
Abstract
Background
Cough is a prevalent symptom that impacts quality of life in COPD. The aim of this study was to assess the relationship between cough-specific quality of life, abdominal muscle endurance, fatigue, and depression in stable patients with COPD.
Methods
Twenty-eight patients with COPD (mean age 60.6±8.7 years) referred for pulmonary rehabilitation participated in this cross-sectional study. Sit-ups test was used for assessing abdominal muscle endurance. Leicester Cough Questionnare (LCQ) was used to evaluate symptom-specific quality of life. Fatigue perception was evaluated with Fatigue Impact Scale (FIS). Beck Depression Inventory (BDI) was used for assessing depression level.
Results
The LCQ total score was significantly associated with number of sit-ups; BDI score; FIS total; physical, cognitive, and psychosocial scores (P<0.05). Scores of the LCQ physical, social, and psychological domains were also significantly related with number of sit-ups, FIS total score, and BDI score (P<0.05). FIS total score and number of sit-ups explained 58% of the variance in LCQ total score (r=0.76, r2=0.577, F(2–20)=12.296, P<0.001).
Conclusion
Chronic cough may adversely affect performance in daily life due to its negative effect on fatigue and decrease abdominal muscle endurance in patients with COPD. Decreased cough-related quality of life is related with increased level of depression in COPD patients. Effects of increased abdominal muscle endurance and decreased fatigue in COPD patients with chronic cough need further investigation.
Introduction
COPD is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response to noxious particles and gases in the airways and lungs. The characteristic symptoms of COPD are chronic and progressive dyspnea, cough, and sputum production that can be variable from day to day. Initially, the cough may be intermittant, but later is present everyday, often throughout the day.Citation1
While cough is an important defence mechanism that helps clear excessive secretions and foreign material from the airways, chronic cough was found to be significantly associated with meaningful adverse psychosocial and physical effects on health-related quality of life (HRQoL).Citation2,Citation3 Decrease in HRQoL with chronic cough was more likely to be psychosocial than physical in nature.Citation2
There is now better evidence for the fact that people who have cough regularly, productive of sputum, are more likely to develop pneumonic complications during COPD exacerbations and subsequently die.Citation4 Chronic cough defined as cough lasting >8 weeks causes significant morbidity and utilization of health care resources.Citation5
Cough-related syncope, incontinence, vomiting, sleep deprivation, and depression are among some of the more severe adverse effects of cough and require prompt assessment and treatment.Citation6,Citation7 It was found that depressive symptomatology is very common in patients with chronic cough.Citation8,Citation9 Whereas abdominal muscle strength is preserved in stable COPD patients,Citation10 it was shown that expiratory muscle endurance that primarily includes abdominal muscles is decreased in COPD.Citation11 Fatigue is found to be significantly increased in COPD patients compared to controls,Citation12,Citation13 and dyspnea and physical symptoms have more impact on fatigue than physiologic variables.Citation14 Prolonged coughing can cause soreness or even strain in the abdominal or rib muscles, and hence have a negative impact on abdominal muscle endurance. Inefficient use of abdominal muscles during cough may increase physical complaints and the patients’ fatigue perception.
Although there are studies about the impact of cough on HRQoL in COPD compared with different diseasesCitation15 and healthy controls,Citation16 we did not find any studies about the relationship between cough-specific quality of life and abdominal muscle endurance, fatigue, and depression in COPD. Therefore, the primary objective of the study was to investigate the relationship between cough-specific quality of life and abdominal muscle endurance, fatigue, and depression in patients with COPD. The secondary objective of the study was to identify which of these factors (abdominal muscle endurance, fatigue, and depression) influence cough-specific quality of life.
Methods
Subjects
This cros-sectional study included 28 COPD patients referred for pulmonary rehabilitation between the ages of 40 and 80 years (22 male/6 female, mean forced expiratory volume in 1 second (FEV1): 53.7%±24.9%) who had been on the same medicine in the previous 3 weeks and not taking antibiotics. Patients who were not able to walk or who have a disability preventing them from walking, and patients who were not able to cooperate with pulmonary function tests and questionnares were not included in the study. The study was approved by the Ethical Committee of Hacettepe University and each subject signed an informed consent form.
Assessments
Physical, physiological, and sociodemographic data were recorded. Body mass index (BMI) was calculated with the formula body weight/height in metersCitation2 (kg/m2).Citation17 The patients’ smoking history was recorded as pack-years. Dyspnea, cough, and sputum symptoms of patients were questioned and recorded. The number of exacerbations in the previous year before participating in this study was recorded. Patients’ dyspnea levels were determined with the Modified Medical Research Council (MMRC) Dyspnea Scale.Citation18
The pulmonary function test was performed with a Spirolab III spirometer (Spirolab; Medical International Research, Rome, Italy) according to the American Thoracic Society/European Respiratory Society criteria. Forced vital capacity (FVC), FEV1, FEV1/FVC rate, peak expiratory flow (PEF), and forced expiratory flow between 25% and 75% of FVC (FEF25%–75%) were recorded. Pulmonary function test parameters were expressed as percentage of the expected value for age, height, body weight, and sex.Citation19,Citation20
Abdominal muscle endurance was assessed using a sit-ups test. Patients were asked to lift up the trunk from the supine position until the lower angle of the scapula with the arms stretched forward consecutively as quickly as possible for 30 seconds. Pressure was given on patients’ knees with therapist’s hands to hold the patients’ feet on the ground. Verbal encouragement was given during test like “You are doing well. Continue”. The number of sit-ups were recorded for analysis.Citation21
The Leicester Cough Questionnaire (LCQ) is a valid and reliable health-related quality of life measurements for adults with chronic cough and patients with COPD. Adaptation of the LCQ was made for the Turkish people and Turkish version of the LCQ was used for evaluation.Citation22 It consists a total of 19 items that are divided into physical (eight items), psychosocial (seven items), and social (four items) subdimensions. Total score ranges from 3 to 21. Low scores on the LCQ means a higher effect of coughing on the subject.Citation22,Citation23
The fatigue perception of the subjects was evaluated by the Fatigue Impact Scale (FIS). FIS is a multidimensional scale to assess the patient’s perception of the limitations in the physical (ten items), cognitive (ten items), and psychosocial (20 items) functions caused by fatigue during the last month. Total score ranges between 0 and 160. High scores represents a higher effect of fatigue.Citation24
Beck Depression Inventory (BDI) is a self-rating scale that has been developed to determine the risk of depression, level, and severity of depressive symptoms in individuals and is practiced in healthy subjects and psychiatric patients. It contains 21 self-assessment sentences. Each item is scored from 0 to 3 and total score is obtained by collecting them. The total score ranges from 0 to 63. A score of 0–9 indicates minimal depressive symptoms, 10–16 mild depressive symptoms, 17–29 moderate depressive symptoms, and 30–63 severe depressive symptoms.Citation25
Statistical analysis
All the analyses were performed using the Statistical Program for the Social Sciences version 15.0 (SPSS Inc., Chicago, IL, USA) for Windows.Citation26 Variables were expressed as mean ± standard deviation, frequency, percentage, median, minimum, and maximum. Normal distribution of variables was tested with Shapiro–Wilk Test. Correlations were analyzed using the Pearson’s correlation analysis because parametric conditions were met by the data. Correlations were classed as “high” (r>0.70), “moderate” (r=0.50–0.69), “low” (r=0.26–0.49), and “little or no correlation” (r=0.00–0.25).Citation27 Multiple regression analysis was carried out using the LCQ total score as dependent variable and variables with a significant relationship with the LCQ total score (P<0.015) based on correlation analysis as independent variable. With a 5% type-1 error level and a total of 28 subjects, the study has 80% power to detect correlations with a magnitude of |r|>0.45 among the study parameters as statistically significant. The level of significance was set to P<0.05.Citation28
Results
Twenty-eight clinically stable patients with COPD were included in the study. Data regarding the characteristics of the participants are presented in . Mean age of the subjects was 60.6±8.7 years and mean BMI was 27.1±5.5 kg/m2. Mean FEV1 (%) of COPD patients was 53.7%±24.9%. Approximately, 17.9% of the patients were in GOLD stage I, 35.7% in GOLD stage II, 25.0% in GOLD stage III, and 21.4% in GOLD stage IV. Approximately, 64.3% (n=18) of patients had chronic cough and 96.4% of subjects had dyspnea symptom, and median of MMRC scores was 1.5.
Table 1 Characteristics of COPD patients
Abdominal muscle endurance, cough-specific quality of life, fatigue perception, and depression level results are given in . Mean number of sit-ups was 17.0±5.7. Mean LCQ total score was 15.9±3.8, mean FIS total score was 40.0±30.7, and mean BDI score was 12.0±9.4. Approximately, 50.0% of patients had minimal depressive symptoms, 19.2% had mild depressive symptoms, 23.1% had moderate depressive symptoms, and 7.7% had severe depressive symptoms.
Table 2 Abdominal muscle endurance, cough-specific quality of life, fatigue perception, and depression level in patients with COPD
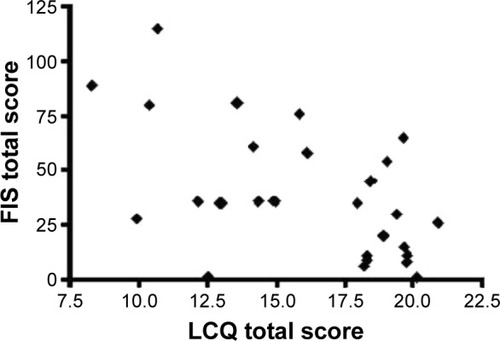
The LCQ total score was significantly correlated with number of sit-ups (r=0.704, P<0.001, ), BDI score (r=−0.550, P=0.004, ), FIS total (r=−0.557, P=0.003, ), physical (r=−0.543, P=0.003), cognitive (r=−0.494, P=0.009), and psychosocial scores (r=−0.566, P=0.002). The LCQ physical score was also significantly related to the number of sit-ups (r=0.713, P<0.001), FIS total score (r=−0.578, P=0.002), and BDI score (r=−0.553, P=0.003). The LCQ social score was also significantly associated with the number of sit-ups (r=0.644, P=0.001), FIS total score (r=−0.444, P=0.020), and BDI score (r=−0.475, P=0.014). The LCQ psychological score was also significantly correlated with the number of sit-ups (r=0.687, P<0.001), FIS total score (r=−0.602, P=0.001), and BDI score (r=−0.552, P=0.003) (). Based on the multiple linear regression analysis, it was found that the FIS total score and number of sit-ups explained 58% of the variance in LCQ total score (r=0.76, r2=0.577, F(2–20)=12.296, P<0.001, ).
Table 3 The correlations between cough-specific quality of life and abdominal muscle endurance, fatigue perception, and depression level in patients with COPD
Table 4 Multiple linear regression analysis
Figure 1 The relationship between cough-specific quality of life and abdominal muscle endurance.
Abbreviation: LCQ, Leicester Cough Questionnaire.
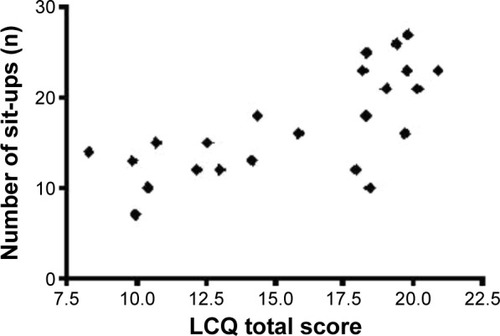
Figure 2 The relationship between cough-specific quality of life and depression level.
Abbreviations: LCQ, Leicester Cough Questionnaire; BDI, Beck Depression Inventory.
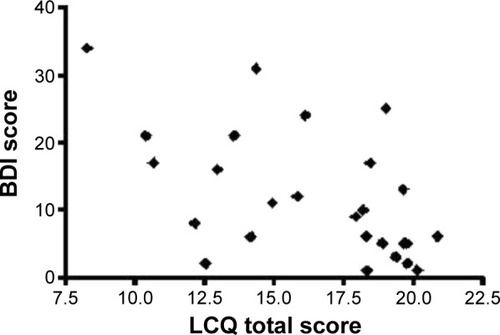
Figure 3 The relationship between cough-specific quality of life and general impact of fatigue on daily living activities.
Discussion
In the present study, we have shown that lower cough-specific quality of life is associated with worse performance in daily living activities due to its negative effect on fatigue and lower abdominal muscle endurance, and higher depression levels are usually observed in patients with COPD. Besides, it was shown that the general impact of fatigue in daily life and abdominal muscle endurance may provide general information about the cough-specific quality of life.
While it is known that patients with chronic cough have a risk of physical complications, patients were found to be widely disturbed from psychosocial complications and combination of these side effects. Most of the patients with persistent cough suspect suffering from a serious condition (72%), and they consult a physician to get assurance that they do not have such a condition (77%). Rib fractures, incontinence, fatigue, shame, unconsciousness, difficult conversations on the phone, hoarse sound, inability to sleep at night, unable to stand close to the their relatives due to cough, and inability to work in school or elsewhere are the other complaints that may impair the quality of life.Citation2,Citation29,Citation30 In the literature, it was shown that cough adversely affects health status in patients with COPD.Citation15,Citation16 In a study that comprised 54 patients with COPD (mean FEV1 (%): 47±13), mean LCQ total score was 13.6±2.8.Citation23 In a group of COPD patients (mean FEV1 (%): 53.7±24.9) in our study, mean LCQ total score was 15.9±3.8. In our study, we have shown that cough impairs HRQoL in a group of COPD patients with chronic cough (64.3%), as reported in the literature.Citation15,Citation16,Citation23
Typical cough consists of four phases: inspiratory, compressive, expulsive, and relaxation phases.Citation31 Coughing involves coordinated contractions of the thoracic, abdominal, and pelvic muscles.Citation32 Abdominal muscles play an important role in expulsive phase.Citation31 Abdominal muscle endurance of patients with COPD was shown to be lower than that of the healthy subjects.Citation11,Citation16 According to the SAFE index score, which is a multidimensional staging system for COPD, HRQoL evaluation is significantly related to the number of sit-ups in moderate to very severe COPD patients.Citation33 In accordance with this finding, we determined that cough-specific quality of life is significantly related to abdominal muscle endurance. Because of the contraction of abdominal muscles during coughing, decrease in the endurance of these muscles may adversely affect cough efficiency and secretion clearance. Therefore, it may impair cough-specific quality of life by creating physical, social, and psychological problems.
According to previous studies, fatigue perception was found to be increased in patients with COPD compared to healthy subjects.Citation16,Citation34,Citation35 It was shown that 95.3% of pulmonary rehabilitation participants with COPD (mean FEV1 (%): 47.8±16.3) experienced high levels of physical fatigue.Citation36 In our previous study, we showed that 59% of the COPD patients aged 52–74 years had severe fatigue and their HRQoL scores, which were evaluated with St George’s Respiratory Questionnaire, were significantly higher.Citation33 Dyspnea, cough, and lack of energy were found to be the most prevalent symptoms in patients with COPD.Citation13 In a study that comprised 564 subjects with COPD, fatigue was found to be affected by respiratory symptoms and concomitant heart disease. In stage ≥ II COPD patients with respiratory symptoms (MMRC dyspnea score ≥2, chronic cough, chronic productive cough, or recurrent wheeze), there was an increased risk for clinically significant fatigue.Citation37 Increase in fatigue in COPD patients was found to be related to reduced time spent outdoors, and increase in depression and annual exacerbation frequency.Citation12 In a cross-sectional study with 130 moderate to severe patients with COPD, a strong relationship was found between fatigue and dyspnea. Dyspnea, depressed mood, and sleep quality explained 42% of the variance in subjective fatigue.Citation38 Because COPD exacerbations are episodes of sustained deterioration in respiratory symptoms due to increased systemic inflammation,Citation39 increase in cough severity and frequency in these exacerbation periods may decrease cough-specific quality of life and increase general impact of fatigue in physical, cognitive, and psychosocial daily life activities. In our study, increase in dyspnea and cough symptoms during exacerbation periods of patients who have maximum two exacerbations in 1 year, depressed mood, and adverse effects of chronic cough can explain relationship between fatigue perception and cough-specific quality of life. Similar to other studies in the literature, we have found a relationship between general fatigue and HRQoL.Citation40,Citation41 To the authors’ knowledge, this is the first study that determines the relation between fatigue perception and cough-specific quality of life.
In a study comprising 57 patients with chronic cough, 33% were identified as anxious while 16% experienced depression. Approximately, 48% of all coughers had moderate or high trait anxiety. In addition, patients’ mean scores on the phobic anxiety, somatization, depression, and obsession subscales were significantly higher than the published mean scores for healthy controls.Citation9 In 53% of the patient group consulting a specialty center for seeking evaluation and treatment of chronic cough, significant depressive symptoms and risk for clinical depression were shown. There was a statistically significant improvement in both cough severity and depression scores after 3 months among subjects followed up at 3 months. Improvement in cough score was found to be correlated significantly with improvement in depression score.Citation8 In another study population, 33.3% of COPD patients showed moderate to severe depressive symptoms. In addition, educational and occupational status, BMI, FEV1, respiratory symptoms, physical impairment, and dyspnea were found to be potential predictors of depression in COPD patients.Citation42 Depression and anxiety were significantly correlated with HRQoL at 1-year follow-up in a meta-analysis with six studies.Citation43 In our study, we found significant relationship between depression level and effects of cough on physical, social, and psychological subdimensions and general quality of life. Our findings in the study population, 32% of whom had moderate to severe depression level, are consistent with literature that reports high prevalence of depressive symptoms in patients with chronic cough and relationship between depression and HRQoL.Citation8,Citation9,Citation42,Citation43
We also found that the FIS total score and the number of sit-ups explain 58% of the variance in the LCQ total score. These findings suggest the important roles of general impact of fatigue on daily life and abdominal muscle endurance on overall cough-specific quality of life. To evaluate the impact of cough on patients and to assess the efficacy of cough treatments, investigators should use both subjective and objective methods because they have the potential to measure different aspects of cough. Subjective measures such as HRQoL instruments are likely to best reflect the severity of cough from the patient’s standpoint because a subjective response most likely integrates both cough frequency and intensity.Citation30,Citation44 Quality of life measures can be used to facilitate communication with patients and establish information regarding the range of problems affecting them. The impact of illness on health and treatment preferences often differ between patient and physician, and, therefore, quality of life considerations should take the patient’s perspective into account.Citation30 The LCQ is a brief, easy to administer, and well-validated chronic cough HRQoL questionnaire developed in the UKCitation45 and validated for Turkish population.Citation22
Limitations
There are several limitations to this study. The sampling was not strong enough to support the conclusions. In addition, fatigue perception questionnaire was not disease-specific.
Conclusion
In conclusion, this study showed that worse cough-specific quality of life is associated with lower abdominal muscle endurance; higher fatigue impact on physical, cognitive, and psychosocial activities; and higher depression level. Chronic cough can have profound effects on quality of life. Its management should include an assessment of health status. In the clinic of chest diseases and pulmonary rehabilitation programs, the LCQ can be used to assess longitudinal changes and identify the specific health domains affected in patients with COPD.Citation46 If cough is an important part of COPD and contributes to deterioration in quality of life, the symptom should be controlled.Citation4 Successful treatment of chronic cough was found to be associated with resolution of patients’ deterioration in HRQoL.Citation3,Citation47 We found in our study that the general impact of fatigue in daily life and abdominal muscle endurance may provide general information about the cough-specific quality of life. Using these FIS questionnares for fatigue perception and the sit-ups test for abdominal muscle endurance for the evaluation of patients with COPD with chronic cough can give us general idea about the patients’ quality of life and give rehabilitation professionals the opportunity to select the most appropriate therapeutic applications in the rehabilitative management of COPD patients.
Further work is required to determine the effects of pulmonary rehabilitation interventions on increasing abdominal muscle endurance and decreasing fatigue in COPD patients with chronic cough.
Acknowledgments
The authors thank Fusun Kalpaklioglu from Kirikkale University, Faculty of Medicine, Department of Allergy, Ankara, Turkey, for her permission to use Turkish version of Leicester Cough Questionnaire.
Disclosure
The authors have no financial disclosures to declare and no conflicts of interest to report.
References
- Goldcopd.org. Global Initiative for Chronic Obstructive Lung Disease (GOLD)Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease Available from: http://www.goldcopd.orgAccessed April 10, 2015
- FrenchCLIrwinRSCurleyFJKrikorianCJImpact of chronic cough on quality of lifeArch Intern Med1998158165716619701100
- FrenchCTIrwinRSFletcherKEAdamsTMEvaluation of a cough-specific quality-of life questionnaireChest20021211123113111948042
- ChungKFCalverleyPMACough in chronic obstructive pulmonary diseaseChungMWiddicombeJBousheyHCough: Causes, Mechanisms and Therapy1stUnited States of AmericaBlackwell Publishing2003125135
- MoriceAHFontanaGASovijarviARERS Task ForceThe diagnosis and management of chronic coughEur Respir J20042448149215358710
- BrignallKJayaramanBBirringSSQuality of life and psychosocial aspects of coughLung2008186S55S5817939003
- IrwinRSComplications of cough: ACCP evidence-based clinical practice guidelinesChest200612954S58S16428692
- DicpinigaitisPVTsoRBanauchGPrevalence of depressive symptoms among patients with chronic coughChest20061301839184317167006
- McGarveyLPACartonCGambleLAPrevalence of psychomorbidity among patients with chronic coughCough20062416780586
- ManWDHopkinsonNSHarrafFAbdominal muscle and quadriceps strength in chronic obstructive pulmonary diseaseThorax20056071872215923239
- Ramírez-SarmientoAOrozco-LeviMBarreiroEExpiratory muscle endurance in chronic obstructive pulmonary diseaseThorax20025713213611828042
- Baghai-RavaryRQuintJKGoldringJJDeterminants and impact of fatigue in patients with chronic obstructive pulmonary diseaseRespir Med200910321622319027278
- TheanderKHasselgrenMLuhrKSymptoms and impact of symptoms on function and health in patients with chronic obstructive pulmonary disease and chronic heart failure in primary health careInt J Chron Obstruct Pulmon Dis2014978579425071370
- GiftAGShepardCEFatigue and other symptoms in patients with chronic chronic obstructive pulmonary disease: do women and men differ?J Obstet Gynecol Neonatal Nurs199928201208
- PolleyLYamanNHeaneyLImpact of cough across different chronic respiratory diseases: comparison of two cough-specific health-related quality of life questionnairesChest200813429530218071022
- Calik-KutukcuESavciSSaglamMA comparison of muscle strength and endurance, exercise capacity, fatigue perception and quality of life in patients with chronic obstructive pulmonary disease and healthy subjects: a cross-sectional studyBMC Pulm Med201414624468029
- JetteDUManagoDMedvedEThe disablement process in patients with pulmonary diseasePhys Ther1997773853949105341
- BestallJCPaulEAGarrodRUsefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary diseaseThorax19995458158610377201
- MillerMRCrapoRHankinsonJATS/ERS Task ForceGeneral considerations for lung function testingEur Respir J20052615316115994402
- PellegrinoRViegiGBrusascoVATS/ERS Task ForceInterpretative strategies for lung function testsEur Respir J20052694896816264058
- AdamsGMExercise Physiology Laboratory Manual1st edDubuque, IAWm C Brown Publishers1990
- KalpakliogluAFKaraTKurtipekEEvaluation and impact of chronic cough: comparison of specific vs generic quality-of-life questionnairesAnn Allergy Asthma Immunol20059458158515945562
- BerkhofFFBoomLNten HertogNEThe validity and precision of the leicester cough questionnaire in COPD patients with chronic coughHealth Qual Life Outcomes201210422230731
- TheanderKCliffordsonCTorstenssonOJakobssonPUnossonMFatigue impact scale: its validation in patients with chronic obstructive pulmonary diseasePsychol Health Med20071247048417620211
- YilmazNGencozTAkMPsychometric properties of the defense style questionnaire: a reliability and validity studyTurk Psikiyatri Derg20071824425317853979
- GreenSBSalkindNJUsing SPSS for Windows and Macintosh: Analyzing and Understanding Data5th edUpper Saddle River, NJPrentice Hall2008
- DomholdtEPhysical Therapy Research: Principles and Applications1st edPhiladelphiaWB Saunders1993
- TabachnickBGFidellLSUsing Multivariate Statistics6th edBostonPearson2013
- IrwinRSFrenchCTFletcherKEQuality of life in coughersPulm Pharmacol Ther200215282286
- MoriceAHFontanaGABelvisiMGEuropean Respiratory Society (ERS)ERS guidelines on the assessment of coughEur Respir J2007291256127617540788
- WiddicombeJGA brief overview of the mechanisms of coughChungMWiddicombeJBousheyHCough: Causes, Mechanisms and TherapyUnited States of AmericaBlackwell Publishing20031723
- StephensREAddingtonWRMillerSPAndersonJWVideofluoroscopy of the diaphragm during voluntary and reflex cough in humansAm J Phys Med Rehabil20038238412704279
- Inal-InceDSavciSSaglamMFatigue and multidimensional disease severity in chronic obstructive pulmonary diseaseMultidiscip Respir Med2010516216722958301
- LewkoABidgoodPLGarrodREvaluation of psychological and physiological predictors of fatigue in patients with COPDBMC Pulm Med200994719845947
- KinsmanRAYaroushRAFenandezESymptoms and experience in chronic bronchitis and emphysemaChest1983837557616839816
- WongCJGoodridgeDMarciniukDDRennieDFatigue in patients with COPD participating in a pulmonary rehabilitation programInt J Chron Obstruct Pulmon Dis2010531933621037955
- StridsmanCMüllerovaHSkärLLindbergAFatigue in COPD and the impact of respiratory symptoms and heart disease – a population-based studyCOPD20131012513223547627
- KapelaMCLarsonJLPatelMKCoveyMKBerryJKSubjective fatigue, influencing variables, and consequences in chronic obstructive pulmonary diseaseNurs Res200655101716439924
- PereraWRHurstJRWilkinsonTMInflammatory changes, recovery and recurrence at COPD exacerbationEur Respir J200729527e3417107990
- BreslinEvan der SchansCBreukinkSPerception of fatigue and quality of life in patients with COPDChest19981149589649792561
- López-CamposJLImportance of fatigue, sleep quality and mood in patients with chronic obstructive pulmonary disease and the need for measurement instrumentsArch Bronconeumol200945Suppl 52620116755
- NegiHSarkarMRavalADPandeyKDasPPresence of depression & its risk factors in patients with chronic obstructive pulmonary diseaseIndian J Med Res201413940240824820834
- BlakemoreADickensCGuthrieEDepression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: systematic review and meta-analysisInt J Chron Obstruct Pulmon Dis2014950151224876770
- IrwinRSFrenchCLFletcherKEThe quality of life in coughersChungMWiddicombeJBousheyHCough: Causes, Mechanisms and TherapyUnited States of AmericaBlackwell Publishing20037579
- BirringSSPrudonBCarrAJDevelopment of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ)Thorax20035833934312668799
- SchmitKMCoeytauxRRGoodeAPEvaluating cough assessment tools: a systematic reviewChest20131441819182623928647
- ChamberlainSBirringSSGarrodRNonpharmacological interventions for refractory chronic cough patients: systematic reviewLung2014192758524121952