
Abstract
Purpose
To explore the association between host serum 25-hydroxyvitamin D (25(OH)D) and the susceptibility and severity of COPD.
Methods
Previous studies on the association between host 25(OH)D and the susceptibility and severity of COPD were collected on the basis of a systematic literature search of PubMed and Web of Science up to June 2015. Continuous variable data were presented as standard mean difference (SMD) or weighted mean difference with 95% confidence interval (CI). The dichotomous variable data were analyzed as relative ratio (RR) or odds ratio with 95% CI for cohort and case-control studies. A systematic review was conducted to understand the curative and side effects of vitamin D intake.
Results
A total of 18 studies including eight cohort, five case-control, and five randomized studies met the inclusion criteria. The serum level of 25(OH)D in COPD patients was comparable with controls with a pooled SMD of 0.191 (95% CI: −0.126 to 0.508, P=0.237) based on pooled analyses of cohort studies. However, the serum level of 25(OH)D in COPD patients was lower with a pooled SMD of 0.961 (95% CI: 0.476–1.446, P<0.001) compared with controls based on pooled analyses of case-control studies. The deficiency rates of 25(OH)D were comparable between controls and COPD patients with a pooled RR of 0.955 (95% CI: 0.754–1.211, P=0.705) based on analyses of cohort studies, and the same results were observed based on pooled analyses of case-control studies. Interestingly, the deficiency rate of 25(OH)D was significantly lower in moderate or severe COPD patients with a pooled RR of 0.723 (95% CI: 0.632–0.828, P<0.001) compared with that in mild COPD patients. The same results were obtained from the pooled analysis between moderate and severe COPD patients. The four randomized studies showed that vitamin D intake provided benefit for COPD patients.
Conclusion
Low serum levels of 25(OH)D were not associated with COPD susceptibility, but the high deficiency rate of 25(OH)D was associated with COPD severity. Vitamin D supplementation may prevent COPD exacerbation.
Keywords:
Introduction
COPD, a systemic inflammatory disease, is characterized by airflow limitation that is not fully reversible.Citation1 It has been estimated that the average prevalence of COPD is 6.2% in Asia and almost one-fifth of identified subjects are categorized as having severe COPD.Citation2 COPD is a major cause of chronic morbidity and mortalityCitation3 and is currently the fourth leading cause of death. The World Health Organization predicts that COPD will become the third leading cause of death worldwide by 2020.Citation3,Citation4 Due to multiple factors involved in the pathogenesis of COPD, the patterns of mechanisms and progression of COPD are extremely difficult to dissect. While it has been widely accepted that tobacco smoking is a major risk factor, a small number of long-term smokers develop symptomatic airflow obstruction.Citation5 Thus, lots of other factors might also play important roles in the morbidity and progression of COPD.
It has been reported that vitamin D is associated with bone health by affecting calcium homeostasis.Citation6,Citation7 However, some studies have also suggested that vitamin D is associated with the pathogenesis of a number of autoimmune diseasesCitation8,Citation9 as well as the development of cancer,Citation10 asthma,Citation11 and infections including respiratory infectionCitation12 and tuberculosis.Citation13 Vitamin D may be involved in the pathogenesis and affect the severity of COPD in several ways, such as reducing the frequency of respiratory infections, impairing response to pathogens, and inhibiting the proliferation of airway smooth muscle.Citation14 The main carrier of vitamin D metabolites is VDBP. The polymorphisms of VDBP gene have been associated with COPD and the serum level of 25-hydroxyvitamin D (25(OH)D).Citation15,Citation16 However, it has been reported that low levels of 25(OH)D was not consistent with vitamin D deficiency.Citation17 Two cohort studies suggested that vitamin D was not associated with COPD based on the observation that the serum levels of 25(OH)D were comparable between healthy subjects and COPD patients.Citation18,Citation19 However, this conclusion was questioned by other studies.Citation20,Citation21
In the present study, we conducted a meta-analysis to evaluate the association between the serum level of 25(OH)D and the susceptibility and severity of COPD. We focused on four aspects: 1) the serum level of 25(OH)D between controls and COPD patients; 2) the deficiency rates of 25(OH)D between controls and COPD patients; 3) the deficiency rates of 25(OH)D in mild, moderate, and severe COPD patients; and 4) the curative effect of supplying vitamin D for COPD patients.
Materials and methods
Literature retrieval
Computerized searches in the National Center for Biotechnology Information PubMed and Web of Science were conducted by two authors (Biyuan Zhu and Biqing Zhu). The search time window was up to June 2015 and all articles searched for were in English. The following keywords were used for literature searching: “COPD” or “chronic obstructive pulmonary disease” combined with “vitamin d”, “vit d”, “cholecalciferol”, or “hydroxyvitamin. We also manually searched the reference lists of the retrieved articles to identify additional qualified studies.
Definitions
COPD patients exhibited stable COPD and acute exacerbation COPD. The severity of COPD was defined on the basis of percentage of the forced expiratory volume in 1 second predicted according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria.Citation3,Citation22–Citation25 The controls were healthy or patients without COPD. Patients with plasma level of 25(OH)D less than 20 ng/mL (50 nmol/L) were categorized into the 25(OH)D deficiency group.Citation6,Citation20
Inclusion and exclusion criteria
Studies were included into the present meta-analysis based on the following criteria. To analyze the serum level of 25(OH)D in controls and COPD patients: 1) the study reported the serum level of 25(OH)D with patient number, mean, and standard deviation and 2) the study included controls (healthy or patients without COPD). To investigate the deficiency rates of 25(OH)D in controls and COPD patients, the study reported the deficiency rate of 25(OH)D in COPD patients and controls. To study the deficiency rates of 25(OH) D in mild, moderate, and severe COPD patients, the study reported the deficiency rates of 25(OH)D in COPD patients and included the severity of COPD (mild, moderate, and severe). To analyze the curative effects of supplying vitamin D for COPD patients: 1) randomized clinical trials were included; and 2) the curative and side effects of vitamin D intake were analyzed. Studies of reviews, in vitro and animal experiments, and comments were excluded from the present meta-analysis.
Quality assessment
The quality of the observational studies was independently assessed by two authors (Biyuan Zhu and Chaolie Xiao) using the Newcastle–Ottawa Scale (NOS).Citation26 Three parameters of quality, including selection, comparability, and exposure/outcome assessments were used in NOS. Studies of low, intermediate, and high-quality studies were defined as NOS scores of 1–3, 4–6, and 7–9, respectively.Citation27 The quality of randomized studies was assessed using the Jadad scoreCitation28 that was rated on a scale of 0–5 according to the presence of three features: randomization, blinding, and patient accountability. A higher-quality trial was defined as a study with a Jadad score ≥3. Discrepancies were resolved by consensus after joint reevaluation of the original studies by a third author (Zhiwen Zheng).
Data extraction
Data were independently extracted by two reviewers (Biyuan Zhu and Chaolie Xiao) and validated by a third reviewer (Zhiwen Zheng). For each eligible study, we extracted first author names, publication year, country, study design, numbers of patients with COPD and controls, and the serum level of 25(OH)D (mean ± standard deviation).
Statistical analyses
Meta-analysis was performed in STATA 11.0 (StataCorp LP, College Station, TX, USA). Continuous variable data (controls versus COPD patients) were presented as standard mean difference (SMD) or weighted mean difference with 95% confidence interval (CI). Dichotomous variable data (controls versus COPD patients, mild versus moderate/severe COPD patients, and moderate versus severe COPD patients) were presented as relative ratio (RR) or odds ratio (OR) with 95% CI for cohort and case-control studies. In the forest plots, the pooled SMD or weighted mean difference >0 represented the higher level of 25(OH)D in controls, and RR or OR <1 represented the lower deficiency rates in controls, mild COPD patients, and severe COPD patients, respectively. A chi-squared test was used to assess the heterogeneity. I2 value <25% was regarded as no heterogeneity. Fixed effects model was used when no significant heterogeneity was identified among the studies analyzed. Random-effects model was performed when significant heterogeneity was identified among the studies analyzed. The publication bias was also evaluated. A P-value <0.05 was considered to be significant on two-sides.
Results
Study search
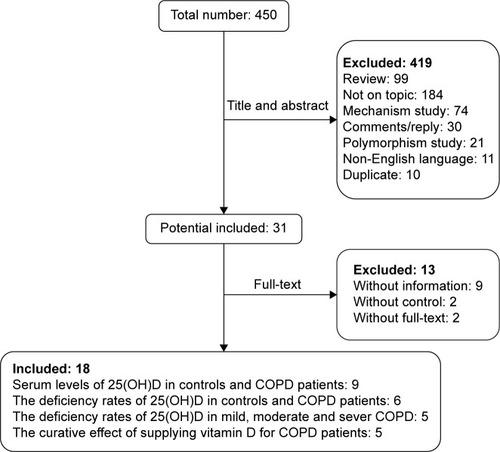
Based on the aforementioned search strategies, a total of 450 articles were collected. After removal of review articles (n=99), studies not related with the topic (n=196), commentary articles (n=30), and others (n=94), 31 studies were identified for further evaluation. In addition, 13 studies without controls (n=2), lacking essential information (n=9), or without full text (n=2) were excluded. Finally, 18 studies that met the inclusion criteria were included in the present meta-analysis. A flowchart of the search and selection process is shown in .
Figure 1 A flowchart of identified studies.
Nine studies containing 919 controls and 990 COPD patients were included to analyze the serum levels of 25(OH)D between controls and COPD patients (). Among these nine studies, five were case-control studiesCitation29–Citation33 and four were cohort studies.Citation18–Citation20,Citation34 Five studies were of high quality because their NOS scores were not less than 7.Citation19,Citation20,Citation29,Citation31,Citation34 Six studies containing 6,375 controls and 2,504 COPD patients were included to analyze the deficiency rates of 25(OH)D in controls and COPD patients (). Among these six studies, two were case-control studiesCitation30,Citation33 and four were cohort studies.Citation19–Citation21,Citation34 Five studies were of high quality because their NOS scores were not less than 7.Citation19,Citation20,Citation29,Citation31,Citation34 Five cohort studies were retrieved to analyze the deficiency rates of 25(OH)D in mild, moderate, and severe COPD patients (). Among the five studies, three studiesCitation20,Citation21,Citation35 contained 1,026 mild and 1,298 moderate/severe COPD patients and four studiesCitation20,Citation35–Citation37 contained 435 moderate and 494 severe COPD patients. Three studies with NOS scores not less than 7 were considered as studies of high quality.Citation20,Citation21,Citation36 Five randomized studies,Citation38–Citation41 containing 296 patients with placebo and 300 patients with vitamin D, were included to analyze the curative effect of supplying vitamin D for COPD patients (). According to Jada scores, one study with a score of 1 was considered as a low-quality study.Citation40
Table 1 Included studies for the serum levels of 25(OH)D
Table 2 Included studies for deficiency rate of 25(OH)D
Table 3 Included studies for curative effect and safety of vitamin D intake
Meta-analysis of the serum level of 25(OH)D
A random-effects model for meta-analysis was used to compare the serum level of 25(OH)D between controls and COPD patients. The results suggested that the serum level of 25(OH)D in COPD patients was significantly lower than that in controls based on a pooled SMD of 0.596 (95% CI: 0.305–0.886, P<0.001) compared with controls (). A significant heterogeneity with I2=88.5, P<0.001, and a publication bias were identified based on the Egger’s test of 0.372 (P=0.046).
Figure 2 Forest plots of the serum level of 25(OH)D in the controls and COPD patients.
Abbreviations: CI, confidence interval; FEV1%pred, forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) predicted; SMD, standard mean difference.
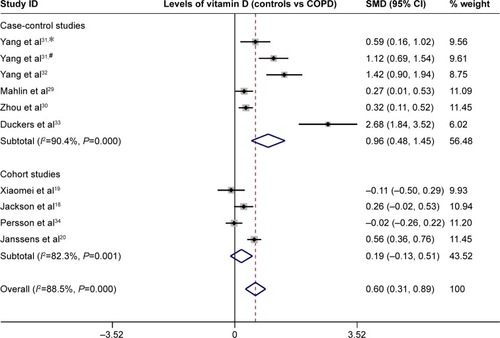
According to the study design, the results of sensitivity analysis were different. The serum level of 25(OH)D in COPD patients was comparable with controls with a pooled SMD of 0.191 (95% CI: −0.126 to 0.508, P=0.237) based on pooled analyses of cohort studies (). No publication bias was identified based on the Egger’s test of 0.235 (P=0.322). However, the serum level of 25(OH)D in COPD patients was lower than that in controls with a pooled SMD of 0.961 (95% CI: 0.476–1.446, P<0.001) based on pooled analyses of case-control studies (). A publication bias was identified based on the Egger’s test of 0.085 (P=0.006).
Meta-analysis of the deficiency rates of 25(OH)D
A random-effects model for meta-analysis was conducted to analyze the deficiency rate of 25(OH)D in controls and COPD patients. The results suggested that the deficiency rate of 25(OH)D was comparable between these two groups with a pooled RR of 0.955 (95% CI: 0.754–1.211, P=0.705) based on pooled analyses of cohort studies (). A significant heterogeneity was identified with I2=72.2, P=0.013, and this result showed no publication bias based on the Egger’s test of 0.216 (P=0.296). The same result was observed in the pooled analysis of case-control studies. No significant difference in the deficiency rate of 25(OH)D was identified between these two groups based on a fixed-effect meta-analysis with a pooled RR of 0.899 (95% CI: 0.678–1.192, P=0.46) (). In addition, no significant heterogeneity was identified with I2 of 0 (P=0.706). The publication bias was not be determined because only two studies were analyzed.
Figure 3 Forest plots of the deficiency rate of serum 25(OH)D.
Abbreviations: 25(OH)D, 25-hydroxyvitamin D; CI, confidence interval; RR, relative ratio.
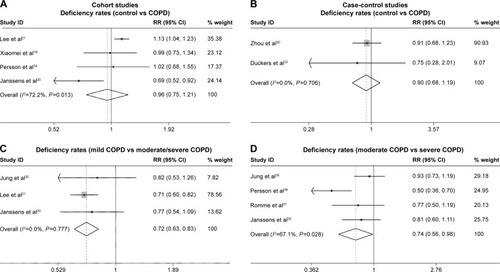
In addition, the deficiency rate of 25(OH)D between mild, moderate, and severe COPD patients was analyzed. A fixed-effect meta-analysis showed that the deficiency rate of 25(OH) D in moderate/severe COPD patients was significantly lower than that in mild COPD patients with a pooled RR of 0.723 (95% CI: 0.632–0.828, P<0.001) (). No significant heterogeneity with I2 of 0 (P=0.777) and no publication bias was observed based on the Egger’s test of 0.018 (P=0.069). A random-effects model for meta-analysis between moderate and severe COPD patients showed the same results.Citation20,Citation35–Citation37 The deficiency rate of 25(OH)D in severe COPD patients was significantly lower than that in moderate COPD patients with a pooled RR of 0.743 (95% CI: 0.561–0.984, P=0.038) (). Significant heterogeneity was observed with I2 of 67.1 (P=0.028) and no publication bias was identified based on the Egger’s test of 0.749 (P=0.548).
Systematic analysis of the curative effects of vitamin D supplement
Five randomized studies were included for systematic analysis of the curative effects of vitamin D supplement in COPD patients (). Four studies showed that vitamin D intake benefited COPD patients.Citation9,Citation38,Citation39,Citation41 One of the four reporters suggested that vitamin D intake inhibited COPD exacerbation among severe patients,Citation41 and one showed that patients with vitamin D intervention had significant improvements in inspiratory muscle strength and maximal oxygen uptake.Citation39 The other two studies demonstrated that vitamin D protected against exacerbation in patients with a baseline serum level of 25(OH)D less than 20 ng/mL.Citation9,Citation38 Only the study conducted by Bjerk et al reported that there was no obvious benefit for severe COPD patients with vitamin D supplement based on two questionnaire scores (Short Physical Performance Battery and St George’s Respiratory Questionnaire).Citation40 Generally, vitamin D intake was a safe approach without severe side effects for COPD patients based on most studies.
Discussion
The critical extra-skeletal effects of vitamin D has been widely recognized in recent years,Citation6 particularly its roles in chronic diseases such as the chronic lung disease COPD. Several studies have reported that VDBP genotype was associated with high COPD susceptibility,Citation15,Citation42,Citation43 suggesting that the serum level of 25(OH)D was linked with COPD susceptibility. However, VDBP level had no effects on serum 25(OH)D concentration.Citation44 Thus, this analysis was conducted to evaluate the association between the serum levels of 25(OH)D and the susceptibility and severity of COPD.
While the pooled results of nine studies demonstrated significant difference in the serum level of 25(OH)D between the controls and COPD patients, heterogeneity and publication bias were identified. The significant difference in the serum level of 25(OH)D between the controls and COPD patients was not identified based on the pooled analysis of cohort studies. More importantly, the deficiency rate of 25(OH)D was also comparable between these two groups based on pooled RR with cohort studies and pooled OR with case-control studies, in which much higher number of controls and patients were included. In addition, no publication bias was identified in these analyses, suggesting the high confidence of these results. While the serum level of 25(OH)D was not associated with COPD, serum deficiency of 25(OH)D (<20 ng/mL) was significantly associated with COPD severity based on the meta-analyses between mild and moderate/severe COPD as well as moderate and severe COPD. These results suggested that the low serum level of 25(OH)D was not associated with COPD susceptibility; however, high deficiency of 25(OH)D was associated with COPD severity. Although vitamin D deficiency may be a consequence rather than the cause of COPD,Citation45 the evidence was not sufficient.
It has been shown that vitamin D intake inhibited asthma exacerbationsCitation45 and accelerated clinical and radiographic improvement in tuberculosis patients.Citation46 Our results showed that vitamin D supplement inhibited COPD exacerbation and improved inspiratory muscle strength and maximal oxygen uptake in severe COPD patients. In addition, vitamin D prevents COPD exacerbation in patients with baseline serum 25(OH)D concentrations of less than 20 ng/mL. Given that serum 25(OH)D deficiency was mainly observed in severe COPD patients, the protective effects of 25(OH)D in severe COPD patients was compared with that in mild COPD patients. While our results are not consistent with the study conducted by Bjerk et alCitation40 our conclusion was not influenced. First, a limited number of patients (n=36) were included in that study. Second, vitamin D was supplied at a dose of 2,000 IU per day and once daily for 6 weeks, which was much less than the dose used in other studies (). Several potential mechanisms could explain vitamin D deficiency in severe COPD patients. First, the evidence from epidemiological studies showed that vitamin D deficiency is a risk factor for respiratory infection.Citation47,Citation48 Second, it has been hypothesized that the changes of airway smooth muscle was the sole manifestation of vitamin D deficiency.Citation49 Third, the positive association between the high level of vitamin D at birth and total and inhalant allergen-specific IgE may be attributable to a different mechanism.Citation50 Thus, vitamin D supplementation may significantly alleviate COPD.
Our meta-analysis has several limitations. First, the studies exploring the relationship between 25(OH)D and COPD or COPD severity were lacking in relation to African ethnicity as only one study contained African ethnicity.Citation21 Second, some meta-analysis results were based on random-effects model which may not be strong, and publication bias was identified in the meta-analysis. While systematic analysis of the curative effects of vitamin D supplement was analyzed on the randomized studies, the dose and treatment duration of vitamin D supplementation varied, and distinct indicators of treatment effects were used in different studies. Thus, more studies should be performed for better understanding of the role of vitamin D in COPD patients.
Conclusion
In conclusion, our results suggest that the low serum level of 25(OH)D was not associated with COPD susceptibility, but the high rate of 25(OH)D deficiency was associated with COPD severity. Vitamin D supplementation can inhibit COPD exacerbation.
Author contributions
Biyuan Zhu, Biqing Zhu, and Chaolie Xiao collected the data and did the statistical analysis. Biyuan Zhu and Biqing Zhu wrote the article. Chaolie Xiao revised the article. Zhiwen Zheng contributed to the conception and design of the study and revised the article.
Disclosure
The authors report no conflict of interests in this work.
References
- DecramerMJanssensWMiravitllesMChronic obstructive pulmonary diseaseLancet20123791341135122314182
- LimSLamDCMuttalifARImpact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: the EPIC Asia population-based surveyAsia Pac Fam Med201514425937817
- PauwelsRABuistASCalverleyPMJenkinsCRHurdSSGOLD Scientific CommitteeGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summaryAm J Respir Crit Care Med200116351256127611316667
- LopezADShibuyaKRaoCChronic obstructive pulmonary disease: current burden and future projectionsEur Respir J20062739741216452599
- FanerRGonzalezNCruzTKalkoSGAgustíASystemic inflammatory response to smoking in chronic obstructive pulmonary disease: evidence of a gender effectPLoS One20149e9749124830457
- HolickMFVitamin D deficiencyN Engl J Med200735726628117634462
- Bischoff-FerrariHAGiovannucciEWillettWCDietrichTDawson-HughesBEstimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomesAm J Clin Nutr200684182816825677
- HaroonMFitzgeraldOVitamin D and its emerging role in immunopathologyClin Rheumatol20123119920222020389
- LehouckAMathieuCCarremansCHigh doses of vitamin D to reduce exacerbations in chronic obstructive pulmonary disease: a randomized trialAnn Intern Med201215610511422250141
- GarlandCFGarlandFCGorhamEDThe role of vitamin D in cancer preventionAm J Public Health20069625226116380576
- LitonjuaAAWeissSTIs vitamin D deficiency to blame for the asthma epidemic?J Allergy Clin Immunol20071201031103517919705
- GindeAAMansbachJMCamargoCAJrAssociation between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination SurveyArch Intern Med200916938439019237723
- Arnedo-PenaAJuan-CerdánJVRomeu-GarcíaMAVitamin D status and incidence of tuberculosis infection conversion in contacts of pulmonary tuberculosis patients: a prospective cohort studyEpidemiol Infect20151431731174125274036
- PfefferPEHawrylowiczCMVitamin D and lung diseaseThorax2012671018102022935474
- HoritaNMiyazawaNTomaruKInoueMIshigatsuboYKanekoTVitamin D binding protein genotype variants and risk of chronic obstructive pulmonary disease: a meta-analysisRespirology20152021922525488093
- PoweCEKarumanchiSAThadhaniRVitamin D-binding protein and vitamin D in blacks and whitesN Engl J Med201437088088124571762
- PoweCEEvansMKWengerJVitamin D-binding protein and vitamin D status of black Americans and white AmericansN Engl J Med20133691991200024256378
- JacksonASShrikrishnaDKellyJLVitamin D and skeletal muscle strength and endurance in COPDEur Respir J20134130931622556020
- XiaomeiWHangXLinglingLXuejunLBone metabolism status and associated risk factors in elderly patients with chronic obstructive pulmonary disease (COPD)Cell Biochem Biophys20147012913424633456
- JanssensWBouillonRClaesBVitamin D deficiency is highly prevalent in COPD and correlates with variants in the vitamin D-binding geneThorax20106521522019996341
- LeeHMLiuMLeeKLuoYWongNDDoes low vitamin D amplify the association of COPD with total and cardiovascular disease mortality?Clin Cardiol20143747347824719373
- EaganTMUelandTWagnerPDSystemic inflammatory markers in COPD: results from the Bergen COPD Cohort StudyEur Respir J20103554054819643942
- DonaldsonGCSeemungalTABhowmikAWedzichaJARelationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax20025784785212324669
- RabeKFHurdSAnzuetoAGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med200717653255517507545
- FabbriLMHurdSSGOLD Scientific CommitteeGlobal Strategy for the Diagnosis, Management and Prevention of COPD: 2003 updateEur Respir J2003221212882441
- WellsGASheaBO ConnellDThe Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses2000 Available from : http://www.medicine.mcgill.ca/rtamblyn/Readings/The%20Newcastle%20-%20Scale%20for%20assessing%20the%20quality%20of%20nonrandomised%20studies%20in%20meta-analyses.pdfAccessed August 31, 2015
- ZhangHZhouYPPengHJPredictive symptoms and signs of severe dengue disease for patients with dengue fever: a meta-analysisBiomed Res Int2014201435930825097856
- JadadARMooreRACarrollDAssessing the quality of reports of randomized clinical trials: is blinding necessary?Control Clin Trials1996171128721797
- MahlinCvon SydowHOsmancevicAVitamin D status and dietary intake in a Swedish COPD populationClin Respir J20148243223711108
- ZhouXHanJSongYZhangJWangZSerum levels of 25- hydroxyvitamin D, oral health and chronic obstructive pulmonary diseaseJ Clin Periodontol20123935035622296704
- YangYMGuoYFZhangHSSunTYAntimicrobial peptide LL-37 circulating levels in chronic obstructive pulmonary disease patients with high risk of frequent exacerbationsJ Thorac Dis2015774074525973241
- YangHLongFZhangY1α,25-Dihydroxyvitamin D3 Induces Neutrophil Apoptosis through the p38 MAPK Signaling Pathway in Chronic Obstructive Pulmonary Disease PatientsPLoS One201510e012051525905635
- DuckersJMEvansBAFraserWDStoneMDBoltonCEShaleDJLow bone mineral density in men with chronic obstructive pulmonary diseaseRespir Res20111210121812978
- PerssonLJAanerudMHiemstraPSHardieJABakkePSEaganTMChronic obstructive pulmonary disease is associated with low levels of vitamin DPLoS One20127e3893422737223
- JungJYKimYSKimSKRelationship of vitamin D status with lung function and exercise capacity in COPDRespirology201520578278925868752
- PerssonLJAanerudMHiemstraPSVitamin D, vitamin D binding protein, and longitudinal outcomes in COPDPLoS One201510e012162225803709
- RommeEARuttenEPSmeenkFWSpruitMAMenheerePPWoutersEFVitamin D status is associated with bone mineral density and functional exercise capacity in patients with chronic obstructive pulmonary diseaseAnn Med201345919622462562
- MartineauARJamesWYHooperRLVitamin D3 supplementation in patients with chronic obstructive pulmonary disease (ViDiCO): a multicentre, double-blind, randomised controlled trialLancet Respir Med2015312013025476069
- HornikxMVan RemoortelHLehouckAVitamin D supplementation during rehabilitation in COPD: a secondary analysis of a randomized trialRespir Res2012138423006613
- BjerkSMEdgingtonBDRectorTSKunisakiKMSupplemental vitamin D and physical performance in COPD: a pilot randomized trialInt J Chron Obstruct Pulmon Dis201389710423430315
- ZendedelAGholamiMAnbariKGhanadiKBachariECAzargonAEffects of Vitamin D Intake on FEV1 and COPD Exacerbation: A Randomized Clinical Trial StudyGlob J Health Sci2015724324825946929
- XieXZhangYKeRVitamin D-binding protein gene polymorphisms and chronic obstructive pulmonary disease susceptibility: A meta-analysisBiomed Rep2015318318825798246
- XiaoMWangTZhuTWenFDual role of vitamin D-binding protein 1F allele in chronic obstructive pulmonary disease susceptibility: a meta-analysisGenet Mol Res2015143534354025966120
- PondaMPMcGeeDBreslowJLVitamin D-binding protein levels do not influence the effect of vitamin D repletion on serum PTH and calcium: data from a randomized, controlled trialJ Clin Endocrinol Metab2014992494249924712573
- FoongREZoskyGRVitamin D deficiency and the lung: disease initiator or disease modifier?Nutrients201352880290023896653
- SalahuddinNAliFHasanZRaoNAqeelMMahmoodFVitamin D accelerates clinical recovery from tuberculosis: results of the SUCCINCT Study [Supplementary Cholecalciferol in recovery from tuberculosis]. A randomized, placebo-controlled, clinical trial of vitamin D supplementation in patients with pulmonary tuberculosis’Bmc Infect Dis2013132223331510
- UrashimaMSegawaTOkazakiMKuriharaMWadaYIdaHRandomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildrenAm J Clin Nutr2010911255126020219962
- CamargoCAJrInghamTWickensKCord-blood 25- hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthmaPediatrics2011127e180e18721187313
- GuptaASjoukesARichardsDRelationship between serum vitamin D, disease severity, and airway remodeling in children with asthmaAm J Respir Crit Care Med20111841342134921908411
- WittkeAWeaverVMahonBDAugustACantornaMTVitamin D receptor-deficient mice fail to develop experimental allergic asthmaJ Immunol20041733432343615322208