
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory condition, and progresses with acute exacerbations. (AE). During AE, levels of acute phase reactants such as C-reactive protein (CRP) and inflammatory cells in the circulation increase. Soluble urokinase-type plasminogen activator receptor (suPAR) levels increase in acute viral and bacterial infections and in diseases involving chronic inflammation. The purpose of this study was to investigate the effectiveness of suPAR in predicting diagnosis of AE of COPD (AE-COPD) and response to treatment.
Methods
The study population consisted of 43 patients diagnosed with AE-COPD and 30 healthy controls. suPAR, CRP, and fibrinogen levels were measured on the first day of hospitalization and on the seventh day of treatment.
Results
We found that fibrinogen (P<0.001), CRP (P<0.001), and suPAR (P<0.001) were significantly higher in patients with AE-COPD than in healthy controls. Fibrinogen (P<0.001), CRP (P=0.001), and suPAR (P<0.001) were significantly decreased by the seventh day of treatment. However, the area under receiver operator characteristic curve showed that suPAR is superior to CRP and fibrinogen in distinguishing AE-COPD. There was a correlation between fibrinogen, CRP, and suPAR. However, only fibrinogen was a powerful predictor of suPAR in multiple linear regression. In multiple logistic regression, only suPAR and fibrinogen were strong predictors of AE-COPD (P=0.002 and P=0.014, respectively). Serum suPAR was negatively correlated with forced expiratory volume in 1 second (r=−478, P=0.001).
Conclusion
suPAR is a marker of acute inflammation. It is well correlated with such inflammation markers as CRP and fibrinogen. suPAR can be used as a predictor of AE-COPD and in monitoring response to treatment.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by recurrent episodes of exacerbations defined by an acute worsening in the severity of a patient’s symptoms, including baseline dyspnea and coughing, that warrants a change in medication or medical intervention.Citation1 Exacerbations have been linked to disease-associated morbidity and mortality, placing significant strain on medical facilities, increasing resource burden, and driving up ongoing health care costs.Citation2
The importance of exacerbation prediction has recently been recognized in the application of effective and aggressive prevention strategies.Citation1 While major advances have been made in the past decade, measurable prognostic factors predicting exacerbation risk in COPD patients remain undefined, which is partly due to controversies in the definition of acute exacerbation of COPD (AE-COPD):Citation3 whether the definition depends solely on symptoms or health care usage, diagnostic criteria remain subjective. This generates difficulty in objectively differentiating exacerbations from day-to day variations. Therefore, a “biomarker” is needed that can yield an objective verification of exacerbations. In addition, a good biomarker may not only indicate the exacerbations, but may also predict the severity of exacerbations.Citation4
Urokinase-type plasminogen activator receptor (uPAR) is expressed on various cell types, and the complex interaction with its ligand urokinase plasminogen activator (uPA) has been shown to promote tissue invasion in malignant diseases by converting plasminogen into plasmin, resulting in degradation of the extracellular matrix.Citation5,Citation6 Migration of inflammatory cells from the bloodstream into tissues is an essential component of inflammation and the immune response against infection in which the uPAR/uPA system is directly involved.Citation7 During inflammatory stimulation, uPAR is cleaved from the cell surface by proteases to create the soluble form of the receptor, suPAR, which can be detected in blood, urine, and cerebrospinal fluid.Citation8 High suPAR levels were shown to be associated with an undesirable outcome in HIV infection,Citation9 active pulmonary tuberculosis,Citation10 bacterial meningitis,Citation8 and pneumococcal bacteremia,Citation11 suggesting that it may be a good biomarker of inflammation.Citation12
In recent years, there have been some studies investigating the potential role of biomarkers during the inflammatory process of chronic diseases.Citation13,Citation14 However, to our knowledge, the effectiveness of the inflammation marker, suPAR, in predicting AE-COPD and in response to treatment has not been investigated so far. We hypothesized that serum suPAR would be increased in patients with AE-COPD, and that it would be decreased by treatment. The study also examined how serum suPAR levels changed with degree of airflow obstruction and with serum level of fibrinogen and CRP.
Materials and methods
Study population
In this cross-sectional study, consecutive patients with AE-COPD were prospectively recruited at Recep Tayyip Erdogan University Hospital, Rize, Turkey between January 2013 and April 2014. The disease control group comprised subjects (both nonsmokers and smokers) who had no history of pulmonary disease.
Study design
The primary objective of the study was to test the hypothesis that suPAR is a blood biomarker, the level of which rises during AE-COPD and decreases with 7 days of treatment. The secondary objective of the study was to show a relationship between suPAR and other putative biomarkers: CRP and fibrinogen.
Smoking status, history of cardiovascular and respiratory disease, diabetes mellitus, and use of medications were documented with help of a questionnaire. Patients with AE-COPD were treated for 7 days and reevaluated to observe the changes in suPAR levels in response to treatment.
Exclusion criteria
Patients who had conditions that could potentially affect circulating suPAR levels were excluded. Accordingly, patients previously diagnosed with bronchial asthma, bronchiectasis, cystic fibrosis, upper airway obstruction, or bronchiolitis related to systemic pathology; patients requiring monitoring in the intensive care unit due to exacerbation; and patients with active cancer, cirrhosis of the liver, acute or chronic kidney failure, heart failure, uncontrolled hypertension, and uncontrolled diabetes mellitus were excluded.Citation12
Diagnosis of COPD
A diagnosis of COPD was made according to the criteria of GOLD, as follows: the diagnosis of COPD was based on current or past smoking history (>20 pack-years), clinical evaluation, and pulmonary function testing showing airflow obstruction (forced expiratory volume in 1 second [FEV1]/forced vital capacity ratio of <0.7) with a change in FEV1 of less than 200 mL and 12% in the bronchodilator test.Citation15
Definition of AE-COPD
Acute exacerbation was defined as prolonged (≥48 hours) worsening of dyspnea sensation, coughing, or sputum production that can become purulent leading to an increase in the use of maintenance medications and/or supplementation with additional medications.Citation16
Pulmonary function tests
Pulmonary function tests were performed at least three times with a ZAN system (ZAN100; ZAN Gerätetechnik GmbH, Oberthulba, Germany) to all COPD patients when the patients were in a stable period. Staging of airflow limitation was made according to GOLD guidelines (GOLD stage I [FEV1 ≥80%], stage II [50%≤ FEV1 <80%], stage III [30%≤ FEV1 <50%], and stage IV [FEV1 <30%]).Citation15
Serum suPAR measurement
Blood samples were collected upon admission to the hospital (prior to therapeutic interventions) as well as in the morning of day 7 after admission. After centrifugation at 2,000 × g at 4°C for 10 minutes, serum and plasma aliquots of 1 mL were frozen immediately at −80°C.
Serum levels of suPAR were measured quantitatively using the enzyme-linked immunosorbent assay with the commercially available suPARnostic kit®, according to the manufacturer’s instructions (ViroGates, Copenhagen, Denmark). The technicians who measured the samples were blinded to the identity of the patient samples.
Ethical concerns
All participants provided written informed consent. The study was approved by the local ethical committee (number =2012/134) and conducted in accordance with the Declaration of Helsinki.
Statistical analysis
Results for normally distributed continuous variables are expressed as the mean value ± standard deviation, and continuous variables with nonnormal distribution are presented as median values and interquartile range. Analyses of normality in the continuous variables were performed using the Shapiro–Wilk test, histograms, and Q–Q plots. Categorical variables were expressed as numbers and percentage. The chi-square test was used to compare proportions in different groups. Student’s t-test or Mann–Whitney U-test was used to compare the two independent groups according to distribution state. If tests of normality were met, one-way analysis of variance was used to compare more than two groups; the cutoff level of α error was reduced to 0.005/(number of tests) (Bonferroni correction), and the Kruskal–Wallis test was used when tests of normality failed. In cases where the Kruskal–Wallis test yielded a statistical significance, post hoc analysis was performed to identify the groups which showed differences by Bonferroni-corrected Mann–Whitney U-test.
Correlations between levels of circulating suPAR and CRP were determined by Pearson correlation. These two parameters were logarithmically transformed because they were not normally distributed.
Univariate associations between continuous baseline characteristics and the presence of AE-COPD were assessed with logistic regression analysis. The Wald test was used to obtain logistic regression analysis parameters. In all multivariate models, backward stepwise selection was used to derive the final model, and significance levels of 0.05 and 0.1 were chosen to include and exclude terms, respectively. Variables that correlated significantly with suPAR levels in univariate analysis (Pearson correlation) were included in a backward stepwise multiple linear regression analysis. In these models, we forced in age, sex, body mass index (BMI), arterial partial pressure of oxygen, inhaled steroid use, pack-years of smoking, hypertension, and platelet count as covariates to adjust for their potential effects on suPAR.
The area under the curve, receiver operating characteristics (ROCs) for each marker were analyzed, to differentiate AE-COPD from the same patient group in whom specific exacerbation treatment was given for 7 days. All statistical analyses were performed with SPSS software (version 21.0; IBM Corporation, Armonk, NY, USA). A two-sided probability value less than 0.05 was considered statistically significant.
Results
This prospective study recruited 43 patients (aged 68±8 years; 37 male; 27.4±4.6 kg/m2) diagnosed with AE-COPD who were age-, sex-, and BMI-matched with 30 healthy controls. Patients with AE-COPD (n=43) were treated for 7 days and reassessed as a newly paired group of patients with AE-COPD.
There were no differences between the COPD and the healthy control groups in relation to smoking history. Most of the patients with AE-COPD had severe airflow obstruction; 81% of the patients had FEV1 <50% predicted. There were no mild COPD cases in the study population. This was not a planned outcome. The characteristics and laboratory findings of participants in the groups and pulmonary function tests of the COPD group are outlined in .
Table 1 Characteristics, laboratory findings, and pulmonary function tests of study groups
There were no intergroup differences with respect to high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides, and fasting concentrations of glucose, or to the use of lipid-lowering medications (data not shown).
Serum suPAR in the study groups
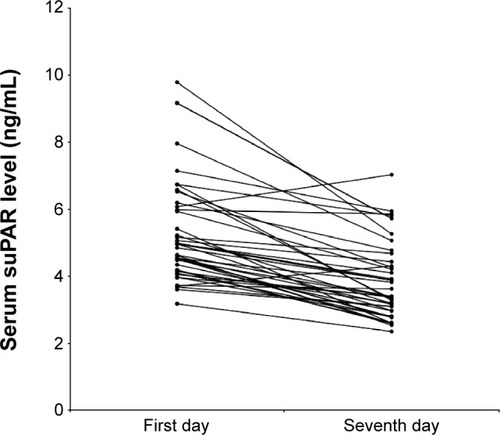
Median plasma suPAR in patients with AE-COPD (4.84±1.90 ng/mL) was significantly higher than in healthy controls (2.36±0.89 ng/mL; P<0.001) (). Serum suPAR levels measured on the first and seventh days were compared to evaluate the response to treatment in patients with AE-COPD. A significant decrease in median suPAR level was observed after treatment, from 4.84±1.90 ng/mL to 3.38±1.34 ng/mL (P<0.001) as shown in .
Figure 1 Serum soluble urokinase-type plasminogen activator receptor (suPAR) in healthy controls and in patients with acute exacerbation of chronic obstructive pulmonary disease (AE-COPD) on the first and seventh days.
Notes: Data are expressed as boxplots, in which the horizontal lines illustrate the 25th, 50th, and 75th percentiles of the values of suPAR. The vertical lines represent the 5th and 95th percentiles.
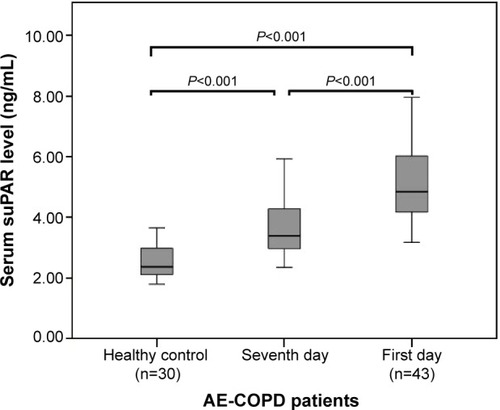
Figure 2 Serum soluble urokinase-type plasminogen activator receptor (suPAR) during an acute exacerbation and on the seventh day of treatment.
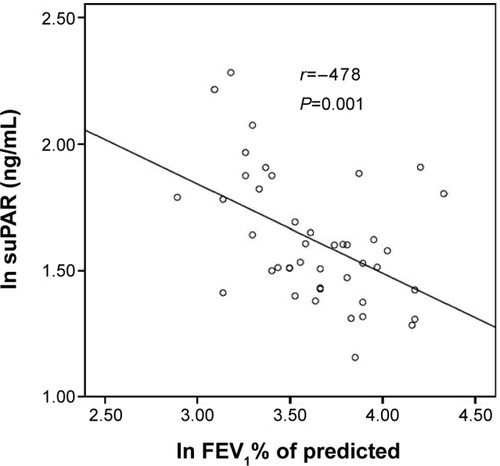
There was a significant inverse correlation between plasma suPAR levels and post-bronchodilator FEV1 (% predicted) (r=−0.478, P=0.001) as shown in . shows suPAR data at admission and FEV1 data at the stable period of patients with AE-COPD.
Figure 3 Serum suPAR and FEV1 % of predicted in patients with acute exacerbation of chronic obstructive pulmonary disease.
Abbreviations: FEV1, forced expiratory volume in 1 second; ln, natural log-transformed; suPAR, soluble urokinase-type plasminogen activator receptor.
Putative inflammatory markers in the study groups
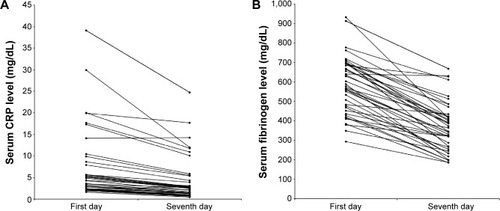
Median serum fibrinogen (4.25±6.26 mg/dL) and CRP (577±226 mg/dL) were significantly higher in patients with AE-COPD on the first day than in healthy control subjects (0.74±1.96 mg/dL; P<0.001 and 240±128 mg/dL; P<0.001, respectively) as shown in .
Figure 4 C-reactive protein (CRP) (A) and fibrinogen (B) in healthy subjects and patients with acute exacerbation of chronic obstructive pulmonary disease (AE-COPD) on the first and the seventh day.
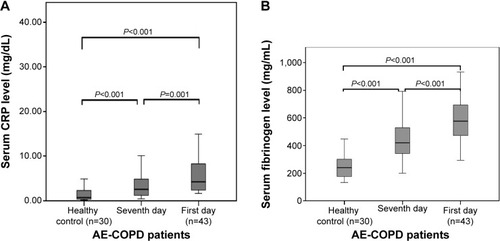
Plasma concentrations of CRP and fibrinogen levels were decreased to 2.54±4.18 mg/dL (P<0.001) and 420±190 mg/dL (P<0.001), respectively, with 7 days of treatment. CRP and fibrinogen levels on the first day and the seventh day are shown in .
Figure 5 Serum C-reactive protein (CRP) (A) and fibrinogen (B) during an acute exacerbation and on the seventh day of the treatment.
Variables associated with serum suPAR
For patients with AE-COPD on the first day, positive correlations were found between suPAR and CRP and fibrinogen (). Stepwise multiple regression analysis adjusting for confounding factors (age, sex, BMI, arterial partial pressure of oxygen, arterial partial pressure of carbon dioxide, pH, pack-years of smoking, smoking status, inhaled corticosteroid therapy) revealed that only fibrinogen was a strong independent predictor (P<0.001) of suPAR, explaining 58% of the total variability of circulating levels of suPAR in AE-COPD on the first day. For patients with AE-COPD on the seventh day, concentrations of suPAR also correlated positively with CRP and fibrinogen (). In stepwise multiple regression analysis, only fibrinogen was an independent predictor of suPAR (P=0.019); however, it explained only 24% of circulating levels of suPAR.
Table 2 Pearson correlation coefficients of suPAR with inflammatory markers in patients with AE-COPD on the first and seventh day
Distinguishing power of all inflammatory markers in patients with AE-COPD on the first day from the seventh day by ROC curve and logistic regression analysis
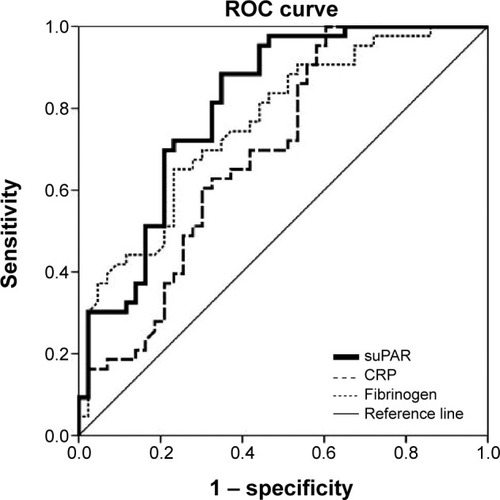
In ROC analysis, the area under the curve was 0.807 (95% confidence interval [CI]: 0.715–0.900, P<0.001) for suPAR, 0.695 (95% CI: 0.583–0.807, P=0.002) for CRP, and 0.763 (95% CI: 0.663–0.862, P<0.001) for fibrinogen in distinguishing patients with AE-COPD on the first day from the seventh day, indicating that suPAR was superior to CRP and fibrinogen as a predictive factor in patients with AE-COPD on the first day ().
Figure 6 ROC curve for suPAR, CRP, and fibrinogen in discrimination of patients with acute exacerbation of chronic obstructive pulmonary disease on the first and seventh day.
Multiple logistic regression analysis was run to predict AE-COPD from suPAR, fibrinogen, and CRP. Only suPAR and fibrinogen were strong predictors of AE-COPD (P=0.002 and P=0.014, respectively) ().
Table 3 Univariate and multivariate logistic regression analysis of inflammatory markers in patients with acute exacerbation of chronic obstructive pulmonary disease as the dependent variable
Discussion
The present study uncovered the following novel findings: serum suPAR levels were significantly higher in patients with AE-COPD than in healthy controls. High serum suPAR levels were decreased with 7 days of treatment. Serum suPAR remained an independent predictor of AE-COPD after multivariate adjustment. Furthermore, serum suPAR levels exhibited a positive strong correlation with the inflammatory markers CRP and fibrinogen. These findings indicate that circulating suPAR levels promise to be a useful biomarker with which to distinguish AE-COPD and can be used to evaluate treatment response in patients with AE-COPD.
AE-COPD is a significant cause of mortality and morbidity. Therefore, diagnosis and prevention of these episodes is one of the major goals in the management of COPD. Currently, the diagnosis of an exacerbation relies exclusively on the clinical presentation of the patient complaining of an acute change of symptoms that is beyond normal day-to-day variation.Citation17 Identification of a biomarker that has the predictive potential of identifying a forthcoming exacerbation would therefore be highly valuable. Biomarkers such as CRP and fibrinogen represent low-grade systemic inflammation, and increased levels have been found in patients with AE-COPD.Citation18–Citation20 However, no clear biological markers have been identified so far.Citation2
In contrast to many inflammatory markers, suPAR can potentially be a robust and independent biomarker of inflammation because suPAR is a very stable molecule and its serum concentrations are not affected by circadian changes.Citation21 It was also shown that treatment of infectious diseases and cancer resulted in a decrease in serum concentrations of suPAR; furthermore, suPAR levels were normalized after full recovery.Citation10,Citation22 To verify whether suPAR is a potential biomarker of AE-COPD, we recruited the patients with AE-COPD, and suPAR levels were measured upon admission of patients and 7 days thereafter. Our study showed that there was a significant decrease in serum suPAR levels measured on the seventh day of treatment compared to those on the first day and suPAR levels in COPD patients were higher than in the healthy controls, suggesting that suPAR might have a role as a distinguishing biomarker of AE-COPD and can be used in the assessment of treatment response.
Cross-sectional studies showed that systemic inflammatory markers are inversely related to lung function.Citation1,Citation23,Citation24 Our study, consistent with previous studies, showed that serum suPAR levels were inversely associated with the degree of airflow obstruction as measured by post-bronchodilator FEV1 (% predicted). This finding also potentiates suPAR as an inflammatory marker.
We also measured two other putative inflammatory markers, even though serum suPAR was the main objective of this study. Indeed, CRP and fibrinogen levels were found to be significantly raised in COPD subjects compared to control subjects in previous studies.Citation2,Citation25–Citation27 Data from the 1,793 individuals from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) cohort found elevated levels of CRP and fibrinogen count to be associated with the occurrence of exacerbations in the first year of follow-up.Citation1,Citation4 Increased CRP and fibrinogen have also been associated with increased risk for COPD hospitalizations.Citation3,Citation28,Citation29 Our study showed that fibrinogen and CRP were increased in AE-COPD patients relative to healthy subjects; this finding is consistent with former studies. Our study also showed a decrease in CRP and fibrinogen levels with 7 days of treatment in patients with AE-COPD. However, the area under the ROC curve analysis showed that suPAR was superior to CRP and fibrinogen in identifying patients with AE-COPD on the first day from the seventh day. In the present study, serum suPAR levels exhibited a positive correlation with CRP and fibrinogen levels at admission of patients with AE-COPD, which is consistent with previous findings.Citation4,Citation30 This correlation was also maintained in parallel with reduction after 7 days of treatment. Furthermore, multilinear regression analysis revealed that only fibrinogen was a strong independent predictor of suPAR, explaining 58% of the total variability of circulating levels of suPAR. All those previous studies and our findings are powerful support for the idea that suPAR is a marker of acute inflammation and can be used in treatment response.
Limitations
There were some limitations in this study. First, this was a retrospective study and was subject to bias. Second, we used a cross-sectional design for this study, which is not the best design for investigating any causal relationships. Although we performed adjustment for significant clinical variables, there remains the possibility of residual confounding from unmeasured variables. Third, our study was not designed to elucidate the mechanistic pathways that lead to higher suPAR ratio in patients with COPD. Further studies should focus on providing a more complete understanding of the biochemical properties and regulatory mechanisms of suPAR in this patient population to be able to better evaluate changes in response to exacerbation-specific therapies. Despite the limitations of the study, we observed that individuals with AE-COPD are significantly more likely to have higher levels of suPAR, which seems a reasonable measure with which to detect exacerbations.
Conclusion
This study showed that serum suPAR was increased in patients with AE-COPD and decreased after 7 days of treatment. This study indicates that elevated suPAR levels have potential value as a robust and independent biomarker of exacerbation in COPD and can be used in response to treatment. Prospective long-term studies are necessary to show whether suPAR levels increase further with disease progression and whether suPAR has a capacity to show comorbidities and mortality in COPD.
Acknowledgments
The study was performed at Recep Tayyip Erdogan University Hospital, Rize, Turkey. The study was approved by the local ethical committee of Recep Tayyip Erdogan University. (number =2012/134).
Disclosure
This is not an industry-supported study. The authors report no conflicts of interest in this work.
References
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med201318734736522878278
- DecramerMJanssensWMiravitllesMChronic obstructive pulmonary diseaseLancet20123791341135122314182
- Rodriguez-RoisinRToward a consensus definition for COPD exacerbationsChest2000117398S401S10843984
- HurstJRVestboJAnzuetoAEvaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) InvestigatorsSusceptibility to exacerbation in chronic obstructive pulmonary diseaseN Engl J Med20103631128113820843247
- OstergaardCBenfieldTLundgrenJDEugen-OlsenJSoluble urokinase receptor is elevated in cerebrospinal fluid from patients with purulent meningitis and is associated with fatal outcomeScand J Infect Dis200436141915000553
- MadsenCDSideniusNThe interaction between urokinase receptor and vitronectin in cell adhesion and signallingEur J Cell Biol20088761762918353489
- PortelliMASiedlinskiMStewartCEGenome-wide protein QTL mapping identifies human plasma kallikrein as a post-translational regulator of serum uPAR levelsFASEB J20142892393424249636
- ThunøMMachoBEugen-OlsenJsuPAR: the molecular crystal ballDis Markers20092715717219893210
- LawnSDMyerLBanganiNVogtMWoodRPlasma levels of soluble urokinase-type plasminogen activator receptor (suPAR) and early mortality risk among patients enrolling for antiretroviral treatment in South AfricaBMC Infect Dis200774117509133
- Eugen-OlsenJGustafsonPSideniusNThe serum level of soluble urokinase receptor is elevated in tuberculosis patients and predicts mortality during treatment: a community study from Guinea-BissauInt J Tuberc Lung Dis2002668669212150480
- WittenhagenPKronborgGWeisNThe plasma level of soluble urokinase receptor is elevated in patients with Streptococcus pneumoniae bacteraemia and predicts mortalityClin Microbiol Infect20041040941515113317
- Eugen-OlsenJAndersenOLinnebergACirculating soluble urokinase plasminogen activator receptor predicts cancer, cardiovascular disease, diabetes and mortality in the general populationJ Intern Med201026829630820561148
- BozinovskiSHutchinsonAThompsonMSerum amyloid a is a biomarker of acute exacerbations of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200817726927818006888
- SmithDJYerkovichSTTowersMACarrollMLThomasRUphamJWReduced soluble receptor for advanced glycation end-products in COPDEur Respir J20113751652220595148
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: Updated 2014Global Initiative for Chronic Obstructive Lung Disease2014 Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jun11.pdfAccessed July 30, 2014
- HalpinDMDecramerMCelliBKestenSLiuDTashkinDPExacerbation frequency and course of COPDInt J Chron Obstruct Pulmon Dis2012765366123055714
- TufvessonEEkbergMBjermerLInflammatory biomarkers in sputum predict COPD exacerbationsLung201319141341623689877
- MiniatiMMontiSBottaiMCocciFFornaiELubranoVPrognostic value of C-reactive protein in chronic obstructive pulmonary diseaseIntern Emerg Med2011642343021249472
- ThomsenMDahlMLangePVestboJNordestgaardBGInflammatory biomarkers and comorbidities in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med201218698298822983959
- MobergMVestboJMartinezGLangePRingbaekTPrognostic value of C-reactive protein, leukocytes, and vitamin d in severe chronic obstructive pulmonary diseaseScientific World Journal2014201414073624587707
- KofoedKSchneiderUVScheelTAndersenOEugen-OlsenJDevelopment and validation of a multiplex add-on assay for sepsis biomarkers using xMAP technologyClin Chem2006521284129316690735
- OstrowskiSRUllumHGokaBQPlasma concentrations of soluble urokinase-type plasminogen activator receptor are increased in patients with malaria and are associated with a poor clinical or a fatal outcomeJ Infect Dis20051911331134115776381
- DahlMTybjaerg-HansenAVestboJLangePNordestgaardBGElevated plasma fibrinogen associated with reduced pulmonary function and increased risk of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20011641008101111587987
- ThorleifssonSJMargretardottirOBGudmundssonGChronic airflow obstruction and markers of systemic inflammation: results from the BOLD study in IcelandRespir Med20091031548155319427181
- Pinto-PlataVMMüllerovaHTosoJFC-reactive protein in patients with COPD, control smokers and non-smokersThorax200661232816143583
- WedzichaJASeemungalTAMacCallumPKAcute exacerbations of chronic obstructive pulmonary disease are accompanied by elevations of plasma fibrinogen and serum IL-6 levelsThromb Haemost20008421021510959691
- Garcia-RioFMiravitllesMSorianoJBEPI-SCAN Steering CommitteeSystemic inflammation in chronic obstructive pulmonary disease: a population-based studyRespir Res2010116320500811
- DahlMVestboJLangePBojesenSETybjaerg-HansenANordestgaardBGC-reactive protein as a predictor of prognosis in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200717525025517053205
- EngströmGSegelstormNEkberg-AronssonMNilssonPMLindgärdeFLöfdahlCGPlasma markers of inflammation and incidence of hospitalisations for COPD: results from a population-based cohort studyThorax20096421121518988660
- DonadelloKScollettaSTacconeFSSoluble urokinase-type plasminogen activator receptor as a prognostic biomarker in critically ill patientsJ Crit Care20142914414924120089