
Abstract
Objective
Osteoporosis is the most common metabolic bone disease and a major public health problem worldwide. Thiazides are widely used as antihypertensive agents with good tolerability and efficacy. Furthermore, thiazides have long been regarded as candidates for the prevention of postmenopausal bone loss. However, there is insufficient evidence that thiazides have a sustained beneficial effect on preserving bone mass and preventing osteoporosis to date.
Materials and methods
We searched the PubMed, the Cochrane Library, and Embase in June 2018 for randomized controlled trials on the use of thiazides to treat osteoporosis. Continuous outcomes are presented as the standardized mean difference (SMD) and 95% CI. Furthermore, P-values <0.05 were considered significant.
Results
Five trials with 756 patients were randomly assigned in the five trials included in this meta-analysis. Serum calcium level was higher in the thiazide group than in the control group (SMD 0.33, 95% CI [0.16, 0.50]), and urinary calcium level was significantly lower in the thiazide group (SMD −0.35, 95% CI [−0.52, −0.17]). There was no significant difference in bone mineral density between the two groups (SMD 0.19, 95% CI [−0.16, 0.54]).
Conclusion
Thiazides might play a role in preserving bone mass and be effective in the prevention and treatment of osteoporosis. Future high-quality trials are needed to confirm our findings in the future.
Introduction
Osteoporosis is a chronic systemic skeletal disorder characterized by decreased bone mass and qualitative alterations in bone and is accompanied by an increased risk of fracture.Citation1–Citation3 It is a common consequence of aging that affectŝ200 million individuals and causes 8.9 million fractures every year.Citation4 In the USA and Europe, 30% of all postmenopausal women have osteoporosis.Citation5 The diagnostic of osteoporosis by the World Health Organization (WHO) criteria is based on the measurement of bone mineral density (BMD), which is usually measured using densitometry applications such as dual X-ray photon absorptiometry.Citation2,Citation6 However, it is not sufficient only to do the densitometry as a diagnostic because many fragility fractures after osteoporosis occurs in the range of normal BMD values, so a clinical diagnostic should combine densitometric examination with clinical evaluations, laboratory tests, and related differential diagnoses.Citation1,Citation2 The National Osteoporosis Foundation suggested that treatment for osteoporosis should start with a non-pharmacologic approach, such as resistance and weight-bearing exercise.Citation6,Citation7 Bisphosphonates are typically the first-line pharmacologic agents for the treatment of patients with osteoporosis.Citation8,Citation9 However, osteonecrosis of the jaw is a known complication in a subset of patients receiving bisphosphonate treatment.Citation10,Citation11 Furthermore, a previous study showed that in MEPS, bisphosphonate use was increased predominantly in women (from 3.5% in 1996 to 16.6% in 2007) compared with men (2.3% in 2007), and women experienced the vast majority of subtrochanteric fractures.
Thiazide diuretics were the first tolerated efficient anti-hypertensive drugs and have been used as a part of treatment strategies in numerous clinical trials involving hypertension; they are considered unequivocally effective in the treatment of hypertensive patients.Citation12,Citation13 Furthermore, thiazides have been regarded as candidates for the prevention of postmenopausal bone loss for many years because of their ability to decrease urinary calcium excretion at the level of the renal tubules.Citation14 Defects in the tubular excretion of calcium are one of the main causes of osteoporosis. In a previous study, thiazide diuretics were shown to slow the rate of bone loss in older adults.Citation15 Furthermore, it has been demonstrated that thiazides have direct effects on osteoclasts and osteoblasts.Citation16,Citation17 However, there is insufficient evidence that thiazides have a sustained beneficial effect in preserving bone mass and preventing osteoporosis to date.
This systematic review and meta-analysis was conducted to determine whether thiazides are beneficial for preserving bone mass and have an effect on the prevention and treatment of osteoporosis. In this study, we analyzed the effect of thiazides on serum and urinary calcium levels and BMD.
Materials and methods
Search strategy
We searched PubMed, the Cochrane Library, and Embase in June 2018 for studies using the following combination of terms: “Thiazides,” “Benzothiadiazines,” “Bendroflu-methiazide,” “Chlorothiazide,” “Cyclopenthiazide,” “Diazoxide,” “Hydroflumethiazide,” “Methyclothiazide,” and “Polythiazidein” in combination with “Osteoporosis,” “Osteoporoses,” “Osteoporosis, Post-Traumatic,” “Osteoporosis, Post Traumatic,” “Post-Traumatic Osteoporoses,” “Post-Traumatic Osteoporosis,” “Osteoporosis, Senile,” “Osteoporoses, Senile,” “Senile Osteoporoses,” “Senile Osteoporosis,” “Osteoporosis, Involutional,” “Osteoporosis, Age-Related,” “Osteoporosis, Age Related,” “Bone Loss, Age-Related,” “Age-Related Bone Loss,” “Age-Related Bone Losses,” “Bone Loss, Age Related,” “Bone Losses, Age-Related,” “Age-Related Osteoporosis,” “Age Related Osteoporosis,” “Age-Related Osteoporoses,” and “Osteopo-roses, Age-Related,” and only English papers were included. Furthermore, the articles in reference lists of the related studies were also reviewed. Two independent reviewers examined the titles and abstracts for eligibility, and if we cannot judge whether the articles are eligible based on the titles and abstracts, the full-text article was obtained and reviewed for final inclusion. Moreover, we only included the complete original articles.
Study selection
The studies were selected according to the following inclusion criteria: 1) the studies were designed as randomized controlled trials (RCTs); 2) participants were adults with osteoporosis or the high-risk group of osteoporosis; 3) the thiazide intervention was compared with placebo control in the meantime – patients in the control groups used placebo that did not influence bone anabolism. Furthermore, studies were excluded according to the following exclusion criteria: 1) participants had taken thiazides, unless patients had gone through a washout period; 2) the patients were allergic to thiazides formerly or currently; and 3) except for RCTs, other types of studies such as abstracts, review articles, and letters.
Data extraction and quality assessment
The following data with regard to thiazide intervention in patients with osteoporosis were extracted: 1) name of the first author, publication year; 2) participants’ characteristics (gender, mean age); 3) type of intervention; 4) number of cases and participants; and 5) BMD, serum calcium, and urinary calcium from each included study. Moreover, the quality of the studies we selected was assessed according to the Cochrane risk of bias tool, including selection bias, performance bias, detection bias, attrition bias, and reporting bias.Citation18 Each category included the following three levels: low risk, unclear risk, and high risk.
Statistical analysis
The data syntheses were performed by Review Manager Software (RevMan version 5.2; The Cochrane Collaboration, Copenhagen, Denmark). Only outcomes addressed by at least two studies were analyzed. The meta-analysis was analyzed with a random effects model. Continuous outcomes were presented as standardized mean difference (SMD) and 95% CI. Study heterogeneity was measured using Cochran’s Q statistic and ICitation2 statistic, and it was regarded significant when P<0.05 for the former and ICitation2 >50% for the latter.Citation19,Citation20
Results
Literature search
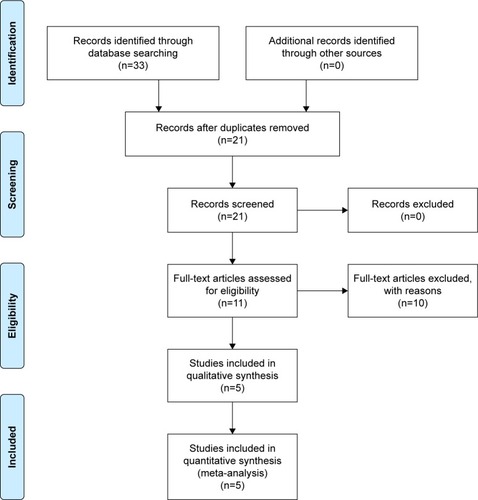
A total of 33 potentially relevant studies as of June 2018 were identified, 12 of which were excluded because they were duplicate publications, were not RCTs, or included exposures or end points not related to our meta-analysis. After a full-text review of the remaining studies, five publications were included.Citation21–Citation25 shows the details of the screening process.
Figure 1 Flow diagram of the search and selection of the studies included in this meta-analysis.
Study and patient characteristics
The five eligible studies included 756 participants, including 614 women (81.2%) and 142 men (18.8%). Moreover, types of interventions included bendroflumethiazide and hydro-chlorothiazide. The total number of the included patients with active treatment and placebo treatment is 372 and 384, respectively. The duration of thiazide therapy ranged from 2 to 3 years. Overall mean age was 64.45±6.69 (mean ± SD) years. shows the characteristics of the included studies in detail.
Table 1 Characteristics of the included studies
Quality of trials
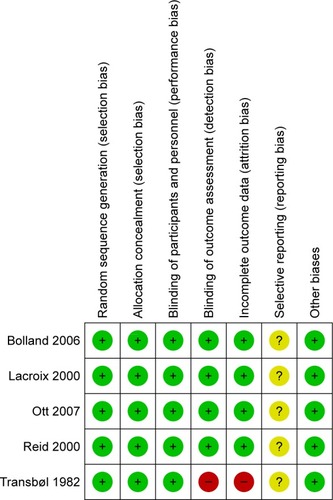
The quality of the five included RCTs was assessed using the Cochrane risk of bias tool, as described in in detail. All the studies were judged to be at low risk of bias in terms of random sequence generation, allocation concealment, and blinding of participants and personnel. One trial was judged to be at high risk for incomplete outcome data and blinding of outcome assessment, while other trials (such as recruitment bias and contamination of the interventions) were at low risk. The rate of patients lost to follow-up was also assessed, and one trial indicated the presence of loss to follow-up, which was 3.44%.Citation22 Disagreement was resolved by discussion among the authors.
Figure 2 Risk of bias summary.
Serum calcium
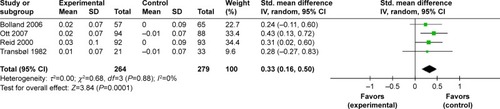
Four trials (543 patients) included an analysis of serum calcium after the intervention. The results showed that patients treated with thiazides had significantly higher calcium levels compared with patients in the control group (SMD 0.33, 95% CI [0.16, 0.50]; ICitation2 of heterogeneity 0%; random effects model) ().
Figure 3 Forest plot for serum calcium.
Urinary calcium
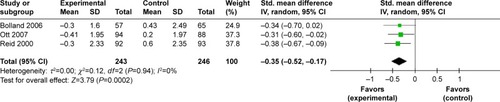
Three trials (489 patients) included an analysis of urinary calcium after the intervention. The results showed that patients in the thiazide group showed significantly lower urinary calcium levels compared with the control groups (SMD −0.35, 95% CI [−0.52, −0.17]; ICitation2 of heterogeneity 0%; random effects model) ().
Figure 4 Forest plot for urinary calcium.
BMD
BMD data obtained using dual-energy X-ray absorptiometry were analyzed in two studies involving 398 patients (200 in the thiazide group and 198 in the control group).Citation22,Citation24 The results showed that patients treated with thiazides had no statistically significant difference in BMD compared with the control group (SMD 0.19, 95% CI [−0.16, 0.54]; ICitation2 of heterogeneity 68%; random effects model) (). Although significant heterogeneity was evident, sensitivity analysis was not performed due to the small number of trials. The significant heterogeneity could be attributed to the different methods of evaluation used in the trials.
Figure 5 Forest plot for bone mineral density.

Discussion
Thiazides have been widely used as antihypertensive drugs with a tolerable efficiency.Citation26 Previous studies have shown that thiazides may also affect bone metabolism and BMD.Citation27,Citation28 However, the effectiveness of thiazides in the treatment of osteoporosis has not been fully elucidated. The present meta-analysis summarized the results of the five included RCTs that assessed the effects of thiazides on the BMD and mineral metabolism in the elderly. The findings suggest that thiazides have some benefits for preserving bone mass and may be effective in the prevention and treatment of osteoporosis.
BMD in the thiazide group did not differ significantly from that in the control group. The quality of this evidence was assessed to be very low because only two RCTs provided BMD data.Citation22,Citation24 Therefore, insufficient data limited the quality of evidence. Four of the RCTs indicated that thiazides had a positive effect on BMD.Citation21–Citation24 Thus, there is evidence to support the beneficial effects of thiazides on BMD, but this was not confirmed in this analysis. If we want to confirm that thiazides have beneficial effect on BMD, more high-quality RCTs are needed in the future.
Measurement of serum calcium should be one of the first-line investigations in patients with osteoporosis.Citation1 Elevated serum calcium is associated with a wide range of adverse health outcomes including osteoporosis, and decreased urinary calcium excretion can lead to increased serum calcium levels. In the current meta-analysis, the results suggest that the use of thiazides could lead to a significant increase in serum calcium level compared with that in the control group. Furthermore, urinary calcium excretion has been shown to be low in many postmenopausal women and in the elderly because of impaired intestinal calcium absorption.Citation29,Citation30 Previous studies have reported that thiazides can reduce urinary calcium excretion by 25%–40%, potentially improving bone mass and reducing fracture risk, while intestinal calcium absorption keeps on persistently elevated.Citation31–Citation35 In these results, urinary calcium excretion declined signifi-cantly in the thiazide group. There was no heterogeneity in these results, which could reach statistical significance in the current meta-analysis. To sum up, combining the results, the meta-analysis indicated that thiazides have the possible effect on the prevention and treatment of osteoporosis.
Certain limitations of this meta-analysis should be acknowledged. First, evidence of the benefit was limited because of the small number of RCTs. Second, not all the included studies provided all the data that we sought; for example, although two studies reported significant between-group differences in BMD, the data provided were not detailed. Thus, quality of the evidence was limited by insufficient data. Third, this meta-analysis included the only papers published in English language, and so trials published in other languages were systematically excluded. Fourth, over 81.2% (n=614) of the included subjects were females and only 18.8% (n=142) of the included subjects were males, so the results of this study are more applicable to females. Despite these limitations, this study supports the use of thiazides to increase serum calcium levels and decrease urinary calcium excretion in patients with osteoporosis.
Conclusion
The results of this meta-analysis demonstrated that thiazides might play a role in preserving bone mass in patients with osteoporosis and have the possible effect on the prevention and treatment of osteoporosis. However, we must interpret the results cautiously because of some limitations, and future high-quality trials are needed to confirm these findings.
Disclosure
The authors report no conflicts of interest in this work.
References
- RossiniMAdamiSBertoldoFGuidelines for the diagnosis, prevention and management of osteoporosisReumatismo201668113927339372
- UlivieriFMCaudarellaRCamisascaMAssessment of bone quality in osteoporosis treatment with bone anabolic agents: really something new?Curr Rheumatol Rev2018141536127908253
- ShiZZhouHPanBEffectiveness of Teriparatide on Fracture Healing: A Systematic Review and Meta-AnalysisPLoS One20161112e016869127997614
- HadjiPJacobLKostevKGender- and age-related treatment compliance in patients with osteoporosis in GermanyPatient Prefer Adherence2016102379238527920504
- BockOFelsenbergDBisphosphonates in the management of postmenopausal osteoporosis – optimizing efficacy in clinical practiceClin Interv Aging20083227929718686751
- CosmanFde BeurSJLeboffMSClinician’s Guide to Prevention and Treatment of OsteoporosisOsteoporos Int201425102359238125182228
- HintonPSNighPThyfaultJEffectiveness of resistance training or jumping-exercise to increase bone mineral density in men with low bone mass: A 12-month randomized, clinical trialBone20157920321226092649
- BlackDMBauerDCSchwartzAVCummingsSRRosenCJContinuing bisphosphonate treatment for osteoporosis – for whom and for how long?N Engl J Med2012366222051205322571169
- RodanGReszkaAGolubERizzoliRBone safety of long-term bisphosphonate treatmentCurr Med Res Opin20042081291130015324532
- OteriGBramantiENigroneVCicciùMDecayed, Missing, and Filled Teeth Index and Periodontal Health in Osteoporotic Patients Affected by BRONJ: An Observational StudyJ Osteoporos2013201323128924455411
- Nastro SiniscalchiEAllegraADe PonteFSSpontaneous Healing of Clodronate-Related Osteonecrosis of the JawJ Craniofac Surg2017287e687e68928857991
- ReillyRFPeixotoAJDesirGVThe evidence-based use of thiazide diuretics in hypertension and nephrolithiasisClin J Am Soc Nephrol20105101893190320798254
- SalvettiAGhiadoniLThiazide diuretics in the treatment of hypertension: an updateJ Am Soc Nephrol2006174 Suppl 2S25S2916565243
- HeshmatiHMKhoslaSBurrittMFO’FallonWMRiggsBLA defect in renal calcium conservation may contribute to the pathogenesis of postmenopausal osteoporosisJ Clin Endocrinol Metab1998836191619209626119
- WasnichRDavisJRossPVogelJEffect of thiazide on rates of bone mineral loss: a longitudinal studyBMJ19903016764130313052271853
- HallTJSchaueblinMHydrochlorothiazide inhibits osteoclastic bone resorption in vitroCalcif Tissue Int19945542662687820777
- LajeunesseDDelalandreAGugginoSEThiazide diuretics affect osteocalcin production in human osteoblasts at the transcription level without affecting vitamin D3 receptorsJ Bone Miner Res200015589490110804019
- HigginsJPAltmanDGGotzschePCCochrane Bias Methods Group; Cochrane Statistical Methods GroupThe Cochrane Collaboration’s tool for assessing risk of bias in randomised trialsBMJ2011343d592822008217
- HigginsJPThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- ShiZZhouHLuLAquatic Exercises in the Treatment of Low Back Pain: A Systematic Review of the Literature and Meta-Analysis of Eight StudiesAm J Phys Med Rehabil201897211612228759476
- BollandMJAmesRWHorneAMOrr-WalkerBJGambleGDReidIRThe effect of treatment with a thiazide diuretic for 4 years on bone density in normal postmenopausal womenOsteoporos Int200718447948617120180
- LacroixAZOttSMIchikawaLScholesDBarlowWELow-dose hydrochlorothiazide and preservation of bone mineral density in older adults. A randomized, double-blind, placebo-controlled trialAnn Intern Med2000133751652611015164
- OttSMLaCroixAZScholesDIchikawaLEWuKEffects of three years of low-dose thiazides on mineral metabolism in healthy elderly personsOsteoporos Int20081991315132218425402
- ReidIRAmesRWOrr-WalkerBJHydrochlorothiazide reduces loss of cortical bone in normal postmenopausal women: a randomized controlled trialAm J Med2000109536237011020392
- TransbølIChristensenMSJensenGFChristiansenCMcNairPThiazide for the postponement of postmenopausal bone lossMetabolism19823143833867078423
- SinhaADAgarwalRThiazides are useful agents in CKDJ Am Soc Hypertens201610428828926987648
- MortonDJBarrett-ConnorELEdelsteinSLThiazides and bone mineral density in elderly men and womenAm J Epidemiol199413911110711158192143
- RejnmarkLVestergaardPPedersenARHeickendorffLAndreasenFMosekildeLDose-effect relations of loop- and thiazide-diuretics on calcium homeostasis: a randomized, double-blinded Latin-square multiple cross-over study in postmenopausal osteopenic womenEur J Clin Invest2003331415012492451
- GallagherJCRiggsBLEismanJHamstraAArnaudSBDeLucaHFIntestinal calcium absorption and serum vitamin D metabolites in normal subjects and osteoporotic patients: effect of age and dietary calciumJ Clin Invest1979643729736468987
- SakhaeeKNicarMJGlassKZerwekhJEPakCYReduction in intestinal calcium absorption by hydrochlorothiazide in postmenopausal osteoporosisJ Clin Endocrinol Metab1984596103710436490791
- PakCYNicarMNorthcuttCThe definition of the mechanism of hypercalciuria is necessary for the treatment of recurrent stone formersContrib Nephrol1982331361516749417
- AdamsJSSongCFKantorovichVRapid recovery of bone mass in hypercalciuric, osteoporotic men treated with hydrochlorothiazideAnn Intern Med1999130865866010215562
- FeskanichDWillettWCStampferMJColditzGAA prospective study of thiazide use and fractures in womenOsteoporos Int19977179849102069
- HeaneyRPLifelong calcium intake and prevention of bone fragility in the agedCalcif Tissue Int199149Suppl(S1)S42S451933596
- LambergBAKuhlbackBEffect of chlorothiazide and hydrochlorothiazide on the excretion of calcium in urineScand J Clin Lab Invest195911435135714413581