6MWT, while another found that the ESWT was, in turn, more repeatable than the ISWT.Citation23 The comparative results of exercise tests are inconsistent. Furthermore, there are only very limited data to support the repeatability and/or reproducibility of all cycle tests and treadmill tests. Repeatability and reproducibility were generally improved with familiarization in all types of test. Although this review assesses the influence of protocol variations, it is possible that some studies in which variations were not the primary focus may not have been identified. However, it is clear that even in ostensibly identical tests (eg, two studies reporting the 6MWT), responses can be significantly affected by subtle variations in track layout or environment, or by encouragement from the researchers conducting the test.
When studies reporting the sensitivity of two or more exercise tests to therapeutic intervention were reviewed, there was no consistent evidence supporting the use of one test over any other. Nine of the eleven studies assessing the 6MWT after pulmonary rehabilitation,Citation53–Citation55,Citation57,Citation59,Citation61,Citation63,Citation65,Citation66 two of the four studies assessing 6MWT after bronchodilators,Citation18,Citation67 and the only study assessing the 6MWT after lung-volume reduction surgeryCitation71 all reported distance improvements greater than the MCID. Additionally, three of the five studies assessing ISWTCitation60–Citation62 and all five of the studies assessing ESWT after pulmonary rehabilitationCitation23,Citation47,Citation59,Citation60,Citation62 reported distance improvements greater than the MCID. Performance improvements were also observed to be in excess of the MCID in the only two studies assessing the ESWT following bronchodilator therapy;Citation14,Citation69 this was therefore the only exercise test reported by multiple papers that consistently responded to therapeutic interventions to a clinically relevant degree. It must be considered that these exercise tests have differing physiological demands, and it may be that the benefits of each intervention are measured differently by each test. However, limited data for bronchodilator therapy and lung-volume reduction surgery make it difficult to identify any obvious differences in the responses of tests to these interventions.
The review has several limitations that must be acknowledged. As well as identifying whether or not test responses have exceeded the MCID, we have also reported percentage changes in exercise test performance whenever possible to enable a very crude comparison of test outcomes recorded in different units. However, we are aware that the validity of this comparison relies on a direct relationship between these test outcomes, which is unlikely to be true: a large percentage change in one test result may not be equivalent to a large percentage change in another.
In an attempt to assess the validity of exercise tests in patients with COPD as comprehensively as possible, we have collated data from studies that have used various definitions of COPD, which include distinct subcategories such as emphysema and chronic bronchitis, and that have employed diverse methods of assessing diagnosis and severity. Moreover, the study designs included are very diverse. These issues make meaningful meta-analysis difficult. We have, however, tried to provide the ranges of responses (both absolute and percentage changes) when possible, to provide an indication of the magnitude of exercise test responses. A further consequence of the comprehensive nature of this review is that the sample sizes of the identified studies vary widely. For this reason, we have included study sample sizes in our tables.
Decisions regarding which test to use are also influenced by the practicalities of routine clinical practice. It is reasonable to assume that walking is more representative of daily life than cycling for patients with COPD. Furthermore, given the equivocal evidence for the use of the ESWT over the ISWT, clinicians may wish to consider that the ESWT requires a prior “workload setting” ISWT to be performed by the patient, requiring additional time and resource considerations. Any test of exercise capacity should be highly repeatable and reproducible and also should be able to detect changes in performance after interventions aiming to improve exercise capacity.
Conclusion
This review of the published literature has found good evidence to support the repeatability and reproducibility of all tests, particularly the 6MWT, as long as a prior familiarization is conducted. There is consistent evidence to suggest that the ESWT is highly sensitive to therapeutic intervention. Sensitivity data that are available for other tests are largely inconsistent, and the 6MWT and ISWT appear to be less sensitive to intervention than the ESWT and ICET. These factors, allied to practical aspects, must be considered when planning interventional trials.
Author contributions
All authors contributed to the conception and design of the study, the analysis and interpretation of data, and revision of the manuscript. All authors approved the final version of the manuscript for publication.
Acknowledgments
The study was funded by GlaxoSmithKline UK. Writing support was provided by Martin Bell of Oxford Pharma-Genesis™ Ltd, funded by GlaxoSmithKline UK. Georgina Meakin and Iain Fotheringham are employees of Oxford PharmaGenesis Ltd, which has received funding from GlaxoSmithKline UK. Yogesh Suresh Punekar, John Riley, and Sarah Cockle are current employees of GlaxoSmithKline, Uxbridge, UK. Sally J Singh was involved with the development of the incremental shuttle walk test, and has served on advisory boards for GlaxoSmithKline. Sally J Singh was part funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East Midlands. Support was also provided by the NIHR Leicester Respiratory Biomedical Research Unit. The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR, or the Department of Health.
Supplementary materials
Complete Ovid search strings
Table S1 Embase™ search strings, search conducted January 22, 2013
Table S2 Medline® search strings, search conducted January 22, 2013
Table S3 The Cochrane Library search strings, search conducted January 22, 2013
Disclosure
Other than the funding outlined in the “Acknowledgments” section, the authors declare no conflicts of interest in this work.
References
- LopezADShibuyaKRaoCChronic obstructive pulmonary disease: current burden and future projectionsEur Respir J200627239741216452599
- HalbertRJNatoliJLGanoABadamgaravEBuistASManninoDMGlobal burden of COPD: systematic review and meta-analysisEur Respir J200628352353216611654
- MathersCDLoncarDProjections of global mortality and burden of disease from 2002 to 2030PLoS Med2006311e44217132052
- American Thoracic Society/European Respiratory Society Task ForceStandards for the Diagnosis and Management of Patients with COPD [Internet] Version 1.2New YorkAmerican Thoracic Society2004 [updated September 8, 2005]. Available from: http://www.thoracic.org/go/copd-guidelines/Accessed May 19, 2014
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)Global Strategy for the Diagnosis, Management and Prevention of COPD [Internet]GOLD2014 Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jun11.pdfAccessed September 12, 2014
- CorhayJLDangDNVan CauwenbergeHLouisRPulmonary rehabilitation and COPD: providing patients a good environment for optimizing therapyInt J Chron Obstruct Pulmon Dis20149273924368884
- JonesPMiravitllesMvan der MolenTKulichKBeyond FEV(1) in COPD: a review of patient-reported outcomes and their measurementInt J Chron Obstruct Pulmon Dis2012769770923093901
- CooperCBThe connection between chronic obstructive pulmonary disease symptoms and hyperinflation and its impact on exercise and functionAm J Med200611910 Suppl 1213116996896
- JonesPWIssues concerning health-related quality of life in COPDChest1995107Suppl 5187S193S7743825
- MahlerDAHarverAA factor analysis of dyspnea ratings, respiratory muscle strength, and lung function in patients with chronic obstructive pulmonary diseaseAm Rev Respir Dis19921452 Pt 14674701736759
- National Institute for Health and Clinical Excellence (NICE)Management of chronic obstructive pulmonary disease in adults in primary and secondary care (partial update)NICE guideline CG101LondonNICE2010 Available from: http://guidance.nice.org.uk/cg101Accessed May 19, 2014
- PuhanMAChandraDMosenifarZThe minimal important difference of exercise tests in severe COPDEur Respir J201137478479020693247
- SinghSJJonesPWEvansRMorganMDMinimum clinically important improvement for the incremental shuttle walking testThorax200863977577718390634
- PepinVBrodeurJLacasseYSix-minute walking versus shuttle walking: responsiveness to bronchodilation in chronic obstructive pulmonary diseaseThorax200762429129817099077
- MoherDLiberatiATetzlaffJAltmanDGGroupPPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementBMJ2009339b253519622551
- AnderssonMMobergLSvantessonUSundbomAJohanssonHEmtnerMMeasuring walking speed in COPD: Test-retest reliability of the 30-metre walk test and comparison with the 6-minute walk testPrim Care Respir J201120443444021938352
- BansalVHillKDolmageTEBrooksDWoonLJGoldsteinRSModifying track layout from straight to circular has a modest effect on the 6-min walk distanceChest200813351155116018263673
- EiserNWillsherDDoreCJReliability, repeatability and sensitivity to change of externally and self-paced walking tests in COPD patientsRespir Med200397440741412693802
- JenkinsSCecinsNMSix-minute walk test in pulmonary rehabilitation: do all patients need a practice test?Respirology20101581192119620920121
- StevensDElpernESharmaKSzidonPAnkinMKestenSComparison of hallway and treadmill six-minute walk testsAm J Respir Crit Care Med19991605 Pt 11540154310556117
- VagagginiBTaccolaMSeverinoSShuttle walking test and 6-minute walking test induce a similar cardiorespiratory performance in patients recovering from an acute exacerbation of chronic obstructive pulmonary diseaseRespiration200370657958414732787
- O’ReillyJFShaylorJMFromingsKMHarrisonBDThe use of the 12 minute walking test in assessing the effect of oral steroid therapy in patients with chronic airways obstructionBr J Dis Chest19827643743826758833
- McKeoughZJLeungRWAlisonJAShuttle walk tests as outcome measures: Are two incremental shuttle walk tests and two endurance shuttle walk tests necessary?Am J Phys Med Rehabil2011901353920975522
- RevillSMWilliamsJSewellLCollierRSinghSJWithin-day repeatability of the endurance shuttle walk testPhysiotherapy200995214014319627696
- BrownSEFischerCEStansburyDWLightRWReproducibility of VO2max in patients with chronic air-flow obstructionAm Rev Respir Dis198513134354383977183
- BehnkeMWewelARKirstenDJorresRAMagnussenHExercise training raises daily activity stronger than predicted from exercise capacity in patients with COPDRespir Med200599671171715878487
- BrooksDSolwaySWeinachtKWangDThomasSComparison between an indoor and an outdoor 6-minute walk test among individuals with chronic obstructive pulmonary diseaseArch Phys Med Rehabil200384687387612808541
- ChatterjeeABRissmillerRWMeadeKReproducibility of the 6-minute walk test for ambulatory oxygen prescriptionRespiration201079212112719468196
- KozuRJenkinsSSenjyuHMukaeHSakamotoNKohnoSPeak power estimated from 6-minute walk distance in Asian patients with idiopathic pulmonary fibrosis and chronic obstructive pulmonary diseaseRespirology201015470671320409022
- PoulainMDurandFPalombaB6-minute walk testing is more sensitive than maximal incremental cycle testing for detecting oxygen desaturation in patients with COPDChest200312351401140712740254
- RejeskiWJFoleyKOWoodardCMZaccaroDJBerryMJEvaluating and understanding performance testing in COPD patientsJ Cardiopulm Rehabil2000202798810763155
- RoomiJJohnsonMMWatersKYohannesAHelmAConnollyMJRespiratory rehabilitation, exercise capacity and quality of life in chronic airways disease in old ageAge Ageing199625112168670523
- SciurbaFCrinerGJLeeSMSix-minute walk distance in chronic obstructive pulmonary disease: reproducibility and effect of walking course layout and lengthAm J Respir Crit Care Med2003167111522152712615634
- SpencerLMAlisonJAMcKeoughZJSix-minute walk test as an outcome measure: are two six-minute walk tests necessary immediately after pulmonary rehabilitation and at three-month follow-up?Am J Phys Med Rehabil200887322422817912139
- TroostersTVilaroJRabinovichRPhysiological responses to the 6-min walk test in patients with chronic obstructive pulmonary diseaseEur Respir J200220356456912358329
- ArnardóttirRHSorensenSRingqvistILarssonKNo increase in walking distance on repeated tests in COPD patients with exercise-induced hypoxaemiaAdv Physiother200794161168
- BeaumontACockcroftAGuzAA self paced treadmill walking test for breathless patientsThorax19854064594644024007
- BergerRSmithDEffect on inhaled metaproterenol on exercise performance in patients with stable ‘fixed’ airway obstructionAm Rev Respir Dis198813836246293202416
- McGavinCRGuptaSPMcHardyGJTwelve minute walking test for assessing disability in chronic bronchitisBMJ1976160138228231260350
- MungallIPHainsworthRAssessment of respiratory function in patients with chronic obstructive airways diseaseThorax1979342254258483195
- SwinburnCRWakefieldJMJonesPWPerformance, ventilation, and oxygen consumption in three different types of exercise test in patients with chronic obstructive lung diseaseThorax19854085815864035628
- CampoLAChilingaryanGBergKParadisBMazerBValidity and reliability of the modified shuttle walk test in patients with chronic obstructive pulmonary diseaseArch Phys Med Rehabil200687791892216813778
- PerraultHBarilJHenophySRycroftABourbeauJMaltaisFPaced-walk and step tests to assess exertional dyspnea in COPDCOPD20096533033919863362
- ArnardóttirRHEmtnerMHedenstromHLarssonKBomanGPeak exercise capacity estimated from incremental shuttle walking test in patients with COPD: a methodological studyRespir Res20067127
- SinghSJMorganMDScottSWaltersDHardmanAEDevelopment of a shuttle walking test of disability in patients with chronic airways obstructionThorax19924712101910241494764
- RevillSMNoorMZButcherGWardMJThe endurance shuttle walk test: An alternative to the six-minute walk test for the assessment of ambulatory oxygenChron Respir Dis20107423924521084548
- RevillSMMorganMDSinghSJWilliamsJHardmanAEThe endurance shuttle walk: a new field test for the assessment of endurance capacity in chronic obstructive pulmonary diseaseThorax199954321322210325896
- CoveyMKLarsonJLAlexCGWirtzSLangbeinWETest-retest reliability of symptom-limited cycle ergometer tests in patients with chronic obstructive pulmonary diseaseNurs Res199948191910029397
- CoxNJHendriksJCBinkhorstRAFolgeringHTvan HerwaardenCLReproducibility of incremental maximal cycle ergometer tests in patients with mild to moderate obstructive lung diseasesLung198916721291332494393
- MathurRSRevillSMVaraDDWaltonRMorganMDComparison of peak oxygen consumption during cycle and treadmill exercise in severe chronic obstructive pulmonary diseaseThorax19955088298337570432
- van’t HulAGosselinkRKwakkelGConstant-load cycle endurance performance test-retest reliability and validity in patients with COPDJ Cardiopulm Rehabil200323214315012668937
- CooperCBAbrazadoMLeggDKestenSDevelopment and implementation of treadmill exercise testing protocols in COPDInt J Chron Obstruct Pulmon Dis2010537538521103404
- Borghi-SilvaAArenaRCastelloVAerobic exercise training improves autonomic nervous control in patients with COPDRespir Med2009103101503151019464865
- Borghi-SilvaABaldisseraVSampaioLML-carnitine as an ergogenic aid for patients with chronic obstructive pulmonary disease submitted to whole-body and respiratory muscle training programsBraz J Med Biol Res200639446547416612469
- CooperCBDesensitization to dyspnea in COPD with specificity for exercise training modeInt J Chron Obstruct Pulmon Dis20094334319436684
- ArnardóttirRHBomanGLarssonKHedenströmHEmtnerMInterval training compared with continuous training in patients with COPDRespir Med200710161196120417188853
- Carrieri-KohlmanVGormleyJMDouglasMKPaulSMStulbargMSExercise training decreases dyspnea and the distress and anxiety associated with it. Monitoring alone may be as effective as coachingChest19961106152615358989072
- CortopassiFCastroAAPortoEFComprehensive exercise training improves ventilatory muscle function and reduces dyspnea perception in patients with COPDMonaldi Arch Chest Dis200971310611219999956
- EatonTYoungPNicolKKolbeJThe endurance shuttle walking test: A responsive measure in pulmonary rehabilitation for COPD patientsChron Respir Dis2006313916509172
- GreeningNJEvansRAWilliamsJEGreenRHSinghSJSteinerMCDoes body mass index influence the outcomes of a waking-based pulmonary rehabilitation programme in COPD?Chron Respir Dis2012929910622414784
- NgaageDLHasneyKCowenMEThe functional impact of an individ-ualized, graded, outpatient pulmonary rehabilitation in end-stage chronic obstructive pulmonary diseaseHeart Lung200433638138915597292
- O’FarrellRGargoumFO’ConnorBComparison of incremental and endurance shuttle walk testing after pulmonary rehabilitationAm J Resp Crit Care Med2011183 AbsA2024
- OngKCChongWFSohCEarnestAComparison of different exercise tests in assessing outcomes of pulmonary rehabilitationRespir Care200449121498150315571640
- RiesALMakeBJLeeSMThe effects of pulmonary rehabilitation in the National Emphysema Treatment TrialChest200512863799380916354848
- Van HelvoortHADe BoerRCVan De BroekLDekhuijzenRHeijdraYFExercises commonly used in rehabilitation of patients with chronic obstructive pulmonary disease: cardiopulmonary responses and effect over timeArch Phys Med Rehabil201192111111721092932
- Van RanstDOttenHMeijerJWvan’t HulAJOutcome of pulmonary rehabilitation in COPD patients with severely impaired health statusInt J Chron Obstruct Pulmon Dis20116164765722162650
- CazzolaMBiscioneGLPasquaFUse of 6-min and 12-min walking test for assessing the efficacy of formoterol in COPDRespir Med2008102101425143018621519
- OgaTNishimuraKTsukinoMHajiroTIkedaAIzumiTThe effects of oxitropium bromide on exercise performance in patients with stable chronic obstructive pulmonary disease: a comparison of three different exercise testsAm J Respir Crit Care Med200016161897190110852763
- PepinVSaeyDWhittomFLeBlancPMaltaisFWalking versus cycling: sensitivity to bronchodilation in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2005172121517152216166613
- ZhangXWatermanLAWardJBairdJCMahlerDAAdvantages of endurance treadmill walking compared with cycling to assess bron-chodilator therapyChest201013761354136120040610
- LedererDJThomashowBMGinsburgMELung-volume reduction surgery for pulmonary emphysema: Improvement in body mass index, airflow obstruction, dyspnea, and exercise capacity index after 1 yearJ Thorac Cardiovasc Surg200713361434143817532935
- PepinVLavioletteLBrouillardCSignificance of changes in endurance shuttle walking performanceThorax201166211512021148135
- CrisafulliELorenziMCGherardiniGTest del cammino dei 6 minuti in pazienti con bronchopneupatia cronica ostruttiva: confronto cone senza incoraggiamento [Six-minute walk test in patients with chronic obstructive pulmonary disease: comparison with and without active coaching]Rassegna di Patologia dell’Apparato Respiratorio2007223186192
- BenzoRPParameshSPatelSASlivkaWASciurbaFCOptimal protocol selection for cardiopulmonary exercise testing in severe COPDChest200713251500150517925427
- Borghi-SilvaAMendesRGToledoACAdjuncts to physical training of patients with severe COPD: oxygen or noninvasive ventilation?Respir Care201055788589420587101
- CasasAVilaroJRabinovichREncouraged 6-min walking test indicates maximum sustainable exercise in COPD patientsChest20051281556116002916
- DavidsonACLeachRGeorgeRJGeddesDMSupplemental oxygen and exercise ability in chronic obstructive airways diseaseThorax198843129659713238640
- de AlmeidaFGVictorEGRizzoJAHallway versus treadmill 6-minute-walk tests in patients with chronic obstructive pulmonary diseaseRespir Care200954121712171619961638
- DeanNCBrownJKHimelmanRBDohertyJJGoldWMStulbargMSOxygen may improve dyspnea and endurance in patients with chronic obstructive pulmonary disease and only mild hypoxemiaAm Rev Respir Dis199214649419451416422
- HoneymanPBarrPStubbingDGEffect of a walking aid on disability, oxygenation, and breathlessness in patients with chronic airflow limitationJ Cardiopulm Rehabil199616163678907444
- HsiaDCasaburiRPradhanATorresEPorszaszJPhysiological responses to linear treadmill and cycle ergometer exercise in COPDEur Resp J2009343605615
- MiyaharaNEdaRTakeyamaHCardiorespiratory responses during cycle ergometer exercise with different ramp slope increments in patients with chronic obstructive pulmonary diseaseIntern Med2000391151910674842
- OzalevliSOzdenAGocenZCimrinAHComparison of six-minute walking tests conducted with and without supplemental oxygen in patients with chronic obstructive pulmonary disease and exercise-induced oxygen desaturationAnn Saudi Med20072729410017356317
- RosaFWCamelierAMayerAJardimJREvaluating physical capacity in patients with chronic obstructive pulmonary disease: Comparing the shuttle walk test with the encouraged 6-minute walk testJ Bras Pneumol200632210611317273579
- SandlandCJMorganMDSinghSJDetecting oxygen desaturation in patients with COPD: Incremental versus endurance shuttle walkingRespir Med200810281148115218571914
- SwertsPMMostertRWoutersEFComparison of corridor and treadmill walking in patients with severe chronic obstructive pulmonary diseasePhys Ther19907074394422356220
- MorganMDSinghSJAssessing the exercise response to a bronchodilator in COPD: time to get off your bike?Thorax200762428128317387209