
Abstract
Objectives
The aim of this study is to evaluate the ability and practice of spirometry, training of technicians, and spirometry features in primary care centers in Spain, evaluating those located in a rural environment against those in urban areas.
Methods
An observational cross-sectional study was conducted in 2012 by a telephone survey in 970 primary health care centers in Spain. The centers were divided into rural or urban depending on the catchment population. The survey contacted technicians in charge of spirometry and consisted of 36 questions related to the test that included the following topics: center resources, training doctors and technicians, using the spirometer, bronchodilator test, and the availability of spirometry and maintenance.
Results
Although the sample size was achieved in both settings, rural centers (RCs) gave a lower response rate than urban centers (UCs). The number of centers without spirometry in rural areas doubled those in the urban areas. Most centers had between one and two spirometers. However, the number of spirometry tests per week was significantly lower in RCs than in UCs (4 [4.1%] vs 6.9 [5.7%], P<0.01). The availability of a specific schedule for conducting spirometries was higher in RCs than in UCs (209 [73.0%] vs 207 [64.2%], P=0.003). RCs were more satisfied with the spirometries (7.8 vs 7.6, P=0.019) and received more training course for interpreting spirometry (41.0% vs 33.2%, P=0.004). The performance of the bronchodilator test showed a homogeneous measure in different ways. The spirometer type and the reference values were unknown to the majority of respondents.
Conclusion
This study shows the differences between primary care RCs and UCs in Spain in terms of performing spirometry. The findings in the present study can be used to improve the performance of spirometry in these areas.
Introduction
Rural and urban communities have distinct characteristics in terms of demographics, social, and physical environments and may vary in access to health care facilities and services. The characteristics of rural patients have been studied in some communities showing sociodemographic differences.Citation1 Additionally, important differences have been reported in different respiratory conditions in different countries between rural and urban areas from a epidemiological and clinical standpoint.Citation2,Citation3 Of note, disparities in pulmonary function have also been reported.Citation4 Examination of geographic variation in disease occurrence and other disease measures provides a method for detection of gaps in quality of public health activities and clinical health care services.Citation5
Spirometry is a necessary diagnostic technique for the diagnosis of many prevalent chronic respiratory diseases. In fact, spirometry is the most used guidelines for diagnosis and treatment of chronic obstructive pulmonary disease (COPD) as the Global Initiative for Chronic Obstructive Lung Disease indicates that it is a prerequisite for diagnosing the disease and a necessary tool to establish the best treatment possible.Citation6 The Global Initiative for Asthma (GINA) recommends spirometry to measure airflow limitation, and its reversibility highlights and confirms the diagnosis of asthma.Citation7
In Spain, a recent study was done comparing the use of spirometry in primary and secondary care (3E project).Citation8 The study showed important differences in the use, training, and maintenance of spirometers. By using the 3E database, the aim of the study was to evaluate the ability and practice of spirometry, training of technicians, and spirometry features in primary care centers in Spain, evaluating those located in a rural environment against those in urban areas.
Methods
This study is a subanalysis of the 3E project, whose methodology is available elsewhere.Citation8 In short, it is a cross-sectional study of 970 primary care centers in Spain that routinely evaluated adult patients with respiratory disease. The questionnaire consisted of 36 items that included the following topics: center resources, training doctors and technicians, using the spirometer, bronchodilator test (BDT), and the availability of spirometry and maintenance. The survey was conducted between January 2012 and March 2012 by telephone, through a semi-structured computer-assisted telephone interview done to the technicians responsible for performing the spirometries with an average of 20 minutes duration.
The aim of this study was to obtain information from 20% of the primary care centers in Spain. The centers were divided in rural or urban depending on the catchment population (25,000 habitants was considered the limit). The present study did not involve human subjects, material, or data, so an ethics committee approval was deemed not to be necessary. All participants gave oral consent to complete the survey.
Data analysis was performed using the Statistical Package for the Social Sciences software version 18.0 (IBM Corporation, Armonk, NY, USA). Description of variables was done using the absolute and relative frequencies for categorical responses. Inferential studies were conducted comparing data from rural centers (RCs) to urban centers (UCs) using chi-square test and Student’s t-test for independent data. A P-value lower than 0.05 was considered statistically significant.
Results
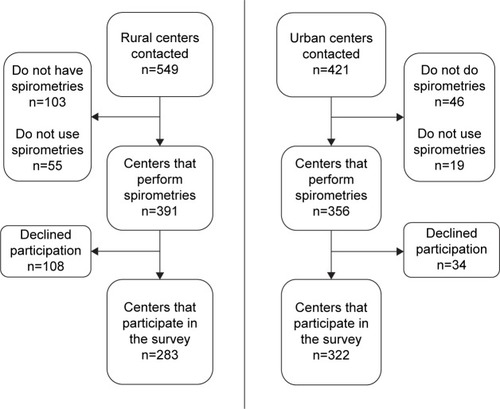
To survey 20% of primary care centers in Spain, 970 centers were screened (43.9% RCs and 56.6% UCs). Data were obtained from 21.2% of those in Spain. The response rate was 51.5% for RCs and 76.4% for UCs (P<0.001). Of these 266 RCs that were not surveyed, 38.7% did not have spirometer, 20.7% did have a spirometer but were not using it, and 40.6% declined participation. In the 99 UCs that were not surveyed, 46.5% did not have spirometer, 19.2% did have a spirometer but were not using it, and 34.3% refused participation (). Accordingly, the number of centers without spirometry in rural areas doubled the urban areas.
Figure 1 Flowchart of the centers surveyed.
In most primary care centers, spirometry was performed only in the center, 264 (94.0%) of RCs and 313 (97.2%) of UCs. Most centers, both UCs and RCs, had between one and two spirometers (). However, the number of spirometry tests per week was significantly lower in RCs than in UCs (P<0.001). Among major needs for the performance and interpretation were to have more training (20.5% of UCs and 15.9% of RCs) and adequate room (11.0% of RCs and 14.6% of UCs), while major needs for the interpretation of spirometry were being properly trained (15.8% of UCs and 17.0% of RCs), followed by having staff who can interpret them (4.7% of UCs and 4.2% of RCs). The availability of a specific schedule for conducting spirometries in absolute numbers is very close but in percentage was higher in RCs than in UCs (P=0.003).
Table 1 Information on center resources
Staff and training outcomes are summarized in . Nurses were the main professional who did spirometries both in RCs and UCs, but mostly in UCs (P=0.005). Most centers had received some training for performing spirometry. In most centers, this training was both theoretical and practical, but usually at only one point with a mean of 22.5 months from the last training in RCs and 18.5 months in UCs, without training further repeated. RCs were more satisfied with the spirometries (7.8 vs 7.6, P=0.019) and passed more training course for interpreting spirometry (41.0% vs 33.2%, P=0.004).
Table 2 Information regarding staff and training
Regarding using the spirometer (), the majority of the indications were to the study of asthma or COPD, with an estimated number of spirometry considered invalid approximately 10%.
Table 3 Information regarding spirometer use
The realization of the BDT () was performed homogeneously, which is demonstrated by analyzing different points. According to current recommendations,Citation9 an improvement in either forced vital capacity (FVC) or forced expiratory volume in 1 second (FEV1) was considered reversible. Most centers used short-acting β2 agonists for BDT, but in general, the number of inhalations was often insufficient and time to wait was often incorrect. The criteria for considering a positive BDT were right in almost half of the respondents.
Table 4 Information regarding the bronchodilator test
The spirometer type and the reference values were unknown to the majority of responding technicians (); UCs used values of the Spanish Society and RCs had a greater ignorance of the values used.
Table 5 Information regarding spirometer features
Finally, information on the maintenance of the spirometer is summarized in . Not all centers calibrated the spirometer daily. When asked for the reason of not calibrating, the most common response was nonavailability of syringe calibration or nonrequirement by the device.
Table 6 Information regarding spirometer maintenance
Discussion
The study of 3E project highlights the differences between primary care UCs and RCs in Spain in terms of scope of practice of spirometry. The principal findings are differences in the number of spirometry performed and specific planning, which is higher in UCs than in RCs; satisfaction with the performance of spirometry and the number of centers receiving courses for interpretation, which is higher in RCs than UCs; and the use and knowledge of the reference values, which is higher in UCs than in RCs.
This is the first survey that was published in Spain with national coverage, whose results were partially published previously.Citation10,Citation11 The most important strength of our study is the analysis of the rural and urban population in terms of performing spirometry, something that had not been described previously. The main contribution of this study is the large sample size, with a representation of the entire national territory and a protocol applied evenly. However, there are a number of limitations that should be considered. The first one is that the survey was conducted to the technician who did the test. This way of performing the survey are beneficial in that the questions are to the person that daily performed the test, although when assessing questions about the interpretation of results have to be cautious. Additionally, the work has been done through a telephone survey, which has the advantages of access to centers with less resource, be faster than the mail or personal interviews, and to survey a large number of centers but always carries some degree of non-response and make necessary to confirm the veracity of what the respondent answered. Survey was self-reported, in which remained external validity. But because the response rate was high, we trusted the validity and representativeness of the data obtained. Finally, in order to encourage participation, we deliberately limited the number of questions to those which we thought were most relevant. It is then possible that some relevant aspects of spirometry may have been left out. In particular, the quality criteria to consider a valid spirometry were not included in the survey. In addition, one interesting approach for the future would be to correlate our findings with the clinical management of the patients in order to evaluate if performing a correct spirometry may have some influence on clinical care provided to patients or on clinical outcomes.
Spirometry is an essential technique for the diagnosis of prevalent diseases such as asthma or COPD. However, its use in primary care centers is not widely achieved. In Spain, only half of the patients diagnosed with COPD in primary care had a spirometry,Citation12 which has also been identified in other countries like the USA in studies with more than 90,000 patients.Citation13 People with unrecognized COPD may miss the opportunity to improve their health status because of lack of performance of functional tests.Citation14 The evaluation of the variability among rural and urban regions is essential in order to explore the situation in Spain. This variability in primary care has also been described within other countries. In Italy, a study conducted on 617,280 patients revealed that treatment was usually prescribed without performing pulmonary function tests or without taking into account the severity of airway obstruction.Citation15 Importantly, COPD patients in rural areas have been associated with worse health status and greater impairment.Citation16 There is little information in Spain to analyze the characteristics of the population using these services. In order to make informed decisions about the allocation of resources, it seems important to know more information on these patients than the number of patients who have undergone spirometry.
One of the most important points of our study is the finding of the low number of spirometry tests that are done in the primary care centers in Spain. Differences between UCs and RCs are shown both in spirometry number and programming the time and schedule. Rural and urban communities have distinct characteristics in terms of demographic, social, and physical environments and may vary in access to health care facilities and services. Some studies have shown that in certain areas such as in Canada, rural residents tend to be older and are more likely to be obese, have less education, and have lower income than urban residents.Citation17 Rural populations also have a higher prevalence of chronic conditions such as diabetes and heart disease.Citation18 End-of-life decisions in COPD are also different in rural areas in Spain.Citation19 However, rural residents report several barriers to accessing health care, including transportation difficulties and distance to care, social isolation, financial constraints, limited health care facilities (hospitals and pharmacies), physician shortages, and lack of access to specialist care. The lack of access to primary care physicians, specialists, or health care facilities could result in decreased prescribing of evidence-based medications. In fact, in a sample of COPD patients in the USA, it was found that rural residents were associated with poorer health status and higher levels of utilization of selected health care services compared to urban residents.Citation16 Because rural communities have a higher proportion of older residents, there is a higher demand of health care services for chronic conditions; hence, the services provided should be better.
Another important finding in this study is the difference found in the degree of satisfaction with spirometry and the number of centers that perform training courses for interpretation of spirometry. Training is surprisingly higher in RCs than in UCs. Spirometry is not an extremely difficult technique to perform but requires learning, and this is maintained over time. This is what the European Respiratory Society aimed with the dissemination of a spirometry training program within Europe.Citation20 Educational program had a very limited impact on general practitioners’ clinical practice. The usage of spirometry is poor with the general practitioners tending to perform more chest X-rays than pulmonary function tests.Citation21 In our study, it appears that the satisfaction and the amount of training is higher in RCs than in UCs.
The usefulness of the BDT in the diagnosis and treatment of asthma and COPD has been and continues to be a source of debate. Despite its simplicity, it remains difficult to interpret and translate into specific therapeutic strategies, particularly in COPD.Citation22 In our study, it seems that there are few differences between the UCs and RCs. As for the bronchodilator used, we enquired on the most commonly used. However, it is possible that some centers used more than one, but the survey did not ask for this possibility and the respondents were forced to choose one.
Calibration is absolutely necessary, this being one of the weaknesses we have observed with our work. In our study, we found no differences in calibration, but it stresses that not all centers’ spirometers calibrated daily. We believe that these data should be assessed and encourage health authorities to take the necessary measures to resolve this problem that can cause problems in diagnosis.
In summary, this study shows the differences between primary care RCs and UCs in Spain in terms of performing spirometry. In RCs, less spirometries are performed, but the degree of satisfaction and the number of training sessions are greater in UCs. These findings can be used to improve and standardize health care resources to ensure similar coverage to the entire population, regardless of the area in which resides.
Acknowledgments
This study was conducted on behalf of the 3E project of which the following people were involved: Steering committee; Myriam Calle Rubio, Joan B Soriano, Jose Luis Lopez-Campos. Working panel (by alphabetical order of the scientific society they represent); AIRE, Borja Garcia Cosio, Isabel Mir. ASTURPAR, Cristina Martínez González. NEUMOCAN, Ana Velázquez. NEUMOMADRID, Jose Miguel Rodríguez González-Moro. NEUMOSUR, Aurelio Arnedillo. SADAR, Luis Borderias Clau. SEAR, Juan Antonio Riesco Miranda. SEPAR, Juan Ruiz Manzano (president), German Peces Barba. SOCALPAR, Jose Luis Viejo Bañuelos. SOCAMPAR, Encarnación López Gabaldón (president). SOCAP, Eduard Monso Molas (president). SOGAPAR, Marina Blanco Aparicio. SOMUPAR, Juan Luis de la Torre Alvaro (president). SVNEUMO, Mª Cruz González Villaescusa. SVNPR, Juan Bautista Galdiz.
Disclosure
The authors report no conflicts of interest in this work.
References
- SmithKBHumphreysJSWilsonMGAddressing the health disadvantage of rural populations: how does epidemiological evidence inform rural health policies and research?Aust J Rural Health2008162566618318846
- WangSKouCLiuYRural-urban differences in the prevalence of chronic disease in northeast ChinaAsia Pac J Public Health201527439440625246500
- O’LearySTBarnardJLockhartSUrban and rural differences in parental attitudes about influenza vaccination and vaccine delivery modelsJ Rural Health2015Accessed May 7, 201510.1111/jrh.12119 Epub ahead of print
- SonnappaSLumSKirkbyJDisparities in pulmonary function in healthy children across the Indian urban-rural continuumAm J Respir Crit Care Med20151911798625412016
- RadleyDCSchoenCGeographic variation in access to care – the relationship with qualityN Engl J Med201236713622693955
- Global Initiative for Obstructive Lung Disease Available from: http://www.goldcopd.orgAccessed May 20, 2015
- BouletLPFitzGeraldJMLevyMLA guide to the translation of the Global Initiative for Asthma (GINA) strategy into improved careEur Respir J20123951220122922282546
- López-CamposJLSorianoJBCalleMEncuesta de Espirometría en España (3E) ProjectA comprehensive, national survey of spirometry in Spain: current bottlenecks and future directions in primary and secondary careChest2013144260160923411500
- PellegrinoRViegiGBrusascoVInterpretative strategies for lung function testsEur Respir J200526594896816264058
- Lopez-CamposJLSorianoJBCalleM3E ProjectDeterminants of use of the bronchodilator test in primary and secondary care: results of a national survey in SpainClin Respir J2014 Epub ahead of print
- López-CamposJLSorianoJBCalleM3E ProjectInter-regional changes in the performance and interpretation of spirometry in Spain: 3E studyArch Bronconeumol2014501147548324816035
- MonteagudoMRodriguez-BlancoTParcetJVariability in the performing of spirometry and its consequences in the treatment of COPD in primary careArch Bronconeumol201147522623321295903
- JooMJLeeTAWeissKBGeographic variation of spirometry use in newly diagnosed COPDChest20081341384518347201
- YawnBPWollanPCKnowledge and attitudes of family physicians coming to COPD continuing medical educationInt J Chron Obstruct Pulmon Dis20083231131718686740
- CazzolaMBettoncelliGSessaECricelliCPrimary care of the patient with chronic obstructive pulmonary disease in ItalyRespir Med2009103458258819103479
- JacksonBECoultasDBSuzukiSSinghKPBaeSRural-urban disparities in quality of life among patients with COPDJ Rural Health201329suppl 1s62s6923944281
- VanasseACourteauJCohenAAOrzancoMGDrouinCRural-urban disparities in the management and health issues of chronic diseases in Quebec (Canada) in the early 2000sRural Remote Health2010104154821039080
- BanegasJRRodriguez-ArtalejoFde la Cruz TrocaJJBlood pressure in Spain: distribution, awareness, control, and benefits of a reduction in average pressureHypertension199832699810029856963
- López-CamposJLRuiz-RamosMMendezCGarcía-LeónJCharacteristics of subjects who died of chronic obstructive pulmonary disease in Andalusia in 2010 and 2011J Palliat Med201316121610161324206007
- SteenbruggenIMitchellSSeverinTHarmonising spirometry education with HERMES: training a new generation of qualified spirometry practitioners across EuropeEur Respir J201137347948121357919
- BertellaEZadraAVitaccaMCOPD management in primary care: is an educational plan for GPs useful?Multidiscip Respir Med2013812423509969
- CalverleyPMAlbertPWalkerPPBronchodilator reversibility in chronic obstructive pulmonary disease: use and limitationsLancet Respir Med20131756457324461617