Abstract
The major public health concern worldwide is coronary heart disease, with dyslipidemia as a major risk factor. Statin drugs are recommended by several guidelines for both primary and secondary prevention. Rosuvastatin has been widely accepted because of its efficacy, potency, and superior safety profile. Inflammation is involved in all phases of atherosclerosis, with the process beginning in early youth and advancing relentlessly for decades throughout life. C-reactive protein (CRP) is a well-studied, nonspecific marker of inflammation which may reflect general health risk. Considerable evidence suggests CRP is an independent predictor of future cardiovascular events, but direct involvement in atherosclerosis remains controversial. Rosuvastatin is a synthetic, hydrophilic statin with unique stereochemistry. A large proportion of patients achieve evidence-based lipid targets while using the drug, and it slows progression and induces regression of atherosclerotic coronary lesions. Rosuvastatin lowers CRP levels significantly. The Justification for Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) trial was designed after the observation that when both low density lipoprotein and CRP were reduced, patients fared better than when only LDL was lowered. Advocates and critics alike acknowledge that the benefits of rosuvastatin in JUPITER were real. After a review, the US Food and Drug Administration extended the indications for rosuvastatin to include asymptomatic JUPITER-eligible individuals with one additional risk factor. The American Heart Association and Centers of Disease Control and Prevention had previously recognized the use of CRP in persons with “intermediate risk” as defined by global risk scores. The Canadian Cardiovascular Society guidelines went further and recommended use of statins in persons with low LDL and high CRP levels at intermediate risk. The JUPITER study focused attention on ostensibly healthy individuals with “normal” lipid profiles and high CRP values who benefited from statin therapy. The backdrop to JUPITER during this period was an increasing awareness of a rising cardiovascular risk burden and imperfect methods of risk evaluation, so that a significant number of individuals were being denied beneficial therapies. Other concerns have been a high level of residual risk in those who are treated, poor patient adherence, a need to follow guidelines more closely, a dual global epidemic of obesity and diabetes, and a progressively deteriorating level of physical activity in the population. Calls for new and more effective means of reducing risk for coronary heart disease are intensifying. In view of compelling evidence supporting earlier and aggressive therapy in people with high risk burdens, JUPITER simply offers another choice for stratification and earlier risk reduction in primary prevention patients. When indicated, and in individuals unwilling or unable to change their diet and lifestyles sufficiently, the benefits of statins greatly exceed the risks. Two side effects of interest are myotoxicity and an increase in the incidence of diabetes.
Keywords:
- rosuvastatin
- JUPITER study
- statin drugs
- C-reactive protein
- dyslipidemia
- cholesterol
- primary prevention
- cardiovascular risk
- coronary heart disease
- inflammation
- low-density lipoprotein
- high-density lipoprotein
- diabetes
- metabolic syndrome
- Framingham risk score
- Reynolds risk score
- coronary artery calcification
- carotid intima-media thickness
- hypertension
- obesity
- HMG CoA reductase
- mevalonate
- prenylation
- statin myopathy
- pleiotropic
- dolichol
Introduction
Cardiovascular disease (CVD) has been the leading cause of death for the past century in the United States (US), except for 1918, the year of an influenza pandemic. Even though deaths from coronary heart disease (CHD) have fallen during the past 2 decades, the mortality rate from this disease remains the top cause of death in the US, and, by 2020, will attain that status globally as well. An analysis of the fall in CHD death rates from 1980 to 2000 using the IMPACT model of analyzing data from the US National Center for Health StatisticsCitation1,Citation2 revealed that half of this decline was due to improvements in risk factors; 79% was attributable to primary prevention and 21% to secondary prevention.Citation3 Cholesterol reduction accounted for 42.7% of the death rate reduction in asymptomatic individuals, and for 34% in those with CHD. Use of statin drugs accounted for <20% of the improvement in death rate during those 20 years. Reductions in systolic blood pressure accounted for 38.8% of the fall in asymptomatic individuals and 52.8% in patients with CHD. Decreased use of tobacco accounted for 18.4% of the fall in deaths in asymptomatic individuals, and 12.9% in those with CHD. While the contribution of statins, 3-hydroxy-3- methyl-glutaryl-coenzyme A reductase (HMGR) inhibitors, was surprisingly small, these results illustrate the power of primary prevention in the management of CHD. Given the lower usage of less potent statins in many of the years surveyed, the data simultaneously suggest that using statin drugs earlier in the disease, for longer periods of time during pathogenesis, and titrated to lower targets, has substantial unrealized potential.
The cardiovascular risk burden in the populations of nearly all countries continues to rise at an alarming rate, and recent analyses show that gains in reducing the death rate from CHD are now being offset by the pressure of increases in reversible factors of obesity,Citation4 metabolic syndrome, and diabetes, along with the progressive aging of the population.Citation5–Citation8 Control of risk factors, while impressive thus far, have also fallen short of guideline targets and public health goals. Hence, there is ongoing interest in the best use of all elements of primary prevention in order to improve national heart health. Statin drugs are uniquely effective and prominently recommended in current guidelines. The potency and favorable benefit to risk ratio of rosuvastatin account for its increasing usage in primary and secondary prevention.
Significant and voluminous research concerning the biochemistry, physiology, and clinical potential of measuring C-reactive protein (CRP), has intensified discussions concerning the role CRP monitoring will have in current guidelines for primary prevention. The Justification for the Use of Statins in Primary Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) trial, first reported in October 2008, presented evidence that a plasma CRP ≥2 mg/L reflects higher cardiovascular risk in asymptomatic individuals with low-density lipoprotein levels (LDL) <130 mg/dL, and that they would benefit from rosuvastatin therapy.Citation9 Following the JUPITER report, there was lively debate about the data, clinical significance, and how the new information should be incorporated into clinical practice. Many fundamental questions concerning primary prevention have since been revisited, including the early beginnings of CHD and its long incubation period; methods of evaluating risk in the population; how populationbased versus individual risk-based approaches may best be employed; role and refinement of global risk factor scores; choice and merits of nontraditional risk factors; assessment of multiple biomarker panels; role of imaging techniques in evaluation and ongoing therapy; value of advanced lipid testing; weights assigned to traditional risk factors, cutoff values, and treatment targets, particularly LDL goals in guidelines; use of statins in primary prevention; reasons for low patient adherence with evidence-based therapies; causes of “clinical inertia” and lack of physician compliance with guidelines; and the etiologies, extent, and minimization of residual risk.
C-reactive protein
The fundamental role of inflammation in the pathogenesis of atherothrombotic disease is based upon strong evidence and is well-accepted.Citation11–Citation61 CRP protein is an acute phase reactant discovered by Tillett and Francis at Rockefeller University in 1930 in the blood of patients with pneumonia,Citation62 was crystallized in 1947, and today, over 60 years later, there is still controversy about its physiology and applications in biomedicine. CRP protein is a pentraxin comprised of 5 subunits () which is primarily synthesized in the liver, and plays an active part in regulating the innate immune system. Since CRP mRNA levels rise in adipose tissue as CRP expression is enhanced in vitro by interleukin-6 (IL-6), adipose cells also have some ability to synthesize CRP. Innate immunity and adaptive immunity significantly modulate atherosclerosis,Citation13,Citation63,Citation64 with both pro- and anti-atherogenic potential.Citation64–Citation66
Figure 1 A picture of C-reactive protein (CRP) from 1B09.pdb made using pymol.Citation10 CRP is a pentameric molecule containing a recognition face that binds phosphocholine and calcium ions, and on the opposite side, an effector face that contains a C1q-binding site. Function depends upon Ca2+-dependent ligand binding. See text for details. Reproduced by permission of Skolstoe through Wikipedia commons.
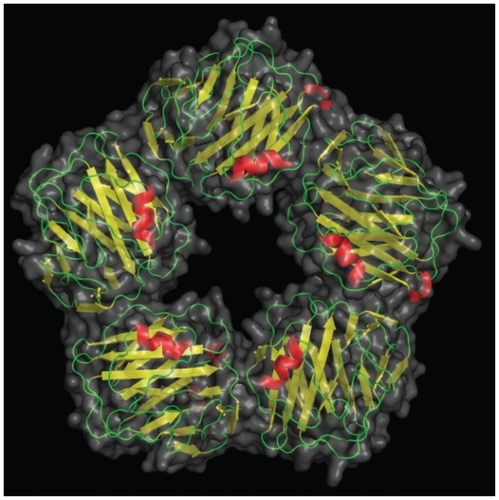
CRP binding offers a glimpse into teleological function. CRP binds to phosphocholine, commonly found in cell membranes as well as in bacterial and fungal polysaccharides. Phosphocholine is used by the placenta and nematodes to cloak them from their host immune system. Binding to complement C1q complex and factor H, CRP assists in human complement activity to promote antigen presentation and phagocytosis,Citation67 essentially functioning as an innate opsonin. In addition, CRP binds directly with phagocyte Fcγ receptors,Citation68 literally becoming the interface between innate immunity, C1q on complement, and inflammation, Fcγ on macrophages. Details of CRP binding to its ligands and their implications have been recently reviewed.Citation53 As an acute phase reactant during infections or diffuse tissue destruction, CRP concentrations may increase 50,000-fold quickly.Citation69 A constant potent stimulus may sustain high circulating CRP concentrations, depending upon synthetic capacity; the half-life of CRP in the circulation is about 19 hours.Citation70 Hepatic synthesis is driven at the transcriptional level by IL-6, largely expressed by macrophages, T cells, and adipocytes.Citation11,Citation71 Several upstream cytokines also regulate hepatic CRP release. In part because there is overlap in signaling, plasma CRP values are related to other inflammatory markers. However, despite a plethora of research, the precise role(s) of CRP remain unclear.
Variation and significance of CRP levels
Baseline values of CRP are influenced by genetics.Citation72,Citation73 Even after correction for age, CRP polymorphisms, and smoking, ancestry affects CRP levels, the highest values being found in blacks, with an average of 2.6 mg/L, followed by Hispanics, 2.51 mg/L, South Asians, 2.34 mg/L, whites, 2.03 mg/L, and East Asians with the lowest level at 1.01 mg/L.Citation74 CRP levels also vary with the environment, eg, pollutant burdens;Citation75 fiber intake,Citation76–Citation79 coffee ingestion,Citation80 and other dietary factors;Citation26,Citation29,Citation81–Citation84 smoking;Citation85 body mass index;Citation86,Citation87 alcohol consumption;Citation88,Citation89 drugs, including contraceptivesCitation90 and hormone replacement therapy;Citation91 chronic infections,Citation92,Citation93 and noninfectious inflammatory conditions, such as the autoimmune diseases,Citation94–Citation97 cancer,Citation98 and polycystic ovary syndrome;Citation99–Citation102 as well as multiple risk factors for atherosclerosis, including obesity, diabetes, metabolic syndrome, and hypertension. Triage of patients according to CRP levels generally control, correct for, and consider these variations.
Since CRP binds to LDL and can be identified within atherosclerotic plaque,Citation103,Citation104 is involved with inflammatory atherogenic processes,Citation105–Citation116 is elevated in patients with acute (ACS) and chronic coronary syndromesCitation117–Citation120 with unfavorable plaque compositions in these syndromes,Citation55 and is associated with complications of heart failureCitation121 a causal role in atherothrombotic disease has long been suspected. At this time, causality remains unproven.Citation107,Citation122,Citation123 One intriguing property of CRP is the associated inhibition of endothelial nitric oxide synthase in vitroCitation124 and the relationship to impaired vasoreactivity and hypertension in such models.Citation125 Overall, the evidence for a role of CRP in endothelial cell dysfunction and monocyte activation in metabolic syndrome is impressive and difficult to ignore.Citation126 The prevalence of this syndrome is approaching 53% in some populations (excluding those with diabetes)Citation127 and the importance of endothelial dysfunction in pathogenesis is now unassailable.Citation128
It is generally appreciated that a high CRP level (here-after meaning hs-CRP [hs, highly sensitive] measurements) usually portends a poorer prognosis in patients with CHD, diabetes, hypertension, pre- or postoperative surgery, and vascular comorbidities. A high prevalence of elevated circulating CRP levels in the general population has been known for some time. At the 53rd Annual Scientific Session of the American College of Cardiology, data were presented from the 1999–2000 National Health and Nutrition Examination Survey (NHANES) indicating that 47.1% of respondents aged 20 years or over had high CRP values.Citation129,Citation130 Levels were higher in females, the obese, and in the elderly, aged 55 to 74. About one-third of the population has CRP levels above 3 mg/L.Citation131 However, smaller elevations in CRP are even more common, and over half of the population has a CRP ≥ 2 mg/L.Citation132 Such “minor” elevations in CRP also imply a poorer prognosis compared with lower values, both in the ill and the apparently healthy.Citation133 Raised values of CRP strongly suggest clinical attention is necessary. Common associations of CRP elevations may reflect not only inflammation but widespread tissue distress, degeneration, and/or destruction, much of which may be age-related. At the other end of the continuum, a low CRP has been considered a measure of wellness,Citation134 and as lifestyle becomes progressively unhealthy in a population, CRP rises. As shown in the Monitoring Trends and Determinants in Cardiovascular Disease (MONICA) Augsburg Study, negative behaviors and factors, such as a poor quality “Western” diet with low intake of vegetables, fruits, and fiber, high consumption of saturated fats, poor physical fitness, and overfeeding and obesity, are all associated with higher CRP levels.Citation135 In a global sense, when no overt disease is evident, the CRP level roughly follows the level of self-inflicted abuse. In these instances CRP elevations reflect poor lifestyle choices that lead to deranged metabolic signaling, inflammation, and the appearance and worsening of traditional risk factors during the early incubation period of atherosclerosis. As such, elevations tend to cluster with conventional risk factors, and teasing apart the significance has been difficult,Citation136 but studies confirm that the properties of CRP and significance of changes are different. Lifestyle has a greater influence on CRP than does genetics.Citation137 Conversely, sustained improvement in lifestyle, particularly weight loss with exercise, and measures that relieve the risk burden, including statins, all reduce plasma CRP levels.
In a review of hospital records of 22,962 patients in a large urban population, an analysis of change in CRP status – normal (≤ 3 mg/L) to elevated (>3 mg/L) and vice versa – and mortality, revealed a significant graded association between CRP levels and mortality.Citation138 The patients were not healthy or chosen at random, but rather a cohort selected by physicians who believed their patients needed a CRP level performed. A change from normal to elevated CRP levels within a year was associated with a 6.7-fold hazard ratio (HR) for all-cause mortality during the following 4 years, compared to subjects whose CRP remained normal. When CRP levels changed from elevated to normal, the HR halved to 3.5. In the hospital setting as well, CRP levels reflect risk and subsequent survival, with a strong relationship to all-cause mortality, particularly in vascular diseases and cancer.Citation139
In the elderly, high CRP values are associated with greater risk of all-cause mortality, especially in apolipoprotein E4 carriers, as well as with cognitive decline.Citation140 The Rancho Bernardo Study reported that the lower the circulating CRP level in elderly men, the greater their longevity, and plasma concentrations of IL-6 were inversely related to survival time in elderly women who did not use estrogen.Citation141 Finally, the classic paper that showed CRP was a stronger predictor of cardiovascular events than LDL, and measuring both together provided better prognostic information than screening for either alone, firmly established the potential clinical significance of following circulating CRP concentrations.Citation142 This study also demonstrated the inverse relationship between CRP levels and the probability of event-free survival.
The work cited above supports the significance of circulating CRP levels in “ordinary” individuals as a sensitive but nonspecific index of quality of lifestyle prior to the diagnosis of disease, as a screen for risk refinement beyond traditional risk factors, and as an index that reflects the intensity of either the amount of inflammation or volume of cell distress.Citation133
When CRP was compared to other inflammatory markers as a predictor of relative risk of hard coronary events (postmenopausal women, highest versus lowest quartile) relative risk scores were CRP, 4.4, serum amyloid A, 3.0, soluble intercellular adhesion molecule type 1, 2.6, IL-6, 2.2, total cholesterol, 2.4, LDL, 2.4, apolipoprotein B-100, 3.4, high-density lipoprotein (HDL), 0.3, and for the ratio total cholesterol/HDL, 3.4.Citation35 The predictive power of CRP remained significant for LDL values <130 mg/dL. Of all nontraditional risk factors, CRP is the most studied, with over 34,000 general PubMed results, and 12,500 in connection with CVD, authored by investigators around the world over an extended period of time. CRP is involved in basic pathophysiology, and/or reflects additional risk and/or has predictive power in a number of CVDs, equivalents, or comorbidities, which include hypertension,Citation143–Citation151 hypertension and blood pressure variability,Citation152 percutaneous coronary intervention,Citation153,Citation154 re-endothelialization,Citation110 stent implantation,Citation155 coronary artery bypass surgery,Citation156–Citation158 heart failure,Citation159–Citation167 peripheral arterial disease,Citation168,Citation169 carotid artery disease,Citation170 sudden cardiac death (SCD),Citation171–Citation173 atrial fibrillation,Citation174–Citation176 ventricular tachycardia after myocardial infarction (MI) and implantable cardioverter-defibrillator implantation,Citation177 calcific aortic valve disease,Citation178 venous thromboembolism,Citation179,Citation180 pulmonary arterial hypertension,Citation181 diabetes,Citation116,Citation182–Citation186 metabolic syndrome,Citation87,Citation93,Citation168,Citation180,Citation185,Citation187–Citation199 rheumatic mitral stenosis,Citation200 chronic lung disease and asthma,Citation201–Citation203 chronic kidney disease,Citation154,Citation204–Citation206 obstructive sleep apnea,Citation207–Citation208 air pollution vis-à-vis inflammation and cardiac risk,Citation75,Citation209,Citation210 obesity,Citation137,Citation197,Citation211–Citation223 eclampsia,Citation224 blood concentrations of reactive oxygen species,Citation225 depression in the obese,Citation211 depression associated with coronary artery disease,Citation226 and HIV disease progression.Citation225 Statins have been found useful in many of these clinical situations. The preponderance of the evidence, from many diverse sources, indicates that CRP measurement has significant broad-based value and is also uniquely related to vascular disease.
CRP and genetic studies
CRP genetic (pentraxin-related) polymorphisms exist, which, together with diet and other lifestyle factors, contribute to significant interindividual variation in plasma CRP levels, as well as differences in responses to therapeutic agents.Citation227 Such variants in the CRP locus may account for 30% to 50% of the phenotypic variation in CRP levels,Citation228 and may also explain some ethnic differences.Citation229 CRP concentrations are 16% lower, for instance, in Asians, but 26% higher in black people than in whites.Citation230 In addition, other genetic loci that encode for upstream cytokines (IL-6, IL-1, tumor necrosis factor α) that affect CRP synthesis influence CRP levels, as well as genes related to obesity and insulin resistance.Citation187
Mendelian randomization, the random assortment of genes that occurs during reproduction, provides a method for assessing cause and effect that is not influenced by reverse causation.Citation231–Citation233 By comparing natural variation in known genes and phenotype, strengths of environmental influences may be inferred.Citation234 A large genome-wide association (n = 17,967) and replication study (n = 13,615) examined the association of genetic loci with plasma CRP concentrations and risk of CHD.Citation235 The authors found that genetic variants expected to lower the CRP expression by about 20% did not reduce CHD risk by the predicted amount of 6%. The discordance between anticipated versus actual CRP phenotype argued that, in genetic variants, high CRP levels throughout life do not cause increased risk for ischemic heart disease. Several limitations to the study, and in the use of Mendelian randomization generally, were identified.Citation236 Another Mendelian randomization study of 47,000 individuals from the general population revealed a comparable situation elsewhere: high plasma CRP values were robustly associated with higher risk of atrial fibrillation, but not with genetically elevated CRP levels.Citation176
Causation versus predictive utility
The Emerging Risk Factors Collaboration (ERFC) reported a meta-analysis of records of 160,309 people with medical histories of vascular disease, associating logeCRP concentrations with conventional risk factors and inflammatory markers.Citation237 Their data confirmed that downstream markers of inflammation, especially fibrinogen levels, but also the leukocyte count, plasma albumin concentration, and erythrocyte sedimentation rate, were associated with CRP levels. As the investigators adjusted for conventional risk factors, the associations of CRP levels with risk of CHD weakened, but the most significant adjustment was for fibrinogen perturbations during inflammation. Hepatic synthesis of this protein is also regulated by IL-6. Hence, the ERFC concluded that most of the association of CRP with coronary artery disease depends upon conventional risk factors and fibrinogen levels.Citation18,Citation238–Citation240 Their views are consistent with findings using Mendelian randomization discussed above, noting a disparity between CRP-related phenotypes, coronary risk, and subsequent coronary events.
Interestingly, after adjusting for conventional risk factors, the relative risks for CHD in this meta-analysis were CRP, 1.37, non-HDL cholesterol, 1.28, and systolic blood pressure, 1.35. Therefore, despite the conclusion, their data actually confirmed that CRP concentrations have a significant predictive association with risk of CHD, stroke, and vascular and nonvascular mortality.
While the ERFC appears to argue against a causative role of CRP in atherosclerosis, the issue is far from settled, since there is much convincing basic science that requires specific refutation.Citation126 In addition, a significant putative role for the monomeric form of CRP (mCRP) has been proposed.Citation241 Mediated by activated platelets, formation of mCRP,Citation242 a conformationally distinct isoform which is prothromboticCitation243 and inflammatory,Citation244 might confound conclusions if monomeric conversion of CRP from the pentameric moiety (pCRP) – commonly measured as hs-CRP – were not considered. Indeed, it has been shown that mCRP localizes monocyte-mediated inflammation in the atherosclerotic plaque, and may be deposited in plaques but not in healthy vessels, whereas pCRP is not found in either healthy or diseased arteries.Citation244 Moreover, mCRP and pCRP have differing actions on neutrophil migration and thrombus evolution. The various metabolic roles of pCRP and mCRP are expertly reviewed in an editorial accompanying the aforementioned paper.Citation115 There is further evidence that mCRP inserts into lipid raft microdomains within endothelial cell membranes, rather than binds to surface proteins, as a complex function of membrane cholesterol content. The result of this incorporation is endothelial cell activation, as part of an early inflammatory step in the atherosclerotic process.Citation245 These data are but a small part of the burgeoning scientific literature that underscores the importance of CRP in atherothrombosis, and the need for further research.
A randomized trial using a drug that targets CRP will be necessary to decide whether or not CRP is causally involved in atherogenesis. However, even if proof of CRP participation in the atherothrombotic process is incomplete, separate evidence indicates that measurement of CRP levels is useful in predicting and monitoring particular groups of patients. For instance, AFCAPS-TexCAPS found that patients with higher CRP may anticipate a better response to statins,Citation246 and selection of patients with high CRP levels in different circumstances adds to absolute risk assessment.Citation142,Citation247,Citation248 As mentioned above, the ERFC, a large meta-analysis, reported a consistent 1.6-fold rise in vascular risk for each 1-SD rise in CRP levels.Citation237
After de Beer reported that elevations in CRP levels predicted a poor outcome after MI,Citation249 baseline levels were found to predict future cardiac events in stable and unstable angina.Citation250,Citation251 These observations were extended to people without heart disease in whom baseline CRP measurements also correlated with future cardiac prognosis.Citation135,Citation252 Lowering CRP concentrations in patients without elevations in LDL following statin administration improved prognosis.Citation248,Citation253 Reporting bias, with multiple ways of comparing CRP values, together with publication bias in CRP studies, may hamper full evaluation of prognostic capability.Citation254 Several studies confirm that patients with higher CRP levels are at greater risk than those with lower values.Citation118,Citation255 These data support the view that measurement of CRP improves prediction of risk.Citation118,Citation256 Another approach, as suggested by the American Heart Association, the CDC, and the Canadian Cardiovascular Society, is that patients with heart disease falling in the “intermediate risk” category – with a Framingham Risk Score (FRS) of 10% to 20% – have increased CHD risk if CRP levels are elevated, and may be considered for statin therapy. The Canadian Cardiovascular Society recommends prophylactic statins for men >50 years and women >60 years with a CRP level >2 mg/L, and who are otherwise considered “intermediate risk”.Citation257 Prior to the JUPITER study,Citation9 considerable data showed that CRP levels ≥ 2 mg/L significantly raised risk, but currently laboratory reports continue to mention that CRP levels 2 to 3 mg/L reflect an average risk, and levels >3 mg/L reflect greater than average risk.Citation258 Large prospective cohort studies reported age-adjusted relative risks for coronary artery disease from about 2.0 to 3.0 for the highest versus the lowest levels of CRP, again documenting a consistent association with heart disease that has predictive power.Citation12,Citation86,Citation259
Some studies report that CRP does not discriminate sufficiently,Citation260,Citation261 adds little to traditional risk factors,Citation86 in particular the FRS, and hence may lack cost-effectiveness. On the other hand, investigators have reported remarkable discrimination in a number of clinical settings,Citation255 have found that when CRP is added to existing risk evaluation systems predictive power is enhanced,Citation256,Citation262–Citation268 and reported that cost-effectiveness is indeed significant.Citation269–Citation271 All things considered, CRP is admittedly imperfect, as are all risk factors. However, it is much better than other nontraditional risk factors when used to refine risk, particularly when used along with traditional risk factors. In conclusion, CRP is an acknowledged sensitive marker of systemic inflammation,Citation11 and in primary prevention, over 40 reports from prospective studes and 2 meta-analyses report a consistent association of CRP with subsequent CHD events.Citation86,Citation272,Citation273 One evolving view is that traditional risk factors and scores should be used initially, and CRP measured in patients at intermediate risk or in complex patients. If elevated, a more aggressive therapeutic stance may be warranted.
Although lifestyle measures and some pharmacological agents do reduce CRP levels, statins are most frequently employed, and lower CRP levels about 15% to 35%.Citation274,Citation275 Rosuvastatin and atorvastatin in higher doses have the most significant CRP-lowering properties.Citation274
Rosuvastatin
The word cholesterol derives from the Greek chole- (bile), stereos (solid), and –ol, the chemical suffix for alcohol. First identified in gallstones in 1769, the modern name was begun by chemist Eugène Chevreul in 1815. By 1971 Japanese biochemist Akira Endo began seeking compounds to lower cholesterol, and in 1987 Merck began marketing lovastatin isolated from Aspergillus terreus.
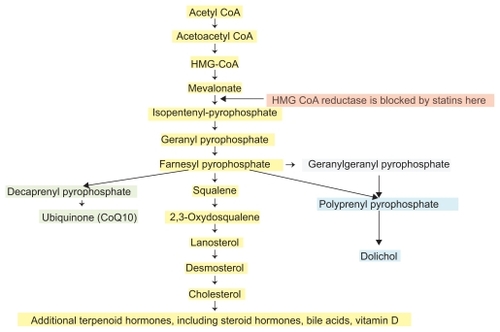
The endogenous biosynthesis of cholesterol occurs through the mevalonate pathway (). HMGR is a highly regulated enzyme which catalyzes the rate-limiting step in cholesterol synthesis. Although HMGR is located within membranes of the endoplasmic reticulum, its catalytic domain remains active after it is cleaved from the transmembrane portion of the enzyme. The reduction of HMG to mevalonic acid involves the transfer of 4 electrons, using 2 molecules of nicotinamide adenine dinucleotide (NADPH) as a reductant in 2 steps. The carboxyl moiety of hydroxymethlyglutarate esterified to the thiol of CoA is first reduced to an aldehyde, and then to an alcohol. Statin drugs are highly efficient competitive inhibitors of HMGR.
Clinical pharmacology
Rosuvastatin () is a sulfur-containing, hydrophilic statin with multiple sites that form a strong interaction with HMGR and therefore provide more potent enzyme inhibition than other statins. Stereochemical details of the molecular binding between rosuvastatin and HMGR have been detailed elsewhere.Citation276,Citation277 Rosuvastatin, like other statins, is a competitive antagonist of HMGR, competing directly with the endogenous substrate for the active site cavity of the enzyme. Rosuvastatin employs a modified hydroxyglutaric acid moiety that mimics the 3-hydroxyglutaryl unit of the substrate, HMG CoA, and the mevaldyl CoA transition state intermediate. The pyrimidine ring in rosuvastatin binds tightly to the HMGR enzyme in the same area that normally binds the CoA component of the endogenous substrate HMG CoA. As a synthetic, “type 2”, or second-generation statin, rosuvastatin contains a fluorophenyl group which provides additional polar interactions that strengthen binding to HMGR. All told, rosuvastatin has an affinity for the HMGR active site that is >104-fold higher than that of HMG CoA.
Figure 3 The structure of rosuvastatin, uniquely containing sulfur, a fluorophenyl group, and a modified hydroxyglutaric acid moiety. The IUPAC name of rosuvastatin is (E,3R,5R)-7-[4-(4-fluorophenyl)-2-[methyl(methylsulfonyl)amino]-6-propan- 2-ylpyrimidin-5-yl]-3,5-dihydroxyhept-6-enoic acid.
![Figure 3 The structure of rosuvastatin, uniquely containing sulfur, a fluorophenyl group, and a modified hydroxyglutaric acid moiety. The IUPAC name of rosuvastatin is (E,3R,5R)-7-[4-(4-fluorophenyl)-2-[methyl(methylsulfonyl)amino]-6-propan- 2-ylpyrimidin-5-yl]-3,5-dihydroxyhept-6-enoic acid.](/cms/asset/c5012b3c-b41c-432f-966d-5c007d85b5b8/dddt_a_10812_f0003_b.jpg)
Rosuvastatin is administered in its active acid form, meaning that the pharmacophore binding to the HMGR needs no transformation for activity compared with simvastatin or lovastatin, which are administered as lactones, a portion of which is hydrolyzed to the active acid form. Rosuvastatin is a hydrophilic statin, with relatively greater hepatoselectivity due to a unidirectional carrier-mediated active transport system. Hydrophilic statins tend to be retained in the liver, in part because they cannot passively diffuse out, whereas lipophilic statins concentrate in nonhepatic tissues. This property of hydrophilic statins is believed to account for fewer adverse events.Citation278,Citation279 As a result, rosuvastatin joins fluvastatin and pravastatin among statins least likely to produce myotoxicity.
Peak plasma concentration (Cmax) is reached 3 to 5 hours after oral administration,Citation280 and both Cmax and the area under the plasma concentration-time curve (AUC) increase almost linearly with the dose. Absolute bioavailability is about 20%. Rosuvastatin is 88% bound to plasma proteins, chiefly albumin. Mean volume of distribution under steady-state conditions is ≈134 L. The half-life of rosuvastatin is 19 hours, the longest of the available statins. While pharmacokinetics do not differ meaningfully among white, Hispanic, or black individuals, Asians have about double the median exposure (Cmax and AUC) than whites. As a result, lower starting doses are advised in Asian-Americans.
Elimination is primarily in the liver, with ≈10% through the action of cytochrome CYP2C9, producing a metabolite, N-desmethyl rosuvastatin, having up to half the potency of rosuvastatin. After oral administration, 90% of rosuvastatin and its metabolites are excreted in the feces. Following an intravenous dose, about 72% of total body clearance is via the hepatic route, and 28% through the kidneys. Lipophilic statins must be metabolized to water-soluble forms for renal excretion, reactions that depend upon CYP450 isoenzymes. Compared to atorvastatin and some other statins, rosuvastatin has an advantage, since it is not metabolized predominantly through CYP3A4, eliminating many potential drug and food interactions. There are, however, other variables affecting pharmacokinetics and potential dose-related toxicity. P-glycoprotein (P-gp, also called ABCB1), an intestinal ATP-dependent drug efflux pump located in epithelial plasma membranes, prevents cellular uptake of xenobiotic foreign substances. P-gp also transports a number of endogenous biochemicals and drugs across cell membranes, noteably digoxin, and is inhibited by several statins. Available data do not indicate that rosuvastatin inhibits P-gp significantly, and therefore interactions with P-gp substrates and inhibitors, many of which are also CYP3A4 interactants, are not clinically relevant. Another potential interaction involves a hepatic uptake transporter, organic anion transporting polypeptide 1B1 (OATP1B1).Citation281 Cyclosporine and gemfibrozil are OATP1B1 inhibitors, which may explain coadministration interactions.Citation282 (See further discussion below under Side effects).
For each 39 mg/dL (1 mmol/L) fall in LDL, there is a 21% reduction in major cardiovascular events.Citation283 Atorvastatin lowers LDL up to 60% at a maximal dose of 80 mg. Rosuvastatin lowers LDL by 45% to 63% (5 mg, 38%; 10 mg, 43%; 20 mg, 48%; 40 mg, 53%; 80 mg, 58%), reduces triglyceride levels by 10% to 35%, and raises HDL by 8% to 14%.Citation179,Citation284 The rise in HDL is believed to be due to a combination of a lower apolipoprotein A-1 (apoA-1) catabolism, raised hepatic apoA-1 synthesis, peroxisome proliferator-activated receptor-α activation and inhibition of cholesteryl ester transfer protein.Citation280 Of all the statins, rosuvastatin has the lowest half maximum inhibitory concentration for cholesterol synthesis in the liver. The milligram-equivalent reductions in LDL and elevations in HDL are superior to those of other statins,Citation179 thereby achieving evidence-based LDL targets in a higher portion of patients and greater success during intensive LDL reduction (). Rosuvastatin also lowers small, dense LDL concentrations. Although the reductions in LDL are dose-related, increasing the dose beyond 10 mg generally produces progressively smaller absolute reductions in LDL levels per unit.
Table 1 Rough equivalent doses of rosuvastatin
Clinical studies with rosuvastatin
The Galaxy ProgramCitation285 is a long-term, multi-trial research initiative sponsored by AstraZeneca, a planned portfolio of studies to investigate and support use of rosuvastatin to improve cardiovascular events and outcomes. The JUPITER study is one component, among others such as ASTEROID, METEOR, and CORONA. JUPITER sought to determine whether 20 mg of rosuvastatin could lower the number of major cardiovascular events in patients with acceptable LDL (under current guidelines) and elevated CRP levels, using a combined end point of death, MI, stroke, unstable angina or revascularization, and is further described below.
The Measuring Effects on Intima-Media Thickness: an Evaluation of Rosuvastatin (METEOR) trial randomized 984 asymptomatic participants with a mean age of 57 years, FRS < 10%, modest carotid intima-media thickness (CIMT) thickening (1.2 to <3.5), and elevated LDL (mean, 154 mg/dL) to either rosuvastatin 40 mg or placebo.Citation286,Citation287 The primary end point was the annualized rate of change in maximum CIMT at 12 sites during the 2-year study period. The rate of progression of maximum CIMT was significantly reduced by rosuvastatin therapy, but actual lesion regression was not achieved.
The Controlled Rosuvastatin Multinational Trial in Heart Failure (CORONA) was conducted from 2003 to 2005 in 371 sites in 21 countries.Citation288 The study randomized 5011 patients ≥ 60 years of age with chronic New York Heart Association (NYHA) class II, III, or IV ischemic systolic heart failure and an ejection fraction less than 40% to either rosuvastatin 10 mg or placebo. Median follow up was 32.8 months. There was a sharp fall in mean LDL (137 mg/dL) and CRP (3.1 mg/dL) at baseline to 3-month values of 76 and 2.1 respectively. The primary end point of the study was a composite of cardiovascular-related death, nonfatal MI, and nonfatal stroke. Secondary outcomes were total and cardiovascular mortality, time to first coronary event, and number of hospitalizations. By the end of the follow-up period, almost one-third of the participants sustained one end point event. There was no significant effect of rosuvastatin on primary or secondary end points, but a subsequent analysis suggested that those with CRP ≥ 2.0 had a 13% relative risk reduction and better outcomes.Citation289 The Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico Heart Failure (GISSI-HF) trial, which took place at 357 medical facilities in Italy, also prospectively randomized 4574 patients with NYHA class II-IV heart failure to rosuvastatin 10 mg or placebo, without an improvement in the primary end point.Citation290 In GISSI-HF the event rate was similarly high, with over half the patients sustaining a cardiovascular death or hospitalization, reporting a 29% all-cause mortality during a follow-up of over 4 years. Although no explanation was forthcoming, it is apparent that these patients were quite ill with well advanced structural changes and pathophysiology. A recent commentary hypothesized that progression beyond a critical threshold in the pathogenesis of heart failure may have precluded any beneficial effect, citing the need for additional trials.Citation291
Likewise, in A Study to Evaluate the Use of Rosuvastatin in Subjects on Regular Hemodialysis: An Assessment of Survival and Cardiovascular Events (AURORA), 2776 patients with end-stage chronic renal disease (ESRD) at 284 dialysis facilities in 25 countries were randomized to rosuvastatin 10 mg or placebo, and there was no significant difference between groups in a primary end point of time to a major cardiovascular event, even though LDL and CRP levels were substantially reduced in the treatment group.Citation292 In this population the event rate of MI, stroke and cardiovascular death was >35%, again reflecting complex, advanced disease and extremely high absolute risk. One author proposed that in both ESRD and calcific aortic stenosis, once disease has progressed sufficiently, particularly with anatomical changes, statins may become unable to help achieve the end points chosen.Citation293 When begun earlier during aortic sclerosis or mild stenosis, improvement is more likely than when stenosis is advanced. In ESRD, since cardiovascular mortality rises sharply by the time a patient requires dialysis, the threshold for benefit may have been passed prior to enrolling in the study.
The results of the A Study to Evaluate the Effect of Rosuvastatin on Intravascular Ultrasound-Derived Coronary Atheroma Burden (ASTEROID) study offer insight into the effects of rosuvastatin on the atherosclerotic process using two different, complementary techniques. First, monotherapy with 40 mg rosuvastatin for 24 months, which lowered LDL and raised HDL by about 53% and 15% respectively, significantly reduced atheroma volume in major coronary arteries that were angiographically normal or were stenosed, as assessed with intravascular ultrasound.Citation294 Second, using quantitative coronary angiography (QCA), rosuvastatin decreased percentage diameter of coronary stenoses and improved minimum lumen diameter.Citation295 Intravascular ultrasound images the coronary artery wall in proximal areas with minimal lumen stenosis, and QCA examines luminal narrowing in different segments of the coronary tree. Concordance of the findings strongly suggests rosuvastatin causes both slowing of progression of atherosclerosis and lesion regression in concert with LDL levels ≤ 70 mg/L (1.81 mmol/L). Reduction of luminal diameter, as detected by QCA, correlates with lower risk of future coronary eventsCitation296 and subsequent mortality.Citation297 Interestingly, changes in atheroma volume, when stratified above or below a median change of −37.1% in LDL and −21.4% in CRP levels, was greatest in those with reductions in both LDL and CRP (−2 mm3), less when CRP fell but not LDL (−1 mm3), progressed when LDL fell but CRP was high (+2 mm3), and progressed the most when both LDL and CRP were high (+8 mm3).Citation294
The JUPITER study
Based upon (a) the ability of CRP to predict future vascular events,Citation142,Citation299–Citation301 and (b) of statins to lower CRP,Citation301 together with (c) additional evidence that the benefits of statins were greater when both LDL and CRP levels were lowered,Citation249,Citation253 and (d) a post-hoc analysis of the AFCAPS/TExCAPS study that indicated that healthy individuals with elevated CRP levels and normal LDL values could benefit from statin therapy,Citation246 the global, multicenter JUPITER study was designed.Citation9,Citation302,Citation303 After screening some 90,000 prospects, JUPITER enrolled 17,802 men (≥ 50 years) and women (≥ 60 years). The study population was not diagnosed with either CHD or diabetes, and had “normal” LDL levels (LDL < 130 mg/dL), but high hs-CRP levels (≥ 2.0 mg/L, median, 4.2 mg/L).
Participants were randomized to either treatment with rosuvastatin 20 mg daily or placebo. Participants’ median age was 66 years, and they comprised 62% men, 38% women, 71% Caucasians, 12.5% blacks, and 12.7% Hispanics (). Although free from clinical illness, the JUPITER population was not healthy, with 41% qualifying for the metabolic syndrome cluster of risk factors, 16% using tobacco, and 11.5% with a family history of premature heart disease. The cohort was fairly representative of the general population, with as-yet undetected, but substantial risk burden. This is an important point, since sometimes the term “healthy” may automatically be interpreted to mean “no treatment is necessary”.
Table 2 Baseline clinical data in the JUPITER trial
The primary end point composite included a nonfatal MI, nonfatal stroke, hospitalization for unstable angina, an arterial revascularization procedure, or confirmed death from a cardiovascular cause. The secondary end points included the individual components of the primary end point and all-cause mortality.
Although planned as a 5-year study, when patients in the rosuvastatin group had significantly fewer events and deaths than the controls, an independent data and safety monitoring board performed an interim efficacy analysis, and the trial was stopped after a median follow-up time of 1.9 years. About 75% of the treated participants were still taking rosuvastatin when the trial was ended. At that time there were 142 first major cardiovascular events in the rosuvastatin group, and 251 events in the placebo group, for a 44% reduction in first major cardiovascular events (HR 0.56, 95% confidence interval [CI] 0.46 to 0.69; P < 0.00001). There was also a 54% drop in nonfatal MI, a 48% reduction in nonfatal stroke, and a 47% fall in the cumulative incidence of hard end points of MI, stroke, or cardiovascular death in the rosuvastatin group (). In addition, there was a significant reduction in all-cause mortality of 20% in the treatment group, comparatively greater than in previous statin trials considering the duration. Rosuvastatin lowered CRP levels by 37%, with a 12 month mean of 2.2 mg/L, and lowered LDL by 50%, with a mean treated value of 55 mg/dL. Without a control group with normal CRP levels, whether CRP reduction was responsible for the observed benefits could not be answered.
Table 3 JUPITER trial: comparison of outcomes between treated and nontreated patients
The number needed to treat to prevent a first major primary end point event in 2 years was 95, falling to 31 in 4 years, and 25 for 5 years of treatment with rosuvastatin. The cardiovascular event rate in the rosuvastatin group was about 1 in 100, compared to approximately 2 in 100 in the placebo group, an absolute risk reduction of ≈1.2% for the 1.9-month study. Hence 25 individuals would require treatment for 5 years to prevent a single event, an absolute risk reduction of about 4%. Note that in primary prevention the baseline risk and event rate is low, so there is relatively less benefit in absolute risk anticipated. It is also instructive to compare the improvement in absolute risk achieved using the Mediterranean diet as the intervention, which may exceed 5% in some situations.Citation304,Citation305
JUPITER recorded 270 new cases of diabetes in the treatment group compared to 216 in the control group, and a rise in median glycated hemoglobin (HbA1c) levels, also noted in prior statin studies, amounting to a 25% increase in physician-reported incidence of diabetes over a 1.9-year period. There were 10 cases of myopathy in the rosuvastatin group versus 9 in the control group, with only 1 instance of rhabdomyolysis associated with rosuvastatin, numbers that are consistent with previous rosuvastatin trials.
Given prior data that CRP values improved prediction of risk, JUPITER suggested that a seemingly healthy patient population at high risk, previously ineligible for statin therapy, may benefit from rosuvastatin treatment, guided by the CRP level.Citation306 Attention was focused on the large body of research that points to inflammation as a common denominator in atherothrombosis, ie, that inflammation matters at a clinical level.Citation57 JUPITER, called a landmark study immediately after presentation, has since been the subject of many editorials, discussions, and intense debate. An online poll conducted by the New England Journal of Medicine followed publication, with 2553 votes cast over 18 days.Citation307 Half of the respondents believed JUPITER data should change screening in the general population, with the remainder voting against any change. Similarly, the votes for and against a change in the therapeutic use of statins based upon JUPITER results were about evenly divided.
Subsequent analyses pertaining to JUPITER
Using data from 1999–2004 NHANES and applying NCEP ATP III 2004 Update (ATP III) criteria, Spatz et alCitation308 calculated that 57.9% of older adults (men ≥ 60 years, women ≥ 50 years) are either taking a statin (24.4%) or eligible for a statin (33.5%). If one includes individuals satisfying strict JUPITER criteria – no history of cardiovascular disease, LDL <130 mg/dL, and CRP ≥ 2 mg/L – an additional 13.9% of the age group mentioned above, or nearly 8 million people, would become eligible for rosuvastatin therapy. If expanded JUPITER criteria were used – LDL between 130 and 160 mg/dL and CRP ≥ 2 mg/L – another 5.3%, or 3 million individuals, would become statin-eligible. Hence a grand total of just under 80% of the older population would have an indication for statin therapy. Compared to the remaining 20%, the “JUPITER group” was composed of more females, was older with a higher body mass index, and tended to have hypertension and metabolic syndrome. They also shared many characteristics with ATP III subjects, particularly the use of tobacco, visceral obesity, and hypertension. Interestingly, the investigatorsCitation308 noted that in the Women’s Health Study, about 20% of the women with low and intermediate FRS were reclassified by using the Reynolds risk score, which incorporates CRP values.Citation35,Citation256,Citation263 These findings support the growing realization that risk is greater than generally believed, and the validity of CRP-guided risk reduction.
Michos and BlumenthalCitation309 also estimated the prevalence of JUPITER-eligible individuals in the US population using NHANES 1999–2004 data. They found about 6.5 million individuals would be added if strict JUPITER criteria were followed. Based upon the number needed to treat (NNT) of 25 at 5 years, they estimated about 260,000 cardiovascular events could be prevented with rosuvastatin therapy. A subsequent recalculation, after adding the number of venous thromboses that would be avoided, raised the number to about 500,000 per annum.
RidkerCitation310 clarified aspects of the JUPITER study in mid- 2009, observing that all prespecified subgroups benefited by rosuvastatin therapy, including those participants considered at low risk. The decision to terminate the study early was based on rigorous pre-agreed principles. It was noted that the NNT to prevent 1 event for 5 years was comparable to that reported in AFCAPS/TexCAPS, and less than those accepted for the use of diuretics or beta-blockers in treating hypertension for primary prevention. Another point emphasized was that 80% of individuals who developed diabetes occurred among those participants who had impaired glucose tolerance at baseline, but those patients also benefited from treatment in terms of end points. Last, reduction of both LDL and CRP levels was especially successful, and dual targeting may simplify decisions to treat. Another detailed analysis of absolute risk reductions and consequent NNT within the JUPITER trial, including alternative statin regimens, concluded that NNT values are acceptable.Citation311
Yang et al,Citation312 using a JUPITER-eligible cohort from the Atherosclerosis Risk in Communities (ARIC) Study (men ≥ 50, women ≥ 60, CRP ≥ 2 mg/L, LDL <130 mg/dL), sought to determine if the absolute event rates and risk reduction seen in JUPITER would persist for a period longer than the 1.9 year follow-up. Of their JUPITER-eligible participants, there was an absolute CVD risk of ≈10.9% over a mean follow-up of 6.9 years, or 1.57% per year. Applying JUPITER HRs to this group generated an NNT of 38 over 5 years and 26 over 6.9 years. They concluded that the use of age and CRP level was a convenient method of identifying higher risk individuals.
Vaccarino and coworkersCitation313 noted the absolute risk reduction of 0.59% per year for the primary end point required 169 persons to be treated for 1 year to prevent a single combination of events. To prevent a major coronary event, such as an MI, 500 patients needed to be treated for 1 year for a single event. An estimate of a drug cost for rosuvastatin of US$638,750 per year was made to prevent 1 event, and for a generic statin, US$24,000 per year. In their view, adding CRP screening costs of US$62,500, and then for additional liver function, glucose, and HbA1c monitoring, a total of over US$137,000 was reached per year for each event prevented. These authors suggested that the funds instead be invested in effective, proven population-based strategies to lower risk, as discussed elsewhere.Citation314–Citation316 In general, the costs per life year for lifetime treatment using simvastatin vary from US$2500 to US$10,990, depending on age and risk.Citation317 Accad and FredCitation318 also opined that, according to their calculations, treatment of 95 individuals for 2 years to avoid 1 event is not a sufficient reward for the person with a high CRP level, but may be acceptable on a population level. On the other hand, Slejko et alCitation269 maintained that statin therapy in JUPITER patients is cost-effective, at a cost of US$40,457 per quality adjusted life-year, below the customary threshold of US$50,000. MacDonaldCitation271 estimated that treating JUPITER-eligible individuals with rosuvastatin is highly cost-effective, but is a function of the initial FRS.
Kappagoda and AmsterdamCitation319 reviewed treatment in the JUPITER study according to traditional risk factors and guidelines, and their calculations showed the following. Baseline characteristics of the participants revealed 2225 in each group with systolic blood pressures over 145 mm Hg. Treating these elevations would have lowered the number of strokes by 12 over the duration of the study. Similarly, by treating those individuals with LDL >119 mg/dL and HDL <40 mg/dL (about 25% of the subjects), and over-weight individuals (>50%) with weight loss, and eliminating tobacco use in the 16% who smoked, along with administering evidence-based aspirin prophylaxis in men for CHD prevention, and in women for stroke prevention, meaningful benefits would have changed outcomes. Aspirin alone could potentially have prevented 72 of the 99 MIs that occurred during the course of the JUPITER trial. Finally, since the baseline median HbA1c was 5.7% (reference range 4.8% to 5.9%), 2225 individuals in each group had levels >5.9%, suggesting that close to 25% of the entire JUPITER population met this criterion for diabetes. These authors suggested that because guidelines for care were not strictly followed, a spuriously high event rate may have caused an appearance of higher benefit from statin therapy. The event rate, however, was similar in the ARIC profile cohort that was JUPITER-eligible,Citation312 although smaller, which would argue against this view.
A most significant dual target analysis of the JUPITER study evaluated the effects of rosuvastatin 20 mg versus placebo on the prespecified end points according to on-treatment values of LDL (<70 or ≥ 70 mg/dL) and CRP (<2 mg/L, or <1 mg/L).Citation320 Compared to placebo, those in the treatment group who achieved an LDL < 70 mg/dL had a 55% reduction in vascular events per 100-person years (). Those who achieved CRP < 2 mg/L had a 62% reduction in events. Among those who reached dual reductions, there was a 65% reduction in events compared to a 33% reduction in those who achieved one or neither target. Those who reached an LDL < 70 mg/dL and a CRP < 1 mg/L enjoyed a 79% reduction in events (). Treatment CRP levels predicted the event rate no matter what lipid end point was used, including the ratio of aopB/aopA-1. Therefore, regardless of the lipid profile, the lower the CRP, the better was the prognosis. An editorial concluded that JUPITER provided “key experimental data” that inflammation mediated the benefits of rosuvastatin, but mused at the prospect of comparing the absolute risk reduction of statins with the effects of weight loss and regular exercise, remarking that such a study is unlikely,Citation321 both for lack of funding and interest. Many of the pleiotropic effects of rosuvastatin are anti-inflammatory, and a catalog of those actions – significant improvement in endothelial function, immune responses, plaque stabilization, vascular remodeling, and oxidative stress – and antithrombotic actionsCitation322 further underpins the observation that targeting CRP is worthwhile and clinically rewarding.
Table 4 Cardiovascular events fell based on LDL cholesterol and on hs-CRP levels <2 mg/L
Table 5 Cardiovascular events fell based on LDL cholesterol and on hs-CRP levels <1 mg/L
The use of statins in women, particularly for primary prevention, has been heavily debated.Citation323–Citation325 Mora and coworkersCitation326 performed a specific gender-specific analysis from JUPITER using rosuvastatin 20 mg or placebo employing the criteria mentioned above. Focusing only on 6801 female participants in JUPITER, treatment significantly lowered the relative risk of the primary end point, composite of MI, stroke, revascularization, hospitalization for unstable angina, and death from cardiovascular causes, by 46%. The greatest benefit was seen for revascularization, associated with a treatment-related reduction of 76% compared to placebo. A meta-analysis of 5 studies reporting sex-specific outcomes was also undertaken. Absolute CVD rates per 100 person-years in JUPITER women were lower than for men, with similar relative risk reductions between the sexes. A total of 13,154 women were included from primary prevention trials, and a significant reduction in primary CVD events with statins by one-third was found (relative risk 0.63; 95% CI 0.49 to 0.82; P < 0.001). These results were similar to prior results in men, and also to findings for secondary prevention in women. It was postulated that the greater numbers enrolled allowed JUPITER to demonstrate the benefit.Citation327 CRP was noted as a tighter predictor of events in women than in men, along with the correlation between the degrees of CRP lowering and associated clinical benefit. These authors concluded that while CRP level as an independent predictor of events remains controversial, CRP is accepted as a marker which may be involved in the atherogenic process.Citation237
The FDA approved rosuvastatin for primary prevention on February 9, 2010, following a 12-4 vote in a panel 2 months before, which only seemed to flare the ongoing controversy about its use in “healthy” individuals.Citation328 The new indication was for men ≥ 50 years and women ≥ 60 years with fasting LDL ≤ 130 mg/dL, CRP ≥ 2.0 mg/L, triglycerides ≤ 500 mg/dL, no diagnosed CVD, and at least 1 additional CVD risk factor.
Summary of articles in the Archives of Internal Medicine
Kaul and collaboratorsCitation329 challenged 3 aspects of the JUPITER study, asking (a) does CRP predict risk and treatment response? (b) did early stoppage of JUPITER unduly raise the benefit? and (c) what about guideline recommendations? First, they believed that the predictive value of 1.35%, although positive in JUPITER (241 events in 17,802 patients), was weak, and basically that treatment decisions should not be stratified using CRP values because there was no low-CRP, low-LDL control arm for comparison. This arm was excluded in the design of JUPITER because of the prior post-hoc analysis of AFCAPS/TexCAPS showing no benefit in a group with low CRP.Citation246,Citation330 The JUPITER authors hypothesized, with considerable supporting evidence from other investigators and studies outlined above, that high CRP levels reflected increased risk, and treatment with rosuvastatin addressed that component over and above any LDL lowering.Citation310 A fair consensus from the many commentaries and blogs would be that a high level of CRP does have clinical utility, portends an otherwise poorer prognosis, but a normal CRP value does not assure low risk.
Second, the early termination of JUPITER may have led to a somewhat higher benefit than would have been observed from a longer study period. Compared to other statin studies in primary prevention, JUPITER reported unexpectedly larger reductions in ischemic end points including mortality. Studies terminated prematurely in other trials are known to exaggerate benefits, which regresses to the mean when follow-up is longer.Citation331–Citation334 A large systematic review reported that for interventions showing a 20% improvement in completed trials, stopping them early might double the apparent benefit.Citation332 It is true that other studies used less potent statins, but a rapid mortality benefit within this period is exceptional. Details provided subsequent to JUPITER concerning the circumstances of the early termination did not reflect any intent to exaggerate the positive results. Kaul agreed that rosuvastatin benefits did occur in JUPITER, although perhaps were increased by the early stoppage of the study.Citation330 The pathology in the CORONA and AURORA populations was sufficiently different from JUPITER to make a comparison of results difficult.
Third, Kaul et alCitation329 question the conclusion that high CRP levels predict preferential improved response in JUPITER, based on an FDA analysis showing, essentially, that treatment effect of statins was not proportional to the degree of elevation in CRP.Citation335 This conclusion was based on a stratification of FRS risk scores according to the CRP level. In addition, however, data presented in show a clear relationship between low CRP values and good prognosis.Citation321 Kaul et al concluded that 44% risk reductions in JUPITER-eligible patients in the population will not be typically attained if CRP-guided rosuvastatin therapy is used. Their second conclusion, with which everyone agrees, is that control of risk factors with lifestyle modification trumps pharmacologic intervention in primary prevention. The third conclusion advises that if patients do not change their lifestyle, then statins may be used. In practice, since ≈95% of individuals will fall into this category, ultimately most patients will receive statins, simply because there are no comparable alternatives.
De Lorgeril et alCitation336,Citation337 maintained that a) there was a discrepancy between the reduction in mortality between end point subgroups; b) cardiovascular mortality was 5% to 18% compared with total mortality and the expected rate is about 40%; c) the case-fatality rate of MI was low compared to an expected figure of 50%; the case mortality rate in the placebo group was 8.8% compared to 29% in the rosuvastatin group; d) no sudden cardiac death was reported in JUPITER; and e) bias may have been introduced because of conflicts of interest and commercial sponsorship. These analysts believed that there was no significant difference in cardiovascular mortality between the two groups in JUPITER. Last, they lamented the secondary end point and subgroup analyses published concerning benefit in preventing venous thromboembolic disease,Citation338 efficacy in women,Citation326 lower stages of chronic renal disease,Citation339 and in the elderlyCitation340 because they shared the limitations of the original study.
Several of the earnest concerns summarized in the papers by KaulCitation329 and de LorgerilCitation336 have been addressed by investigators other than JUPITER, and have also been answered in part by subanalyses and refinements presented by the JUPITER authors during the past 2 years. For instance, the association of high levels of CRP with vascular risk has considerable supportive evidence from multiple sources, and the recent meta-analysis of 54 prospective studies by the Emerging Risk Factors Collaboration confirmed this relationship.Citation237 Specifically, the adjusted risk associated with a 1-standard deviation increase in CRP (HR 1.4; 95% CI 1.3 to 1.5) compared quite favorably with that associated with a similar increase in cholesterol (HR 1.2; 95% CI 1.1 to 1.3).
A closer evaluation of the relationship between base-line CRP measurements and cardiovascular risk is also available.Citation268 Treating CRP as a continuous variable, an ordinal variable and as a threshold variable, relative risk reduction after rosuvastatin therapy was similar maintained across the entry levels of CRP. Absolute risk reductions therefore were greatest in the patients with the highest entry levels of CRP. Independent corroboration of these data is found in the ARIC studyCitation312 in which groups with similar FRS and LDL levels had higher vascular risk when the CRP was elevated, compared to counterparts with low CRP values.
JUPITER findings incorporated into the Canadian Cardiovascular Society guidelines
The Canadian Cardiovascular Society acknowledged JUPITER findings in their guidelines and recommended measurement of CRP in JUPITER-eligible individuals at “intermediate risk” as a step toward prophylactic statin treatment.Citation257 The Society extended recommendations from the CDC in which CRP levels were considered an adjunct to risk assessment in healthy persons with an FRS between 5%–20%, ie, at intermediate risk.Citation341 In JUPITER, the event rate in the placebo group was greater than in AFCAPS/TexCAPS study, and most individuals had an FRS between 5% and 20%. Analysis of JUPITER trial data stratified according to both the Framingham and Reynolds 10-year risk scores confirmed that treatment of JUPITER-eligible men and women in the “intermediate” categories (5% to 10% and 10% to 20% 10-year risk) significantly reduced cardiovascular events.Citation342 In the 5% to 10% FRS category who were treated, HR was 0.55 (95% CI 0.36 to 0.84; 5-year NNT = 40, P = 0.005) (). In the 11% to 20% risk category, HR was 0.51 (95% CI 0.39 to 0.68, 5-year NNT = 18; P < 0.0001).
Table 6 Event rates and hazard ratios for the primary end point correlated with estimated 10-year Framingham and Reynolds risk scores at baseline
Using the FRS, no significant benefit occurred in the groups with either low or very high risk. The Reynolds risk score reclassified more individuals into these two categories, low (<5%) and high (>20%), and rosuvastatin did produce a benefit in those at highest risk. Since the FRS underestimates risk in women, and frequently women do not have FRS > 10%, they may not be considered for treatment under current guidelines. Using CRP ≥ 2 mg/L as part of JUPITER criteria would include almost 7000 of such women who could potentially benefit from rosuvastatin therapy. This number becomes considerable in view of the growing awareness of serious gender disparities in CHD treatment.Citation343
Summary of response of JUPITER authors
Ridker and GlynnCitation330,Citation344 and RidkerCitation345 responded to the four major issues raised by De Lorgeril et al,Citation336 namely a potential deficiency in trial design and execution; early termination of the study was inappropriate and/or favored to exaggerate benefit; inconsistencies existed concerning mortality, statin treatment and CRP; and pharmaceutical company sponsorship played a significant part in the positive outcomes, as summarized below.
JUPITER study design
The study was logically designed, participant follow-up was careful and full, end point adjudication was rigorous, and followed a pre-specified analysis plan.
Early termination of the trial
The details concerning the charter between the investigators and members of the independent Monitoring Board that decided to end the trial early were described. The decision to do so followed that agreement and was just and proper. The investigators reiterated that any overestimate of relative risk reduction involved would have been small, estimated by an FDA statistical analysis at ≤ 1%.Citation346 Since the benefit was highly significant at 44% reduction in relative risk for the primary end point, there would be no clinically significant change in outcome interpretation. Simulation studies indicated that stopping the study early under similar circumstances produced valid treatment results.Citation347,Citation348
The benefits of rosuvastatin therapy in JUPITER were much larger than those reported in earlier statin trials. However, the relative risk lowering in JUPITER was similar to the analysis of a JUPITER-eligible cohort in the AFCAPS/TexCAPS study previously reported.Citation246 In addition, earlier statin trials showed that a 1% fall in LDL level corresponded to a 1% reduction in relative risk. This was approximately the same in JUPITER, since rosuvastatin lowered LDL by 50%, and the resulting fall in relative risk was about the same magnitude.
A sequential review of the benefit of rosuvastatin treatment throughout JUPITER demonstrates that the differences between treatment and placebo groups increased steadily as the study progressed, rather than decreased.Citation344
Inconsistencies in case-fatality rate
Instances of events and deaths required proof to be classified as cardiovascular, and many out-of-hospital deaths were termed “noncardiovascular” in the absence of such proof. There were 35 deaths from CVD in the treated group and 43 in the placebo group. The death rates for SCD were 16 in the rosuvastatin group versus 25 in the placebo group, suggesting a larger beneficial effect in the SCD component than was reported for total and cardiovascular mortality ().
Table 7 Components of the primary end point reached in the JUPITER study
Influence of the sponsor-affected outcomes
The sponsor, AstraZeneca, had no access to the data or any role in the analyses or manuscript writing.
Side effects
Pharmaceuticals nearly always have side effects, but most do not rise to clinical significance. Adverse events associated with statins have been exceptionally well studied. As the most potent member of its class, rosuvastatin is also associated with unwanted events. Molecular mechanisms have yet to be fully characterized. No one study imposes use of drugs on any patient – use is weighed on the ratio of potential benefits with respect to risks, first by the FDA, then subsequently by the prescribing physician. A vast amount of clinical evidence suggests that, for statins in general, and rosuvastatin in particular, this ratio is large.
JUPITER reported a rise in the number of cases of diabetes in the treatment group, amounting to 270 events, or about a 25% increased risk of developing diabetes. In about 1.4% of prescriptions, rosuvastatin has to be discontinued due to adverse reactions, with the Package Insert quoting the incidence of myalgia at 3.1%, abdominal discomfort, 2.6%, asthenia, 2.5%, and nausea at 2.2%. The frequency of overt myotoxicity, with diagnostic elevations in creatine kinase (CK) 10-fold higher than the upper limit of normal and requiring inpatient care, is in the order of 0.4 per 10,000 person-years.Citation349,Citation350 Less severe myalgia, however, may be responsible for discontinuing statins in 5% to 10% of statin users.Citation351,Citation352 Both myotoxicity and an increase in the incidence of diabetes, as noted in JUPITER, are currently of greatest interest.
Statins raise incidence of diabetes
In a study of 345,417 men, Sukhija et alCitation353 reported that a decrease in insulin sensitivity was a class effect of statin drugs, and found that the change in fasting plasma glucose level in nondiabetic statin users was 7 mg/dL (versus 5 mg/dL in patients not using statins; P < 0.0001), and in diabetic statin users, the rise was 39 mg/dL (versus 32 mg/dL in patients not using statins; P < 0.0001). The effect has subsequently been confirmed for atorvastatinCitation354 and for rosuvastatin,Citation355 which produced a dose-dependent rise in insulin resistance. Using data from the Cholesterol Treatment Trialists’ Collaborators,Citation356 Sattar and colleaguesCitation357 conducted a meta-analysis of 13 randomized statin trials and studied the incidence of diabetes among 91,140 participants. Statin therapy was associated with a 9% increased risk for diabetes, translating to 1 extra case of diabetes per 255 patients treated over 4 years. Absolute risk was low, at 1 case per 1000 patient-years of treatment. During those 4 years, however, 5.4 MIs or cardiovascular deaths and 5.4 coronary revascularizations and strokes would be prevented, amounting to an overall benefit of 9:1 events. Their analysis also indicated that lowering glucose tolerance was a class effect of statins, in agreement with a review of several statin trials prior to JUPITER. Citation310 Baker et alCitation358 systematically reviewed 16 studies and determined there was no class effect of statins upon glucose tolerance in patients without diabetes, and that differences between statins may have accounted for prior findings.
Some side effects of statins are obligatory consequences of HMGR inhibition of the mevalonate pathway used for cholesterol synthesis (), and are molecularly unavoidable, extending throughout the metabolome. Among the intermediate products of this pathway are the 15-carbon farnesyl pyrophosphate and 20-carbon geranylgeranyl pyrophosphate molecules, used to add an isoprenoid group to over 100 signaling proteins in a fundamental post-translational modification known as prenylation.Citation359 This addition of an isoprenoid group is necessary for function of small Rho-family GTPases such as Rac, Rho, and Rab. Some of these GTPases serve as molecular switches, and others are involved in intracellular membrane trafficking, using the lipophilic prenyl group to anchor in membranes.Citation360 Many desirable pleiotropic actions of statins, such as the antioxidant, anti-inflammatory, and antiproliferative propertiesCitation361–Citation363 may be related to decreased ability to prenylate signaling molecules. Inhibition of Rho and its downstream target Rho kinase (ROCK) function is especially important, since elevated ROCK activity may occur in association with elevated CRP levelsCitation364 and contribute to atherosclerosis.Citation365,Citation366 Less desirable consequences of HMGR inhibition may arise from deficiencies in downstream metabolites of the mevalonate pathway such as ubiquinone and dolichol, which are, respectively, ignored and largely unknown. Dolichol, a family of linear polyisoprenols containing 16 to 22 isoprene units, are carriers involved in N-glycosylation of nascent polypeptides, and serve as sites for assembly of oligosaccharides during the formation of glycoproteins, ensuring the membrane fluidity and permeability required for glycoprotein maturation and secretion.
Figure 2 Cholesterol is synthesized via the mevalonate pathway. Acetyl-CoA forms 3-hydroxyl-3-methylglutaryl CoA (HMG-CoA) in several steps. The conversion of 3-hydroxy-3-methylglutaryl (HMG)-CoA to mevalonate, the rate-limiting step in cholesterol synthesis, is catalyzed by HMG-CoA reductase (HMGR), an enzyme within the endoplasmic reticulum. Rosuvastatin is an efficient competitive inhibitor of HMGR, reducing not only mevalonate levels, but also prenylated downstream products. The post-translational process of prenylation is needed for the function of small G proteins, including geranylgeranylation of Rho, Ras, and Rab, necessary for cellular signaling, transduction, and intermembrane translocation. As beneficial as statins are, there are obligatory molecular consequences inherent in their use, some related to their beneficial pleiotropic actions, but also to their side effects. Many steps and enzymes are omitted for clarity.
There are several signaling steps between the insulin receptor and translocation of the glucose transporter GLUT4 from specialized intracellular compartments to the plasma membrane. Individual statins may have different effects upon these steps, and which of them predominate may account for differences on overall glucose tolerance.Citation367 Thus, in one preparation, atorvastatin may improve glucose tolerance, possibly by lowering membrane cholesterol contentCitation368 yet in another report atorvastatin appeared to attenuate the expression of GLUT-4 in adipocytes to lower glucose tolerance.Citation369 In addition, there may be differential effects of statins upon levels of adiponectin, leptin, and other inflammatory mediators that affect glucose intolerance. Differences in lipophilicity among the statins may contribute both to the effects on insulin sensitivity and myotoxicity. Pravastatin, which improves glucose tolerance when compared with atorvastatin, has a relatively favorable effect on beta-cell function.Citation370,Citation371 It has been suggested that pravastatin, hydrophilic but forming weak steric interactions with HMGR, has limited ability to block the mevalonate pathway in cells outside the liver.Citation358 Simvastatin, which worsens glucose tolerance, has a greater affinity for cell membranes due to its lipophilicity, and may block L-type calcium channels, interfering with glucose-induced cytosolic calcium signaling and insulin secretion in beta cells.Citation372 Another possible explanation for statin-induced glucose intolerance includes dysfunctional insulin receptors and/or insulin-like growth factor receptors as a result of impaired glycosylation (see above).Citation373 Finally, by upregulating hepatic LDL receptors, a greater number of triglyceride-rich particles returning to the liver may induce hepatic insulin resistance.Citation374
In view of the large reduction in major vascular events associated with use of statins in diabetics,Citation356 the small increase in diabetes discussed above has not changed clinical practice,Citation375 and further work is needed to delineate its clinical significance.
Statin-induced myopathy
Statin myotoxicity is a major concern of practitioners; part of the reluctance to titrate LDL levels down to guideline targets is a fear of myopathy. Although this phenomenon has received enormous attention from researchers, clinicians, the lay press, and on the internet, its mechanism and optimal management remain uncertain. The spectrum of myopathy or myotoxicity includes myalgia (muscle ache or weakness without CK elevation), myositis (muscle symptoms with raised CK levels), and rhabdomyolysis (symptoms with CK over the upper limit of normal by a factor of at least 10).Citation376 Myalgia is noted in randomized statin trials in the order of <3%, compared to the incidence in outpatient lipid clinics, which varies between 5% and 10%.Citation377 Underreporting is commonly assumed, but individuals with predisposing conditions are carefully screened, and many randomized trials include a run-in period, then fail to randomize candidates with myopathic symptoms.
During vigorous exercise, the phenomenon is accentuated, raising the reported incidence of myalgia up to 25%.Citation378 Statin intolerance among athletes is well known. Factors that predispose to myopathy are increasing age, female gender, hepatic or renal disease, diabetes, polypharmacy, and any condition that diminishes muscle reserve (small frame, frailty, sarcopenia), or causes muscle pathology, including hypothyroidism or hyperthyroidism, metabolic muscle disease, polymyalgia rheumatica, autoimmune diseases with myositis, postoperative status, hypovitaminosis D, chronic alcohol use, and others.
Some adverse reactions may be minimized by avoiding negative drug–drug interactions. As mentioned above, since rosuvastatin is not eliminated through the CYP3A4 pathway, only minimally metabolized by the CYP2C9 enzyme, and does not interfere with P-gp, drugs that inhibit OATP1B1, a transporter that facilitates rosuvastatin uptake in the liver, may clinically be more important offenders than cytochrome P450 inhibitors or substrates. Common drugs usually mentioned that may raise the likelihood of myotoxicity are cyclosporine, gemfibrozil, itraconazole, ketoconazole, fluconazole, lopinavir/rotinavir, atazanavir/ritonavir, fosamprenavir/ritonavir, warfarin, and amiodarone. Some of the quantitative effects of coadministered drugs are summarized in and . As noted in , digoxin coadministered with rosuvastatin only raises the AUC 4%, reflecting the statin is not a P-gp substrate. Genetic polymorphism within SLCO1B1, the gene that encodes OATP1B1, produces a variant which increases susceptibility to statin-induced myopathy.Citation379
Table 8 Effect of coadministered drugs on rosuvastatin systemic exposure
Table 9 Effect of rosuvastatin coadministration with warfarin, digoxin, and an oral contraceptive
Since statins affect many different molecules and signaling systems, the mechanism of statin myopathy also remains uncertain. A relationship to a deficiency of prenylating moieties, farnesyl pyrophosphate and geranylgeranyl pyrophosphate, is again likely. Inability to prenylate seleno-proteins, dolichols, and small GTPases Rho, Ras, and Rac is believed to disturb intracellular trafficking of proteins between membranes needed for muscle growth and repair. Statins specifically activate mechanisms that lead to muscle atrophy in a number of circumstances, mediated by overexpression of atrogin-1, a muscle-specific E3 ubiquitin ligase in the ubiquitin proteasome proteolytic pathway.Citation380–Citation382 Induction of atrogin-1 appears to be significant in the pathogenesis of statin myopathy, but is by no means the only mechanism. Experimental overexpression of peroxisome proliferator- activated receptor-gamma coactivator-1α (PPARγ coactivator 1α or PGC-1α), coactivator of many transcription factors and a regulator of mitochondrial number and function, attenuates statin-induced atrogin-1 expression, protects against statin myotoxicity, and may lead to a therapeutic target.
Skeletal muscle expresses drug transporters such as OATP2B1, high-affinity uptake transporters for both atorvastatin and rosuvastatin.Citation383 A number of efflux transporters, multidrug-resistance-associated proteins 1, 4, and 5, are also expressed on the sarcolemmal membrane of skeletal muscle. Susceptibility to myotoxicity may depend not only on the serum concentration of rosuvastatin, but also locally on the balance between activities of muscle fiber uptake and efflux transporters. For example, in one experimental model, probenecid, which inhibits efflux transporter MRP1, raised myocyte rosuvastatin levels and promoted myotoxicity.Citation384
Lipophilic statins, such as lovastatin or simvastatin, inhibit protein synthesis in skeletal myotubules to a greater extent than hydrophilic statins, such as pravastatin.Citation385 Statins in higher doses may decrease the ability of muscle progenitor cells (satellite cells) to repair and regenerate skeletal muscle. Citation386 Only in part because they severely reduce ubiquinone (coenzyme Q10) levels, statins are associated with multiple defects in muscle mitochondrial anatomy and function.Citation387 Lower mitochondrial volume, mitochondrial DNA loss, reduction in mitochondrial membrane potential, inefficient oxidative phosphorylation, anatomical fractionation, leakage of pro-apoptotic chemicals through mitochondrial membranes, and apoptosis have all been reported. Apoptosis of muscle cells – direct myotoxicity – has been described after acute statin exposure.Citation383,Citation388 Intracellular calcium overload and activation of caspase-3 to initiate apoptosis is yet another proposed mechanism.Citation389 Dolichol is needed for synthesis of α-dystroglycan, a major protein in the skeletal muscle dystrophin–glycoprotein complex, and deficiencies have been linked to muscle dysfunction. Finally, some evidence also implicates immune involvement, which may persist after statin therapy is discontinued.Citation390,Citation391 Four detailed, well-referenced recent reviews of statin myotoxicity are available.Citation392–Citation395
In summary, it appears that the side effects of statins are just as multimechanistic, or “pleiotropic”, as the beneficial actions. Despite these seemingly complex biochemical effects, in practice, the incidence of myopathy and glucose intolerance is far outweighed by the overall benefits of statins in general, and rosuvastatin in particular.Citation396,Citation397 Most serious events may be averted with careful monitoring and avoidance of drug interactions, but individual and genetic susceptibility can unfortunately not yet be predicted clinically. The overwhelming majority of patients tolerate rosuvastatin well. In JUPITER, there were no significant differences in myotoxicity between treatment and control groups.
Conclusion
The challenge of a rising sea of cardiovascular risk, threatening to reverse improved coronary death rates, is immense. The reality is that few individuals will sustain the necessary lifestyle and behavioral changes to lower their risk, and this is amply reflected by the dismal success in weight control. Obesity drives the dual epidemics of diabetes and CHD. Primary prevention, sometimes regarded as an illusion, is only effective if it is done early and intensively. When lifestyle modification fails, reduction of elevated risk factors through pharmacological means is imperative, because by the time they are evident, atherosclerotic processes are already advanced. If we are to stem the tide, simply waiting for a cardiovascular event or diagnosis will no longer suffice.
Asymptomatic individuals randomized in the JUPITER study, many similar to those in the general population, bore a considerable cardiovascular burden, even though they were free from a formal diagnosis of heart disease, diabetes and dyslipidemia. Studies other than JUPITER confirm that higher values of CRP are associated with greater cardiovascular risk, which may assist in the decision of whether to treat or not. With the FDA approval for the use of rosuvastatin in JUPITER-eligible patients with at least one additional cardiovascular risk factor, an additional choice became available to clinicians.
The prevalence of metabolic syndrome in JUPITER participants was about the same as in US adults at the present time. Jupiter demonstrated that within this population, those persons with elevations in CRP levels benefited from rosuvastatin therapy. While, as mentioned, some critics, observing that 41% of JUPITER participants had metabolic syndrome, suggested this diminished the value of the study. However, one can argue that the opposite was true, in that JUPITER demonstrated that rosuvastatin therapy in this syndrome, when CRP was elevated, was effective therapy. The prevalence of metabolic syndrome more closely follows the rise in level of visceral adiposity within the population, now averaging 53%.Citation398 At the moment, the highest prevalence of metabolic syndrome reported in an US subpopulation also stands at 53%.Citation127 The evidence that inflammation plays a critical role in the pathogenesis of components of metabolic syndrome is of high quality.Citation198,Citation199 A recent systematic review and meta-analysis of 87 studies involving 951,083 patients found that metabolic syndrome is associated with a 2-fold increase in risk of CVD, cardiovascular mortality, and stroke, and a 1.5-fold rise in all-cause mortality.Citation399
DeMazumder et alCitation400 noted that the use of global risk assessment tools may result in denial of statin therapy to individuals at low risk when current guidelines are employed, while others with a high absolute risk may not benefit from statin therapy. These authors therefore suggested that statin therapy might be better allocated on the basis of randomized trial evidence rather than global risk scores. Nambi and BallantyneCitation401 proposed a formal protocol using the FRS, lifetime risk, and CRP, CIMT, calcium artery calcification burden, or genetic risk markers for progressive refinement of stratification. CRP measurements may be repeated easily, and are less involved than imaging, with no radiation exposure.
The reaction to JUPITER, many physicians will agree, has been most unusual. The rationale and findings are bracketed by many other independent investigations, but the final interpretation of the data presented is up to each physician. A repeat of JUPITER will probably not occur. The study is not perfect, and limitations are clear and well known. Controversies in medicine may endure for years without resolution. In the individual case, certainly other methods for risk stratification, such as CIMT measurement and coronary artery calcium score, are available. Processes bringing about alterations in each risk factor are different but overlap, and the information their changes bring to the physician’s desk are complementary, not identical. Eventually a place for each will be found in the clinician’s toolbox, but ultimately, the individual practitioner has the choice of where to reach in his armamentarium, the essence of the “art of medicine”. It is encouraging to note that in blog comments written by individuals critical of some results and potential applications of JUPITER, when presented with specific cases, rosuvastatin is in fact being prescribed for high-risk individuals with elevated CRP values in primary prevention, indicating that patients’ needs are being valued with higher priority than personal views.
Almost all JUPITER-eligible patients who would benefit from rosuvastatin have an alternative. Weight loss, especially in conjunction with exercise and dietary changes, are powerful techniques to lower cardiac risk and CRP levelsCitation197,Citation213–Citation222 and in fact would be preferred. The pervasive condition for which rosuvastatin has been found effective in JUPITER differs significantly from other diseases. This “illness” of unrecognized cardiovascular risk is diffuse, significant, difficult to quantitate, but deadly nonetheless. However, it is also largely self-inflicted, with a common cause in poor personal lifestyle choices. A recurring comment that ostensibly healthy people are being subjected to testing and side effects may be, in part, rooted in erroneously equating “asymptomatic” with ideal cardiovascular health – free of risk factors and a likelihood that none will appear in the near futureCitation402 – by the public. Perception of risk by patients is commonly inaccurate, and educational programs have been repeatedly recommended.Citation403
The broader message of JUPITER is, first, it reminds us that the level of cardiovascular risk is currently oppressive, and greater than previously recognized when evaluated by LDL and global risk scores. Second, physicians must go on the offensive, delve into the population, and ferret out the risk, rather than wait for the risk to open their office door.
Today the clinician has a much greater amount of information and a wider variety of techniques from which to choose in order to evaluate individuals for primary prevention. Rosuvastatin will lower risk in JUPITER-eligible subpopulations, but also in many others selected differently for risk, even if one uses age for stratification, simply because the current level of risk is so high. Whatever markers or techniques are chosen, a fresh view of preventive care is before us, and action is now imperative. New guidelines in preparation will hopefully provide even greater direction in maximizing returns in primary prevention and improve future outcomes in our patients.
Acknowledgment
The author thanks Michelle Delaney for her suggestions, computer skills, and astuteness in the preparation of this manuscript.
Disclosure
The author states that he has not received any funds or favors from any private or public entity, corporation, agency, or other source related to this work.
References
- USDHHS, National Center for Health StatisticsSecond National Health and Nutrition Examination Survey (NHANES II)Hyattsville MDCDC19761980
- USDHHS, National Center for Health StatisticsSecond National Health and Nutrition Examination Survey (Continuous NHANES)Hyattsville MDCDC19992002
- YoungFCapewellSFordESCritchleyJACoronary mortality declines in the US between 1980 and 2000. Quantifying the contributions from primary and secondary preventionAm J Prev Med20103922823420709254
- FordESCapewellSCoronary heart disease mortality among young adults in the US from 1980 to 2002: concealed leveling or mortality ratesJ Am Coll Cardiol2007502128213218036449
- CDC National Center for Health StatisticsCDC mortality data, 2008: CDC latest release mortality data, 2005 www.cdc.gov/nchs/fastats/deaths.htmAccessed 2010 Oct 7
- SackerAHeadJBartleyMImpact of coronary heart disease on health functioning in an aging population: are there differences according to socioeconomic positionPsychosom Med20087013314018256343
- AllenderSScarboroughPPetoVEuropean cardiovascular disease statistics 2008European Heart Network, 2008 www.heart-stats.org/uploads/documents%5Cproof30NOV2007.pdfAccessed 2010 Oct 7
- WHO Statistical Information SystemMortality data for ICD 10 codings www.who.int/whosis/database/mort/download/ftp/morticd10.zipAccessed 2010 Oct 7
- RidkerPMDanielsonEFonsecaFAfor JUPITER Study GroupRosuvastatin to prevent vascular events in men and women with elevated C-reactive proteinN Engl J Med20083592195220718997196
- ThompsonDPepysMBWoodSPThe physiological structure of human C-reactive protein and its complex with phosphocholineStructure1999716917710368284
- PepysMBHirschfieldGMC-reactive protein: a critical updateJ Clin Invest20031111805181212813013
- RidkerPMCushmanMStampferMJTracyRPHennekensCHInflammation, aspirin, and the risk of cardiovascular disease in apparently healthy menN Engl J Med19973369739799077376
- HanssonGKLibbyPThe immune response in atherosclerosis: a double-edged swordNat Rev Immunol2006650851916778830
- HwangSJBallantyneCMSharrettARCirculating adhesion molecules VCAM-1, ICAM-1, and E-selectin in carotid atherosclerosis and incident coronary heart disease cases: the Atherosclerosis Risk in Communities (ARIC) studyCirculation199796421942259416885
- RidkerPMRifaiNStampferMJHennekensCHPlasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy menCirculation20001011767177210769275
- RossRAtherosclerosis–an inflammatory diseaseN Engl J Med19993401151269887164
- LibbyPRidkerPMInflammation and atherothrombosis: from population biology and bench research to clinical practiceJ Am Coll Cardiol200648A3346
- HanssonGKInflammation, atherosclerosis, and coronary artery diseaseN Engl J Med20053521685169515843671
- LibbyPNahrendorfMPittetMJSwirskiFKDiversity of denizens of the atherosclerotic plaque: not all monocytes are created equalCirculation20081173168317018574058
- MachFSchoenbeckUBonnefoyJYPoberJLibbyPActivation of monocyte/macrophage functions related to acute atheroma complication by ligation of CD40. Induction of collagenase, stromelysin, and tissue factorCirculation1997963963999244201
- SpagnoliLGBonannoEMaurielloAMulticentric inflammation in epicardial coronary arteries of patients dying of acute myocardial infarctionJ Am Coll Cardiol2002401579158812427409
- AbbateABonannoEMaurielloAWidespread myocardial inflammation and infarct-related artery patencyCirculation2004110465015210601
- LombardoABiasucciLMLanzaGAInflammation as a possible link between coronary and carotid plaque instabilityCirculation20041093158316315184282
- NakajimaTSchulteSWarringtonKJT-cell-mediated lysis of endothelial cells in acute coronary syndromesCirculation200210557057511827921
- BlakeGJRidkerPMInflammatory bio-markers and cardiovascular risk predictionJ Intern Med200225228329412366601
- EspositoKGiuglianoDDiet and inflammation: a link to metabolic and cardiovascular diseasesEur Heart J200627152016219650
- FreedmanJELoscalzoJPlatelet–monocyte aggregates: bridging thrombosis and inflammationCirculation20021052130213211994242
- SteinhublSRPlatelets as mediators of inflammationHematol Oncol Clin North Am20072111512117258122
- NettletonJAMatijevicNFollisJLFolsomARBoerwinkleEAssociations between dietary patterns and flow cytometry-measured biomarkers of inflammation and cellular activation in the Atherosclerosis Risk in Communities (ARIC) Carotid Artery MRI StudyAtherosclerosis201021226026720537646
- LibbyPInflammation in atherosclerosisNature200242086887412490960
- RidkerPMTesting the inflammatory hypothesis of atherothrombosis: scientific rationale for the cardiovascular inflammation reduction trial (CIRT)J Thromb Haemost20097Suppl 133233919630828
- BrugalettaSBiasucciLMPinnelliMNovel anti-inflammatory effect of statins: reduction of CD4+CD28null T lymphocyte frequency in patients with unstable anginaHeart20069224925016415193
- TaubesGDoes Inflammation cut to the heart of the matterScience200229624224511951014
- WilliamsKJTabasIAtherosclerosis and inflammationScience200229752152212143880
- RidkerPMHennekensCHBuringJERifaiNC-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in womenN Engl J Med200034283684310733371
- PackardRRSLibbyPInflammation in atherosclerosis: from vascular biology to biomarker discovery and risk predictionClin Chem200843243818160725
- AltmanRRisk factors in coronary atherosclerosis ather-inflammation: the meeting pointThrombosis J200314
- VorchheimerDAFusterVInflammatory markers in coronary artery disease. Let prevention douse the flamesJAMA20012862154215611694158
- RossRThe pathogenesis of atherosclerosis: a perspective for the 1990sNature19933628018098479518
- CybulskyMIGimbroneMAJrEndothelial expression of a mono-nuclear leukocyte adhesion molecule during atherogenesisScience19912517887911990440
- BonettiPOLermanLOLermanAEndothelial dysfunction: a marker of atherosclerotic riskArterioscler Thromb Vasc Biol20032316817512588755
- LiuzzoGBiasucciLMGallimoreJLThe prognostic value of C-reactive protein and serum amyloid A protein in severe unstable anginaN Engl J Med19943314174247880233
- BiasucciLMVitelliALiuzzoGElevated level of interleukin-6 in unstable anginaCirculation1996948748778790019
- LibbyPRidkerPMMaseriAInflammation and atherosclerosisCirculation20021051135114311877368
- WuKKAleksicNBallantyneChMAhnChJunejaHBoerwinkleEInteraction between soluble thrombomodulin and Intercellular Adhesion Molecule-1 in predicting risk of coronary heart diseaseCirculation20031071729173212668515
- BhattDLTopolEJNeed to test the arterial inflammation hypothesisCirculation200210613614012093783
- KereiakesDJThe fire that burns within. C-reactive proteinCirculation200310737337412551855
- RidkerPMHigh-sensitivity C-reactive protein, inflammation, and cardiovascular risk: from concept to clinical practice to clinical benefitAm Heart J2004148S192615211329
- DhingraRGonaPNamB-HC-reactive protein, inflammatory conditions, and cardiovascular disease riskAm J Med20071201054106218060926
- GustafsonBHammarstedtAAnderssonCXSmithUInflamed adipose tissue: a culprit underlying the metabolic syndrome and atherosclerosisAtheroscler Thromb Vasc Biol20072722762283
- LiuYYuHZhangYZhaoYTLRs are important inflammatory factors in atherosclerosis and may be a therapeutic targetMed Hypoth200870314316
- ViraniSSPolsaniVRNambiZVNovel markers of inflammatioin in atherosclerosisCurr Atheroscler Rep20081016417018417072
- PeisajovichAMarnellLMoldCDu ClosTWC-reactive protein at the interface between innate immunity and inflammationExpert Rev Clin Immunol2008437939020476927
- IkonomidisIStamatelopoulosKLekakisJVamvakouGDKremastinosDTInflammatory and non-invasive vascular markers: the multimarker approach for risk stratification in coronary artery diseaseAtherosclerosis200819931118378239
- OtakeHShiteJShinkeTRelation between plasma adiponectin, high sensitivity C-reactive protein, and coronary plaque components in patients with acute coronary syndromeAm J Cardiol20081011718157956
- ChamberlainJFrancisSBrookesZInterleukin-1 regulates multiples atherogenic mechanisms in response to fat feedingPLoS ONE20094e507319347044
- LibbyPOkamotoYRochaVZFolcoEInflammation in atherosclerosis: transition from theory to practiceCirc J20107421322020065609
- IkedaUInflammation and coronary artery diseaseCurr Vasc Pharmacol20031657015320854
- HeinischRHZanettiCRCominFFernandesJLRamiresJASerranoCVJrSerial changes in plasma levels of cytokines in patients with coronary artery diseaseVasc Health Risk Manag2005124525017319110
- RidkerPMInflammation, high-sensitivity C-reactive protein, and vascular protectionTex Heart Inst J201037404120200625
- CurtissLKReversing atherosclerosisN Eng J Med200936011441146
- TillettWSFrancisTJrSerological reactions in pneumonia with a non-protein fraction of pneumococcusJ Exp Med19305256157119869788
- NorataGDMarchesiPPulakazhiVKDeficiency of the long pentraxin PTX3 promotes vascular inflammation and atherosclerosisCirculation200912069970819667236
- HanssonGKLibbyPSchönbeckUYanZQInnate and adaptive immunity in the pathogenesis of atherosclerosisCirc Res20029128129112193460
- Abou-RayaAAbou-RayaSInflammation: a pivotal link between autoimmune diseases and atherosclerosisAutoimmun Rev2006533133716782558
- SunJHartvigsenKChouM-YDeficiency of antigen-presenting cell invariant chain reduces atherosclerosis in miceCirculation201012280882020697023
- OkemefunaAINanRMillerAGorJPerkinsSJComplement factor H binds at two independent sites to C-reactive protein in acute phase concentrationsJ Biol Chem20102851053106519850925
- Bodman-SmithKBMelendezAJCampbellIHarrisonPTAllenJMRaynesJGC-reactive protein-mediated phagocytosis and phospholipase D signaling through the high-affinity receptor for immunoglobulin G (FcγRI)Immunology200220725226012383205
- GabayCKushnerIAcute-phase proteins and other systemic responses to inflammationN Eng J Med1999340448454
- VigushinDMPepysMBHawkinsPNMetabolic and scintigraphic studies of radioiodinated human C-reactive protein in health and diseaseJ Clin Invest199391135113578473487
- LauDCDhillonBYanHSzmitkoPEVermaSAdipokines: molecular links between obesity and atheroslcerosisAm J Physiol Heart Circ Physiol2005288H2031204115653761
- BrullDJSerranoNZitoFHuman CRP gene polymorphism influences CRP levels: implications for the prediction and pathogenesis of coronary heart diseaseArterioscler Thromb Vasc Biol2003232063206912842840
- KathiresanSLarsonMGVasanRSContribution of clinical correlates and 13 C-reactive protein gene polymorphisms to inter-individual variability in serum C-reactive protein levelCirculation20061131415142316534007
- ShahTNewcombePSmeethLAncestry as a determinant of mean population C-reactive protein values: implications for cardiovascular risk predictionCirc Cardiovasc Genet2010343644420876875
- RückerlRGrevenSLjungmanPfor the Airgene studyAir pollution and inflammation (interleukin-6, C-reactive protein, fibrinogen) in myocardial infarction survivorsEnviron Health Perspect20071151072108017637925
- KingDEEganBMWoolsonRFMainousAGIIIAl-SolaimanYJesriAEffect of a high-fiber diet vs a fiber-supplemented diet on C-reactive protein levelArch Intern Med200716750250617353499
- BoSDurazzoMGuidiSDietary magnesium and fiber intakes and inflammatory and metabolic indicators in middle-aged subjects from a population-based cohortAm J Clinical Nutrition2006841062106917093158
- KingDEMainousAGIIIEganBMWoolsonRFGeeseyMEEffect of psyllium fiber supplementation on C-reactive protein: the trial to reduce inflammatory markers (TRIM)Ann Fam Med2008610010618332401
- AjaniUAFordESMokdadAHDietary fiber and C-reactive protein: findings from national health and nutrition examination survey dataJ Nutr20041341181118515113967
- ZampelasAPanagiotakosDBPitsavosCAssociations between coffee consumption and inflammatory markers in healthy persons: the ATTICA studyAm J Clin Nutr20048086286715447891
- CavicchiaPPSteckSEHurleyTFA new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive proteinJ Nutr20091392365237219864399
- MastersRCLieseADHaffnerSMWagenknechtLEHanleyAJWhole and refined grain intakes are related to inflammatory protein concentrations in human plasmaJ Nutr201014058759420089789
- EsmaillzadahAKimiagarMMehrabiYAzadbakhtLHuFBWillettWCFruit and vegetable intakes, C-reactive protein, and the metabolic syndromeAm J Clin Nutr2006841489249717158434
- MicallefMAMunroIAGargMLAn inverse relationship between plasma n-3 fatty acids and C-reactive protein in healthy individualsEur J Clin Nutr2009631154115619352379
- YenMLYangCYYenBLIncreased high sensitivity C-reactive protein and neutrophil count are related to increased standard cardiovascular risk factors in healthy Chinese menInt J Cardiol200611019119816305810
- DaneshJWheelerJGHirschfieldGMC-reactive protein and other circulating markers of inflammation in the prediction of coronary heart diseaseN Engl J Med20043501387139715070788
- FaberDRvan der GraafYWesterinkJVisserenFLJIncreased visceral adipose tissue mass is associated with increased C-reactive protein in patients with manifest vascular diseasesAtherosclerosis201021227428020494358
- ImhofAFroehlichMBrennerHEffect of alcohol consumption on systemic markers of inflammationLancet200135776376711253971
- AlbertMAGlynnRJRidkerPMAlcohol consumption and plasma concentration of C-reactive proteinCirculation200310744344712551869
- DreonDMSlavinJLPhinneySDOral contraceptive use and increased plasma concentration of C-reactive proteinLife Sci2003731245125212850240
- FrohlichMMuhlbergerNHankeHMarkers of inflammation in women on different hormone replacement therapiesAnn Med20033535336112952022
- BlackSKushnerISamolsDC-reactive proteinJ Biol Chem2004279484874849015337754
- McDadeTWRutherfordJNAdairLKuzawaCPopulation differences in associations between C-reactive protein concentration and adiposity: comparison of young adults in the Philippines and the United StatesAm J Clin Nutr2009891237124519225115
- RussellAICunninghame GrahamDSShepherdCPolymorphism at the C-reactive protein locus influences gene expression and predisposes to systemic lupus erythematosusHum Mol Genet20041313714714645206
- JönsenAGunnarssonIGullstrandBAssociation between SLE nephritis and polymorphic variants of the CRP and Fcgamma;RIIIa genesRheumatology (Oxford)2007461417142117596285
- EdbergJCWuJLangefeldCDGenetic variation in the CRP promoter: association with systemic lupus erythematosus (SLE)Hum Mol Genet2008171147145518182444
- GrafJScherzerRGrunfeldCImbodenJLevels of C-reactive protein associated with high and very high cardiovascular risk are prevalent in patients with rheumatoid arthritisPLoS ONE20094e624219606218
- CoventryBJAshdownMLQuinnMAMarkovicSNYatomi-ClarkeSLRobinsonAPCRP identifies homeostatic immune oscillations in cancer patients: a potential treatment targeting toolJ Transl Med2009710219948067
- Morin-PapunenLRautioKRuokonenAHedbergPPuukkaMTapanainenJSMetformin reduces serum C-reactive protein levels in women with polycystic ovary syndromeJ Clin Endocrinol Metab2003884649465414557435
- TosiFDorizziRCastelloRBody fat and insulin resistance independently predict increased serum C-reactive protein in hyperandrogenic women with polycystic ovary syndromeEur J Endocrinol200916173774519713424
- SathyapalanTKilpatrickESCoadyAMAtkinSLThe effect of atorvastatin in patients with polycystic ovary syndrome: a randomized double-blind placebo-controlled studyJ Clin Endocrinol Metab20099410310818940877
- HoegerKMPolycystic ovary syndrome, inflammation and statins: do we have the right targetJ Clin Endocrinol Metab200994353719126632
- De BeerFSoutarAKBaltzMLTraynerIMFeinsteinAPepysMBLow density lipoprotein and very low density lipoprotein are selectively bound by aggregated C-reactive proteinJ Exp Med19821562302427086355
- ZhangYXCliffWJSchoeflGIHigginsGCoronary C-reactive protein distribution: its relation to development of atherosclerosisAtherosclerosis199914537537910488966
- PasceriVWillersonJTYehETDirect proinflammatory effect of C-reactive protein on human endothelial cellsCirculation20001022165216811056086
- TorzewskiMRistCMortensenRFC-reactive protein in the arterial intima: role of C-reactive protein receptor-dependent monocyte recruitment in atherogenesisArterioscler Thromb Vasc Biol2000202094209910978254
- DevarajSDavisBSimonSIJialalICRP promotes monocyte-endothelial cell adhesion via Fcgamma;receptors in human aortic endothelial cells under static and shear flow conditionsAm J Physiol Heart Circ Physiol2006291H1170117616603696
- RockerCManolovDEKuzmenkinaEVAffinity of C-reactive protein toward FcgammaRI is strongly enhanced by the gamma-chainAm J Pathol200717075576317255341
- SchwartzROsborne-LawrenceSHahnerLC-reactive protein downregulates endothelial NO synthase and attenuates reendothelialization in vivo in miceCirc Res20071001452145917446434
- SzmitkoPEVermaSC-reactive protein and reendothelialization: NO involvementCirc Res20071001405140717525379
- XingDHageFGChenYFExaggerated neointima formation in human C-reactive protein transgenic mice is IgG Fc receptor type 1 (Fc gamma RI)-dependentAm J Pathol2008172223018063701
- SalioMChimentiSde AngelisNCardioprotective function of the long pentraxin PTX3 in acute myocardial infarctionCirculation20081171055106418268142
- Van VréEABultHHoymansVYvan TendelooFIVrintsCJBosmansJMHuman C-reactive protein activates monocyte-derived dendritic cells and induces dendritic cell-mediated T-cell activationArterioscler Thromb Vasc Biol20082851151818218989
- FujitaYKakinoANishimichiNOxidized LDL receptor LOX-1 binds to C-reactive protein and mediates its vascular effectsClin Chem20095528529419074514
- FilepJGPlatelets affect the structure and function of C-reactive proteinCirc Res200910510911119608987
- JinCLuLZhangRYAssociation of serum glycated albumin, C-reactive protein and ICAM-1 levels with diffuse coronary artery disease in patients with type 2 diabetes mellitusClin Chim Acta2009408454919615354
- RidkerPMC-reactive protein: eighty years from discovery to emergence as a major risk marker for cardiovascular diseaseClin Chem20095520921519095723
- GelukCAPostWJHillegeHLC-reactive protein and angiographic characteristics of stable and unstable coronary artery disease: data from the prospective PREVEND cohortAtherosclerosis200819637238217157301
- NabataAKurokiMUebaHC-reactive protein induces endothelial cell apoptosis and matrix metalloproteinase-9 production in human mononuclear cells: implications for the destabilization of atherosclerotic plaqueAtherosclerosis200819612913517531242
- SciricaBMCannonCPSabatineMSConcentrations of C-reactive protein and B-type natriuretic peptide 30 days after acute coronary syndromes independently predict hospitalization for heart failure and cardiovascular deathClin Chem20095526527319074516
- SciricaBMMorrowDACannonCPThrombolysis in Myocardial Infarction (TIMI) Study GroupClinical application of C-reactive protein across the spectrum of acute coronary syndromesClin Chem2007531800180717717132
- SciricaBMMorrowDAIs C-reactive protein an innocent bystander or proatherogenic culprit? The verdict is still outCirculation20061132128213416651484
- VermaSDevarajSJialalIIs C-reactive protein an innocent bystander or proatherogenic culprit? C-reactive protein promotes atherothrombosisCirculation20061132135215016671184
- JialalIVermaSDevarajSInhibition of endothelial nitric oxide synthase by C-reactive protein: clinical relevanceClin Chem20095520620819095724
- GuanHWangPHuiREdinMLZeldinDCWangDWAdeno-associated virus-mediated human C-reactive protein gene delivery causes endothelial dysfunction and hypertension in ratsClin Chem20095527428419056836
- RadjeshJBisoendialSBoekholdtMVergeerMStroesESGKasteleinJJPC-reactive protein is a mediator of cardiovascular diseaseEur Heart J2010312087209120685682
- SinclairKABogartABuchwaldDHendersonJAThe prevalence of metabolic syndrome and associated risk factors in Northern Plains and Southwest American IndiansDiabetes Care2010923 [Epub ahead of print]
- KearneyMTTargeting the endothelium to prevent diabetes-related atherosclerosisDiab Vasc Dis Res2010717720699387
- FordESGilesWHMyersGLManninoDMPopulation distribution of high-sensitivity C-reactive protein among US men: findings from national health and nutrition examination survey 1999–2000Clin Chem200349686690 http://www.clinchem.org/cgi/content/full/49/4/68612651834
- Centers for Disease Control and PreventionNHANES 1999–2000 public data release file documentation http://www.cdc.gov/nchs/data/nhanes/gendoc.pdfAccessed 2010 Oct 18
- RifaiNRidkerPMPopulation distributions of C-reactive protein in apparently healthy men and women in the United States: implication for clinical interpretationClin Chem20034966666912651826
- WoloshinSSchwartzLMDistribution of C-reactive protein values in the United StatesN Eng J Med200535216111613
- KushnerIRzewnickiWSamolsDWhat does minor elevation of C-reactive protein signify?Am J Med2006119166.e17166.e2816443421
- KaoPCShieshS-CWuTJSerum C-reactive protein as a marker for wellness assessmentAnn Clin Lab Sci20063616316916682512
- KoenigWSundMFrohlichMC-reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992Circulation1999992372429892589
- MillerMZhanMHavasSHigh attributable risk of elevated C-reactive protein level to conventional coronary heart disease risk factors: the Third National Health and Nutrition Examination SurveyArch Intern Med20051652063206816216995
- GreenfieldJRSamarasKJenkinsABObesity is an important determinant of baseline serum C-reactive protein concentration in monozygotic twins, independent of genetic influencesCirculation20041093022302815184288
- CurrieCJPooleCDConwayPEvaluation of the association between the first observation and the longitudinal change in C-reactive protein, and all-cause mortalityHeart20089445746217761503
- MarsikCKazemi-ShiraziLSchickbauerTC-reactive protein and all-cause mortality in a large hospital-based cohortClin Chem20085434334918156283
- KravitzBACorradaMMKawasCHHigh levels of serum C-reactive protein are associated with greater risk of all-cause mortality, but not dementia, in the oldest-old: results from the 90+ studyJ Am Ger Soc200957641646
- WasselCLBarrett-ConnorELaughlinGAAssociation of circulating C-reactive protein and interleukin-6 with longevity into the 80s and 90s: The Rancho Bernardo StudyJ Clin Endocrinol Metab2010954748475520660034
- RidkerPMRifaiNRoseLBuringJECookNRComparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular eventsN Engl J Med20023471557156512432042
- DiazJJArguellesJMalagaIC-reactive protein is elevated in the offspring of parents with essential hypertensionArch Dis Child20079230430817158147
- ManciaGde BackerGDominiczakA2007Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)Eur Heart J2007281462153617562668
- RidkerPMDanielsonERifaiNGlynnRJValsartan, blood pressure reduction, and C-reactive protein: primary report of the Val-MARC trialHypertension200648737916714425
- SessoHDBuringJERifaiNBlakeGJGazianoJMRidkerPMC-reactive protein and the risk of developing hypertensionJAMA20032902945295114665655
- SathiyapriyaVNandeeshaHSelvarajNBobbyZAgrawalAPavithranPAssociation between protein-bound sialic acid and high-sensitivity C-reactive protein in essential hypertension: a possible indication of underlying cardiovascular riskAngiology20095972172618388037
- LandeMBPearsonTAVermilionRPAuingerPFernandezIDElevated blood pressure, race/ethnicity, and C-reactive protein levels in children and adolescentsPediatrics20081221252125719047242
- BlackGJRifaiNBuringJERidkerPMBlood pressure, C-reactive protein, and risk of future cardiovascular eventsCirculation20031082993299914638538
- PerticoneFMaioRSciacquaAEnodthelial dysfunction and C-reactive protein are risk factors for diabetes in essential hypertensionDiabetes20085716717117928395
- VardasPEMarketouMECRP in non-dippers: new perspectives and old queriesJ Human Hypertension200822447449
- VeerabhadrappaPDiazKMFeairhellerDLEnhanced blood pressure variability in a high cardiovascular risk group of African Americans: FIT4 Life StudyJ Am Soc Hypertens2010418719520885987
- IijimaRByrneRANdrepepaGPre-procedural C-reactive protein levels and clinical outcomes after percutaneous coronary interventions with and without abciximab: pooled analysis of four ISAR trialsHeart20099510711218801777
- IshiiHToriyamaTAoyamaTPrognostic values of C-reactive protein levels on clinical outcome after implantation of sirolimuseluting stents in patients on hemodialysisCirc Cardiovasc Interv2009251351820031768
- IliodromitisEKKyrzopoulosSParaskevaidisIAIncreased C reactive protein and cardiac enzyme levels after coronary stent implantation. Is there protection by remote ischaemic preconditioningHeart2006921821182616855045
- KangasniemiOPBiancariFLuukkonenJPreoperative C-reactive protein is predictive of long-term outcome after coronary artery bypass surgeryEur J Cardiothorac Surg20062998398516682213
- WypasekEUndasASniezek-MaciejewskaMThe increased plasma C-reactive protein and interleukin-6 levels in patients under-going coronary artery bypass grafting surgery are associated with the interleukin-6-174G. C gene polymorphismAnn Clin Biochem20104734334920592333
- LoBFijnheerRNierichAPBruinsPKalkmanCJC-reactive protein is a risk indicator for atrial fibrillation after myocardial revascularizationAnn Thorac Surg2005791530153515854929
- KardysIKnetschAMBleuminkGSC-reactive protein and risk of heart failure. The Rotterdam StudyAm Heart J200615251452016923423
- WilliamsESShahSJAliSNaBYSchillerNBWhooleyMAC-reactive protein, diastolic dysfunction, and risk of heart failure in patients with coronary disease: Heart and Soul StudyEur J Heart Fail200810636918160340
- BraunwaldEBiomarkers in heart failureN Engl J Med20083582148215918480207
- BozkurtBMannDLDeswalABiomarkers of inflammation in heart failureHeart Fail Rev20101533134119363700
- AraujoJPLourencoPAzevedoAPrognostic value of high-sensitivity C-reactive protein in heart failure: a systematic reviewJ Cardiac Fail200915256266
- CollinsonPOConcentrations of C-reactive protein and B-type natriuretic peptide 30 days after acute coronary syndromes independently predict hospitalization for heart failure and cardiovascular death: just another brick in the wallClin Chem20095520320519095728
- LamblinNMouquetFHennacheBHigh-sensitivity C-reactive protein: potential adjunct for risk stratification in patients with stable congestive heart failureEur Heart J2005262245225016183690
- AnandISLatiniRFloreaVGC-reactive protein in heart failure: prognostic value and the effect of valsartanCirculation20051121428143416129801
- VasanRSSullivanLMRoubenoffRInflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: the Framingham Heart StudyCirculation20031071486149112654604
- ConenDRexrodeKMCreagerMARidkerPMPradhanADMetabolic syndrome, inflammation, and risk of symptomatic peripheral artery disease in women: a prospective studyCirculation20091201041104719738135
- PandeRLPerlsteinTSBeckmanJACreagerMAAssociation of insulin resistance and inflammation with peripheral arterial disease: the National Health and Nutrition Examination Survey, 1999 to 2004Circulation20081181334118559705
- SchlagerOExnerMMlekuschWC-reactive protein predicts future cardiovascular events in patients with carotid stenosisStroke2007381263126817322087
- AlbertCMMaJRifaiNProspective study of C-reactive protein, homocysteine, and plasma lipid levels as predictors of sudden cardiac deathCirculation200241052595259912045163
- SpoonerPMZipesDPSudden death predictors: an inflammatory associationCirculation20021052574257612045156
- BeriAContractorTKhasnisAThakurRStatins and the reduction of sudden cardiac death: antiarrhythmic or anti-ischemic effectAm J Cardiovasc Drugs20101015516420524717
- CorbalánRBraunSPereiraJNavarreteCGonzalezIC-reactive protein and atrial fibrillation: evidence for the presence of inflammation in the perpetuation of the arrhythmiaInt J Cardiol200610832633115985301
- ConenDRidkerPMEverettBMA multimarker approach to assess the influence of inflammation on the incidence of atrial fibrillation in womenEur Heart J2010311730173620501475
- MarottSCWNordestgaardBGZachoJDoes elevated C-reactive protein increase atrial fibrillation risk? A mendelian randomization of 47,000 individuals from the general populationJ Am Coll Cardiol20105678979520797493
- BlangyHSadoulNDoussetBSerum BNP, hs-C-reactive protein, procollagen to assess the risk of ventricular tachycardia in ICD recipients after myocardial infarctionEuropace2007972472917526509
- JeevananthamVSinghNIzuoraKD’souzaJPHisDHCorrelation of high sensitivity C-reactive protein and calcific aortic valve diseaseMayo Clin Proc20078217117417290723
- JonesPDavidsonMSteinEComparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial)Am J Cardiol20039215216012860216
- AyCTenglerTVormittagRVenous thromboembolism a manifestation of the metabolic syndromeHaematologica20079237438017339187
- QuarckRNawrotTMeynsBDelcroixMC-reactive protein a new predictor of adverse outcome in pulmonary arterial hypertensionJ Am Coll Cardiol2009531211121819341863
- SoinioMMarniemiJLaaksoMHigh-sensitivity C-reactive protein and coronary heart disease mortality in patients with type 2 diabetes: a 7-year follow-up studyDiabetes Care20062932933316443882
- MarcovecchioMLGianniniCWidmerBC-reactive protein in relation to the development of microalbuminuria in type 1 diabetesDiabetes Care20083197497618235049
- DehghanAKardysIde MaatMPMGenetic variation, C-reactive protein levels, and incidence of diabetesDiabetes20075687287817327459
- KahnSEZinmanBHaffnerSMObesity is a major determinant of the association of C-reactive protein levels and the metabolic syndrome in type 2 diabetesDiabetes2006552357236416873701
- GoldbergRBCytokine and cytokine-like inflammation markers, endothelial dysfunction, and imbalanced coagulation in development of diabetes and its complicationsJ Clin Endocrinol Metab2009943171318219509100
- RidkerPMPareGParkerALoci related to metabolic-syndrome pathways including LEPR, HNF1A, IL6R, and GCKR associate with plasma C-reactive protein: the Women’s Genome Health StudyAm J Hum Genet2008821185119218439548
- RidkerPMBuringJECookNRRifaiNC-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: an 8-year follow-up of 14,719 initially healthy American womenCirculation200310739139712551861
- Moreno-NavarreteJMMartinez-BarricarteRCatalanVComplement factor H is expressed in adipose tissue in association with insulin resistanceDiabetes20105920020919833879
- JialalIThe role of the laboratory in the diagnosis of the metabolic syndromeAm J Clin Pathol2009132216116219605808
- SteinbergerJDanielsSREckelRHAmerican Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing; and Council on Nutrition, Physical Activity, and Metabolism. Progress and challenges in metabolic syndrome in children and adolescents: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular Nursing; and Council on Nutrition, Physical Activity, and MetabolismCirculation200911962864719139390
- CornierMADabeleaDHernandezTLThe metabolic syndromeEndocr Rev20082977782218971485
- SuzukiTKatzRJennyNSMetabolic syndrome, inflammation, and incident heart failure in the elderly: the Cardiovascular Health StudyCirc Heart Fail2008124224819808298
- YouTNicklasBJDingJThe metabolic syndrome is associated with circulating adipokines in older adults across a wide range of adiposityJ Gerontol A Biol Sci Med Sci20086341441918426966
- DaiDFLinJWKaoJHThe effects of metabolic syndrome versus infectious burden on inflammation, severity of coronary atherosclerosis, and major adverse cardiovascular eventsJ Clin Endocrinol Metab2007922532253717426096
- YeXYuZLiHFrancoOHLiuYLinXDistributions of C-reactive protein and its association with metabolic syndrome in middle-aged and older Chinese peopleJ Am Coll Cardiol2007491798180517466231
- PitsavosCPanagiotakosDBTzimaNDiet, exercise, and C-reactive protein levels in people with abdominal obesity: the ATTICA epidemiological studyAngiology20075822523317495273
- DevarajSValleggiDSiegelDJialalIRole of C-reactive protein in contributing to increased cardiovascular risk in metabolic syndromeCurr Atheroscler Rep20101211011820425246
- WangANakayamaTInflammation, a link between obesity and cardiovascular diseaseMediators Inflamm2010201053591820847813
- AlyanOMetinFKacmazFHigh levels of high sensitivity C-reactive protein predict the progression of chronic rheumatic mitral stenosisJ Thromb Thrombolysis200928636918622582
- LeeHMLeTVLopezVAWongNDAssociation of C-reactive protein with reduced forced vital capacity in a nonsmoking US population with metabolic syndrome and diabetesDiabetes Care2008312000200218591402
- MagnussenHWatzHSystemic inflammation in chronic obstructive pulmonary disease and asthma: relation with comorbiditiesProc Am Thorac Soc2009664865120008868
- EickhoffPValipourAKissDDeterminants of systemic vascular function in patients with stable chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20081781211121818836149
- WahbaIMMakRHObesity and obesity-initiated metabolic syndrome: mechanistic links to chronic kidney diseaseJ Am Soc Nephrol20072550562
- ChenHYChiuYLHsuSPElevated C-reactive protein level in hemodialysis patients with moderate/severe uremic pruritus: a potential mediator of high overall mortalityQJM201010383784620350963
- LahrachHGhalimNTakiHSerum paraoxonase activity, high-sensitivity C-reactive protein, and lipoprotein disturbances in end-stage renal disease patients on long-term hemodialysisJ Clin Lipidol200824350
- LuiMMLamJCMakHK-FC-reactive protein is associated with obstructive sleep apnea independent of visceral obesityChest200913595095619225064
- SchizaSEMermigkisCPanagiotisC-reactive protein evolution in obstructive sleep apnoea patients under CPAP therapyEur J Clin Invest20104096897520629709
- ZekaASullivanJRVokonasPSSparrowDSchwartzJInflammatory markers and particulate air pollution: characterizing the pathway to diseaseInt J Epidemiol2006351347135416844771
- DixonJBHaydenMJLambertGWRaised CRP Levels in obese patients: symptoms of depression have an independent positive associationObesity2008162010201518497736
- HakAEStehouwerCDBotsMLAssociations of C-reactive protein with measures of obesity, insulin resistance, and subclinical atherosclerosis in healthy, middle-aged womenArterioscler Thromb Vasc Biol1999191986199110446082
- McLaughlinTAbbasiFLamendolaCDifferentiation between obesity and insulin resistance in the association with C-reactive proteinCirculation20021062908291212460870
- WeeCCMukamalKJHuangADavisRBMcCarthyEPMittlemanMAObesity and C-reactive protein levels among white, black, and hispanic US adultsObesity20081687588018379563
- SkinnerACSteinerMJHendersonFWPerrinEMMultiple markers of inflammation and weight status: cross-sectional analyses throughout childhoodPediatrics2010125e801e80920194272
- PuglisiMJFernandezMLModulation of C-reactive protein, tumor necrosis factor α, and adiponectin by diet, exercise, and weight lossJ Nutr20081382293229619022947
- SacheckJPediatric obesity: an inflammatory conditionJPEN J Parenter Enteral Nutr20083263363718974243
- RankinJWTurpynADLow carbohydrate, high fat diet increases C-reactive protein during weight lossJ Am Coll Nutr20072616316917536128
- SelvinEPaynterNPErlingerTPThe effect of weight loss on C-reactive protein: a systematic reviewArch Intern Med2007167313917210875
- PopeCAIIIParticulate air pollution, C-reactive protein, and cardiac riskEur Heart J2001221149115011440485
- NicklasBJYouTPahorMBehavioural treatments for chronic systemic inflammation: effects of dietary weight loss and exercise trainingCMAJ20051721199120915851714
- GentileMPanicoSRubbaFObesity, overweight, and weight gain over adult life are main determinants of elevated hs- CRP in a cohort of Mediterranean womenEur J Clin Nutr20106487387820517327
- HamerMSteptoeAProspective study of physical fitness, adiposity, and inflammatory markers in healthy middle-aged men and womenAm J Clin Nutr200989858919056563
- WelshPPoliseckiERobertsonMUnraveling the directional link between adiposity and inflammation: a bidirectional Mendelian randomization approachJ Clin Endocrinol Metab201095939919906786
- HubelCAPowersRWSnaedalSC-reactive protein is elevated 30 years after eclamptic pregnancyHypertension2008511499150518413489
- LauBSharrettSRKingsleyLAC-reactive protein is a marker for human immunodeficiency virus disease progressionArch Intern Med2006166647016401812
- SurteesPGWainwrightNWJBoekholdtSMLubenRNWarehamNJKhawKTMajor depression, C-reactive protein, and incident ischemic heart disease in healthy men and womenPsychosom Med20087085085518725428
- RidkerPMHigh-sensitivity C-reactive protein: potential adjunct for global risk assessment in the primary prevention of cardiovascular diseaseCirculation20011031813181811282915
- PankowJSFolsomARCushmanMFamilial and genetic determinants of systemic markers of inflammation: the NHLBI family heart studyAtherosclerosis200115468168911257270
- LeeCCYouNCSongYRelation of genetic variation in the gene coding for C-reactive protein with its plasma protein concentrations: findings from the Women’s Health Initiative Observational CohortClin Chem200955235136019095725
- Kelley-HedgepethALloyd-JonesDMColvinAEthnic differences in C-reactive protein concentrationsClin Chem2008541027103718403563
- SmithGDEbrahimSMendelian randomization: can genetic epidemiology contribute to understanding environmental determinants of diseaseInt J Epidemiol20033212212689998
- ZachoJTybjaerg-HansenAJensenJSGrandePSillesenHNordestgaardBGGenetically elevated C-reactive protein and ischemic vascular diseaseN Engl J Med20083591897190818971492
- SmithDGCapitalizing on Mendelian randomization to assess the effects of treatmentsJ R Soc Med200710043243517766918
- SheehanNADidelezVBurtonPRTobinMDMendelian randomisation and causal inference in observational epidemiologyPLoS Med20085e17718752343
- ElliottPChambersJCZhangWGenetic loci associated with C-reactive protein levels and risk of coronary heart diseaseJAMA2009302374819567438
- SmithGDEbrahimSMendelian randomization: prospects, potentials, and limitationsInt J Epidemiol200433304215075143
- EmergingRiskFactorsCollaborationKaptogeSDi AngelantonioELoweGC-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysisLancet201037513214020031199
- DaneshJKaptogeSMannAGLong-term interleukin-6 levels and subsequent risk of coronary heart disease: two new prospective studies and a systematic reviewPLoS Med20085e7818399716
- ClarkeREmbersonJRBreezeEBiomarkers of inflammation predict both vascular and non-vascular mortality in older menEur Heart200829800809
- HeikkilaKHarrisRLoweGAssociations of circulating C-reactive protein and interleukin-6 with cancer risk: findings from two prospective cohorts and a meta-analysisCancer Causes Control200920152618704713
- HabersbergerJEisenhardtSPeterKC-reactive protein measurement and cardiovascular disease. Original TextLancet20109720107820346805
- JiSRWuYZhuLCell membranes and liposomes dissociate C-reactive protein (CRP) to form a new, biologically active structural intermediate: mCRP(m)FASEB J20072128429417116742
- MolinsBPenaEVilahurGMendietaCSlevinMBadimonLC-reactive protein isoforms differ in their effects on thrombus growthArterioscler Thromb Vasc Biol2008282239224618787187
- EisenhardtSUHabersbergerJMurphyADissociation of pentameric to monomeric C-reactive protein on activated platelets localizes inflammation to atherosclerotic plaquesCirc Res200910512813719520972
- JiSRMaLBaiCJMonomeric C-reactive protein activates endothelial cells via interaction with lipid raft microdomainsFASEB J2009231806181619136614
- RidkerPMRifaiNClearfieldMMeasurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary eventsN Engl J Med20013441959196511430324
- TuzcuEMKapadiaSRTutarEHigh prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasoundCirculation20011032705271011390341
- RidkerPMCannonCPMorrowDAtorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT – TIMI 22) InvestigatorsC-reactive protein levels and outcomes after statin therapyN Engl J Med2005352202815635109
- De BeerFCHindCRFoxKMMeasurement of serum C-reactive protein concentration in myocardial ischaemia and infarctionBr Heart J1982472392437059401
- HaverkateFThompsonSGPykeSDProduction of C-reactive protein and risk of coronary events in stable and unstable angina. European Concerted Action on Thrombosis and Disabilities Angina Pectoris Study GroupLancet19973494624669040576
- NiccoliGBiasucciLMBiscioneCIndependent prognostic value of C-reactive protein and coronary artery disease extent in patients affected by unstable anginaAtherosclerosis200819677978517306806
- RidkerPMCushmanMStampferMJPlasma concentration of C-reactive protein and risk of developing peripheral vascular diseaseCirculation1998974254289490235
- NissenSETuzcuEMSchoenhagenPStatin therapy, LDL cholesterol, C-reactive protein, and coronary artery diseaseN Engl J Med2005352293815635110
- HemingwayHPhilipsonPChenRFitzpatrickNKDamantJEvaluating the quality of research into a single prognostic biomarker: a systematic review and meta-analysis of 83 studies of C-reactive protein in stable coronary artery diseasePLoS Med20107e100028620532236
- BoekholdtSMHackCESandhuMSC-reactive protein levels and coronary artery disease incidence and mortality in apparently healthy men and women: the EPIC-Norfolk prospective population study 1993–2003Atherosclerosis200618741542216257408
- CookNRBuringJERidkerPMThe effect of including C-reactive protein in cardiovascular risk prediction models for womenAnn Intern Med2006145212916818925
- GenestJMcPhersonRFrohlichJ2009Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult – 2009 recommendationsCan J Cardiol20092556757919812802
- AlbertMAGlynnRJRidkerPMPlasma concentration of C-reactive protein and the calculated Framingham Coronary Heart Disease Risk ScoreCirculation200310816116512835213
- RidkerPMRifaiNCookNRBradwinGBuringJENon-HDL cholesterol, apolipoproteins A-I and B100, standard lipid measures, lipid ratios, and CRP as risk factors for cardiovascular disease in womenJAMA200529432633316030277
- ShahTCasasJPCooperJACritical appraisal of CRP measurement for the prediction of coronary heart disease events: new data and systematic review of 31 prospective cohortsInt J Epidemiol20093821723118930961
- WaldDSKasturiratneABestwickJPThe value of C-reactive protein in screening for future coronary heart disease eventsJ Med Screen20091621221420054097
- LakoskiSGGreenlandPWongNDSchreinerPJCoronary artery calcium scores and risk for cardiovascular events in women classified as “low risk” based on Framingham risk score: the Multi- Ethnic Study of Atherosclerosis (MESA)Arch Intern Med20071672437244218071165
- RidkerPMBuringJERifaiNCookNRDevelopment and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk ScoreJAMA200729761161917299196
- WilsonPWPencinaMJacquesPSelhubJD’AgostinoRSrO’DonnellCJC-reactive protein and reclassification of cardiovascular risk in the Framingham Heart StudyCirc Cardiovasc Qual Outcomes20081929720031795
- RidkerPMPaynterNPRifaiNGazianoJMCookNRC-reactive protein and parental history improve global cardiovascular risk prediction: the Reynolds Risk Score for MenCirculation20081182243225118997194
- CookNRThe case for C-reactive protein as a risk marker for coronary heart diseaseAnn Intern Med201015240620231582
- CookNRRidkerPMAdvances in measuring the effect of individual predictors of cardiovascular risk: the role of reclassification measuresAnn Intern Med20095079580219487714
- RidkerPMMacFadyenJLibbyPGlynnRJRelation of baseline high-sensitivity C-reactive protein level to cardiovascular outcomes with rosuvastatin in the Justification for Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER)Am J Cardiol201010620420920599004
- SlejkoJFPageRLIISullivanPWImplications of Jupiter prevention in adults with elevated C-reactive protein: statin therapy is cost-effective for vascular eventJ Am Coll Cardiol201055A131.E1229
- RaoADMilbrandtEBTo JUPITER and beyond: statins, inflammation, and primary preventionCritical Care20101431020497597
- MacDonaldGPCost-effectiveness of rosuvastatin for primary prevention of cardiovascular events according to Framingham Risk Score in patients with elevated C-reactive proteinJ Am Osteopath Assoc201011042743620805548
- DaneshJCollinsRApplebyPPetoRAssociation of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective studiesJAMA1998279147714829600484
- DaneshJWhincupPWalkerMLow grade inflammation and coronary heart disease: prospective study and updated meta-analysesBMJ200032119920410903648
- NambiVBallantyneCMUtility of statin therapy using high- sensitivity C-reactive protein as an indicator of coronary heart disease riskCurr Atheroscler Rep20057222815683598
- RidkerPMHigh-sensitivity C-reactive protein and cardiovascular risk: rationale for screening and primary preventionAm J Cardiol20039217K22K
- RocheVFAntihyperlipidemic statins: a self-contained, clinically relevant medicinal chemistry lessonAm J Pharm Educ200569546560
- IstvanESDeisenhoferJStructural mechanism for statin inhibition of HMG-CoA reductaseScience20012921160116411349148
- HamelinBATurgeonJHydrophilicity/lipophilicity: relevance for the pharmacology and clinical effects of HMG-CoA reductase inhibitorsTrends Pharmacol Sci19981926379509899
- McTaggartFComparative pharmacology of rosuvastatinAtheroscler Suppl2003491412714032
- KapurNKRosuvastatin: a highly potent statin for the prevention and management of coronary artery diseaseExpert Rev Cardiovasc Ther2007516117517338662
- HoltzmanCWWigginsBSSpinlerSARole of P-glycoprotein in statin drug interactionsPharmacotherapy2006261601160717064205
- KostapanosMSHaralamposJElisafMSRosuvastatin-associated adverse effects and drug-drug interactions in the clinical setting of dyslipidemiaAm J Cardiovasc Drugs201010112820104931
- BaigentCKeechAKearneyPMCholesterol Treatment Trialists’ (CTT) CollaboratorsEfficacy and safety of cholesterollowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomized trials of statinsLancet20053661267127816214597
- McKenneyJMPharmacologic options for aggressive low-density lipoprotein cholesterol lowering: benefits versus risksAm J Cardiol20059660E66E
- The Galaxy Program http://www.galaxyprogramme.org/about-galaxy/?itemId=2592383Accessed 2010 Oct 18
- CrouseJRIIIRaichlenJSRileyWAMETEOR study groupEffect of rosuvastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosisJAMA20072971344135317384434
- CrouseJRIIIBotsMLEvansGWDoes baseline carotid intima-media thickness modify the effect of rosuvastatin when compared with placebo on carotid intima-media thickness progression? The METEOR studyEur J Cardiovasc Prev Rehabil20101722322920038840
- KjekshusJApetreiEBarriosVRosuvastatin in older patients with systolic heart failureN Engl J Med20073572248226117984166
- McMurrayJJVKjekshusJGullestadLCORONA Study GroupEffects of statin therapy according to plasma high-sensitivity C-reactive protein concentration in the Controlled Rosuvastatin Multinational trial in Heart Failure (CORONA). A retrospective analysisCirculation20091202188219619917888
- Gissi-HFInvestigatorsTavazziLMaggioniAPMarchioliREffect of rosuvastatin in patients with chronic heart failure (the GISSI-HF trial): a randomised, double-blind, placebo-controlled trialLancet20083721231123918757089
- Van der HarstPde BoerRAStatins in the treatment of heart failureCirc Heart Fail2010346246420484198
- FellströmBCJardineAGSchmiederRERosuvastatin and cardiovascular events in patients undergoing hemodialysisN Eng J Med200937311751182
- NarlaVBlahaMJBlumenthalRSMichosEDThe JUPITER and AURORA clinical trials for rosuvastatin in special primary prevention populations: perspectives, outcomes, and consequencesVasc Health Risk Manag200951033104220057896
- NissenSENichollsSJSipahiIEffect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trialJAMA20062951556156516533939
- BallantyneCMRaichlenJSNichollsSASTEROID InvestigatorsEffect of rosuvastatin therapy on coronary artery stenoses assessed by quantitative coronary angiography: a study to evaluate the effect of rosuvastatin on intravascular ultrasound-derived coronary atheroma burdenCirculation20081172458246618378607
- MackWJXiangMSelzerRHHodisHNSerial quantitative coronary angiography and coronary eventsAm Heart J200013999399910827379
- BuchwaldHMattsJPFitchLLProgram on the Surgical Control of the Hyperlipidemias (POSCH) GroupChanges in sequential coronary arteriograms and subsequent coronary eventsJAMA1992268142914331512911
- FonsecaFAHIzarMCOPrimary prevention of vascular events in patients with high levels of C-reactive protein: the JUPITER StudyExpert Rev Cardiovasc Ther200971041105619764857
- LibbyPRidkerPMNovel inflammatory markers of coronary risk: theory versus practiceCirculation19991001148115010484532
- LemieuxIPascotAPrud’hommeDAlmerasNElevated C-reactive protein: another component of the atherothrombotic profile of abdominal obesityArterioscler Thromb Vasc Biol20012196196711397704
- RidkerPMRifaiNPfefferMAInflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events (CARE) InvestigatorsCirculation1998988398449738637
- RidkerPMJUPITER Study GroupRosuvastatin in the primary prevention of cardiovascular disease among patients with low levels of low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein: rationale and design of the JUPITER trialCirculation20031082292229714609996
- RidkerPMFonsecaFAHGenestJJUPITER Trial Study GroupBaseline characteristics of participants in the JUPITER Trial, a randomized placebo-controlled primary prevention trial of statin therapy among individuals with low low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive proteinAm J Cardiol20071001659166418036365
- De LorgerilMSalenPMartinJLMonjaudIDelayeJMamelleNMediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction – final report of the Lyon Diet Heart StudyCirculation1999997797859989963
- RemboldCMTo statin or to non-statin in coronary disease – considering absolute risk is the answerAtherosclerosis20071951617064710
- EverettBMRidkerPMUsing inflammatory biomarkers to guide lipid therapyCurr Cardiovasc Risk Reports200822934
- KritekPCampionEWJUPITER Clinical Directions – polling resultsN Eng J Med2009360e14
- SpatzESCanavanMEDesaiMMFrom here to JUPITER. Identifying new patients for statin therapy using data from the 1999–2004 National Health and Nutrition Examination SurveyCirc Qual Outcomes200924148
- MichosEDBlumenthalRSPrevalence of the JUPITER (Justification for the Use of Statins in Primary Prevention: an Intervention Trial Evaluating Rosuvastatin) StudyJ Am Coll Cardiol20095393193519281922
- RidkerPMThe JUPITER trial. Results, controversies, and implications for preventionCirc Cardiovasc Qual Outcomes2009227928520031849
- RidkerPMMacFadyenJGFonsecaFAHJUPITER Study GroupNumber needed to treat with rosuvastatin to prevent first cardiovascular events and death among men and women with low low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein. Justification for the Use of statins in Prevention: an Intervention Trial Evaluation Rosuvastatin (JUPITER)Circ Cardiovasc Qual Outcomes2009261662320031900
- YangEYNambiVTangZClinical implications of JUPITER (Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin) in a US population: insights from the ARIC (Atherosclerosis Risk in Communities) studyJ Am Coll Cardiol2009542388239520082929
- VaccarinoVBremmerJDKelleyMEJUPITER. A few words of cautionCirc Cardiovasc Qual Outcomes2009228628820031850
- KonesRRecent advances in the management of chronic stable angina. II. Anti-ischemic therapy, options for refractory angina, risk factor reduction, and revascularizationVasc Health Risk Manag2010674977420859545
- EyreHKahnRRobertsonRMPreventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart AssociationDiabetes Care2004271812182415220271
- LeviJSegalLMJulianoCPrevention for a healthier America: investments in disease prevention yield significant savings, stronger communities: Trust for America’s Health Issue Report 2008 Jul. http://healthyamericans.org/reports/prevention08/Accessed 2010 Sep 1
- Heart Protection Study Collaborative GroupStatin cost-effectiveness in the United States for people at different vascular risk levelsCirc Cardiovasc Qual Outcomes20092657220031817
- AccadMFredHLIs JUPITER also a God of primary preventionTex Heart Inst J2010376720200621
- KappagodaCTAmsterdamEAAnother look at the results of the JUPITER trialAm J Cardiol20091041603160519932800
- RidkerPMDanielsonEFonsecaFAReduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trialLancet20093731175118219329177
- DespresJPBringing JUPITER down to EarthLancet20093731147114819329179
- KostapanosMSMilionisHJElisafMSAn overview of the extra-lipid effects of rosuvastatinJ Cardiovasc Pharmacol Ther20081315717418460672
- KendrickMShould women be offered cholesterol lowering drugs to prevent cardiovascular disease? NoBMJ200733498317494018
- EisenbergTWellsMStatins and adverse cardiovascular events in moderate-risk females: a statistical and legal analysis with implications for FDA preemption claimsJ Empir Leg Stud20085507550
- RosenbergHAllardDWomen and statin use: a women’s health advocacy perspectiveScand Cardiovasc J20084226827318609063
- MoraSGlynnRJHsiaJMacFadyenJGGenestJRidkerPMStatins for the primary prevention of cardiovascular events in women with elevated high-sensitivity C-reactive protein or dyslipidemia: results from the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) and meta-analysis of women from primary prevention trialsCirculation20101211069107720176986
- DuvernoyCSBlumenthalRThe numbers are in: statins for the primary prevention of cardiovascular disease in womenCirculation20101211063106520176993
- Highlights of prescribing information: Crestor (rosuvastatin calcium) tablets http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021366s016lbl.pdfAccessed 2010 Apr 16
- KaulSMorrisseyRPDiamondGABy Jove! What is a clinician to make of JUPITERArch Int Med20101701073107720585074
- Jupiter criticism addressed again in more detail2010101 http://www.theheart.org/article/1130113.doAccessed 2010 Oct 15
- BasslerDBrielMMontoriVMSTOPIT-2 Study GroupStopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysisJAMA20103031180118720332404
- MontoriVMDevereauxPJAdhikariNKJRandomized trials stopped early for benefit: a systematic reviewJAMA20052942203220916264162
- PocockSJCurrent controversies in data monitoring for clinical trialsClin Trials2006351352117170035
- McCatneyMLeaping to conclusionsBMJ20083361213121418511794
- Department of Health and Human Services, United States Food and Drug Administration, Center for Drug Evaluation and ResearchTranscript for the 2009 Dec 15, Meeting of the Endocrinologic and Metabolic Drugs Advisory Committee http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM200611.pdfAccessed 2010 Oct 7
- De LorgerilMSalenPAbramsonJCholesterol lowering, cardiovascular diseases, and the rosuvastatin-JUPITER controversy: a critical reappraisalArch Intern Med20101701032103620585068
- De LorgerilMAnswers to R. Ridker by M. de Lorgeril2010630 http://michel.delorgeril.info/dwnl/JUPITER/2010_Answers-to-Ridker-by-de-Lorgeril.pdfAccessed 2010 Aug 15
- GlynnRJDanielsonEFonsecaFAHA randomized trial of rosuvastatin in the prevention of venous thromboembolismN Engl J Med20093601851186119329822
- RidkerPMMacfadyenJCressmanMGlynnRJEfficacy of rosuvastatin among men and women with moderate chronic kidney disease and elevated high-sensitivity C-reactive protein: a secondary analysis from the JUPITER (Justification for the Use of Statins in Prevention – an Intervention Trial Evaluating Rosuvastatin) trialJ Am Coll Cardiol2010551266127320206456
- GlynnRJKoenigWNordestgaardBGShepherdJRidkerPMRosuvastatin for primary prevention in older persons with elevated C-reactive protein and low to average low-density lipoprotein cholesterol levels: exploratory analysis of a randomized trialAnn Intern Med2010152488496W17420404379
- PearsonTAMensahGAAlexanderRWMarkers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart AssociationCirculation200310749951112551878
- RidkerPMMacFadyenJGBørgeGNordestgaardBGRosuvastatin for primary prevention among individuals with elevated high-sensitivity C-reactive protein and 5% to 10% and 10% to 20% 10-year risk: implications of the Justification for Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) Trial for “Intermediate Risk”Circ Cardiovasc Qual Outcomes2010344745220736443
- KonesRRecent advances in the management of chronic stable angina I: approach to the patient, diagnosis, pathophysiology, risk stratification, and gender disparitiesVasc Health Risk Manag2010663565620730020
- RidkerPMGlynnRJThe JUPITER Trial: Responding to the criticsAm J Cardiol20101061351135621029837
- HarringtonRRidkerPMThe Bob Harrington ShowEpisode #26: Dissecting the controversy around JUPITER with Dr Paul Ridker http://radio.theheart.org/bob-harrington-show/2010/8/20/episode-26-dissecting-the-controversy-around-jupiter-with-dr-paul-ridker2010827
- http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/EndocrinologicandMetabolicDrugsAdvisoryCommittee/UCM193831.pdf. (FDA memorandum, 2009 Nov 12, Appendix, page 11)Accessed 2010 Oct 7
- FriedlinBKornEStopping clinical trials early for benefit: impact on estimationClin Trials2009611912519342463
- KornELFriedlinBMooneyMStopping or reporting early for positive results in randomized clinical trials: the National Cancer Institute Cooperative Experience from 1990 to 2005J Clin Oncol2009271712172119237631
- BruckertEHayemGDejagerSMild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients: the PRIMO studyCardiovasc Drugs Ther20051940341416453090
- HsuISpinlerSAJohnsonNEComparative evaluation of the safety and efficacy of HMG-CoA reductase inhibitor monotherapy in the treatment of primary hypercholesterolemiaAnn Pharmacother1995297437598520093
- Garcia-RodriguezLAMasso-GonzalezELWallanderMAJohanssonSThe safety of rosuvastatin in comparison with other statins in over 100,000 statin users in UK primary carePharmacoepidemiol Drug Saf20081794395218425988
- Garcia-RodriguezLAGonzalez-PerezAStangMRThe safety of rosuvastatin in comparison with other statins in over 25,000 statin users in the Saskatchewan Health DatabasesPharmacoepidemiol Drug Saf20081795396118425987
- SukhijaRPrayagaSMarashdehMEffect of statins on fasting plasma glucose in diabetic and nondiabetic patientsJ Investig Med200957495499
- KohKKQuonMJHanSHLeeYKimSJShinEKAtorvastatin causes insulin resistance and increases ambient glycemia in hypercholesterolemic patientsJ Am Coll Cardiol2010551209121620298928
- KostapanosMSMilionisHJAgouridisADRizosCVElisafMSRosuvastatin treatment is associated with an increase in insulin resistance in hyperlipidaemic patients with impaired fasting glucoseInt J Clin Pract2009631308131319691613
- Cholesterol Treatment Trialists’ (CTT) CollaboratorsEfficacy of cholesterol-lowering therapy in 18,696 people with diabetes in 14 randomised trials of statins: a meta-analysisLancet200837111712518191683
- SattarNPreissDMurrayHMStatins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trialsLancet201037573574220167359
- BakerWLTalatiRWhiteCMColemanCIDiffering effect of statins on insulin sensitivity in non-diabetics: a systematic review and meta-analysisDiab Res Clin Pract20108798107
- ZhangFLCaseyPJProtein prenylation: molecular mechanisms and functional consequencesAnnu Rev Biochem1996652412698811180
- TakaiYSasakiTMatozakiTSmall GTP-binding proteinsPhysiol Rev20018115320811152757
- GreenwoodJSteinmanLZamvilSSStatin therapy and autoimmune disease: from protein prenylation to immunomodulationNature Rev Immunol2006635837016639429
- ChakrabartiREnglemanEGInterrelationships between mevalonate metabolism and the mitogenic signaling pathway in T lymphocyte proliferationJ Biol Chem199126612216122221712015
- GrahamIAtarDBorch-JohnsenKFourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by representatives of nine societies and by invited experts). European guidelines on cardiovascular disease prevention in clinical practice: executive summaryEur Heart J2007282375241417726041
- LiuPYChenJHLinLJLiaoJKIncreased Rho kinase activity in a Taiwanese population with metabolic syndromeJ Am Coll Cardiol2007491619162417433952
- LiaoJKDoes it matter whether or not a lipid-lowering agent inhibits Rho kinaseCurr Atheroscler Rep2007938438818001621
- DongMYanBPLiaoJKLamYYYipGWKYuCMRho-kinase inhibition: a novel therapeutic target for the treatment of cardiovascular diseasesDrug Discov Today20101562262920601092
- BrozinickJTJrBerkemeierBAElmendorfJS“Acting” on GLUT 4: membrane and cytoskeletal components of insulin actionCurr Diabetes Rev2007311112218220662
- HorvathEMTackettLElmendorfJSA novel membrane-based anti-diabetic action of atorvastatinBiochem Biophys Res Commun200837263964318514061
- NakataMNagasakaSKusakaIMatsuokaHIshibashiSYadaTEffects of statins on the adipocyte maturation and expression of glucose transporter 4 (SLC2A4): implications in glycemic controlDiabetologia2006491881189216685502
- WhiteCMA review of the pharmacologic and pharmacokinetic aspects of rosuvastatinJ Clin Pharmacol20024296397012211221
- MitaTWatadaHNakayamaSPreferable effect of pravastatin compared to atorvastatin on beta cell function in Japanese early-state type 2 diabetes with hypercholesterolemiaEndocr J20075444144717457013
- YadaTNakataMShiraishiTKakeiMInhibition by simvastatin, but not pravastatin, of glucose-induced cytosolic Ca2+ signaling and insulin secretion due to blockade of L-type Ca2+ channels in rat islet b-cellsBr J Pharmacol19991261205121310205010
- SiddalsKWMarshmanEWestwoodMGibsonJMAbrogation of insulin-like growth factor-I (IGF-I) and insulin action by mevalonic acid depletion: synergy between protein prenylation and receptor glycosylation pathwaysJ Biol Chem2004279383533835915247258
- OtokozawaSAiMvan HimbergenTEffects of intensive atorvastatin and rosuvastatin treatment on apolipoprotein B-48 and remnant lipoprotein cholesterol levelsAtherosclerosis200920519720119200542
- American Diabetes AssociationStandards of Medical Care in Diabetes – 2009Diabetes Care200932Suppl 1S136119118286
- PasternakRCSmithSCBairey-MerzCNGrundySMCleemanJILenfantCACC/AHA/NHLBI clinical advisory on the use and safety of statinsStroke2002332337234112215610
- ThompsonPDClarksonPKarasRHStatin-associated myopathyJAMA20032891681169012672737
- TomlinsonSSMangioneKKPotential adverse effects of statins on musclePhys Ther20058545946515842193
- SEARCH Collaborative GroupLinkEParishSArmitageJSLCO1B1 variants and statin-induced myopathy – a genomewide studyN Eng J Med2008359789799
- GomesMDLeckerSHJagoeRTNavonAGoldbergALAtrogin-1, a muscle-specific F-box protein highly expressed during muscle atrophyProc Natl Acad Sci U S A200198144401444511717410
- HanaiJCaoPTanksalePThe muscle-specific ubiquitin ligase atrogin-1/MAFbx mediates statin-induced muscle toxicityJ Clin Invest20071173940395117992259
- CaoPHanaiJ-iTanksalePImamuraSSukhatmeVPLeckerSHStatin-induced muscle damage and atrogin-1 induction is the result of a geranylgeranylation defectFASEB J2009232844285419406843
- KnauerMJUrquhartBLMeyerzu SchwabedissenHEHuman skeletal muscle drug transporters determine local exposure and toxicity of statinsCirc Res201010629730619940267
- DorajooRPereiraBPYuZRole of multidrug resistance-associated protein-1 transporter in statin-induced myopathyLife Sci20088282383018509883
- MastersBAPalmoskiMJGlintOPGreggREWang-IversonDDurhamSKIn vitro myotoxicity of the 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors, pravastatin, lovastatin, and simvastatin, using neonatal rat skeletal myocytesToxicol Appl Pharmacol19951311631747878672
- Thalacker-MercerABakerMCalderonCBammanMSimvastatin Reduces Human Primary Satellite Cell Proliferation in CulturePresentation, American Physiological Society, The Integrative Biology of Exercise V2008 Sep 24–27Hilton Head, SC. http://www.the-aps.org/press/journal/08/32.htmand http://www.the-aps.org/Video/Clips/AnnaThalacker-Mercer.htmAccessed 2010 Nov 20
- MarcoffLThompsonPDThe role of coenzyme Q10 in statinassociated myopathy: a systematic reviewJ Am Coll Cardiol2007492231223717560286
- DirksAJJonesKMStatin-induced apoptosis and skeletal myopathyAm J Physiol Cell Physiol2006291C1208121216885396
- SirventPMercierJLacampagneANew insights into mechanisms of statin-associated myotoxicityCurr Opin Pharmacol2008833333818243052
- NeedhamMFabianVKnezevicWProgressive myopathy with upregulation of MHC-I associated with statin therapyNeuromuscul Disord20071719420017241784
- Grable-EspositoPKatzbergHDGreenbergSAImmune-mediated necrotizing myopathy associated with statinsMuscle Nerve20104118519019813188
- VaklavasCChatzizisisYSZiakasAZamboulisCGiannoglouGDMolecular basis of statin-associated myopathyAtherosclerosis2009202182818585718
- MasEMoriTACoenzyme Q10 and statin myalgia: what is the evidenceCurr Atheroscler Rep20101240741320725809
- VandenbergBFRobinsonJManagement of the patient with statin intoleranceCurr Atheroscler Rep201012485720425271
- MammenALAmatoAAStatin myopathy: a review of recent progressCurr Opin Rheumatol20102264465020827205
- ThompsonPDClarksonPMRosensonRSAn assessment of statin safety by muscle expertsAm J Cardiol20069769C76C
- ArmitageJThe safety of statins in clinical practiceLancet20073701781179017559928
- FordESLiCZhaoGTsaiJTrends in obesity and abdominal obesity among adults in the United States from 1999–2008Int J Obes (Lond)201097 [Epub ahead of print]
- FilionKBGenestJJosephLThe metabolic syndrome and cardiovascular risk: a systematic review and meta-analysisJ Am Coll Cardiol2010561113113220863953
- DeMazumderDHasanRKBlumenthalRSMichosEDJonesSShould statin therapy be allocated on the basis of global risk or on the basis of randomized trial evidenceAm J Cardiol201010690590920816135
- NambiVBallantyneCM“Risky Business”: ten years is not a lifetimeCirculation200911936236419171864
- Lloyd-JonesDMHongYLabartheDAmerican Heart Association Strategic Planning Task Force and Statistics CommitteeDefining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association’s strategic Impact Goal through 2020 and beyondCirculation201012158661320089546
- WebsterRHeeleyEPerceptions of risk: understanding cardiovascular diseaseRisk Management and Healthcare Policy201034960