
Abstract
Arbekacin sulfate (ABK), an aminoglycoside antibiotic, was discovered in 1972 and was derived from dibekacin to stabilize many common aminoglycoside modifying enzymes. ABK shows broad antimicrobial activities against not only Gram-positive bacteria including methicillin-resistant Staphylococcus aureus (MRSA) but also Gram-negative bacteria such as Escherichia coli, Pseudomonas aeruginosa, and Klebsiella pneumoniae. ABK has been approved as an injectable formulation in Japan since 1990, under the trade name Habekacin, for the treatment of patients with pneumonia and sepsis caused by MRSA. The drug has been used in more than 250,000 patients, and its clinical benefit and safety have been proven over two decades. ABK currently shows promise for the application for the treatment of multidrug-resistant Gram-negative bacterial infections such as multidrug-resistant strains of P. aeruginosa and Acinetobacter baumannii because of its synergistic effect in combination with beta-lactams.
Introduction
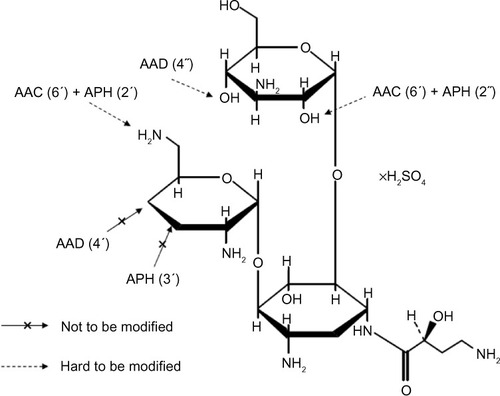
Arbekacin (ABK) (Meiji Seika Pharma Co, Ltd, Tokyo, Japan) has the hydroxy amino-butyryl group as its chemical structure and is classified as a kanamycin family aminoglycoside ().Citation1 ABK causes membrane damage and binds both to the 50S and the 30S ribosomal subunits, resulting in codon misreading and inhibition of translation.Citation2 ABK is not inactivated by aminoglycoside-inactivating enzymes such as (3′) aminoglycoside-phosphotransferase (APH), (4′) aminoglycoside-adenyltransferase (AAD), or AAD (2″) and has a weak affinity for (6′-IV) aminoglycoside-acetyltransferase (AAC). Therefore, ABK exhibits antimicrobial activity against Gram-positive and -negative pathogens including strains resistant to gentamicin (GM), tobramycin (TOB), and amikacin (AMK). In particular, ABK has strong antimicrobial potency against methicillin-resistant Staphylococcus aureus (MRSA) and has been used in Japan since 1990 under the trade name Habekacin (Meiji Seika Pharma Co., Ltd. Tokyo, Japan), to treat sepsis and pneumonia caused by MRSA. In addition, Habekacin has also been used in Korea since 2000.
Figure 1 Structural formula of arbekacin sulfate.
Principal pharmacology (in vitro antibacterial activities)
ABK showed strong antimicrobial activity against Gram-positive bacteria such as S. aureusCitation3 and Staphylococcus epidermidis.Citation4 Antibacterial activities of ABK, GM, TOB, and AMK against 54 methicillin-susceptible S. aureus clinical isolates were determined and the results are shown in .Citation3 The minimal inhibitory concentration (MIC) for 90% of the organisms (MIC90) of ABK was 1 μg/mL, whereas MIC90 of GM, TOB, and AMK were 4, 8, and 16 μg/mL, respectively.Citation3 Furthermore, the MIC90 of ABK against S. epidermidis was 0.5 μg/mL and it was stronger than that of AMK (MIC90 4 μg/mL).Citation4 ABK also has superior antibacterial activity against Gram-negative bacteria including Pseudomonas aeruginosa.Citation3,Citation5
Table 1 In vitro antibacterial activity against aerobic bacteria
The antibacterial activities of ABK against strains producing aminoglycoside-inactivating enzymes were investigated as well as the antibacterial activities of ABK against tested organisms without the influence of aminoglycoside-inactivating enzymes.Citation6 The bactericidal effects of ABK against S. aureus and Escherichia coli were better than those of AMK and GM, and the bactericidal effects against Klebsiella pneumoniae and P. aeruginosa were comparable with AMK and GM.Citation7
Stability to aminoglycoside-inactivating enzymes
ABK was stable to the aminoglycoside-inactivating enzymes produced by MRSA, such as APH, AAD, and AAC.Citation8 Although GM, AMK, TOB, and kanamycin (KM) were completely inactivated by APH (2″), ABK still showed about 50% activity against APH (2″). Furthermore, ABK was not inactivated by AAD (4′) and APH (3′), and also showed stability to these enzymes. These results suggest the excellent antibacterial activities of ABK against MRSA strains.
Antibacterial activity against MRSA
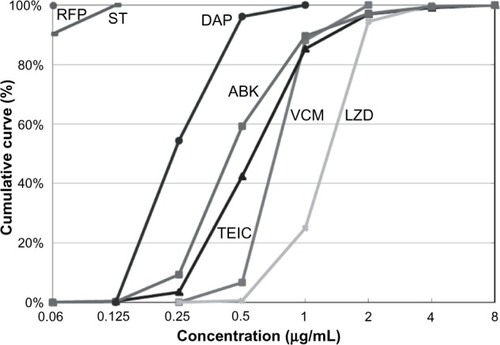
ABK showed the most potent antibacterial effect against clinically isolated MRSA strains among the tested aminoglycosides (GM, TOB, and AMK), and the antibacterial effect of ABK was equivalent to that of vancomycin (VCM).Citation3,Citation9–Citation12 shows the cumulative percentage of MIC against MRSA with the antimicrobial susceptibility surveillance conducted in Japan.Citation9–Citation12 The antimicrobial activity of ABK was more potent than the other anti-MRSA drugs except daptomycin.
Figure 2 Antibacterial activity against MRSA.
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; VCM, vancomycin; TEIC, teicoplanin; ABK, arbekacin; LZD, linezolid; ST, sulfamethoxazole-trimethoprim; RFP, rifampicin; DAP, daptomycin.
The susceptibility of MRSA to ABK has not changed since 1990 when ABK was launched. In another surveillance, the MICs of ABK, VCM, teicoplanin (TEIC), and linezolid (LZD) against 228 MRSA clinical isolates in Japan were determined. The results showed that MIC90/MIC50 of VCM and ABK had not significantly changed in the period from 1990 to 2006 even though MIC90 of TEIC and LZD were slightly increased during the period.Citation13
Bactericidal effect of ABK against MRSA
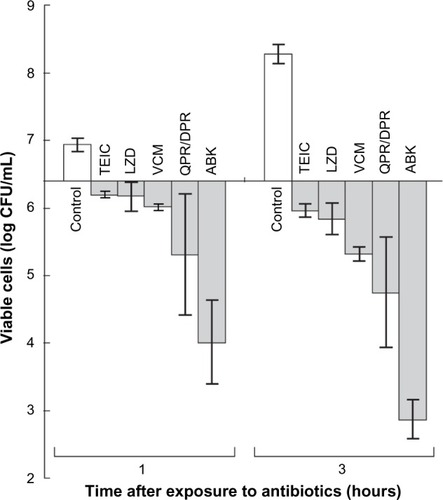
ABK also shows concentration-dependent bactericidal activity.Citation14–Citation18 Viable counts of MRSA were rapidly decreased in a short period after the addition of ABK in comparison with those of VCM, TEIC, and LZD ().Citation18
Figure 3 Bactericidal activity of anti-MRSA agents against five MRSA strains.
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; TEIC, teicoplanin; LZD, linezolid; VCM, vancomycin; QPR/DPR, quinupristin/dalfopristin; ABK, arbekacin; SD, standard deviation; CFU, colony forming units.
Post antibiotic effect of ABK
Post antibiotic effect is another characteristic of aminoglycoside antibiotics. When MRSA was treated either with ABK or VCM with the same concentration, the bactericidal activity of VCM was weaker than ABK, and the post antibiotic effect was shorter compared with ABK.Citation14
Inhibition of toxic shock syndrome toxin-1 (TSST-1) by ABK
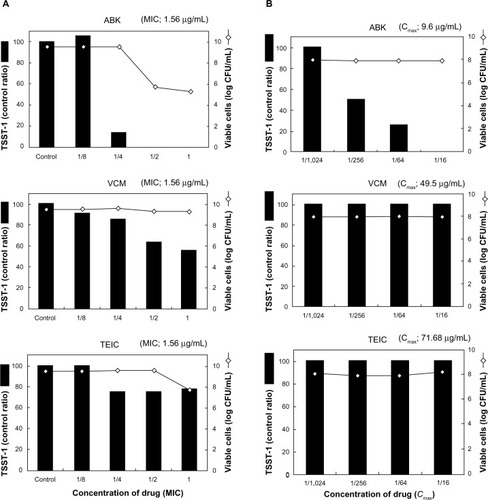
The effect of ABK, VCM, and TEIC on the production of TSST-1 by MRSA strains has been reported.Citation19 In logarithmic phase cultures, ABK, VCM, and TEIC inhibited TSST-1 production by 85, 10, and 25%, respectively, at the concentration of one fourth of each MIC ().
Figure 4 Effect of TSST-1 producing ability of MRSA.
Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; ABK, arbekacin; VCM, vancomycin; TEIC, teicoplanin; TSST-1, toxic shock syndrome toxin-1; CFU, colony forming units; MIC, minimal inhibitory concentration; Cmax, maximum concentration.
Antibacterial activities against multidrug-resistant P. aeruginosa
Multidrug-resistant strains of P. aeruginosa have been an important issue and the strains with the MICs of AMK ≥32 μg/mL, imipenem ≥16 μg/mL, and ciprofloxacin ≥4 μg/mL are defined as multidrug-resistant P. aeruginosa (MDRP) in Japan. It is difficult to treat patients with MDRP infections and colistin (CL) may be a good candidate for treatment. Because CL is not approved for clinical use in Japan, many doctors in Japan are interested in combination therapy such as beta-lactam antibiotics and aminoglycoside antibiotics.
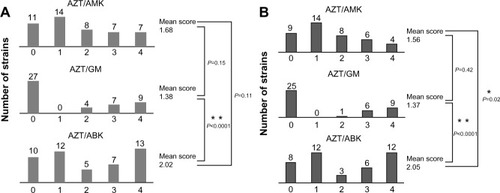
Antibiotic combination therapy study groups studied the effective combination regimen against MDRP and demonstrated that ABK plus aztreonam (AZT) was the most promising combination, the other promising regimens were AZT plus AMK and AZT plus GM ().Citation20
Figure 5 Scoring of combination effect for each drug combination against multidrug-resistant (MDR) Pseudomonas aeruginosa strains.
Abbreviations: MDRP, multidrug-resistant Pseudomonas aeruginosa; AZT, aztreonam; AMK, amikacin; GM, gentamicin; ABK, arbekacin.
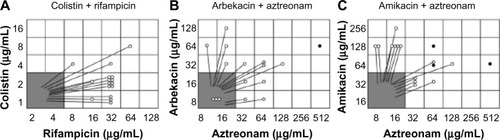
Antibiotic combination therapy study groups also reported that a combination of ABK plus AZT showed synergistic effects as well as the combinations of CL plus rifampin, and AMK plus AZT ().Citation21 These results suggest that ABK is a useful agent for MDRP infections used in combination therapies.
Figure 6 Results of Break-point Checkerboard Plate for (A) colistin plus rifampicin, (B) arbekacin plus aztreonam and (C) amikacin plus aztreonam.
Antibacterial activities against multidrug-resistant Acinetobacter baumannii-calcoaceticus
Recently, ABK has also attracted attention for its antibacterial effect against A. baumannii-calcoaceticus. Zapor et alCitation22 examined the in vitro antibacterial activity of ABK against A. baumannii-calcoaceticus isolated from clinical specimens at The Walter Reed Army Medical Center during the Global War on Terrorism. Additionally, the in vitro MIC of ABK against 200 Acinetobacter baumannii-calcoacetics isolates recovered from wounded soldiers was determined. The median MIC was 2 μg/mL (range: 0.5 to >64 μg/mL). A total of 97.5% of the isolates had ABK MICs of <8 μg/mL and 86.5% had MICs of <4 μg/mL. There was no association between the ABK MIC and susceptibility to 16 other antibiotics or the specimen source. Moreover, synergy testing suggested an enhanced effect of ABK-carbapenem combinations.Citation22
Efficacy in mouse mixed infection model (in vivo)
Since ABK has shown potent activities against both MRSA and P. aeruginosa, the effect of ABK in a mixed infection model using MRSA and P. aeruginosa was investigated. The median effect dose (ED50) that calculated the life and death on 7 days after administration was 19.5 mg/kg for ABK and >100 mg/kg for VCM. Thus, ABK showed a protective polymicrobial effect on MRSA and P. aeruginosa infections.Citation23
Pharmacokinetics in adults
A multi-center collaborative open clinical study was conducted in patients infected with MRSA to evaluate the efficacy, safety, and the pharmacokinetics-pharmacodynamics (PK-PD) of ABK. The patients were administered 200 mg of ABK once daily, and the patients with severe renal dysfunction (creatinine clearance ≥80 mL/min) showed changes in the pharmacokinetic parameters such as prolongation of half-life, decrease of total clearance, and increase of area under the curve (0–24 hr) (AUC0–24) ( and ).Citation24
Figure 7 Plasma (serum) concentration after administration of ABK.
Abbreviations: ABK, arbekacin; MRSA, methicillin-resistant Staphylococcus aureus; SD, standard deviation; Ccr, creatinine clearance (mL/min).
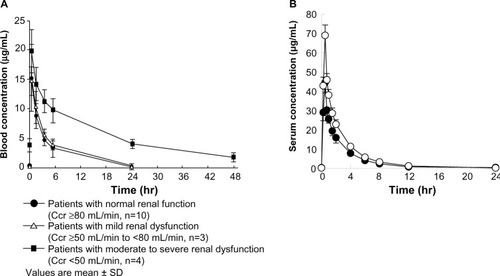
Table 2 Pharmacokinetic parameters after administration of ABK
On the other hand, the pharmacokinetics in healthy volunteers with normal renal function did not change on 400 and 600 mg single dose or on multiple administrations of ABK over a period of 7 days ( and ).Citation25 These data suggest that renal clearance and total clearance do not decrease at a high dose, and ABK has no tendency toward accumulation if renal function is normal.
Pharmacokinetics in children
Recommended initial dosing regimens were 5 mg/kg every 48 hours for preterm infants (postnatal age was within 28 days), 5 mg/kg every 24 hours for preterm infants (postnatal age was 28 days or more), and 4 mg/kg every 24 hours for term infants. These initial dosing regimens could manage the maximum concentration (Cmax) 7–15 μg/mL and trough concentration (Ctrough) 0–2 μg/mL in 72.2%–93.5% of infant patients.Citation26
Administration of ABK once daily in neonates has been investigated; the mean serum peak and Ctrough of ABK were 15.2±4.3 μg/mL and 2.0±1.4 μg/mL, respectively. Overall clinical effectiveness was 78.9% and no adverse effect was observed. During the period of administration, serum creatinine levels of some cases increased slightly, although the highest was 0.27 mg/dL but returned to baseline (pre-dose value) promptly after stopping ABK administration. Therefore, it is supposed that ABK therapy once daily in neonates is a treatment option.Citation27
Distribution of ABK
The PK-PD parameters of ABK in bronchial epithelial lining fluid (ELF) were investigated and the mean Cmax in serum and bronchial ELF were 26.0±12.2, and 10.4±1.9 μg/mL, respectively.Citation28 The ratio of concentrations of the drug in bronchial ELF to Cmax in serum was 0.465±0.188. These data suggest that transitivity of ABK to the respiratory tract was relatively good, because transitivity of aminoglycosides to the lungs is about 30% in general.Citation29
It has been reported that volume of distribution of aminoglycosides generally correlates with the extracellular fluidCitation30,Citation31 and tissue fluids, such as interstitial fluid or synovial fluid, with a sufficient concentration of the drug infiltrating a surgical wound site and subcutaneous tissue.Citation32–Citation38 Distribution of ABK from circulating blood to a wound site was evaluated in patients with wound infection caused by S. aureus who were treated with 200 mg of ABK once daily. In this study, high levels of distribution in the wound exudate, 46.2%–55.3%, were observed.Citation39
Therapeutic drug monitoring of ABK
Therapeutic drug monitoring (TDM) of ABK is required for maximizing efficacy while minimizing toxicities. In the population of patients with normal renal function, the target peak concentration (Cpeak) value of 15–20 μg/mL was not achieved with once daily administration of 150–200 mg as the approved dose, and a higher dosing regimen is required to improve clinical efficacy. A clinical practice guideline for TDM of ABK was developed by the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug Monitoring.Citation40 Experts recommend 300 mg/day (5.5–6.0 mg/kg) to reach the target concentration.
PK-PD parameters
The PK-PD parameter of ABK which was associated with a therapeutic effect was Cmax/MIC and/or AUC/MIC, with a low correlation of efficacy observed in T>MIC, and the highest correlation coefficient observed in Cmax/MIC.Citation41–Citation43 It was shown that the probability of cure/improvement rose when the Cmax of ABK was increased, with an odds ratio of 6.7 for a change in Cmax from 7.9–12.5 μg/mL.Citation44 In other studies, a key determinant of clinical efficacy of ABK was considered to be Cmax/MIC, and the appropriate Cmax/MIC value which showed a good correlation between bacteriological efficacy was 8 or higher.Citation44–Citation48
Clinical efficacy
There are several reports on clinical efficacy, bacteriological efficacy, and safety against MRSA infection which compared the treatment of VCM and ABK.Citation49,Citation50 Hwang et alCitation50 reported that the bacteriological efficacy responses of ABK and VCM were 71.2% and 79.5%, respectively, and the clinical efficacy responses of those were 65.3% and 76.1%, respectively, and that there was no statistically significant difference between ABK and VCM. The incidence of complications was significantly higher in the VCM group (32.9%) in comparison with the ABK group (15.1%) (P=0.019). ABK was not inferior to VCM, and it could be a good alternative drug for the treatment of MRSA infection.Citation49 However, further prospective randomized trials are needed to confirm this finding.Citation50
Clinical trial for re-assessment of higher dose regimen
There is a report on a clinical study to examine the efficacy and safety of ABK in patients with pneumonia or sepsis caused by MRSA.Citation51 In this study, the target Cpeak was initially set at 15–20 μg/mL and TDM was conducted. The efficacy rate was 87.5% (7/8 patients) for sepsis, 90.5% (19/21 patients) for pneumonia, and 89.7% (26/29 patients) in total ().
Table 3 Relationship between final daily dosage and efficacy/adverse drug reaction (ADR) rates
Based on the results, it was recommended that the dosage regimen of ABK should be initially set at 5–6 mg/kg or higher, and adjusted to achieve Cpeak at 10–15 μg/mL or higher and Ctrough lower than 2 μg/mL for treatment of patients with MRSA pneumonia or sepsis. With this strategy, low incidence of adverse drug reactions and higher clinical efficacy would be achieved. As for clinical effects, the efficacy rates for sepsis and pneumonia observed in this study were higher than the 70% efficacy rate which was observed in two other studies.Citation24,Citation52 This high efficacy rate might be attributable to the higher concentration of ABK designed in this study. As the result of TDM intervention, the patients with higher Cpeak at the final TDM than at the first TDM showed a 100% efficacy rate.
A study in elderly patients with pneumonia or sepsis caused by MRSA after once daily administration of ABK at the mean dose of 269.2 mg/day has been reported.Citation53 Cpeak values for all patients, in whom ABK treatment had been effective, were 15 μg/mL or higher. Their results and another report’s results by Kimura et alCitation54 suggest that therapy at high doses of ABK is recommendable even in old people, but that the control of Ctrough is crucial.
Combination therapy against multidrug-resistant Gram-negative bacteria
The combined effect of aminoglycosides and monobactams was studied using the Break-point Checkerboard Plate against MDRP.Citation55 Based on the result, a combination of AZT and ABK was selected as the anti-infective agent for MDRP treatment and the treatment result was reported. Since ABK also shows antibacterial activity against Gram-negative resistant bacteria, ABK as combination therapy can be used as a treatment option.
Adverse effect of ABK
Nephrotoxicity is a major adverse drug reaction to aminoglycoside antibiotics.Citation56–Citation59 The incidence of renal-related adverse drug reactions after administration of ABK was related to Ctrough. When Ctrough was 1, 2 or 5 μg/mL, the estimated rate of adverse drug reactions were 2.5, 5.2, and 13.1% respectively, and the incidence of renal-related adverse drug reactions increased with a higher Ctrough.Citation44 trough The incidence of ABK-induced nephrotoxicity was observed in all patients when ABK was administrated at a total dose of over 5,000 mg, while it was 4% at a total dose of less than 5,000 mg.Citation45
It is supposed that ototoxicity of aminoglycoside occurs because of the gradual drug accumulation of endolymph and perilymph in the inner ear.Citation60–Citation63 In addition, the results of some meta-analyses reported that there was no difference between single dosing and divided dosing in the incidence of ototoxicity.Citation64,Citation65 Yamasoba et al reported that the cochlea could easily be damaged by aminoglycoside antibiotics because of mitochondrial point mutation at location 1555, and that hearing loss might occur with the administration of small amounts of aminoglycoside antibiotics.Citation66,Citation67 This might suggest that hearing loss might occur in a patient who is not taking aminoglycoside antibiotics, but that the hearing loss is due to a familial or hereditary condition.
Conclusion
ABK has been used for the treatment of MRSA infections for over 20 years in Japan and about 15 years in Korea. Clinical evidence achieved in these two countries revealed the safety and efficacy of this drug. Since ABK shows good antibacterial activity against Gram-negative bacteria in addition to MRSA, some physicians reported the high efficacy of ABK for the treatment of multidrug-resistant Gram-negative bacterial infections such as A. baumannii and P. aeruginosa. Therefore, it is expected that ABK will be a good potential antibiotic as an additional treatment option, such as in combination with beta-lactams (eg, AZT), for serious infections due to its potent antibacterial activities against both MRSA and multidrug-resistant Gram-negative bacteria.
Disclosure
T Matsumoto has served as a speaker for Pfizer Inc., Meiji Seika Pharma Co, Ltd, MSD Co, Ltd, and Dainippon Sumitomo Pharma Co, Ltd.
References
- KondoSアルベカシンの開発とメチシリン耐性黄色ブドウ球菌による酵素的修飾をうけない新規誘導体の合成. [Development of arbekacin and synthesis of new derivatives stable to enzymatic modifications by methicillin-resistant Staphylococcus aureus]Jpn J Antibiot1994476561574 Japanese8072163
- TanakaNMatsunagaKHirataAMatsuhisaYNishimuraTMechanism of action of Habekacin, a novel amino acid containing aminoglycoside antibioticAntimicrob Agents Chemother19832457978026362557
- WatanabeAYanagiharaKMatsumotoTNationwide surveillance of bacterial respiratory pathogens conducted by the Surveillance Committee of Japanese Society of Chemotherapy, Japanese Association for Infectious Diseases, and Japanese Society for Clinical Microbiology in 2009: general view of the pathogens’ antibacterial susceptibilityJ Infect Chemother201218560962022766652
- YamaguchiKIshiiYIwataMMeropenem を含む各種注射用抗菌薬に対する2006年臨床分離株の感受性サーベイランス. [Nationwide surveillance of parenteral antibiotics containing meropenem activities against clinically isolated strains in 2006]Jpn J Antibiot2007606344377 Japanese18447206
- NishinoTSakuraiMIn vitro activity of everninomicin (SCH 27899)Proceedings of the 33rd Interscience Conference on Antimicrobial Agents and ChemotherapyOctober 17–20, 1993Louisiana, New Orleans Abstract No 462
- OkamotoRIyobeSMitsuhashiSHBKの細菌学的検討 [Antibacterial activity of HBK]Chemother198634110 Japanese
- KazunoYTsunetaSTamraABactriological evaluation of a new aminoglycoside antibiotic, HBKChemother1986346171
- MatsuhashiYYamamotoHメチシリン・セフェム耐性黄色ブドウ球菌の産生するアミノ配糖体系抗生物質不活化酵素に関する研究 [The enzymatic mechanisms of resistant to aminoglycoside antibiotics in methicillin-cephem-resistant Staphylococcus aureus]Jpn J Antibiot1988415523529 Japanese3216474
- NikiYHanakiHYagisawaMJapanese Society of Chemotherapy. The first nationwide surveillance of bacterial respiratory pathogens conducted by the Japanese Society of Chemotherapy. Part 1: a general view of antibacterial susceptibilityJ Infect Chemother200814427929018709531
- NikiYHanakiHMatsumotoTNationwide surveillance of bacterial respiratory pathogens conducted by the Japanese Society of Chemotherapy in 2007: general view of the pathogens’ antibacterial susceptibilityJ Infect Chemother200915315616719554400
- NikiYHanakiHMatsumotoTNationwide surveillance of bacterial respiratory pathogens conducted by the Japanese Society of Chemotherapy in 2008: general view of the pathogens’ antibacterial susceptibilityJ Infect Chemother201117451052321409533
- TakesueYWatanabeAHanakiHNationwide surveillance of antimicrobial susceptibility patterns of pathogens isolated from surgical site infections (SSI) in JapanJ Infect Chemother201218681682623143280
- MikuniyaTKatoYMuto-KobayashiYPrevalence of drug resistant gene and changes in susceptibility of methicillin-resistant Staphylococcus aureus strains isolated from 1990 to 2006 in Japan to antimicrobial agentsJpn J Chemother20096153740
- WatanabeTOhashiKMatsuiKKubotaTComparative studies of the bactericidal, morphological and post-antibiotic effects of arbekacin and vancomycin against methicilin-resistant Staphylococcus aureusJ Antimicrob Chemother19973944714769145819
- FlandroisJPFardelGCarretGEarly stages of in vitro killing curve of LY146032 and vancomycin for Staphylococcus aureusAntimicrob Agents Chemother19883244544572837137
- AsserayNJacquelineCLe MabecqueVActivity of glycopeptides against Staphylococcus aureus infection in a rabbit endocarditis model: MICs do not predict in vivo efficacyAntimicrob Agents Chemother200549285785915673789
- TakahashiTMatsumotoFMiyazakiSComparison of in vitro antibacterial activity of arbekacin, vancomycin and teicoplanin against methicillin-resistant Staphylococcus aureusJpn J Chemother1999472103107
- KurazonoMYamadaKHiraiYIdaTInoueMMRSA の疫学動向と各種抗菌薬の抗菌活性について. [Epidemiological survey of drug resistance of methicillin–resistant Staphylococcus aureus isolated in Japan in 2000]Jpn J Chemother2002508494499 Japanese
- MiyataAAraakeMOgawaHHanakiHHiramatsuKMRSAの Toxic shock syndrome toxin-1(TSST-1)産生に及ぼす arbekacinの作用. [Effect of Arbekacin of the production of toxic shock syndrome toxin 1 by methicillin-resistant Staphylococcus aureus]Jpn J Antibiotics2001547372381 Japanese11560056
- AraokaHBabaMTatedaKIn vitro combination effects of aztreonam and aminoglycoside against multidrug-resistant Pseudomonas aeruginosa in JapanJpn J Infect Dis2012651848722274165
- KataokaHIdaTIshiiYAnalysis of the influence of drug resistance factors on the efficacy of combinations of antibiotics for multidrug-resistant Pseudomonas aeruginosa isolated from hospitals located in the suburbs of Kanto area, JapanJournal of Global Antimicrobial Resistance2013129196
- ZaporMJBarberMSummersAIn vitro activity of the aminoglycoside antibiotic arbekacin against Acinetobacter baumannii calcoaceticus isolated from war-wounded patients at Walter Reed Army Medical CenterAntimicrob Agents Chemother20105473015301720404121
- Overview of Habekacin Injectable Solution (additional pediatric indication)In-house document of Meiji Seika Kaisha, Ltd
- AikawaNKohnoSKakuMWatanabeAYamaguchiKTanigawaraYAn open clinical study of arbekacin 200 mg qd in patients infected with methicillin-resistant Staphylococcus aureus (MRSA) – A clinical pharmacology studyJpn J Chemother2008563299312
- SunakawaKHoriS健康成人男性におけるアルベカシン硫酸塩400mg又は600mg投与時の安全性及び薬物動態. [Safety and pharmacokinetics of 400 and 600 mg arbekacin sulfate to healthy male volunteers]Jpn J Antibiotics201366297109 Japanese23951728
- SuzukiKTanikawaKMatsuzakiTPharmacokinetics and dosing of arbekacin in preterm and term newborn infantsPediatr Int200345217517912709144
- KinoshitaD新しい推奨ピーク値を目標とした新生児に対するアルベカシン1日1回投与法の検討. [Evaluation of once a day of arbekacin administration to neonates as a new object of peak concentration]Kansenshogaku Zasshi2010846727733 Japanese21226325
- FunatsuYHasegawaNNamkoongHPenetration of arbekacin sulfate to the lung tissueProceedings of the 52nd interscience conference on antimicrobial agents and chemotherapySeptember 9–12, 2012San Francisco Abstract No 2068
- CarcasAJGarcia-SatueJLZapaterPFrias-IniestaJTobramycin penetration into epithelial lining fluid of patients with pneumoniaClin Pharmacol Ther199965324525010096256
- KimuraTSunakawaKMatsuuraNKuboHShimadaSYagoKPopulation pharmacokinetics of arbekacin, vancomycin, and panipenem in neonatesAntimicrob. Agents Chemother20044841159116715047516
- KogaKKusawakeYItoYSugiokaNShibataNTakadaKEnhancing mechanism of Labrasol on intestinal membrane permeability of the hydrophilic drug gentamicin sulfateEur J Pharm Biopharm2006641829116750354
- BlaserJRiederHLLuthyRInterface-area-to-volume ratio of interstitial fluid humans determined by pharmacokinetic analysis of netilmicin in small and large skin blistersAntimicrob Agents Chemother19913558378391854165
- DeeTHKozinFGentamicin and tobramycin penetration into synovial fluidAntimicrob Agents Chemother1977124548549921252
- ThysJPSerruvs-SchoutensERocmansPHerchuelzAVanderlindenMPYourassowskyEAmikacin concentration in uninfected post thoracotomy pleural fluid and in serum after intravenous and intrapleural injectionChest19848545025056705579
- KozakAJGerdingDNPetersonLRHallWHGentamicin intravenous infusion rate: effect on interstitial fluid concentrationAntimicrob Agents Chemother1977125606608921257
- ChisholmGDWaterworthPMCalnanJSGarrodLPConcentration of antibacterial agents in interstitial tissue fluidBr Med J1973158535695734694402
- LorentzenHKallehaveFKolmosHJKniggeUBulowJGottrupFGentamicin concentrations in human subcutaneous tissueAntimicrob Agents Chemoter199640817851789
- RosinEEbertSUphoffTSEvansMHSchultz-DarkenNJPenetration of antibiotics into the surgical wound in a canine modelAntimicrob Agents Chemoter1989335700704
- HayashiMOoiKYamadaアルベカシン硫酸塩静注後の滲出液中濃度と血中濃度を測定した4症例. [Arbekacin sulfate concentration in peripheral lymph and in serum after intravenous injection: report of four cases]Jpn J Antibiot2012653207215 Japanese23173295
- OkadaKKimuraTMikamoHClinical practice guidelines for therapeutic drug monitoring of arbekacin: A consensus review of the Japanese Society of Chemotherapy and the Japanese Society of Therapeutic Drug MonitoringJ Infect Chemother20142011524486168
- ShimizuAMaebashiKNiidaMS03044. Pharmacokinetic-pharmacodynamic (PK-PD) study of arbekacin using mouse MRSA thigh infection modelIn-house document of Meiji Seika Kaisha, Ltd2003
- MattieHCraigWAPechereJCDetermination of efficacy and toxicity of aminoglycosidesJ Antimicrob Chemother19892432812932681115
- CraigWAPharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and menClin Infect Dis19982611129455502
- SatoRTanigawaraYKakuMAikawaNShimizuKPharmacokinetic-pharmacodynamic relationship of arbekacin for treatment of patients infected with methicillin-resistant Staphylococcus aureusAntimicrob Agents Chemother200650113763376917065622
- NegitaKYamashitaMKubotaTStudy on therapeutic drug monitoring of arbekacin in patients infected with methicillin-resistant Staphylococcus aureus and its efficacyJpn J Pharm Health Care Sci2001272123131
- NambaraMIkeueHKawasakiETomiokaSShimokawaFTanabeKEffectiveness and adverse reactions between once daily and every other day administration of arbekacin sulfateJpn J Ther Drug Monit2003203241248
- KobayashiMSaikyoASomaKYagoKSunakawaKPharmacokinetic and pharmacodynamics (PK-PD) analysis to determine the optimal method of arbekacin administrationJpn J Chemother20065411824
- TanikazeNKomatsuMShimakawaKYamamotoIメチシリン耐性黄色ブドウ球菌肺炎に対する硫酸アルベカシン治療における PK/PD 解析の臨床的有用性. [Study of clinical significance of PK/PD (pharmacokinetics/pharmacodynamics) parameters after administering arbekacin to patients with pulmonary methicillin-resistant Staphylococcus aureus infection]Jpn J Chemother2004529469473 Japanese
- HwangJHLeeJHMoonMKKimJSWonKSLeeCSThe usefulness of arbekacin compared to vancomycinEur J Clin Microbiol Infect Dis20123171663166622124537
- HwangJHLeeJHMoonMKKimJSWonKSLeeCSThe efficacy and safety of arbekacin and vancomycin for the treatment in skin and soft tissue mrsa infection: preliminary studyInfect Chemother2013451626824265951
- MatsumotoTHanakiHKimuraTClinical efficacy and safety of arbekacin sulfate in patients with MRSA sepsis or pneumonia: a multi-institutional studyJ Infect Chemother201319112813723263188
- KawanoHTanigawaraYPostmarketing surveillance review of arbekacin sulfate in patients with therapeutic drug monitoringJpn J Ther Drug Monit20102725571
- YamamotoYIzumikawaKHashiguchiKThe efficacy and safety of high-dose arbekacin sulfate therapy (once-daily treatment) in patients with MRSA infectionJ Infect Chemother201218224124622398881
- KimuraTSunakawaKTotsukaKDose finding study on arbekacin sulfate for appropriate peak levelsJpn J Chemother2011596597604
- AraokaHBabaMTakagiSMonobactam and aminoglycoside combination therapy against metallo-beta-lactamase-producing multi-drug-resistant Pseudomonas aeruginosa screened using a ‘break-point checkerboard plate’Scand J Infect Dis201042323123320001223
- Mingeot-LeclercqMPTulkensPMAminoglycosides: nephrotoxicityAntimicrob Agents Chemother19994351003101210223907
- SwanSKAminoglycoside nephrotoxicitySemin Nephrol199717127339000547
- GiulianoRAVerpootenGAVerbistLWedeenRPDe BroeMEIn vivo uptake kinetics of aminoglycosides in the kidney cortex of ratsJ Pharmacol Exp Ther198623624704753944768
- RougierFClaudeDMaurinMAminoglycoside nephrotoxicity: modeling, simulation, and controlAntimicrob Agents Chemother20034731010101612604535
- ChanbersHEChemotherapy of microbial diseases antimicrobial agents: the aminoglycosidesHardmanJGLimbirdLEGoodman and Gilman’s The Pharmacological Basis of Therapeutics, 10th editionNew YorkMcGraw-Hill200112191238
- HuyPTBMannelCMenlemansAKinetics of aminoglycoside antibiotics in perilymph in animalsLernerSAMartzGJHawkinsJEAminoglycoside OtotoxicityLittle, Brown and Company19818197
- TulkensPMClerckx-BraunFDonnezJSafety and efficacy of aminoglycosides once-a-day: experimental data and randomized, controlled evaluation in patients suffering from pelvic inflammatory diseaseJ Drug Dev19881Suppl 37182
- TotsukaKShimizuKMitomiNNiizatoTAraakeMArbekacinの1日1回投与法の検討 基礎的検討及びヒトにおける体内動態. [Evaluation of once-daily administration of arbekacin]Jpn J Antibiotics1994476676692 Japanese8072176
- BatesDEAminoglycoside ototoxicityDrugs Today (Barc)200339427728512743643
- BarclayMLKirkpatrickCMBeggEJOnce daily aminoglycoside therapy – Is it less toxic than multiple daily doses and how should it be monitored?Clin Pharmacokinet1999362899810092956
- YamasobaTInner ear disorders and mitochondrial DNA mutationPractica Oto-Rhino-Laryngologica20111048533540
- HamasakiKRandoRRSpecific binding of aminoglycosides to a human rRNA construct based on a DNA polymorphism which causes aminoglycoside-induced deafnessBiochemistry1997364012323123289315872