
Abstract
Purpose
Most guidelines recommend pulmonary rehabilitation (PR) for patients with chronic obstructive pulmonary disease (COPD) and modified Medical Research Council dyspnea scale (mMRC) levels ≥2, but the effectiveness of PR in patients with less advanced disease is not well established. Our aim was to investigate the effects of PR in patients with COPD and mMRC ≤1.
Methods
The methodology was developed as a part of evidence-based guideline development and is in accordance with the principles of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group. We identified randomized controlled trials (RCTs) through a systematic, multidatabase literature search and selected RCTs comparing the effects of PR with usual care in patients with COPD and mMRC ≤1. Predefined critical outcomes were health-related quality of life (HRQoL), adverse effects and mortality, while walking distance, maximal exercise capacity, muscle strength, and dropouts were important outcomes. Two authors independently extracted data, assessed trial eligibility and risk of bias, and graded the evidence. Meta-analyses were performed when deemed feasible.
Results
Four RCTs (489 participants) were included. On the basis of moderate-quality evidence, we found a clinically and statistically significant improvement in short-term HRQoL of 4.2 units (95% confidence interval [CI]: [−4.51 to −3.89]) on St George’s Respiratory Questionnaire, but not at the longest follow-up. We also found a statistically significant improvement of 25.71 m (95% CI: [15.76–35.65]) in the 6-minute walk test with PR; however, this improvement was not considered clinically relevant. No difference was found for mortality, and insufficient data prohibited meta-analysis for muscle strength and maximal exercise capacity. No adverse effects were reported.
Conclusion
We found a moderate quality of evidence suggesting a small, significant improvement in short-term HRQoL and a clinically nonsignificant improvement in walking distance following PR in patients with COPD and mild symptoms. This resulted in a weak recommendation of routine PR in these patients using the GRADE approach.
Introduction
The beneficial effects of pulmonary rehabilitation (PR) in patients with advanced-stage chronic obstructive pulmonary disease (COPD) are well established.Citation1 In most countries, PR is recommended for COPD patients with a dyspnea score of ≥2 on the modified Medical Research Council dyspnea scale (mMRC).Citation2–Citation5 In these patients, PR results in increased health-related quality of life (HRQoL), increased exercise capacity, and decreased dyspnea.Citation1 Patients with less advanced COPD and fewer symptoms are not routinely offered PR.
It has been suggested that the lack of rehabilitation in patients with COPD and mild symptoms according to mMRC scoring (mMRC ≤1) may result in less focus on nonpharmacological strategies such as smoking cessation and may result in a faster deterioration in the patients’ clinical status due to physical inactivity.Citation4
By extrapolating known benefits of physical exercise in a healthy population to COPD patients with mild symptoms, it could be assumed that these patients also will benefit from physical activity.Citation6 In population studies, reduced levels of physical activity in patients with all grades of COPD are associated with higher risk of hospital admissions and increased mortality; but it is difficult to determine whether reduced physical activity was causal or consequential to the deteriorating health status.Citation7–Citation9 However, a recent large cluster-randomized trial in a primary care setting by Kruis et alCitation10 investigated the effects of integrated COPD management (including exercise) in patients with mean MRC levels of 2 and found no significant effects on the quality of life, hospital admissions, and hospital days.
In this systematic review, we used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) Working Group tool to substantiate and formulate a recommendation on PR in less symptomatic patients with COPD (mMRC ≤1). The study was initiated by the Danish Health and Medicines Authority in the context of a larger project to produce evidence-based national clinical guidelines.Citation11
Methods
Protocol and registration
We did not publish a protocol of prespecified objectives and methods since this review was performed according to standardized methods within the Danish Health and Medicines Authority using GRADE guidelines for the process.Citation12 Further, the population, intervention, control intervention, as well as critical and important outcomes (PICO) were decided by the working-group members prior to our literature search.Citation13
Eligibility criteria
Randomized controlled trials (RCTs) that compared the effects of PR with usual care in patients with COPD and mild symptoms according to dyspnea scores, mMRC ≤1, were considered for inclusion, as were systematic reviews and guidelines based on RCTs. Studies were excluded if they were not RCTs or did not cover the predefined PICO. Our prespecified outcomes were evaluated immediately after PR or at the longest follow-up. The critical outcomes included HRQoL, adverse effects, and mortality, while important outcomes were walking distance (6-minute walk test [6MWT] or shuttle walk test), maximal exercise capacity, muscle strength, and dropout rates. We included manuscripts in English, Danish, Swedish, and Norwegian.
Information sources
Trials were identified searching multiple electronic databases, including Medline, Embase, CINAHL, PsycINFO, G-I-N International, NICE, National Guideline Clearinghouse, Scottish Intercollegiate Guidelines, HTA (The Health Technology Assessment) Database, The Cochrane Library, SBU (Sweden), Socialstyrelsen (Sweden), Helsedirektoratet (Norway), Kunnskapssenteret (Norway), PEDro and OTseeker. The last search was performed on 20 November, 2013.
Search
A research librarian performed the literature search in cooperation with UWI as part of a comprehensive guideline development within the Danish Health and Medicines Authority. First, we performed a broad multidatabase search yielding a total of 2,412 records, followed by a second more specific search for RCTs in Embase and Medline, where 95 records were identified. All records were screened for relevant titles and abstracts, while reference lists of included studies were assessed for further eligible literature (UWI). We searched for guidelines and systematic reviews within the last 10 years, but no specific time restrains were applied to the second search. The specific search strategies are shown in Supplementary materials – Section A.
Study selection
The full texts of relevant guidelinesCitation2,Citation3 were evaluated by two authors independently using the AGREE II (Appraisal of Guidelines for Research and Evaluation) tool (Supplementary materials – Sections B and C), while eligible systematic reviews were assessed using AMSTAR (A Measurement Tool to Assess Systematic Reviews) (Supplementary materials – Section D). On the basis of the AGREE II and AMSTAR assessments, we determined whether the guidelines and reviews could be used directly or in part (eg, literature, quality assessment, and/or meta-analyses) in our study. The AGREE II assessments were also used for other related PICOs within the Danish guideline. RCTs were included if they met the prespecified PICO criteria and were not already included through guidelines or reviews. Any disagreements between reviewers were resolved through discussion.
Data collection process
Data extraction was performed independently by two authors in a predefined Microsoft Excel 2010 spreadsheet (KJJ, UWI) standardized for guideline development within the Danish Health and Medicines Authority, and any disagreements between the authors were solved though discussion. In addition, contact with three corresponding authors of the included RCTs was established (MR) to clarify study design and access additional data. In order to estimate the effect of PR on HRQoL using St George’s Respiratory Questionnaire (SGRQ), both directly after the intervention and at the longest follow-up, additional data were provided from Gottlieb et alCitation14 and van Wetering et al.Citation15 The SGRQ scale ranges from 0 to 100 units, and changes of >4 are regarded clinically relevant.Citation16 Additional data regarding the 6MWT were provided by both van Wetering et alCitation15 and Román et al.Citation17 Regarding the 6MWT, the minimal clinically important difference is 54 m.Citation18
Risk of bias in individual studies
The risk of bias in each study was assessed using the Cochrane Risk of Bias ToolCitation19 by two independent authors (KJJ, UWI). Disagreements were solved through discussion.
Summary measures
All outcomes were assessed using random-effects meta-analyses. Effects of dichotomous outcomes were presented using odds ratios (ORs), and continuous outcomes were presented using mean differences if measured on the same scale, while standardized mean differences were used if different scales measuring the same outcome needed to be combined. Review Manager version 5.3 was used for statistical analyses.Citation20
Synthesis of results
An I Citation2 value of less than 40% was regarded to indicate acceptable heterogeneity. Statistical significance was assessed using 95% confidence intervals (CIs).
Risk of bias for individual outcomes across studies
Two authors (UWI, KJJ) independently evaluated the strength of the evidence for each outcome across studies using the GRADE criteria, and any disagreements were resolved through discussion. If our confidence in the effect measure was downgraded, the reasons were mentioned in footnotes to the “summary of findings” table (). Our overall confidence of the evidence for the intervention was determined by the critical outcome with the lowest rating.Citation21
Table 1 Pulmonary rehabilitation compared to usual care in COPD with mild symptoms
Results
Study selection
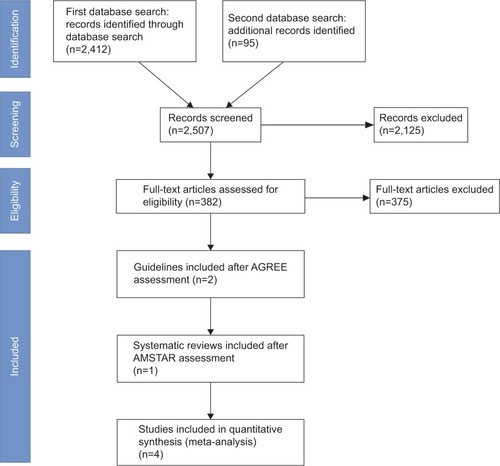
Two national guidelines,Citation2,Citation3 one systematic review,Citation21 and four RCTsCitation14,Citation15,Citation17,Citation22 were included. Neither the guidelines nor the systematic review reported any overall effect estimates and contributed with reference lists only. Data from the four RCTs were included in our meta-analyses.Citation14,Citation15,Citation17,Citation22 A flow diagram of the selection process is presented in .
Figure 1 Flow diagram showing the selection process of material from identification to inclusion.
Characteristics of included studies
The four eligible RCTs included a total of 489 participants with mean ages ranging from 61.3 to 74.1 years. Three of the four studies reported a male predominance ().Citation15,Citation17,Citation22 The PR exercise programs carried out by the intervention groups varied in duration between 7 weeksCitation14 and 6 months,Citation22 frequencies of two to three times weekly, and exercise durations of 30–90 minutes followed by maintenance programs of various lengths.
Table 2 Baseline characteristics of the included studies
Breathing techniques, respiratory physiotherapy, and educational programs in physiology and anatomy were additional elements in combination with the exercise training in the four studies.Citation14,Citation15,Citation17,Citation22 All the four studies were performed in an outpatient setting, but one study also included exercises at home.Citation15 The control groups received usual care consisting of medical treatment, while one study also offered smoking cessation advice.Citation15 No differences in baseline characteristics were reported in any of the four studies. The characteristics of the included studies are summarized in detail in .
Risk of bias within studies
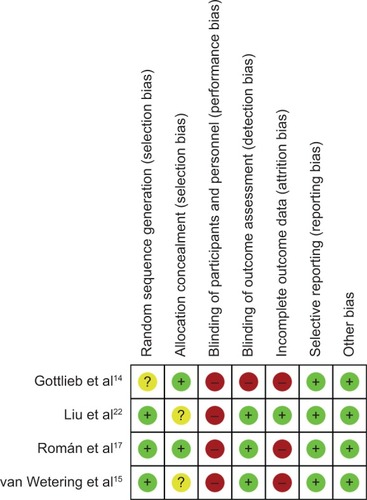
The allocation concealment was not described in two studies,Citation15,Citation22 while one study did not report the randomization process.Citation14 None of the studies blinded the participants or personnel, as this was impossible due to the intervention. Owing to high dropout rates in three of the studies, ranging from 20.6% to 55.7%, a high risk of attrition bias was estimated ().Citation14,Citation15,Citation17 No selective reporting of outcomes or other sources of bias were detected. The risk of bias table is shown in .
Table 3 Dropout characteristics
Figure 2 Risk of bias summary: the review authors’ evaluations of each risk of bias item for each included study.
Effects of the intervention
A meta-analysis could be performed for four predefined outcomes.
Health-related quality of life
The HRQoL was assessed using SGRQ. Two studies were included,Citation14,Citation15 and data from 207 participants were pooled in a meta-analysis evaluating HRQoL directly after the PR and showed a small but statistically and clinically significant improvement of 4.2 units on the SGRQ scale (0–100 points) (95% CI: [−4.51 to −3.89]) in the PR group, compared with the control group (), and there was no observed heterogeneity (I Citation2=0%). Since the participants were not blinded,Citation14,Citation15 the quality of evidence for the short-term evaluation of HRQoL was downgraded to moderate ().
Figure 3 PR versus usual care: short-term evaluation of health-related quality of life measured by St George’s Respiratory Questionnaire.

The same two studiesCitation14,Citation15 also provided data from 205 participants on the effects of PR on HRQoL 18–24 months from baseline, and showed no statistically or clinically relevant difference (mean difference: −1.65; 95% CI: [−5.45 to 2.16]) and an I Citation2 value of 25% (). Our confidence in this result was downgraded to very low due to lack of blinding, dropouts, a wide CI, and effect estimates for the individual trials pointing in opposite directions, reflecting inconsistency ().
Figure 4 PR versus usual care: evaluation of health-related quality of life measured on St George’s Respiratory Questionnaire at the longest follow-up (18–24 months from baseline).

Adverse effects
None of the included studies reported on adverse effects from PR.Citation14,Citation15,Citation17,Citation22
Walking distance
The 6-minute walking distance (6MWD) was investigated in all four studies. Pooling the results of 157 and 156 participants from usual care and PR, respectively,Citation14,Citation15,Citation17,Citation22 yielded a statistically significant mean difference in walking distance of 25.71 m, favoring PR (95% CI: [15.76–35.65]). No heterogeneity was found, I Citation2=0% (). Lack of blinding of the participants led to downgrading of the confidence in our effect estimate to moderate ().
Figure 5 PR versus usual care: walking distance (6-minute walking distance).

Mortality
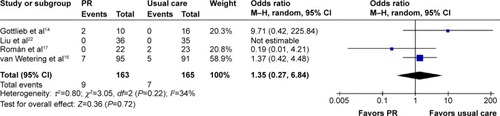
Total mortality was reported in the four studies, including 328 randomized participants with 165 and 163 participants in the usual care group and PR group, respectively.Citation14,Citation15,Citation17,Citation22 Nine events were reported in the PR group, whereas seven events were reported in the control group. No statistically significant difference was found in our analysis, OR =1.35 (95% CI: [0.27–6.84]) (), but the CI was wide due to the small number of events. Accordingly, our confidence in the effect estimate was downgraded to moderate due to imprecision ().
Figure 6 PR versus usual care: mortality, odds ratio.
Muscle strength
The strength of the quadriceps muscle was assessed in only one study, with 87 and 88 participants in the PR and usual care group, respectively. No significant difference was found.Citation15 The same study investigated hand grip force and found a statistically significant improvement in the PR group (mean [standard error] change from baseline was 2.9 (1.1) Ib in the PR group, compared to −1.2 (1.2) Ib in the control group, P<0.01), suggesting a beneficial effect of PR on hand grip force, although this result was found in only one study. The quality of evidence was downgraded due to the lack of blinding and inclusion of only one study.
Maximal exercise capacity
One study investigated the effects of PR on maximal exercise capacity and stated that PR led to an improvement of 234 seconds in a cycling endurance test (P=0.04),Citation15 an improvement that was regarded as clinically relevant.Citation23 The corresponding improvement in the control group was 29 seconds.Citation15 Lack of blinding and lack of data led to downgrading the quality of the evidence to low.
Dropouts
The dropouts reported in the four studies varied from 1 to 54, ranging from 0.8% to 55.7% of the randomized participants ().Citation14,Citation15,Citation17,Citation22
Discussion
Summary of the evidence
The results of the meta-analyses suggested small but statistically and clinically significant improvements of HRQoL in patients with COPD and mild symptoms immediately after participation. However, no long-lasting benefits were found 18–24 months from baseline. Walking distance also improved, but the effect was too small to be considered clinically relevant. In accordance with the GRADE Working Group recommendations, we deemed the overall quality of the evidence to be “very low”, reflecting the lowest quality rating of our critical outcomes.
Our findings in relation to other studies
Jácome and MarquesCitation21 presented a systematic review which similarly indicated that PR may be beneficial to patients with COPD and mild symptoms. However, this study differs methodologically from our study, given that the search strategy presented by Jácome and MarquesCitation21 involved four databases and limited search terms, included only one RCT, and did not provide any effect estimates or meta-analyses.
The prevalence of COPD in Denmark is among the highest in the world.Citation24,Citation25 Therefore, the health-care-related burden of COPD is considerable. The socioeconomic consequences of offering PR to all patients with COPD have, to our knowledge, not been explored, and this was not within the scope of our study. However, we decided on a weak recommendation of routine PR in COPD with mild symptoms for several reasons:
First, we found moderate quality of evidence for both a statistically and clinically significant improvement in HRQoL immediately after the intervention. The HRQoL was assessed using SGRQ, and as we found an improvement of 4.2 units on the SGRQ scale (0–100 points), this was just within what is defined as clinically relevant (>4-point improvement).Citation16 This result was noteworthy since the baseline values for SGRQ were relatively low, suggesting that PR can improve HRQoL in a clinically significant manner in patients with COPD and a relatively preserved health status. However, it is a concern that it was not possible to blind participants when assessing this subjective outcome. In contrast, the aforementioned study of Kruis et al investigated the effects of an integrated COPD management (including exercise) in primary care, but found this intervention to be without effects on the quality of life. The authors state that the low intensity of the exercise training and the unsupervised nature of the program might have contributed to the negative findings, but that they were, nevertheless, representative for a primary care setting.Citation10 The authors advise the application of more intensive exercise programs for patients with a higher burden of disease since these patients possess greater potential for improvement.Citation10
On the basis of very low quality of evidence, we could not detect beneficial effects of PR on HRQoL when assessed at the longest follow-up. Thus, the observed initial beneficial effects on HRQoL were lost after 18–24 months even though two of the included studies provided maintenance programs for the participants.Citation14,Citation15 This result is in agreement with estimates of the long-term effects of PR when provided to more advanced stages of COPD.Citation26
Second, no adverse effects with PR were reported in any of the included RCTs, which is in keeping with our clinical experience.Citation14,Citation15,Citation17,Citation22 Additionally, we found no difference in total mortality between the PR groups and the control groups, which was also in accordance with our expectations. A significant correlation between physical activity levels and a lower mortality was recently described in a systematic review by Gimeno-Santos et alCitation7, and a recent longitudinal study based on the general population of Copenhagen indicated that low baseline values of physical activity are associated with increased mortality.Citation6 Furthermore, determining whether the observed association between physical activity and mortality in the studies was causal or consequential is difficult, and in order to determine the effects of long-term adherence to physical activity on mortality, prospective studies are needed. However, when studying a relatively asymptomatic subgroup of COPD patients, it is difficult to determine the effects of PR on mortality, since the follow-up is relatively short and the number of participants is small.
Third, our results suggest that PR slightly improves exercise capacity, indicated by a statistically significant improvement of the 6MWD in patients with COPD and mild symptoms. However, the average improvement of 26 m is well below what is considered the minimal clinically relevant improvement, and it is unknown whether the conventional outcomes for evaluating the impact of PR are applicable to these mostly asymptomatic patients. Thus, whether the effects of PR can be assessed properly using the 6MWD has previously been questioned,Citation1,Citation27 since a “ceiling effect” has been demonstrated in patients with COPD and mild symptoms, which obviously limits the ability of the test to detect improvements in exercise capacity.Citation27 The use of cycle endurance testing as another measure of exercise capacity was suggested by Laviolette et alCitation23 since their study indicated that cycle endurance is more responsive to the improvement of physical capacity after PR than is the 6MWT. Cycle endurance was investigated in only one of the included studies in our review, and thus, not meta-analyzed. However, results from this trial suggested a clinically significant improvement in the PR group.Citation15 Further, this study was the only one to assess muscle strength, showing that hand grip strength was significantly improved following PR compared to usual care.Citation15
Finally, although positive effects of PR were found, the overall very low quality of evidence led to a weak recommendation. Therefore, clinicians should assess the need for PR individually according to patients’ preferences and clinical manifestations of the disease. We suggest that clinical characteristics such as muscle weakness and inactivity should be taken into consideration when referring patients with less advanced COPD to PR, as we would expect greater individual benefits in these patients than the average improvements seen in our analysis.
Limitations
An important limitation of this study is the high risk of performance bias in the four included studies, in which the lack of blinding of participants and study staff is a recurring issue.Citation14,Citation15,Citation17,Citation22 Especially regarding SGRQ, the risk of performance bias must be considered, since this outcome is easily affected by a lack of blinding. Three of the studies had a high risk of attrition bias due to large dropout rates, and consequently, incomplete outcome data.Citation14,Citation15,Citation17
Moreover, the high dropout rates reflect a general challenge in PR studies, in which dropout rates vary between 20% and 40% in most studies.Citation28 In studies of physical exercise, it is very likely that patients with the poorest health status would drop out more frequently in the intervention arm, leading to an effect estimate biased in favor of the intervention, but this would likely not lead to differential attrition.Citation29
For HRQoL, it must be considered that participants who experience deterioration or no change during the studies are at a higher risk of dropping out, which could also skew results in favor of the intervention.
As with any review, a limitation of this study is the comparability of the intervention, setting, duration of the trial, etc, between the studies. Finally, we did not find sufficient data to produce meta-analyses for muscle strength and the maximal exercise capacity.
Conclusion
On the basis of moderate quality of evidence, we found a small, clinically and statistically significant effect in favor of PR on HRQoL when assessed immediately after the intervention in patients with COPD and mild symptoms. For HRQoL assessed 18–24 months after baseline, no improvement was seen, based on very low quality of evidence.
Further, we found low-to-moderate-quality evidence of improved exercise capacity indicated by increased cycle endurance and 6MWD, but the effect on 6MWD was not regarded as clinically relevant. An overall very low quality of evidence and these moderately positive results on short-term HRQoL and exercise capacity led to a weak recommendation for the use of routine PR in patients with COPD and mild symptoms.
Acknowledgments
We thank Gottlieb et al, Román et al and van Wetering et al who all kindly provided us additional data regarding their studies. A special thanks to both Conni Skrubbeltrang, who assisted in performing the literature search, and Professor Jørgen Vestbo, MD, DMsc, who contributed with valuable comments.
The Centre of Inflammation and Metabolism (CIM) is supported by a grant from the Danish National Research Foundation (DNRF55). The Centre for Physical Activity Research (CFAS) is supported by a grant from Trygfonden. This study was further supported by the Danish Health and Medicines Authority, the Axel Muusfeldt Foundation, the Capital Region of Denmark, and the Novo Nordisk Foundation. CIM is a member of DD2 – the Danish Center for Strategic Research in type 2 diabetes (the Danish Council for Strategic Research, grant no 09-067009 and 09-075724).
Disclosure
PL has received research grants from Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Pfizer; received fee for speaking from AstraZeneca, Boehringer Ingelheim, Glaxo-SmithKline, Novartis, Nycomed, Pfizer, and Sandoz; and received fee for consulting from Almirall, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Mundipharma, Novartis, Nycomed, Sandoz, and Pfizer. All the authors report no other conflicts of interest in this work.
References
- LacasseYMartinSLassersonTJGoldsteinRSMeta-analysis of respiratory rehabilitation in chronic obstructive pulmonary disease. A Cochrane systematic reviewEur Medicophys2007434475485
- BoltonCEBevan-SmithEFBlakeyJDBritish Thoracic Society guideline on pulmonary rehabilitation in adultsThorax201368Suppl 2ii1ii3023880483
- MarciniukDDBrooksDButcherSOptimizing pulmonary rehabilitation in chronic obstructive pulmonary disease – practical issues: a Canadian Thoracic Society Clinical Practice GuidelineCan Respir J201017415916820808973
- SpruitMASinghSJGarveyCAn official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitationAm J Respir Crit Care Med20131888e13e6424127811
- The Danish Health and Medicines AuthorityKOL – Kronisk obstruktiv lungesygdom: Anbefalinger for tidlig opsporing, opfølgning, behandling og rehabilitering [COPD – chronic obstructive pulmonary disease. Recommendations for early recognition, follow-up, treatment and rehabilitation]. Version 2; 2007 Available from: http://sundhedsstyrelsen.dk/da/sundhed/puljer-og-projekter/projekter/kol-projektet-tidlig-opsporing,-opfoelgning,-behandling-og-rehabilitering-af-kol/kol-anbefalinger-for-tidlig-opsporing,-opfoelgning,-behandling-og-rehabiliteringAccessed September 1, 2014 Danish
- VaesAWGarcia-AymerichJMarottJLChanges in physical activity and all-cause mortality in COPDEur Respir J20144451199120925063247
- Gimeno-SantosEFreiASteurer-SteyCDeterminants and outcomes of physical activity in patients with COPD: a systematic reviewThorax201469873173924558112
- TroostersTvan der MolenTPolkeyMImproving physical activity in COPD: towards a new paradigmRespir Res201314111524229341
- Garcia-AymerichJSerraIGomezFPPhysical activity and clinical and functional status in COPDChest20091361627019255291
- KruisALBolandMRAssendelftWJEffectiveness of integrated disease management for primary care chronic obstructive pulmonary disease patients: results of cluster randomised trialBMJ2014349g539225209620
- The Grading of Recommendations Assessment Development and Evaluation (GRADE) Working Group Available from: http://www.gradeworkinggroup.org/Accessed August 8, 2014
- The Danish Health and Medicines AuthorityNationale Kliniske Retningslinjer [National Clinical Guidelines] Available from: https://sundhedsstyrelsen.dk/da/sundhed/kvalitet-og-retningslinjer/nationale-kliniske-retningslinjer. Updated August 21, 2014Accessed August 29, 2014 Danish
- GuyattGHOxmanADKunzRGRADE guidelines, 2: framing the question and deciding on important outcomesJ Clin Epidemiol201164439540021194891
- GottliebVLyngsoAMNyboBFrolichABackerVPulmonary rehabilitation for moderate COPD (GOLD 2) – does it have an effect?COPD20118538038621936683
- van WeteringCRHoogendoornMMolSJRutten-van MolkenMPScholsAMShort- and long-term efficacy of a community-based COPD management programme in less advanced COPD: a randomised controlled trialThorax201065171319703824
- JonesPWInterpreting thresholds for a clinically significant change in health status in asthma and COPDEur Respir J200219339840411936514
- RománMLarrazCGomezAEfficacy of pulmonary rehabilitation in patients with moderate chronic obstructive pulmonary disease: a randomized controlled trialBMC Fam Pract2013142123399113
- RedelmeierDABayoumiAMGoldsteinRSGuyattGHInterpreting small differences in functional status: the Six Minute Walk test in chronic lung disease patientsAm J Respir Crit Care Med19971554127812829105067
- The Cochrane CollaborationCochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 Available from: www.cochrane-handbook.org. Updated March 2011Accessed August 11, 2014
- Review Manager 5.3 [computer program]Copenhagen, DenmarkThe Nordic Cochrane Centre, The Cochrane Collaboration2014
- JácomeCMarquesAPulmonary rehabilitation for mild COPD: a systematic reviewRespir Care201459458859424106321
- LiuX-DJinH-ZNgBH-PGuY-HWuY-CLuGTherapeutic effects of qigong in patients with COPD: a randomized controlled trialHKJOT20122213846
- LavioletteLBourbeauJBernardSAssessing the impact of pulmonary rehabilitation on functional status in COPDThorax200863211512117901158
- BuistASMcBurnieMAVollmerWMInternational variation in the prevalence of COPD (The BOLD Study): a population-based prevalence studyLancet2007370958974175017765523
- FabriciusPLøkkeAMarottJLVestboJLangePPrevalence of COPD in CopenhagenRespir Med2011105341041720952174
- BeauchampMKEvansRJanaudis-FerreiraTGoldsteinRSBrooksDSystematic review of supervised exercise programs after pulmonary rehabilitation in individuals with COPDChest201314441091109324081336
- SmithDRUse of the 6-Min Walk Test: A Pro and Con Review. PCCSU article2320096 Available from: http://69.36.35.38/accp/pccsu/use-6-min-walk-test-pro-and-con-review?page=0,3Accessed September 1, 2014
- FischerMJScharlooMAbbinkJJDrop-out and attendance in pulmonary rehabilitation: the role of clinical and psychosocial variablesRespir Med2009103101564157119481919
- AlmadanaVRomeroCValidoAGómez-BasteroASánchezJMontemayorTProfile of patients who drop out of a pulmonary rehabilitation program [meeting abstracts]Chest2014145Suppl 3370A24493508