
Abstract
Purpose
Since electroporation (EP) can increase the permeability of biological membranes, we hypothesized that it offers an opportunity to enhance the transdermal delivery of drugs for intra-articular indications. Our aim was to compare the anti-inflammatory and analgesic efficacy of EP-combined topical administration of diclofenac sodium hydrogel (50 mg mL−1 in 230 µL volume) with that of an equivalent dose of oral (75 mg kg−1) and simple topical administration.
Methods
Arthritis was induced with the injection of 2% λ-carrageenan and 4% kaolin into the right knee joints of male Sprague Dawley rats. EP was applied for 8 min with 900 V high-voltage pulses for 5 ms followed by a 20 ms break. Drug penetration into the synovial fluid and plasma was detected by high-performance liquid chromatography. Leukocyte–endothelial interactions were visualized by intravital videomicroscopy on the internal surface of the synovium. Inflammation-induced thermal and mechanical hyperalgesia reactions, knee joint edema, and inflammatory enzyme activities were assessed at 24 and 48 h after arthritis induction.
Results
EP significantly increased the plasma level of diclofenac as compared with the topical controls 10 min after the 2% λ-carrageenan and 4% kaolin injection. Increased leukocyte–endothelial interactions were accompanied by joint inflammation, which was significantly reduced by oral and EP diclofenac (by 45% and by 30%, respectively) and only slightly ameliorated by simple topical diclofenac treatment (by 18%). The arthritis-related secondary hyperalgesic reactions were significantly ameliorated by oral and EP-enhanced topical diclofenac treatments. The knee cross-section area (which increased by 35%) was also reduced with both approaches. However, simple topical application did not influence the development of joint edema and secondary hyperalgesia.
Conclusion
The study provides evidence for the first time of the potent anti-inflammatory and analgesic effects of EP-enhanced topical diclofenac during arthritis. The therapeutic benefit provided by EP is comparable with that of oral diclofenac; EP is a useful alternative to conventional routes of administration.
Introduction
Arthritis is a collective term encompassing many diseases with distinct etiologies but common symptoms, such as joint pain and inflammation. Owing to its high incidence, it is of significant public health and economic importance, yet therapeutic options are limited to pain relief and reduction of inflammation.Citation1,Citation2 Today, the “gold standard” therapy for alleviating arthritis-related pain is diclofenac, a nonsteroidal anti-inflammatory drug (NSAID) of the phenylacetic acid class.Citation3,Citation4
Table S1 Parameters of the chromatographic measurement
Table S2 Comparison of the parameters of the long and short methods
Unfortunately, the side effects of such an effective compound are also significant. Diclofenac usages are associated with the NSAID category risk of dose-related gastrointestinal, cardiovascular, and renal adverse effects; topical preparations were thus developed to limit the potentially serious complications of systemic treatments. Diclofenac is a lipophilic organic acid, but formulations with salts are water-soluble, and this property renders the compound capable of penetrating the skin and the synovial lining of diarthrodial joints. The systemic absorption of topically administered diclofenac is 3%–5% of that of oral products, and the dosage reaches the site of action ten times later as compared with that of an equivalent oral dose.Citation5,Citation6 On the whole, since passive transdermal passage after topical administrations is rather slow and therapeutic drug levels cannot always be reached, new delivery methods are needed to achieve locally effective drug concentrations directly at the application site.Citation7
Various skin penetration techniques have been developed to improve transdermal drug delivery and bioavailability, including ultrasound and electroporation (EP).Citation8–Citation14 With EP, applications of short, high-voltage pulses cause transitory structural perturbations in the lipid bilayer of the membranes. Lipophilic or hydrophilic molecules, neutral or highly charged compounds, can thus be transported through or into membranes of bacteria or mammalian cells, if they are up to 40 kDa in molecular weight.Citation15 Common fields of indication for EP are biological and artificial membranes, but complex structures such as the stratum corneum or the synovium can also be targeted.Citation16,Citation17
Based on this background, we hypothesized that EP can amplify the transport of topical diclofenac into the joints, and thus the effectiveness of local administration increases. The aims were to compare the penetration properties of diclofenac hydrogel into the synovial fluid after different administration routes and to estimate the analgesic and anti-inflammatory reactions after oral and topical drug deliveries in a standardized rat model of carrageenan/kaolin (C/K)-induced knee joint monoarthritis.
Materials and methods
The experiments were performed on male Sprague Dawley rats (average weight 300±50 g). The animals were housed in plastic cages in a thermoneutral environment and provided standard laboratory chow and water ad libitum. The experimental protocol complied with EU Directive 2010/63 for the Protection of Animals Used for Scientific Purposes and was approved by Hungary’s National Scientific Ethical Committee on Animal Experimentation (National Competent Authority) under license number V./148/2013. This study also satisfied the criteria in the US National Institutes of Health Guidelines for the Care and Use of Laboratory Animals.
Arthritis induction
For arthritis induction, the animals were anesthetized with intraperitoneal (IP) ketamine (50 mg kg−1) and xylazine (12 mg kg−1), and the skin over the knees was disinfected with povidone iodide. Then a single intra-articular injection of a 75 µL mixture of 2% λ-carrageenan (Sigma-Aldrich, St Louis, MO, USA) and 4% kaolin in saline was administered to the right knee joint.Citation18,Citation19 The contralateral knee was injected with saline.
Experimental protocols
The goal of the first experimental series was to assess the serum and the synovial concentrations of diclofenac by high-performance liquid chromatography (HPLC). The animals were anesthetized with IP sodium pentobarbital (45 mg kg−1) and placed in a supine position on a heating pad to maintain body temperature between 36°C and 37°C. In the first group (n=16), diclofenac sodium gel (50 mg mL−1 in 230 µL volume) was applied topically above the knee joint. In the second group (n=16), after dispersion of the diclofenac gel over the knee joint, EP was applied for 8 min. Samples of blood from the inferior vena cava and of synovial washing fluid from the knee joint were collected at 10, 30, 60, and 120 min of the experiment. The samples were frozen at −80°C until the HPLC measurement. At the end of the last sampling point, the animals were sacrificed with a single overdose of anesthetic ().
Figure 1 Time sequence of interventions.
Abbreviations: C/K, carrageenan/kaolin; D, diclofenac treatment; HPLC, high-performance liquid chromatography; IVM, intravital videomicroscopy; S, sample taken.
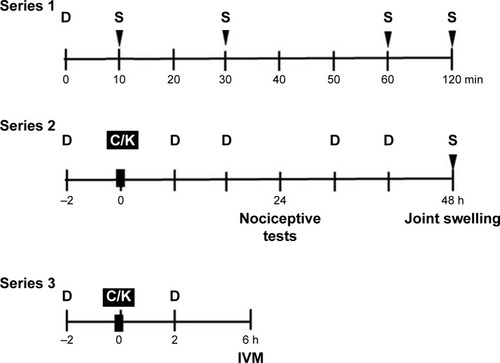
In the second series of experiments, inflammation-related changes to the synovial microcirculation were evaluated directly by intravital videomicroscopy (IVM). The animals were anesthetized with IP sodium pentobarbital (45 mg kg−1) and divided into four groups according to the administration route of diclofenac: The animals were treated with per os diclofenac (75 mg kg−1 diclofenac sodium, Novartis Hungaria Kft., Budapest, Hungary) in Group 1 (n=6), with topical diclofenac gel (50 mg mL−1 in 230 µL volume; n=6) in Group 2, and with EP-combined topical diclofenac gel (50 mg mL−1 in 230 µL volume; n=6) in Group 3. Group 4 served as a per os saline-treated control (n=6). The treatments were always applied 2 h before (t= −2 h) and 2 h after (t=2 h) the arthritis induction ().
In the third experimental series, the effectiveness of different routes of diclofenac treatment on nociception and inflammatory edema formation was compared in C/K-induced arthritis. The animals were divided into four groups (n=6) according to the administration route of diclofenac: 1) per os diclofenac sodium, 2) topical diclofenac gel, 3) EP-enhanced topical diclofenac gel, and 4) sham (per os saline-treated). Treatments were applied twice daily (every 12 h). The nociceptive tests were performed 24 h after the C/K injection, while knee joint swelling was evaluated at the peak of edema formation 48 h after arthritis induction. At the end of the experiments, the animals were anesthetized with IP sodium pentobarbital (45 mg kg−1) for sample taking and thereafter sacrificed with a single overdose of anesthetic. Synovial washing fluid samples and synovium tissue specimens were collected for biochemical measurements and histology. Tissue biopsies were stored at −20°C until the examinations ().
Diclofenac-containing hydrogel formulation
The hydrogel was prepared using the following procedure. Five w/w% diclofenac sodium (Sigma-Aldrich) was dissolved in a mixture of purified water and 30 w/w% ethanol (Sigma-Aldrich). Two w/w% hydroxypropyl methylcellulose (METHOCEL E4M Premium, Dow Chemical, Midland, MI, USA) was added to this solution. The pH value was adjusted to 8.0±0.1 to ensure the dissolution of the active substance by adding triethanolamine (2 w/w% solution, Hungaropharma Ltd., Budapest, Hungary) if necessary (Supplementary materials).
Electroporation protocols
The noninvasive skin EP treatment was performed with a Mezoforte Duo Mez 120905-D instrument (Dr Derm Equipment Ltd., Budapest, Hungary). A polypropylene-covered treating handpiece with a 25 mm diameter plate electrode was used (modulation with 900 V pulses, a 5 ms voltage pulse was followed by a 20 ms break). Two hundred thirty µL diclofenac hydrogel was used, and the EP treatment time was 8 min.
HPLC measurements
The synovial washing fluid and plasma samples were analyzed using an Agilent HPLC system (Agilent Technologies, Palo Alto, CA, USA) equipped with an automated solvent delivery system, which has an integrated degasser (1260 Infinity Quaternary Pump, Agilent Technologies), an Agilent 1260 Infinity autosampler (Agilent Technologies) and a 1024-element diode array detector (1260 Infinity Diode Array Detector, Agilent Technologies). The system control and data acquisition were performed with Agilent ChemStation B.04.03 software (Agilent Technologies). The chromatographic parameters and the sample extraction procedure have been provided in the Supplementary materials.
Nociceptive tests
Mechanical hyperalgesia was quantified using a plantar aesthesiometer (Dynamic Plantar Aesthesiometer mod-37450; UgoBasile, Comerio, Italy) and was expressed as paw withdrawal thresholds. Thermal hyperalgesia was detected with the paw withdrawal test using a Hargreaves apparatus.Citation20 Baseline measurements were performed before the induction of arthritis, while the development of inflammation was investigated at the peak of nociceptive sensitivity 24 h after C/K injection.
Knee joint swelling (morphological assessment)
Joint inflammation was characterized by the changes in the diameter of the joints 48 h after C/K injection. The anteroposterior and mediolateral diameters were measured with a caliper square, and the cross-sectional area was calculated.
Analysis of gastric effects
Gastric lesions potentially associated with diclofenac toxicity were assessed at 48 h. After retrieving and washing with saline, photographs were taken of the freshly prepared stomachs. The location (near the pylorus, lesser curvature of the fundus, or diffuse) was recorded, and the extent of the lesions was evaluated by planimetric analysis using the ImageJ software (National Institutes of Health, Bethesda, MD, USA).
Synovial sampling
The skin over the knee was disinfected with povidone iodide, and 75 µL PBS was injected into the knee to collect synovial fluid. The fluid was centrifuged at 4°C for 5 min at 4,000 g in Eppendorf tubes. Then the samples were frozen at −80°C until they could be tested.
TNF-α levels
The cytokine content of the synovial washing fluid was measured with commercially available enzyme-linked immunosorbent assay kits (Quantikine Ultrasensitive ELISA kit; Biomedica Hungaria Ltd., Budapest, Hungary).
MPO activity
Tissue MPO activity was measured in synovium and periosteum biopsies using the method developed by Kuebler et al.Citation21 Briefly, the tissue was homogenized with Tris-HCl buffer (0.1 M, pH 7.4) containing 0.1 M polymethylsulfonyl fluoride to block tissue proteases and then centrifuged at 4°C for 20 min at 24,000 g. The MPO activities of the samples were measured at 450 nm (UV-1601 spectrophotometer; Shimadzu, Kyoto, Japan), and the data were corrected for the protein content.
XOR activity
Tissue biopsies were homogenized in a phosphate buffer (pH 7.4) containing 50 mM Tris-HCl, 0.1 mM EDTA, 0.5 mM dithiotreitol, 1 mM phenylmethylsulfonyl fluoride, 10 µg mL−1 soybean trypsin inhibitor, and 10 µg mL−1 leupeptin. The homogenate was centrifuged at 4°C for 20 min at 24,000 g, and the supernatant was loaded into centrifugal concentrator tubes. The activity of XOR was determined in the ultrafiltered supernatant by fluorometric kinetic assay based on the conversion of pterine to isoxanthopterine in the presence (total XOR) or absence (XOR activity) of the electron acceptor methylene blue.Citation22
Surgical procedure for the IVM examinations
A detailed description of the surgical procedure can be found elsewhere. In brief, the animals were anesthetized with IP sodium pentobarbital (45 mg kg−1) 6 h after the intra-articular C/K injection.Citation23 The jugular vein was cannulated for further supplementary doses of anesthetic. Cannulation of the trachea maintained the patent airway, and the arterial pressure was monitored through a carotid artery cannule (Statham P23Db transducer; Experimetria Ltd., Budapest, Hungary). The animals were placed on a specially designed heating pad in a supine position for the IVM examination, during which the slightly flexed knee joint of the hind limb was opened with a microsurgical technique. Surgical preparation included a longitudinal skin incision and a transverse cut of the quadriceps femoris tendon. After a circumferential cut on the joint capsule, the patella was turned aside, and the synovial membrane on the medial condyle of the tibia was visible.
IVM examinations
Synovial microcirculation was investigated by means of fluorescent IVM (Zeiss Axiotech Vario 100 HD microscope, 100 W HBO mercury lamp, Acroplan 20× water immersion objective), while the synovial membrane was superfused with 37°C saline. Erythrocytes were labeled with fluorescent isothiocyanate (0.2 mL intravenously, Sigma-Aldrich Chemicals) and leukocytes were stained with rhodamine-6G (0.1 mL intravenously, Sigma-Aldrich).
Video analysis
IVM records were analyzed offline and frame-to-frame using image analysis software (IVM, Pictron Ltd., Budapest, Hungary). Polymorphonuclear leukocytes (PMNs) were defined as cells adherent (stickers) to the endothelial lining within an observation period of 30 s. The number of adherent cells per mm2 of endothelial surface was counted in 5 postcapillary venules (diameter ranges from 11 to 15 µm) per animal.
Statistical analysis
Data analysis was performed with the SPSS 17.0 software (SPSS Inc., Chicago, IL, USA). Changes in variables within and between groups were analyzed by two-way analysis of variance, followed by the Holm–Sidak test. All data are expressed as means ± standard deviation of the mean. P-values <0.05 were considered statistically significant.
Results
Plasma and synovial diclofenac concentrations
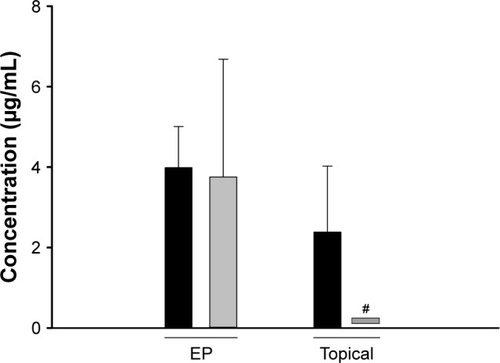
The plasma and the serum concentrations of diclofenac were the highest 10 min after the EP treatment; they then decreased at 30 min and remained constant at 60 and 120 min. EP-enhanced diclofenac delivery exhibited a significantly higher plasma level of diclofenac as compared with the simple topical application 10 min after the application (). There were no significant differences in the diclofenac content of the synovial fluid and the plasma after the EP-combined application. However, simple topical application did not result in detectable diclofenac content in the synovial fluid at the same point in time ().
Figure 2 Diclofenac concentrations in the serum (black columns) and the synovial washing fluid (gray columns) measured by HPLC (Series 1).
Abbreviations: ANOVA, analysis of variance; EP, electroporation; HPLC, high-performance liquid chromatography; SD, standard deviation of the mean.
Leukocyte–endothelial interactions
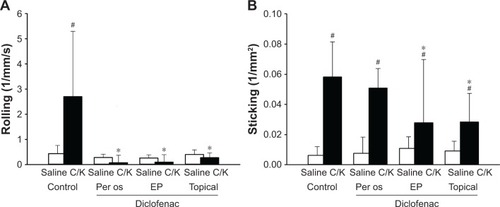
In the second experimental series, the microcirculatory consequences of the joint inflammation were quantified via IVM, and the PMN–endothelial interactions (rolling and sticking) in the postcapillary venules of the synovial membrane were determined. The rolling fraction of the PMNs in the postcapillary synovial venules exhibited a large degree of dispersion, and no baseline differences were observed between the C/K- and saline-injected knees or between the groups which participated in the treatment protocols (data not shown). However, the injection of C/K was accompanied by a statistically significant increase in PMN adherence (sticking) to the endothelial layer as compared to the control side (). This reaction was considerably reduced with the administration of oral diclofenac. However, it was only moderately ameliorated by the EP-enhanced diclofenac hydrogel, and there were no changes in response to the simple topical application of the hydrogel.
Figure 3 The effects of diclofenac treatments on the number of rolling (A) and sticking (B) leukocytes in the postcapillary venules of the synovial membrane (Series 3).
Abbreviations: ANOVA, analysis of variance; C/K, carrageenan/kaolin; SD, standard deviation of the mean.
Inflammatory enzyme activities and cytokine production
XOR activity was significantly increased in response to arthritis induction, in comparison with the saline-injected knee joint. These values were significantly decreased when diclofenac was applied orally or topically ().
Figure 4 The effects of diclofenac treatments on the C/K-induced changes in MPO activity (A), XOR activity (B), and TNF-α levels (C) (Series 2).
Abbreviations: ANOVA, analysis of variance; C/K, carrageenan/kaolin; SD, standard deviation of the mean.
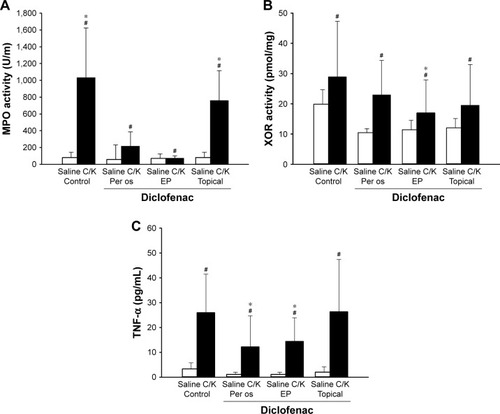
In the C/K-injected limbs, the MPO activity of the synovial tissue was significantly increased as compared with that of the saline-injected controls. In the oral diclofenac and EP-enhanced topical diclofenac-treated groups, MPO activity was significantly lower than in the nontreated animals. However, conventional topical treatment did not influence the increased MPO activity ().
The C/K injection resulted in a significant increase in TNF-α concentration in the synovial lavage fluid, which was diminished by both the oral intake and EP-enhanced topical treatment ().
Nociception and inflammatory edema
In the third series, the extent of inflammation was estimated with functional tests 24 h after arthritis induction. The mechanical touch sensitivity was considerably increased in response to arthritis as the C/K-injected limbs responded to a lower level of trigger than the saline-injected control limbs in animals receiving the saline vehicle (). This parameter was significantly diminished in response to oral and EP-enhanced topical diclofenac treatments, albeit that complete restoration was not achieved. The thermal nociceptive latency () was also significantly decreased in the injured leg in the saline-treated group, and oral and EP-enhanced topical diclofenac treatments exerted similar protective effects to those seen with the von Frey test.
Figure 5 The effects of diclofenac treatments on the C/K-induced changes in mechanical touch sensitivity (A), heat-provoked paw withdrawal latency (B), and changes in knee joint swelling (C) (expressed as a knee cross-section) (Series 2).
Abbreviations: ANOVA, analysis of variance; C/K, carrageenan/kaolin; SD, standard deviation of the mean.
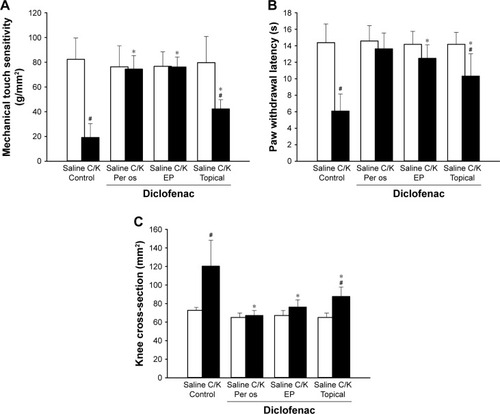
The changes in knee cross-section () furnish a direct and objective measure of joint inflammation. The cross-sectional area in the C/K-injected knees was significantly enlarged 48 h after the challenge but was significantly reduced by both the conventional topical and the EP-enhanced topical diclofenac treatments. In the case of oral diclofenac administration, complete restoration to the level for the saline-injected knees was achieved.
Adverse effects of diclofenac intake
The gastric adverse effects of diclofenac intake were assessed by planimetric analysis of ulcers in the gastric mucosa. The topically applied diclofenac sodium with or without EP had no deleterious effect on gastric mucosa; however, an equivalent dose of oral diclofenac sodium resulted in ulcer formation in 70% of the animals. The location of gastric ulcerations in the rat stomach was variable and included only mild lesions with edema, irritation, and petechia formation (Supplementary materials; Figure S1).
Discussion
This study has demonstrated the added value of EP to the transdermal delivery of diclofenac into the knee joint in experimental arthritis. The analgesic effect of EP-enhanced delivery was comparable to that of the oral administration and manifested in decreased nociceptive sensitivity, reduced joint swelling, and lower cytokine concentration in the synovial fluid and lower inflammatory enzyme activities in the synovial tissue. The EP treatment also influenced the number of PMN–endothelial interactions at the level of the synovial microcirculation.
Following oral administration, diclofenac absorbs rapidly through the gastrointestinal tract. However, due to first-pass metabolism, only 60% of the dose reaches the systemic circulation, where it bonds extensively to plasma proteins, mainly albumin.Citation24 Substantial concentration of the drug is attained in synovial fluid, which may be one of the sites of action of diclofenac. It has been shown that the antinociceptive and anti-inflammatory action of diclofenac is directly proportional to its concentration in the synovial fluid.Citation25 Diclofenac has a short biological half-life (approx 2 h) and is eliminated following biotransformation to glucuroconjugated and sulfate metabolites, which are excreted in urine.Citation26 The pharmacological action of oral drugs depends on the absorption into the circulation and subsequent distribution to the peripheral tissues; in contrast, efficacy of topical drugs relies on penetration through the skin.
EP is promising among skin penetration enhancement techniques; apart from transdermal delivery, application of EP has been widely investigated in cell biology, biotechnology, and electrochemotherapy.Citation13,Citation14,Citation16 EP applies high-voltage pulses to the biological membranes and results in conformation changes in their stereo structures. Transdermal drug penetration into the joint cavity is mostly limited by the low permeability of the stratum corneum of the skin, the thickness of the surrounding tissue layer, and the special physicochemical barrier function of the synovial membrane, which is commonly referred to as the “blood–joint barrier.”Citation27 However, EP is capable of opening transitory pores on complex structures, such as the multilamellar lipid bilayer of the stratum corneum and the synovial membrane.Citation28,Citation29 Macromolecules of up to 40 kDa can thus be transported through and/or into the skin.Citation11,Citation15
Electroporation is now widely used as an alternative to small interfering RNA or naked DNA delivery for targeted suppression of therapeutic genes into the knee joint in arthritis.Citation30,Citation31 However, electrotransfer of painkiller drugs into the knee joint is less widespread.Citation32 According to a recent review, plasma levels of diclofenac after topical administration decrease from 0.2% to 8% of those after oral administration.Citation33 Unfortunately, the resultant synovial concentration is also decreased, as compared to an equivalent oral dose. Effective concentrations in target tissues can be augmented with EP.Citation32 In accordance with literature data, our results revealed that EP causes higher concentration values in the serum as compared with the topical administration. The diclofenac concentration in the synovia was equal to the serum concentrations; however, conventional topical treatment did not result in a detectable amount of diclofenac sodium in the synovial fluid.
Intra-articular injection of C/K is a well-established model of an acute onset monoarthritis resembling osteoarthritis. In this model, arthritis is probably initiated by mechanical damage to the inner surface of the synovium resulting in an inflammatory response indirectly to the activation of the endothelial side of the synovial barrier. It is characterized by an initial nonphagocytic edema and rapid uptake of the late phagocytic inflammatory phase, where PMNs accumulate in the affected area.Citation19,Citation34 It has been demonstrated that PMNs are primed within 1 h and are in the majority up to 12 h after the arthritis induction; subsequently, they are replaced by predominating macrophages until the resolution of the inflammation at 48 h.Citation27 It has also been found that the rate of PMN infiltration is directly related to severity of inflammation in the synovial membrane.Citation35,Citation36 Based on the pivotal role of PMNs in the initiation and maintenance of joint disorders, we employed the PMN-derived experimental model of inflammatory arthritis in these studies.
Adhesive cell-to-cell interactions are regulated by β2 integrins (CD11/CD18) expressed on PMNs and their associated endothelial ligands (ICAMs and VCAMs).Citation37 The presence of adhesion molecules on postcapillary endothelial cells in the inflammatory synovial microenvironment has previously been shown and proven to be an appropriate marker for estimating inflammation.Citation23,Citation38,Citation39 These reactions can be quantitatively assessed by IVM, and the efficacy of various therapeutic interventions can also be judged objectively. PMN accumulation peaks very early, usually at 6–8 h in this model, and (at approx 24 h) macrophages predominate in the exudates thereafter.Citation40 Like other nonselective cyclooxygenase inhibitors, diclofenac diminishes the number of PMN–endothelial interactions.Citation41,Citation42 Sticking in the synovial vessels was considerably reduced with the oral administration of diclofenac. However, it was only moderately ameliorated by the EP-enhanced diclofenac hydrogel, and there were no changes in response to the simple topical application of the hydrogel.
Administration of C/K injection into the knee joint results in primary and secondary hyperalgesia in the inflammatory monoarthritis.Citation43 Secondary hyperalgesia develops at the paw to heat and mechanical stimuli, and primary hyperalgesia is present over the inflamed knee joint.Citation44,Citation45 Secondary hyperalgesia develops as a result of the sensitization of the dorsal horn neurons neighboring the spinal representation of the injured tissue.Citation46 Secondary hyperalgesia reactions were investigated at the peak of the joint inflammation and demonstrated a significant amelioration as a consequence of diclofenac treatment.Citation47 Like the oral diclofenac treatment, EP completely restored thermal nociceptive sensitivity and increased mechanical touch sensitivity, but to a lesser extent. Knee swelling, which is an objective parameter of joint inflammation, was significantly reduced with both the oral and the EP-enhanced diclofenac treatment.Citation48 Again, this increased volume was significantly reduced by both oral and EP-enhanced diclofenac treatments 48 h after arthritis induction.
The C/K-induced arthritis is also an appropriate model for the evaluation of the analgesic and anti-inflammatory properties of diclofenac. The TNF-α response is an early marker in carrageenan-induced inflammation, and thus the changes were measured in the synovial fluid 48 h after intra-articular C/K or saline injections. Free radical formation has been demonstrated in the synovial fluid and synovial membrane under clinical conditions and proposed as a causative factor in joint disorders.Citation22,Citation49 Specifically, oxidoreductive stress has been shown to play a fundamental role in the pathogenesis of arthrosis as a result of increased pressure in the synovial cavity, reduced capillary density and vascular changes, and due to the increased metabolic rate of synovial tissue in joint inflammation.Citation50–Citation52 Being a source of the oxygen free radical formation located in synovial cells, XOR activity has been shown to increase in joint inflammation.Citation36,Citation53 Moreover, joint inflammation was also associated with enhanced XOR activity in the synovial fluid.Citation54 Our present findings demonstrated increases in XOR activity in response to arthritis attenuated by diclofenac treatment, applied either by oral or simple topical routes of administration, the latter being more accentuated in the case of EP. PMNs are also important sources of free radicals through their NADPH oxidase 2 activities.Citation55 As for microcirculatory inflammatory reactions induced by inflammation, the increase in both the primary and secondary forms of PMN–endothelial interactions (rolling and firm adherence) were confined to the periosteal postcapillary venules. In this model, C/K-induced monoarthritis was the positive control. This aggressive arthritis model, which is associated with severe tissue destruction, is also known to be mediated by infiltrating PMNs.Citation19,Citation23 Data regarding the final step of PMN–endothelial interactions (ie, sticking) were well correlated with the tissue accumulation of PMNs, as determined by MPO activity. Diclofenac treatment attenuated the MPO activity in the inflamed synovial tissue, applied either via oral or EP-enhanced topical routes of administration.
The present study has provided evidence for the direct action of EP-enhanced transdermal diclofenac sodium delivery on the synovial microcirculation as proven by the decreased rolling and the reduced sticking of leukocytes. The biochemical measurements also demonstrated that diclofenac achieved an efficient tissue concentration in the synovium since inflammatory enzyme activities decreased. In summary, EP-enhanced transdermal diclofenac sodium delivery attenuated the microcirculatory deterioration and the consecutive stages of tissue inflammation; therefore, this type of mechanism might be an interesting focus for therapeutic strategies in arthritis.
Conclusion
EP-enhanced diclofenac delivery is well tolerated and possesses superior efficacy compared to simple topical application in experimental arthritis. The plasma and the joint concentrations of EP diclofenac are similar to those in oral administration. Further investigations are needed to determine the optimal parameters of EP and to diminish the plasma level of diclofenac.
Supplementary materials
Characterization of the diclofenac sodium-containing hydrogel
Rheological investigations and pH measurements were designed to characterize the hydrogel.
The pH of the semisolid formulations was measured with a Testo 206 pH meter (Testo SE & Co. KGaA, Lenzkirch, Germany). The probe of the device was immersed into three different parts of the sample. The pH was adjusted to 8.0±0.1.
The rheological properties were studied with a Physica MCR101 rheometer (Anton Paar, Graz, Austria). The measuring device was of the parallel plate type (with a 25 mm diameter and a gap height of 0.10 mm). The flow and viscosity curve were recorded over the shear rate range from 0.1 to 100 and from 100 to 0.1 s−1 at 32°C.
The flow curve of the gel can provide information on the viscosity changes under flow conditions and on the time dependency of the structure breakdown and recovery.
The flow curve of the gel presented shear thinning behavior, which means that the shear stress continuously increases with the shear rate, but the rate of the increase decreases. The curves showed slight thixotropy, which means the structure regeneration is time-dependent.
High-performance liquid chromatography (HPLC) measurements of the synovial washing fluid and plasma samples
The quantitative measurement of diclofenac sodium was carried out with the HPLC method.
Chemicals and reagents for HPLC
Methanol, orthophosphoric acid (85% v/v), potassium dihydrogen phosphate, isopropanol, and n-hexane were bought from VWR International GmbH (Darmstadt, Germany). All reagents and solutions used were analytical grade, except the methanol, which was HPLC grade. The purified water for the HPLC was acquired from TKA Smart2Pure device (TKA, Burladingen, Germany).
HPLC system and conditions
The HPLC analysis of diclofenac sodium was conducted using an Agilent HPLC system (Agilent Technologies, Palo Alto, CA, USA) equipped with an automated solvent delivery system, which has an integrated degasser (1260 Infinity Quaternary Pump, Agilent Technologies), an Agilent 1260 Infinity autosampler, and a 1024-element diode array detector (1260 Infinity Diode Array Detector, Agilent Technologies). The system control and data acquisition were performed with Agilent ChemStation B.04.03 software (Agilent Technologies). The chromatographic parameters are provided in Table S1.
The chromatographic separations were performed on Kromasil® 100 5C188 (250×4, 6 mm ID, 5 µm) (Phenomenex Inc., Torrance, CA, USA) analytical column. The column temperature was maintained at a constant 35°C. Separations were performed in gradient mode. The mobile phase was eluted at a flow rate of 1.5 mL min−1, and effluent was monitored at 254 nm.
The mobile phase consisted of two components. Component A was a mixture of methanol and PBS buffer at a ratio of 80:20 volume/volume percentage (potassium hydrogen phosphate, 5 mM and diluted orthophosphoric acid buffer, 5 mM, pH 2.5, adjusted by adding 85% orthophosphoric acid). Component B was a 20:80 (v/v) mixture of methanol and PBS buffer.
The preliminary ratio was 30:70 (v/v) A:B for 1 min; then the volume for B was increased from 70% to 100% after 4.1 min and sustained for 1 min before being returned to the initial conditions after 5 min. After a measurement, 2 min at 154 bar pressure for equilibration of the column was performed before the next injection. The retention time for diclofenac sodium was 4.5±0.054 min (relative standard deviation =0.29%) (Table S1).
Preparation of standard solutions and calibration samples
A stock solution of diclofenac sodium (1,000 µg/mL) was prepared in a 50:50 (v/v) mixture of methanol and HPLC water. External standard calibration solutions were prepared by dilution of the stock solution with the 50:50 (v/v) mixture of methanol and HPLC water to produce solutions with concentrations of 0 (as blank), 10, 20, 50, 100, and 150 µg/mL (six standard solutions).
Sample extraction procedure
An aliquot of plasma (1 mL) was combined with 100 µL of the internal standard solution (added amount 1.25 µg). The sample was acidified by adding 2 mL of 0.83 M phosphoric acid and 4 mL of hexane isopropyl alcohol (90:10). The mixtures were shaken for 10 min on a rotating shaker at 250 rpm and then centrifuged at 1,500 g for 10 min. The aqueous phase was frozen, and the organic phase was transferred to another tube and evaporated to dryness with nitrogen gas at room temperature. The dried residue was reconstituted with 300 µL of mobile phase and shaken for 15 s on a vortex mixer, and then a 20 µL aliquot was injected into the HPLC system.
An aliquot of 1.2 mL of synovial fluid was added to 2 mL of orthophosphoric acid (0.83 M) and 0.6 mL of isopropyl alcohol and vortexed for a few seconds. After that, 5.4 mL of n-hexane was added, and the mixture was centrifuged at 9,000 g for 5 min. The organic phase was transferred to a clean tube, and the solvent was evaporated to dryness with nitrogen gas at 30°C. The residue was dissolved in 1.2 mL of the mobile phase by vortexing. An aliquot of 20 µL was injected into the chromatograph.
Linearity
Linearity was studied by preparing standard solutions in the range of 0–150 µg mL−1 (n=6), plotting a graph of concentration against area under the curve and determining the linearity. Two methods (the short and long methods) were compared to choose the optimal one for the HPLC analysis (Table S2).
Based on the linearity test and the low relative standard deviation % values, the short method is recommended. The advantage is a runtime shortened by 42% (35–20 min; Figure S2).
Figure S1 Gastric adverse effects of diclofenac intake.
Notes: The effects of diclofenac treatment on the gastric mucosa. (A) Diclofenac treatment-induced gastric adverse effects. Scale bars represent 10 mm. Black arrows show edema, irritation, and petechia formation. (B) Mean area of gastric lesions. The white column represents the control group (per os saline-treated), and the black column represents the per os diclofenac-treated group. The pale and dark columns (not visible, as values are 0.000) represent the topical and EP-combined topical diclofenac-treated groups, respectively. Data are presented as means ± SD. *p<0.05 vs per os diclofenac-treated group (Kruskal–Wallis one-way analysis and Dunnet test).
Abbreviations: EP, electroporation; SD, standard deviation of the mean.
Figure S2 The flow curve of the diclofenac sodium-containing hydrogel.
Acknowledgments
The authors would like to thank Dr Derm Clinic of Anti-aging Dermatology, Aesthetic Laser and Plastic Surgery (1026 Budapest, Hungary) for providing the Mezoforte Duo Mez120905-D instrument. The study was supported by grants from the National Research Development and Innovation Office (NKFI K120232) and Economic Development and Innovation Operational Program (GINOP-2.3.2-15-2016-00015). PH and EB contributed equally to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- ReginsterJYThe prevalence and burden of arthritisRheumatology (Oxford)200241Suppl 13612173279
- HelmickCGFelsonDTLawrenceRCEstimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part IArthritis Rheum2008581152518163481
- PetersonKMcDonaghMThakurtaSDrug class review: non-steroidal anti inflammatory drugs (NSAIDs). Final update 4 reportPortland (OR)Oregon Health & Science University2010
- PavelkaKA comparison of the therapeutic efficacy of diclofenac in osteoarthritis: a systematic review of randomised controlled trialsCurr Med Res Opin201228116317822168216
- BrunnerMDehghanyarPSeigfriedBMartinWMenkeGMullerMFavourable dermal penetration of diclofenac after administration to the skin using a novel spray gel formulationBr J Clin Pharmacol200560557357716236050
- HeynemanCALawless-LidayCWallGCOral versus topical NSAIDs in rheumatic diseases: a comparisonDrugs200060355557411030467
- DenetARPréatVTransdermal delivery of timolol by electroporation through human skinJ Control Release200388225326212628332
- TachibanaKTransdermal delivery of insulin to alloxandiabetc rabbits by ultrasound exposurePharm Res1992979529541438012
- BommannanDOkuyamaHStaufferPGuyRHSonophoresis. I. The use of high-frequency ultrasound to enhance transdermal drug deliveryPharm Res1992945595641495903
- PrausnitzMRBoseVLangerRWeaverJCElectroporation of mammalian skin: A mechanism to enhance transdermal drug deliveryProc Natl Acad Sci U S A1993902210504105088248137
- VanbeverRLecouturierNPréatVTransdermal delivery of metoprolol by electroporationPharm Res19941111165716627870686
- RiviereJEMonteiro-RiviereNARogersRAPulsatile transdermal delivery of LHRH using electroporation: drug delivery and skin toxicologyJ Control Release1995363229233
- MirLOrlowskiSMechanisms of electrochemotherapyAdv Drug Deliv Rev199935110711810837692
- HellerRGilbertRJaroszeskiMJClinical applications of electrochemotherapyAdv Drug Deliv Rev199935111912910837693
- LombryCDujardinNPréatVTransdermal delivery of macromolecules using skin electroporationPharm Res2000171323710714605
- WeaverJCChizmadzhevYATheory of electroporation: a reviewBioelectrochem Bioenerg1996412135160
- DenetAVanbeverRPréatVSkin electroporation for transdermal and topical deliveryAdv Drug Deliv Rev200456565967415019751
- KhajuriaDKRazdanRMahapatraDRDescription of a new method of ovariectomy in female ratsRev Bras Reumatol201252346247022641600
- DaySMLockhartJCFerrellWRMcLeanJSDivergent roles of nitrergic and prostanoid pathways in chronic joint inflammationAnn Rheum Dis200463121564157015547079
- HargreavesKDubnerRBrownFFloresCJorisJA new and sensitive method for measuring thermal nociception in cutaneous hyperalgesiaPain19983217788
- KueblerWMAbelsCSchuererLGoetzAEMeasurement of neutrophil content in brain and lung tissue by a modified myeloperoxidase assayInt J Microcirc Clin Exp199616289978737712
- BeckmanJSParksDAPearsonJDMarshallPAFreemanBAA sensitive fluorometric assay for measuring xanthine dehydrogenase and oxidase in tissuesFree Radic Biol Med1989666076152753392
- HartmannPSzabóAErosGAnti-inflammatory effects of phosphatidylcholine in neutrophil leukocyte-dependent acute arthritis in ratsEur J Pharmacol20096221–3586419766625
- ToddPASorkinEMDiclofenac sodium. A reappraisal of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacyDrugs19883532442853286213
- VetterGA comparison of naproxen and diclofenac sodium in the treatment of osteoarthritis in elderly patientsBr J Clin Pract19853972762813896286
- DaviesNMAndersonKEClinical pharmacokinetics of diclofenac. Therapeutic insights and pitfallsClin Pharmacokinet19973331842139314611
- DayROMcLachlanAJGrahamGGWilliamsKMPharmacokinetics of nonsteroidal anti-inflammatory drugs in synovial fluidClin Pharmacokinet199936319121010223168
- NishimuraTAkimotoMMiyazakiMNomotoMMiyakawaMDevelopments of transdermal transport system during skin iontophoresis and electroporationPIERS Online201068759763
- BlagusTMarkelcBCemazarMIn vivo real time monitoring system of electroporation mediated control of transdermal and topical drug deliveryJ Control Release2013172386287124113487
- ZhenSHeyongYXiaomingYInhibition of osteoarthritis in rats by electroporation with interleukin-1 receptor antagonistJ Biomed Sci Eng201697323336
- CemazarMSersaGElectrotransfer of therapeutic molecules into tissuesCurr Opin Mol Ther20079655456218041666
- FengSZhuLHuangZControlled release of optimized electroporation enhances the transdermal efficiency of sinomenine hydrochloride for treating arthritis in vitro and in clinicDrug Des Devel Ther20171117371752
- HagenMBakerMSkin penetration and tissue permeation after topical administration of diclofenacCurr Med Res Opin20173391623163428681621
- HansraPMoranELFornasierVLBogochERCarrageenan-induced arthritis in the ratInflammation200024214115510718116
- CremascoVGrahamDBNovackDVSwatWFaccioRVav/phospholipase Cγ2-mediated control of a neutrophil-dependent murine model of rheumatoid arthritisArthritis Rheum20085892712272218759305
- SmithEMcGettrickHMStoneMADuffy antigen receptor for chemokines and CXCL5 are essential for the recruitment of neutrophils in a multicellular model of rheumatoid arthritis synoviumArthritis Rheum20085871968197318576313
- SpringerTATraffic signals for lymphocyte recirculation and leukocyte emigration: the multistep paradigmCell19947623013147507411
- HartmannPErősGVargaRLimb ischemia-reperfusion differentially affects the periosteal and synovial microcirculationJ Surg Res2012178121622222472698
- HaleLPMartinMEMcCollumDEImmunohistologic analysis of the distribution of cell adhesion molecules within the inflammatory synovial microenvironmentArthritis Rheum198932122302463839
- GilroyDWColville-NashPRWillisDChiversJPaul-ClarkMJWilloughbyDAInducible cyclooxygenase may have anti-inflammatory propertiesNat Med19995662162210371498
- SchejaAForsgrenAMarsalLWollheimFInhibition of in vivo leucocyte migration by NSAIDsClin Exp Rheumatol19853153583978895
- MartinezLLOliveiraMAMiguelASEnalapril interferes with the effect of diclofenac on leucocyte-endothelium interaction in hypertensive ratsJ Cardiovasc Pharmacol200443225826514716214
- RadhakrishnanRMooreSASlukaKAUnilateral carrageenan injection into muscle or joint induces chronic bilateral hyperalgesia in ratsPain2003104356757712927629
- SlukaKABaileyKBogushJOlsonRRickettsATreatment with either high or low frequency TENS reduces the secondary hyperalgesia observed after injection of kaolin and carrageenan into the knee jointPain1998771971029755024
- SkybaDARadhakrishnanRSlukaKACharacterization of a method for measuring primary hyperalgesia of deep somatic tissueJ Pain200561414715629417
- HardyJDHaroldGGoodellWGoodellHExperimental evidence on the nature of cutaneous hyperalgesiaJ Clin Invest195029111514015399521
- LeeTHWangCJWuPCBuerkleHLinSHYangLCThe thermal and mechanical anti-hyperalgesic effects of pre- versus post-intrathecal treatment with lamotrigine in a rat model of inflammatory painLife Sci200270253039304712138017
- Peter-SzaboMKekesiGNagyESziverEBenedekGHorvathGQuantitative characterization of a repeated acute joint inflammation model in ratsClin Exp Pharmacol Physiol2007345–652052617439426
- KennettECDaviesMJGlycosaminoglycans are fragmented by hydroxyl, carbonate, and nitrogen dioxide radicals in a site-selective manner: implications for peroxynitrite-mediated damage at sites of inflammationFree Radic Biol Med200947438940019427378
- BlakeDRWinyardPGMarokRThe contribution of hypoxia-reperfusion injury to inflammatory synovitis: the influence of reactive oxygen intermediates on the transcriptional control of inflammationAnn N Y Acad Sci1994723308317
- MappPIGrootveldMCBlakeDRHypoxia, oxidative stress and rheumatoid arthritisBr Med Bull19955124194367552073
- TakPPBresnihanBThe pathogenesis and prevention of joint damage in rheumatoid arthritis: advances from synovial biopsy and tissue analysisArthritis Rheum200043122619263311145019
- SaricaogluFDalDSalmanAEDoralMNKilinçKAyparUKetamine sedation during spinal anesthesia for arthroscopic knee surgery reduced the ischemia-reperfusion injury markersAnesth Analg2005101390490916116012
- HanachiNCharefNBaghianiAComparison of xanthine oxidase levels in synovial fluid from patients with rheumatoid arthritis and other joint inflammationsSaudi Med J200930111422142519882054
- BedardKKrauseKHThe NOX family of ROS-generating NADPH oxidases: physiology and pathophysiologyPhysiol Rev200787124531317237347