
Abstract
Objective
Remimazolam besylate is a novel ultra-short-acting benzodiazepine that is rapidly hydrolyzed to zolpidem propionic acid by tissue lipases. We designed this study to compare the safety and efficacy of remimazolam besylate alfentanil versus dexmedetomidine–alfentanil for fiberoptic bronchoscopy (FB).
Methods
One hundred and twenty patients undergoing FB into this prospective randomized controlled trial were divided into two groups. The anesthesia induction consisted of 6 mg/kg/h of remimazolam besylate in the RA group and 0.5 μg/kg of dexmedetomidine in the DA group. 1–2 mg/kg/h of remimazolam besylate or 0.2–0.7 µg/kg/h of dexmedetomidine were administered to maintain during FB. The lowest oxygen saturation, success rate of FB, hemodynamics, time metrics, bronchoscopy feasibility, drug dose requirements, patient and bronchoscopist satisfaction scores, occurrence of intraoperative awareness, number of patients willing to repeat FB with the same sedation regimen, and occurrence and severity of adverse events.
Results
The lowest oxygen saturation during the FB was significantly higher in the RA group (P = 0.001). Compared with the variables in the DA group, peripheral oxygen saturation, systolic blood pressure, and diastolic blood pressure were significantly lower at T2 and T3 in the RA group (P < 0.05). Heart rates were significantly higher from T2 to T4 in the DA group (P < 0.05). More patients experienced bradycardia in the DA group (P = 0.041). Compared with time metrics in the DA group, the induction time, fully-alert time, and recovery room-leaving time were all significantly shorter in the RA group (P < 0.05). The bronchoscopy feasibility scores in the RA group were significantly lower at T2, whereas they were lower at T3 in the DA group (P < 0.05).
Conclusion
Remimazolam besylate is superior to dexmedetomidine when combined with alfentanil during FB, promoting faster patients’ recovery, better operative conditions and respiratory stability with similar rates of occurrence and severity of adverse events.
Introduction
Fiberoptic bronchoscopy (FB) is an essential procedure for diagnosing and treating respiratory diseases.Citation1 The FB frequency and quality have increased over the past decades, and sedation is recommended by most guidelines for a comfortable procedure in patients without contraindications.Citation2,Citation3 An ideal anesthesia method provides rapid onset and recovery, stable hemodynamics, and early mobilization, achieving high patient turnover, shortening off-work times, and reducing postoperative complication rates.Citation4,Citation5 However, the optimal sedation/analgesia regimen for comfortable FB procedures remains unclear because the line between moderate sedation (conscious sedation) and deep sedation is blurry.Citation6
Drug combinations are more beneficial than single-drug regimens in bronchoscopy sedation because combinations enhance each drug’s therapeutic action while minimizing their adverse effects.Citation7 Benzodiazepines have been the most frequently used sedative agent during bronchoscopies. Combinations of midazolam and opiates may induce hypoventilation, particularly in patients with pre-existing respiratory disease.Citation8–10 Remimazolam besylate is a novel ultra-short-acting benzodiazepine. It is metabolized by tissue lipases and rapidly hydrolyzed to zolpidem propionic acid, an agent with almost no sedation activity. Moreover, remimazolam besylate can be administered to patients with liver and kidney dysfunction because its metabolism is not liver- or kidney-dependent.Citation11 In a study, remimazolam besylate was superior to propofol at preserving the patient’s spontaneous breathing and reducing the incidence of respiratory depression.Citation12 Dexmedetomidine (used for painless endoscopies) is a highly selective α2 adrenergic agonist with sedative and analgesic properties that does not cause respiratory depression. However, it may cause bradycardia and hypotension, and it has a slow onset when used as a single sedative.Citation13,Citation14
Alfentanil has favorable pharmacological advantages for bronchoscopy, such as fast effects and recovery, providing good analgesia, minor cardiovascular effects, minimal respiratory depression, and low incidence of cough, postoperative nausea, and vomiting.Citation15 All these characteristics of alfentanil minimize the postprocedural workload. In addition, all of alfentanil’s actions can be immediately reversed by administering naloxone. As a result, alfentanil is a great choice for patients undergoing daytime surgical procedures.Citation16 The combination of alfentanil and remimazolam besylate can result in fast onset and quick recovery, and should be ideal for FB sedation. Thus, we designed this prospective, randomized controlled trial to compare the safety and efficacy of remimazolam besylate–alfentanil versus dexmedetomidine–alfentanil for FBs.
Materials and Methods
Patients
We conducted this prospective, randomized controlled trial in a tertiary center after obtaining the approval of its protocol by the Medical Ethics Committee of Liaocheng People’s Hospital (#2023045). We also registered the clinical trial in the Chinese site of clinical trial.org (ChiCTR2300070361). This trial adhered to the Helsinki Declaration and the CONSORT guidelines were also followed.
We obtained verbal and written informed consents for this trial from each patient before enrollment. Between April and September 2023, we recruited 120 Patients who were undergoing FB. The inclusion criteria comprised individuals with ages between 50 and 70 years, American Society of Anesthesiologists (ASA) grades between I and II, and oxygen saturation (SpO2) measurements > 90% (room air). We excluded individuals with asthma; severe sleep apnea syndrome (apnea–hypopnea index > 40); drugs or alcohol abuse; difficult airways;Citation17 severe cardiac, hepatic, and/or renal dysfunction; communication barriers; Amsterdam Preoperative Anxiety and Information Scale (APAIS) scores >10; history of psychiatric disorders; and those participating in other clinical trials in the preceding 3 months.
Randomization and Blinding
We randomly assigned 120 patients to one of the two groups using sealed sequentially numbered envelopes to form an RA group (remimazolam besylate combined with alfentanil) and a DA group (dexmedetomidine combined with alfentanil). A staff nurse responsible for the preparation of investigational drugs was the only person with access to the random list. The patients, anesthesiologist, and bronchoscopist were all blinded to the allocations of the trial until the end of the study.
Anesthesia
All patients fasted for 8 h for solids and 2 h for clear fluids without any pre-medication before their FB. After gaining peripheral venous access with a 20-G needle, 5 mL/kg of 0.9% sodium chloride solution was infused before sedation, and then adjusted to 5 mL/kg/h. The patients’ peripheral oxygen saturation (SpO2), electrocardiogram, noninvasive blood pressure measured at 3-minute intervals, end-tidal carbon dioxide (PetCO2), and respiratory rate (RR) were constantly monitored during the FB. Supplemental oxygen flow was administered through a nasal cannula at 3 L/min after the airway nebulization with lidocaine.Citation18
Each patient was administered 10 µg/kg of intravenous (IV) alfentanil 5 minutes before Anesthesia induction and 0.5–2 µg/kg/min during the procedure. We induced anesthesia with 6 mg/kg/h of remimazolam besylate in the RA group and 0.5 µg/kg of dexmedetomidine in the DA group for 10 minutes. Anesthesia was maintained using either remimazolam besylate at a dose of 1–2 mg/kg/h in the RA group or dexmedetomidine at a dose of 0.2–0.7 µg/kg/h in the DA group. The anesthesiologist adjusted the infusion rate of the aforementioned drugs to maintain a Modified Observer’s Assessment of Alert (MOAA/S) score <3. Propofol was the only permitted alternative sedative in this trial. All procedures were performed by the same bronchoscopist who had performed more than 800 endoscopies before participating in the trial, according to the international guidelines.Citation19 During the procedure, the bronchoscopist administered local anesthesia with 6 mL of 2% lidocaine (1 mL to the vocal cords, 2 mL to the bronchus, 1 mL to the tracheal carina, 1 mL to the right main bronchus, and 1 mL to the left main bronchus) to all patients in a spray-as-you-go fashion. Remedial lidocaine was given at the discretion of the bronchoscopist if cough interfered with the procedure, but the total dose never exceeded 5 mg/kg according to the recommendations in a previous study.Citation20 All patients were routinely transferred to the recovery room after the procedure and returned to the ward if the modified Aldrete score became ≥9.
Outcomes
The primary outcome was the lowest oxygen saturation. We also recorded the successful FB rates, demographic characteristics, hemodynamics (recorded at the following time points: T0, patient’s arrival at bronchoscopy room; T1, immediately before FB start; T2, immediately after passing the bronchoscope next to the glottis; T3, 5 min after passing next to the glottis; T4, 10 min after passing next to the glottis; T5, end of FB; T6, 5 min after FB; T7, just before the patient left the recovery room), time metrics (induction time, procedure time, fully alert time, and recovery room-leaving time), bronchoscopy feasibility (extent of coughing, vocal cords movements, and limb movements; scored 3 to 12 with 3 representing the optimal score and 12 the worst one),Citation21 study drug dose requirements, numbers of drugs used, patient and bronchoscopist satisfaction scores (5-point scales: 1, dissatisfied; 5, satisfied), instances of intraoperative awareness, number of patients willing to repeat FB with the same sedation regimen, instances and severity of adverse events (evaluated on the basis of the National Cancer Institute Common Terminology Criteria for Adverse Events 4.0).Citation22
We defined hypoxemia as an SpO2 <90% for >30 s, and we treated it with oxygen supplementation at 10 L/min, verbal, and tactile stimulation, chin lifts, jaw thrust, face mask, temporary manual ventilation, or even tracheal intubation. Bradycardia was defined as a HR < 50 beats/min lasting >30s; and, we treated it with 0.2–0.4 mg of atropine. Hypotension was defined as a mean blood pressure (MBP) decrease >20% compared with the baseline value lasting >30s, we treated it with 8 μg of noradrenaline. Hypertension was defined as an MBP increase >20% compared with the baseline value and lasting >30s; we treated it with 10–15 mg of urapidil.
Statistical Analysis
The mean and standard deviations of the lowest oxygen saturation in the DA and RA groups were 84.52±8.43% and 89.17±8.55%, respectively, according to our pilot study results. A power calculation with β = 0.8 and α = 0.05 revealed a required sample size of 54 patients in each group. Considering a 10% dropout rate for our trial, we recruited 120 patients.
We conducted statistical analyses using GraphPad Prism 9.0 and SPSS 23.0 (SPSS, Chicago, IL, USA). We confirmed the normalcy of the data using a Shapiro–Wilk test. In addition, we assessed the homogeneity of variances using Levene’s test. Continuous Outcomes were presented as means ± standard deviations or medians and interquartile ranges, and we analyzed them by performing the Student’s t or Mann–Whitney U-tests. We used repeated-measures analysis of variance to assess the feasibilities of hemodynamics and bronchoscopy. Qualitative data are presented as numbers and frequencies, and we analyzed them using χ2 or Fisher’s exact tests. We considered P < 0.05 as indicative of statistical significance.
Results
Patient Demographic Characteristics
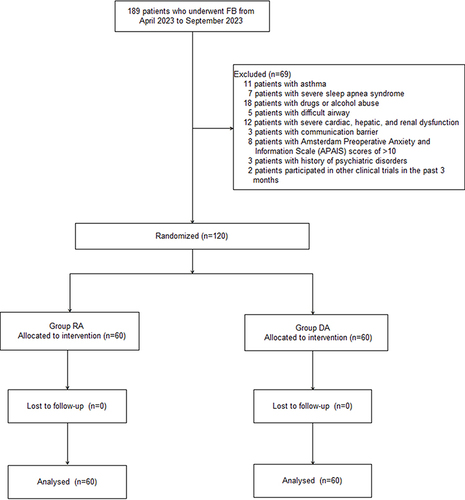
Between April and September 2023, we recruited 189 patients who underwent FB. We excluded 69 patients who presented the following criteria: asthma (n = 11); severe sleep apnea syndrome (apnea–hypopnea index >40) (n = 7); drugs or alcohol abuse (n = 18); difficult airway (n = 5); severe cardiac, hepatic, and/or renal dysfunction (n = 12); communication barriers (n = 3); Amsterdam Preoperative Anxiety and Information Scale (APAIS) scores >10 (n = 8); history of psychiatric disorders (n = 3); and participation in other clinical trials in the preceding 3 months (n = 2). As a result, we randomized 120 patients and divided them into the RA and DA groups (n = 60, each; ). We found similar patient demographic characteristics and FB indications (P > 0.05; ).
Table 1 Demographic Characteristics and Indication of FB Between the Two Groups
Figure 1 Patient flowchart with CONSORT guidelines.
Safety Outcomes
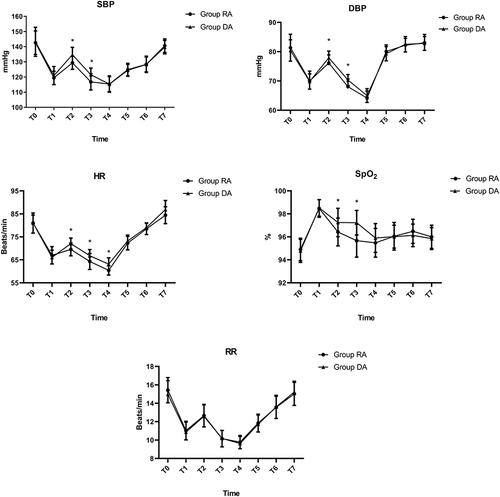
The lowest oxygen saturation during the FB procedure was significantly better in the RA group (89.2±2.5%) than in the DA group (84.9±2.6%, P = 0.001; ). Compared with patients in the DA group, the SpO2, systolic blood pressure (SBP), and diastolic blood pressure (DBP) values were significantly lower at T2 and T3 in the RA group (P < 0.05; ). Similarly, the HRs were significantly higher from T2 to T4 in the DA group (P < 0.05; ). However, the respiratory rates (RR) were similar in both groups (P > 0.05; ).
Table 2 The Safety Outcomes Between the Two Groups
Figure 2 Hemodynamic measurements. Compared with patients in the DA group, SPO2, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were significantly decreased at T2 and T3 in the RA group. Similarly, heart rate (HR) was significantly increased from T2 to T4 in the DA group. Time points are as follows: T0: arrival at bronchoscopy room, T1: immediately before start of FB, T2: immediately after entering the glottis, T3: 5 min after entering the glottis, T4: 10 min after entering the glottis, T5: end of FB, T6: 5 min after FB, T7: leaving the recovery room. *P < 0.05 vs RA group.
The incidences of hypotension, hypertension, tachycardia, and intraoperative awareness were also similar between the groups (P > 0.05; ). However, more patients experienced bradycardia in the DA group than in the RA group (P = 0.041; ). Ten patients in the RA group and 16 in the DA group experienced hypoxia and required increased oxygen delivery; among them, 4 patients in the RA group and 7 patients in the DA group also required verbal and tactile stimulation. However, we did not have to pause the procedure for any patient during this trial. No patients were recorded injection pain and postoperative cognitive impairment in this trial. Both groups presented a grade-1 severity of adverse events.
Efficacy Outcomes
Both groups presented similar rates of successful FBs, numbers of drugs used, patient and bronchoscopist satisfaction scores, and numbers of patients willing to repeat the procedure with the same sedation regimen (P > 0.05; ). Compared with patients in the DA group, those in the RA group had significantly shorter induction times (6.6±2.0 min vs 9.0±1.2 min), times to fully alert (4.4±1.3 min vs 7.0±1.5 min), and recovery room-leaving times (11.8±1.6 min vs 16.6±2.3 min; all Ps < 0.05; ). However, the procedure times were similar for both groups (22.0±3.1 min vs 22.3±3.5 min; P = 0.619; ). Compared with the bronchoscopy feasibility scores in the DA group, those in the RA group were significantly lower at T2 (P < 0.05; ). However, the T3 scores were similar in both groups (P > 0.05; ).
Table 3 The Efficacy Outcomes Between the Two Groups
Discussion
According to our Results, the RA group had a higher lowest oxygen saturation mean during FBs and shorter mean induction, fully alert, and recovery room-leaving times than the DA group. However, the procedure times were similar in both groups. Compared with patients in the DA group, the scores of bronchoscopy feasibility were significantly lower at T2 (but not at T3) in the RA group.
FBs are widely used for diagnosing and treating pulmonary diseases, but the patients’ intolerance throughout the process poses iatrogenic risks. Thus, both the British Thoracic Society guideline of 2013 and Interventional pulmonology group of the Chinese Thoracic Society guideline of 2019 have suggested that drugs providing appropriate levels of sedation and stabilizing cardiovascular and respiratory markers be given in combination during FBs to reduce patients’ pain and anxiety and minimize adverse effects, especially for procedures expected to be long and complex.Citation2,Citation3 All patients presented to the procedural room without any pre-medication because a previous study demonstrated no benefit from either routine glycopyrrolate or atropine premedication.Citation23
The advantages of preserving spontaneous breathing (with sedation) during FBs include obstruction occurrence prevention and stable hemodynamics promotion, especially for patients with a narrowed airway tract.Citation24 The amnesic and anxiolytic properties of benzodiazepines may be more beneficial for patients than the antitussive and analgesic properties of opioids.Citation25,Citation26 The addition of opioids to dexmedetomidine or benzodiazepines is also beneficial as the combinations reduce the amount of sedative and analgesic drugs needed, minimize anxiety, decrease the injection pain of sedative drugs, reduce induction times, and decrease the occurrence of nausea and vomiting. Moreover, these combinations may improve the sedation levels during bronchoscopy.Citation27 Thus, we used remimazolam besylate or dexmedetomidine–alfentanil combinations in our trial.
A propofol–fentanyl combination has been shown to be superior to a propofol–alfentanil combination for sedation-analgesia during colonoscopies. This may be due to the longer acting time of fentanyl, which improves the operation conditions.Citation28 However, the contrasting results of another study remind us to be vigilant to the respiratory depression caused by fentanyl.Citation29 Moreover, alfentanil may bind with more affinity to opioid receptors, it has a shorter effect, a small distribution volume, and displays a more rapid effect onset than fentanyl.Citation30 Due to its low incidence of respiratory obstruction, postoperative nausea, and vomiting, and its minimal impact on the respiratory and circulatory systems, alfentanil is an ideal choice over equipotent doses of fentanyl or sufentanil for spontaneous breathing during general anesthesia.Citation31 Alfentanil and remifentanil have similar effect onset times, but bolus injections of remifentanil can easily cause more serious adverse reactions such as bradycardia, hypotension, respiratory depression, nausea, bucking, and muscle rigidity, which has also been reported in our previous study.Citation32,Citation33 Moreover, alfentanil combined with propofol has been shown to achieve a satisfactory degree of sedation during bidirectional endoscopies.Citation34 We chose to use alfentanil for this trial on the basis of all of these considerations.
The incidence of respiratory depression is relatively high when alfentanil is used alone, whereas fewer instances of respiratory depression occur when propofol is used with alfentanil.Citation35 However, alfentanil (5 μg/kg) cannot be administered immediately before a propofol infusion due to hypoxemia induction risks.Citation36 Immediate injections of 5–10 µg/kg of alfentanil before the infusion of propofol or midazolam caused significant hypoxemia in another study, but the incidence of respiratory depression was significantly reduced after a 5 min interval. In addition, the study recommended using relatively high doses of sedative drugs and low doses of alfentanil for adult patients undergoing bronchoscopy.Citation37,Citation38 We used 10 µg/kg of intravenous (IV) alfentanil 5 minutes before anesthesia induction on the basis of those numbers.
Remimazolam besylate has been suggested to be suitable for application in anesthesia induction to reduce unfavorable hemodynamic responses during intubation.Citation39 We recorded SpO2, HR, SBP, and DBP values and found them all to be significantly lower at T2 and T3 in the RA group than in the DA group. Continuous infusions of remimazolam besylate have become more frequent to induce and maintain anesthesia because these infusions prevent the hemodynamic and anesthesia depth instabilities that were often recorded after intermittent boluses. Moreover, the total administered dose and the patient recovery times tend to be lower and shorter after the continuous infusion than after a bolus of remimazolam besylate.Citation40 Thus, we administered a loading dose (6 mg/kg/h of remimazolam besylate for 10 minutes) during anesthesia induction and a maintenance dose (1–2 mg/kg/h) to the patients in the group RA. The combination of remimazolam besylate with alfentanil has been shown to better preserve the patient’s spontaneous breathing and reduce the incidence of respiratory depression than propofol during FBs.Citation41 However, to the best of our knowledge, the safety and efficacy of remimazolam besylate–alfentanil versus dexmedetomidine–alfentanil had not been compared before this trial.
The combination of dexmedetomidine and alfentanil was shown to result in more instances of respiratory depression than dexmedetomidine alone, but the quality of sedation and the extent of coughing were similar between both regimens.Citation42 In patients undergoing endoscopy, single-use alfentanil causes less damage to postoperative cognitive function, less risk of hypotension, and shorter discharge time than dexmedetomidine.Citation25 A previous study reported a lower lowest oxygen saturation in the RA group compared to the value in the DA group, albeit with a non-statistically significant difference. This may be due to the effects of alfentanil on the respiratory center of the brainstem, especially when opioids are associated with benzodiazepines.Citation43 By contrast, our results showed that the lowest oxygen saturation during the FB (usually during anesthesia induction) was significantly higher in the RA group than in the DA group. However, we did not record significant differences between the two groups regarding RRs. This may be due to differences in monitoring methods, drug combinations, ventilation modes (manually ventilated via laryngeal mask vs spontaneous ventilation with nasal cannula), and discrimination criteria.Citation44
In a finding similar to those of others, more patients experienced bradycardia in the DA group than in the RA group in our trial. According to the British Thoracic Society guidelines, PETCO2 monitoring is most useful for patients with high risk of CO2 retention; however, we found no patients with respiratory depression. Hypertension and tachycardia are common during bronchoscopy and may lead to cardiac ischemia. The prophylactic addition of a β adrenergic antagonist may prevent this response. However, we did not adopt this strategy because the incidences of these two adverse reactions in our initial trial were significantly lower than those in a published study,Citation45 probably due to sedation protocol differences.
According to the results of previous research, we did not find patients reporting injection pain in the RA group, probably due to the water-soluble characteristics of remimazolam besylate and off-target interactions with transient receptor potential receptors on sensory neurons.Citation46 Consistent with the research results of previous study, Our findings on the induction, fully alert, and recovery room-leaving times were consistent with those of others showing all significantly shorter times in the RA group than in the DA group. In addition, the bronchoscopy feasibility scores were higher in the DA group than on the RA group. This may be due to the longer onset and half-life of dexmedetomidine compared to those of remimazolam besylate.Citation47 The rapid recovery of the cognitive function is important for a growing number of people who hope to minimize off-work time immediately after endoscopic procedures. Both remimazolam besylate and dexmedetomidine exert little negative effects on cognitive functions.Citation14,Citation48 Accordingly, we did not find any patients with postoperative cognitive impairment in this trial. Also, in agreement with others’ results, we did not find differences in the number of patients willing to repeat the FB with the same sedation regimen, or in patient satisfaction scores. Patients’ wishes and satisfaction scores may be associated with numerous influencing factors like organization, endoscopy unit facilities, and waiting times.Citation49
This trial had the following limitations: First, our patients all came from one hospital; therefore, a large-sample multicenter study is needed to confirm the conclusions of our trial. Second, we included only subjective indicators of the patient sedation level, a choice that may have biased our results. Accurate objective indicators such as the integrated pulmonary index (IPI) may be more accurate for assessing the patient’s level of sedation. Third, a ceiling effect on synergistic sedation with midazolam and alfentanil may exist in adult patients.Citation50 Further research is needed to explore whether the same phenomenon exists with remimazolam besylate and alfentanil. Finally, to reduce statistical bias refer to the age distribution of patients who have received FBs in the past at our center and reduce the statistical bias, we only recruited patients aged 50 to 70 years undergoing short FBs. As a result, we did not record any related complications outside of the respiratory and circulatory systems. These results cannot be extended to elderly patients undergoing lengthy procedures, who may require deeper sedation during bronchoscopy.
In conclusion, remimazolam besylate is superior to dexmedetomidine when combined with alfentanil during FB, promoting faster patients’ recovery, better operative conditions, and respiratory stability, while the occurrence and severity of adverse events is similar.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the privacy policy but are available from the corresponding authors upon reasonable request.
Ethics Approval and Informed Consent
All procedures performed on the patients were in accordance with the tenets of the 1964 Declaration of Helsinki and its later amendments. The study was approved by the institutional review boards of Liaocheng People’s Hospitals.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Funding
References
- Gerretsen ECF, Chen A, Annema JT, et al. Effectiveness of flexible bronchoscopy simulation-based training: a systematic review. Chest. 2023;164(4):952–962. doi:10.1016/j.chest.2023.05.012
- Du Rand IA, Blaikley J, Booton R, et al. Summary of the British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults. Thorax. 2013;68(8):786–787. doi:10.1136/thoraxjnl-2013-203629
- Interventional pulmonology group of the Chinese Thoracic Society, Chinese Medical Association. [Guideline for diagnostic flexible bronchoscopy in adults (2019)]. Zhonghua Jie He He Hu Xi Za Zhi. 2019;42(8):573–590. Chinese. doi:10.3760/cma.j.issn.1001-0939.2019.08.005
- Zhong J, Zhang J, Fan Y, et al. Efficacy and safety of Ciprofol for procedural sedation and anesthesia in non-operating room settings. J Clin Anesth. 2023;85:111047. doi:10.1016/j.jclinane.2022.111047
- Akulian J, Wahidi M, Shojaee S, et al. Safety and efficacy of remimazolam compared with placebo and midazolam for moderate sedation during bronchoscopy. Chest. 2019;155(1):137–146. doi:10.1016/j.chest.2018.09.015
- Zha B, Wu Z, Xie P, et al. Supraglottic jet oxygenation and ventilation reduces desaturation during bronchoscopy under moderate to deep sedation with propofol and remifentanil: a randomised controlled clinical trial. Eur J Anaesthesiol. 2021;38(3):294–301. doi:10.1097/EJA.0000000000001401
- Wu B, Zhu W, Wang Q, et al. Efficacy and safety of ciprofol-remifentanil versus propofol-remifentanil during fiberoptic bronchoscopy: a prospective, randomized, double-blind, non-inferiority trial. Front Pharmacol. 2022;13:1091579. doi:10.3389/fphar.2022.1091579
- Pastis NJ, Yarmus LB, Schippers F, et al. Safety and efficacy of remimazolam compared with placebo and midazolam for moderate sedation during bronchoscopy. Chest. 2019;155(1):137–146.
- Domínguez-Rodríguez A, Suero-Mendez C, Burillo-Putze G, et al. Midazolam versus morphine in acute cardiogenic pulmonary oedema: results of a multicentre, open-label, randomized controlled trial. Eur J Heart Fail. 2022;24(10):1953–1962. doi:10.1002/ejhf.2602
- Liou JY, Ting CK, Teng WN, et al. Adaptation of non-linear mixed amount with zero amount response surface model for analysis of concentration-dependent synergism and safety with midazolam, alfentanil, and propofol sedation. Br J Anaesth. 2018;120(6):1209–1218. doi:10.1016/j.bja.2018.01.041
- Kilpatrick GJ. Remimazolam: non-clinical and clinical profile of a new sedative/anesthetic agent. Front Pharmacol. 2021;12:690875. doi:10.3389/fphar.2021.690875
- Ye E, Wu K, Ye H, et al. Comparison of 95% effective dose of remimazolam besylate and propofol for gastroscopy sedation on older patients: a single-centre randomized controlled trial. Br J Clin Pharmacol. 2023;89(11):3401–3410. doi:10.1111/bcp.15839
- Albrecht E, Capel D, Rossel JB, et al. A randomised controlled trial of intravenous dexmedetomidine added to dexamethasone for arthroscopic rotator cuff repair and duration of interscalene block. Anaesthesia. 2023;78(3):315–319. doi:10.1111/anae.15942
- Dokpolo LU, Mastriano DJ, Serafin J, et al. Discharge readiness after propofol with or without dexmedetomidine for colonoscopy: a randomized controlled trial. Anesthesiology. 2019;131(2):279–286. doi:10.1097/ALN.0000000000002809
- Dong SA, Guo Y, Liu SS, et al. A randomized, controlled clinical trial comparing remimazolam to propofol when combined with alfentanil for sedation during ERCP procedures. J Clin Anesth. 2023;86:111077. doi:10.1016/j.jclinane.2023.111077
- Li H, Zhang H, Cheng Z, et al. Effects of alfentanil hydrochloride on cough and hemodynamics during induction of general anesthesia in daytime surgery. Minerva Surg. 2023;78(6):730–732. doi:10.23736/S2724-5691.21.09341-2
- Cailleau L, Geeraerts T, Minville V, et al. Is there a benefit for anesthesiologists of adding difficult airway scenarios for learning fiberoptic intubation skills using virtual reality training? A randomized controlled study. PLoS One. 2023;18(1):e0281016. doi:10.1371/journal.pone.0281016
- Madan K, Biswal SK, Mittal S, et al. 1% Versus 2% lignocaine for airway anesthesia in flexible bronchoscopy without lignocaine nebulization (LIFE): a randomized controlled trial. J Bronchology Interv Pulmonol. 2018;25(2):103–110. doi:10.1097/LBR.0000000000000458
- Strohleit D, Galetin T, Kosse N, et al. Guidelines on analgosedation, monitoring, and recovery time for flexible bronchoscopy: a systematic review. BMC Pulm Med. 2021;21(1):198. doi:10.1186/s12890-021-01532-4
- Yüksel H, Yaşar A, Açıkel A, et al. Two different methods of lidocaine inhalation before diagnostic flexible bronchoscopy: effects on post-bronchoscopy respiratory symptoms. Turk J Med Sci. 2021;51(4):2101–2106. doi:10.3906/sag-2012-130
- Chen N, Wang X, Chen L, et al. Estimation of the median effective dose and the 95% effective dose of alfentanil required to inhibit the bronchoscopy reaction during painless bronchoscopy with i-gel supraglottic airway device: an up-and-down sequential allocation trial. J Thorac Dis. 2022;14(5):1537–1543. doi:10.21037/jtd-22-412
- Drake R, Prael G, Phyo Y, et al. Gabapentin for pain in pediatric palliative care. J Pain Symptom Manage. 2023;S0885-S3924(23):00784.
- Malik JA, Gupta D, Agarwal AN, et al. Anticholinergic premedication for flexible bronchoscopy: a randomized, double-blind, placebo-controlled study of atropine and glycopyrrolate. Chest. 2009;136(2):347–354. doi:10.1378/chest.08-2924
- Zhu H, Sun Y, Wang T, et al. Alfentanil and propofol induced anesthesia for patients with huge endotracheal tumor undergoing fiberoptic bronchoscopic interventional therapy: case report. Transl Cancer Res. 2022;11(8):2946–2952. doi:10.21037/tcr-22-199
- Houghton CM, Raghuram A, Sullivan PJ, et al. Pre-medication for bronchoscopy: a randomised double blind trial comparing alfentanil with midazolam. Respir Med. 2004;98(11):1102–1107. doi:10.1016/j.rmed.2004.03.023
- Zhong Y, Jiang M, Wang Y, et al. Evaluating efficacy and safety of sub-anesthetic dose esketamine as an adjuvant to propofol/remifentanil analgosedation and spontaneous respiration for children flexible fibreoptic bronchoscopy: a prospective, double-blinded, randomized, and placebo-controlled clinical trial. Front Pharmacol. 2023;14:1184663. doi:10.3389/fphar.2023.1184663
- Tschiedel E, Eckerland M, Felderhoff-Mueser U, et al. Sedation for bronchoscopy in children: a prospective randomized double-blinded trial. Pediatr Pulmonol. 2021;56(5):1221–1229. doi:10.1002/ppul.25235
- Türk HŞ, Aydoğmuş M, Unsal O, et al. Sedation-analgesia in elective colonoscopy: propofol-fentanyl versus propofol-alfentanil. Braz J Anesthesiol. 2013;63(4):352–357. doi:10.1016/j.bjan.2012.07.006
- van Dam CJ, Algera MH, Olofsen E, et al. Opioid utility function: methods and implications. Ann Palliat Med. 2020;9(2):528–536. doi:10.21037/apm.2019.10.09
- Ford S. Alfentanil-based TIVA during remifentanil shortages: a need for guidance. Anaesthesia. 2023;78(2):259–260. doi:10.1111/anae.15837
- Sridharan K, Sivaramakrishnan G. Comparison of fentanyl, remifentanil, sufentanil and alfentanil in combination with propofol for general anesthesia: a systematic review and meta-analysis of randomized controlled trials. Curr Clin Pharmacol. 2019;14(2):116–124. doi:10.2174/1567201816666190313160438
- Chen X, Xin D, Xu G, Zhao J, Lv Q. The efficacy and safety of remimazolam tosilate versus dexmedetomidine in outpatients undergoing flexible bronchoscopy: a prospective, randomized, blind, non-inferiority trial. Front Pharmacol. 2022;13:902065. doi:10.3389/fphar.2022.902065
- Xin Z, Wang N, Wang H. Remimazolam and remifentanil use induced severe respiratory depression and laryngeal spasm during intravenous sedation and analgesia: a case report. Curr Drug Saf. 2024;19(2):277–281. doi:10.2174/1574886318666230517101142
- Zhang J, Liu R, Bi R, et al. Comparison of ciprofol-alfentanil and propofol-alfentanil sedation during bidirectional endoscopy: a prospective, double-blind, randomised, controlled trial. Dig Liver Dis. 2023;S1590-S8658(23):00960.
- Schult AL, Botteri E, Hoff G, et al. Women require routine opioids to prevent painful colonoscopies: a randomised controlled trial. Scand J Gastroenterol. 2021;56(12):1480–1489. doi:10.1080/00365521.2021.1969683
- Hsieh CH, Lin TY, Wang TY, et al. The safety and efficacy of alfentanil-based induction in bronchoscopy sedation: a randomized, double-blind, controlled trial. Medicine. 2016;95(43):e5101. doi:10.1097/MD.0000000000005101
- Wang LL, Guan ZY, Wang CM, et al. A comparative study on the efficacy and safety of propofol combined with different doses of alfentanil in gastroscopy: a randomized controlled trial. J Anesth. 2023;37(2):201–209. doi:10.1007/s00540-022-03145-5
- Wang L, Wu Q, Wang M, et al. Gender differences in the effective dose of alfentanil in painless bronchoscopy. J Thorac Dis. 2023;15(1):216–218. doi:10.21037/jtd-22-1460
- Xu Q, Wu J, Shan W, et al. Effects of remimazolam combined with sufentanil on hemodynamics during anesthetic induction in elderly patients with mild hypertension undergoing orthopedic surgery of the lower limbs: a randomized controlled trial. BMC Anesthesiol. 2023;23(1):311. doi:10.1186/s12871-023-02249-z
- Sheng XY, Liang Y, Yang XY, et al. Safety, pharmacokinetic and pharmacodynamic properties of single ascending dose and continuous infusion of remimazolam besylate in healthy Chinese volunteers. Eur J Clin Pharmacol. 2020;76(3):383–391. doi:10.1007/s00228-019-02800-3
- Zhang L, Yu L, Xu L, et al. Effectiveness of remimazolam besylate combined with alfentanil for fiberoptic bronchoscopy with preserved spontaneous breathing: a prospective, randomized, controlled clinical trial. Eur Rev Med Pharmacol Sci. 2023;27(13):6071–6080. doi:10.26355/eurrev_202307_32961
- Akhondzadeh R, Olapour A, Rashidi M, et al. Comparison of sedation with dexmedetomidine alfentanil versus ketamine-alfentanil in patients undergoing closed reduction of nasal fractures. Anesth Pain Med. 2020;10(4):e102946. doi:10.5812/aapm.102946
- Riachy M, Khayat G, Ibrahim I, et al. A randomized double-blind controlled trial comparing three sedation regimens during flexible bronchoscopy: dexmedetomidine, alfentanil and lidocaine. Clin Respir J. 2018;12(4):1407–1415. doi:10.1111/crj.12669
- Öztürk MC, Küçük M, Uğur YL, et al. The safety of fiberoptic bronchoscopy in airway pressure release ventilation mode in critically ill patients with severe acute respiratory distress syndrome: a preliminary study. Turk Thorac J. 2022;23(6):403–408. doi:10.5152/TurkThoracJ.2022.21241
- Bi Y, Ma Y, Ni J, et al. Efficacy of premedication with intranasal dexmedetomidine for removal of inhaled foreign bodies in children by flexible fiberoptic bronchoscopy: a randomized, double-blind, placebo-controlled clinical trial. BMC Anesthesiol. 2019;19(1):219. doi:10.1186/s12871-019-0892-6
- Shi W, Cheng Y, He H, et al. Efficacy and safety of the remimazolam-alfentanil combination for sedation during gastroscopy: a randomized, double-blind, single-center controlled trial. Clin Ther. 2022;44(11):1506–1518. doi:10.1016/j.clinthera.2022.09.014
- Deng Y, Qin Z, Wu Q, et al. Efficacy and safety of remimazolam besylate versus dexmedetomidine for sedation in non-intubated older patients with agitated delirium after orthopedic surgery: a randomized controlled trial. Drug Des Devel Ther. 2022;16:2439–2451. doi:10.2147/DDDT.S373772
- Yang M, Liu X, Yang D, et al. Effect of remimazolam besylate compared with propofol on the incidence of delirium after cardiac surgery: study protocol for a randomized trial. Trials. 2021;22(1):717. doi:10.1186/s13063-021-05691-x
- Chartier L, Arthurs E, Sewitch MJ. Patient satisfaction with colonoscopy: a literature review and pilot study. Can J Gastroenterol. 2009;23(3):203–209. doi:10.1155/2009/903545
- Wang L, Wu Q, Wang M, et al. The safety and efficacy of alfentanil combined with midazolam in fiberoptic bronchoscopy sedation: a randomized, double-blind, controlled trial. Front Pharmacol. 2022;13:1036840. doi:10.3389/fphar.2022.1036840