
Abstract
Background
The novel short-acting benzodiazepine drug, remimazolam tosilate, has been employed for sedation during endoscopic procedures. The optimal loading dosage of remimazolam tosilate in gastroscopy for elderly patients when co-administered with fentanyl remains unclear. Therefore, the primary objective of our research was to ascertain the median effective dose (ED50) and the 95% effective dose (ED95) of remimazolam tosilate in combination with various fentanyl dosages for elderly patients undergoing painless gastroscopy.
Methods
Seventy-five patients aged ≥65 years and American Society of Anesthesiologists (ASA) class I–III were recruited to undergo elective painless gastroscopy. All patients were randomized assigned to group F1, group F2, and group F3, and were injected intravenously with different doses of fentanyl (0.5 ug/kg, 1 ug/kg, and 1.5 ug/kg) 3 minutes prior to the administration of remimazolam tosilate, respectively. The initial preset dose of remimazolam tosilate was 0.3 mg/kg in group F1, 0.2 mg/kg in group F2, 0.15 mg/kg in group F3. The dose gradient was 0.02 mg/kg per group according to the up-and-down sequential method. Probibt regression model was employed to determine the ED50 and ED95 of remimazolam tosilate.
Results
The ED50 of remimazolam tosilate in group F3 was lower than that in group F1 and F2 (0.095 [0.088–0.108] mg/kg vs 0.162 [0.153–0.171] mg/kg; 0.258 [0.249–0.266] mg/kg, p < 0.05). The ED95 of remimazolam tosilate was 0.272 mg/kg (95% CI: 0.264–0.295 mg/kg) in group F1, 0.175 mg/kg (95% CI: 0.167–0.200 mg/kg) in group F2 and 0.109 mg/kg (95% CI: 0.101–0.135 mg/kg) in group F3. The total dosage of remimazolam tosilate decreased gradually with the increasing of fentanyl (p < 0.001). The frequency of injection pain was higher in group F1 compared to groups F2 and F3 (p < 0.05). The patients in group F3 had a lower incidence of hypotension than in groups F1 and F2 (p < 0.05). There was no respiratory depression, intraoperative consciousness, dizziness or delirium in the three groups.
Conclusion
The concurrent use of fentanyl reduces the dosage of remimazolam tosilate required for sedative gastroscopy in elderly patients in a dose-dependent manner. Moreover, 1.5 ug/kg fentanyl combined with remimazolam tosilate may reduce the incidence of hypotension and injection pain. These findings should be confirmed in a large-scale study.
Introduction
The use of gastrointestinal endoscopy is considered the gold standard for both diagnosing and treating upper gastrointestinal diseases.Citation1 The number of elderly adults undergoing gastroscopy is increasing yearly due to the aging population and advancements in gastrointestinal endoscopy technology.Citation2 Procedural sedation during gastroscopy can elleviate patients’pain, anxiety, vomit, and discomfort.Citation3 Although procedural sedation is considered safe in the majority of patients, elderly patients who receive procedural sedation have an increased risk of respiratory depression,Citation4 hemodynamic instability,Citation5 arrhythmias,Citation6 and delayed dischargeCitation7 due to the use of certain sedative agents, such as propofol. Therefore, it is crucial for clinicians to select safe and efficient medications for gastroscopy in elderly patients. However, the use of sedative medications in elderly patients during gastroscopy remains controversial.
The newly developed remimazolam tosilate is a short-acting agonist of the gamma-aminobutyric acid A (GABAA) receptor, which effectively inhibits neuronal electrical activity by binding to GABA receptors and induces sedation.Citation8,Citation9 It is rapidly hydrolyzed by hepatic esterases to inactive carboxylic acid metabolites.Citation10 In comparison to conventional benzodiazepine sedative medications, remimazolam tosilate has a quicker onset and elimination, milder respiratory and circulatory depression, and fewer adverse effects.Citation11–13 The safety and efficacy of remimazolam tosilate as a medication for procedural sedation in elderly patients have been demonstrated by several studies.Citation14–16 Borkett et al found that a single administration of remimazolam tosilate given at 0.1–0.2 mg/kg has a high sedation success rate with minimal effects on breathing and circulation during upper gastrointestinal endoscopy. However, the procedure success rate have ranged from 32% to 64%.Citation17 In clinical practice, we also found that the above dose of remimazolam tosilate may be insufficient for achieving adequate sedation in certain patients during gastroscopy, with a higher incidence of cough, hiccup, body movement, which could potentially be attributed to the weak inhibitory effect of remimazolam tosilate on the stress response. Although increasing the dose of remimazolam tosilate can improve the depth of sedation and suppress the stress response, it has a significant inhibitory effect on the patient’s circulatory system, prolonging the time to awaken and leave the hospital. So, for gastroscopy sedation, drug combinations may be preferable to single-drug regimen.Citation18 Hu et al demonstrated that a combination of 0.1 ug/kg sufentanil and 0.2 mg/kg remimazolam tosilate effectively provided sufficient sedation for elderly patients undergoing gastroscopy.Citation19 Guo et al also revealed that 5 ug/kg alfentanil in combination with 0.15 mg/kg remimazolam tosilate can be safely and effectively used for sedation during gastrointestinal endoscopy in elderly patients,Citation20 which may be attributed to the fact that opioids provide better analgesia and reduce the amount of intraoperative sedative medication.Citation21,Citation22 However, the ED50 of remimazolam tosilate combined with different doses of fentanyl in elderly patients for painless gastroscopy has not been completely evaluated. Therefore, the objective of this study was to ascertain the optimal and efficacious dosage of remimazolam tosilate in combination with varying doses of fentanyl for painless gastroscopy in elderly patients.
Materials and Methods
Ethics Approval
The study received approval from the Ethics Committee of Affiliated Hospital of North Sichuan Medical College, Nanchong, China (Approval No. 2023ER368-1) and was registered on the Chinese Clinical Trials Registry at http://www.chictr.org.cn (ChiCTR2300077778). The study was commenced after obtaining written informed consent from all participants.
Study Population
The study recruited a total of 75 patients aged ≥ 65 years, who met the American Society of Anesthesiologists (ASA) physical status I-III, for painless gastroscopy from November 2023 to January 2024.
The exclusion criteria were as follows: patients who declined to sign written informed consent; uncontrolled severe hypertension; experienced significant cardiorespiratory instability, including acute heart failure, myocardial infarction, acute respiratory infection; patients who had a history of alcohol abuse or dependence on opioids or benzodiazepines; Additionally, patients who had a documented allergy or medical contraindication to benzodiazepines or opioids.
Randomization and Blinding
75 patients were randomised into three groups: group F1 with a dose of 0.5ug/kg fentanyl, group F2 with a dose of 1 ug/kg fentanyl and group F3 with a dose of 1.5ug/kg fentanyl. The randomization process was conducted utilizing a computer-generated randomized sequence. The study medication was prepared on the day of endoscopy by an independent anaesthesia nurse according to the randomization sequence. Prior to gastroscopy, the fentanyl dose for each patient was diluted to 5 mL with 0.9% saline using the same syringe. Different doses of remimazolam tosilate were diluted to 20 mL with 0.9% saline in identical syringes. All patients, endoscopist, and other investigators were masked to group allocation.
Anaesthesia
All patients underwent an 8-hour fasting period and were prohibited from consuming water for two hours prior to the procedure. In the operating room, all patients were positioned on the left side with lower limb flexion. Peripheral venous access was established in the left upper limb. Vital signs, including blood pressure, heart rate and pulse oxygen saturation (SpO2) were monitored, and oxygen was supplied via the nasal catheter at a flow rate of 5 L/min before giving intravenous drugs. Fentanyl was given intravenously. After about three minutes following the administration of fentanyl, remimazolam tosilate was injected slowly within 1 min. Gastroscopy was inserted after the patient lost consciousness (Modified Observer’s Assessment of Alertness/Sedation Scale, MOAA/S score ≦1). The patient’s level of sedation was evaluated using the MOAA/S score (score 5: prompt response to the spoken name in a normal tone; score 4: sluggish response to the spoken name in a normal tone; score 3: responds only after the name is called loudly and/or repeatedly; score 2: responds only after mild prodding or shaking; score 1: responds only after experiencing painful trapezius squeeze; score of 0: no response even after painful trapezius squeeze). Remimazolam tosilate 3 mg administered intravenously for therapeutic sedation if the patient presented out coughing, swallowing, retching, frowning, body movement during gastroscopy. After the procedures, patients with MOAA/S score ≧ 4 were sent to the recovery room for observation, and were accompanied by their family members to leave the hospital after the Modified Aldrete score ≧ 9.Citation23 The definition of perioperative hypotension was SBP below 90 mmHg or Mean arterial pressure (MAP) decreased by more than 20% of the baseline value, and ephedrine 6 mg was administered. Bradycardia was defined if heart rate (HR) below 50 beats/min, and atropine 0.3 mg was given. The lower jaw was elevated if hypoxemia (SpO2 < 95%) occurred. If the SpO2 did not increase or continued to fall below 90%, mask-assisted ventilation was carried out.
Determination of the ED50 for Remimazolam Tosilate
The median effective dose of remimazolam tosilate, when combined with different doses of fentanyl for each group, was determined utilizing the up-and-down sequential methodology. The initial dosage of remimazolam tosilate (0.3 mg/kg in group F1, 0.2 mg/kg in group F2, 0.15 mg/kg in group F3) was determined by the pretest data. The subsequent patient’s dose of remimazolam tosilate would be increased by 0.02 mg/kg if the previous patient exhibited a positive response to gastroscopy placement. The subsequent patient’s remimazolam tosilate dose would be reduced by 0.02 mg/kg if the previous patient exhibited a negative response to gastroscopy placement. Positive response to gastroscopy placement was defined as the patient presenting out coughing, swallowing, retching, frowning, body movement. The absence of the above behavior was considered a negative reaction. A cross-over point was defined as a situation where there is a switch from a positive response to a negative response, or vice versa, in consecutive patients. When six cross-over points were obtained in each group, we considered that the sample size for this study was adequate.
Secondary Data Collection
We monitored SBP, diastolic blood pressure (DBP), SPO2, HR and MAP at the following time points: before the administration of fentanyl (T0), insertion of the endoscope into the pharyngeal cavity (T1), withdrawal of the endoscope from the pharyngeal cavity (T2), the time of awakening from anesthesia (T3), the time away from the recovery room (T4). The procedure time, consciousness recovery time, length of recovery room stay, and adverse effects, including injection pain, hypotension, bradycardia, respiratory depression, were documented. In the postanesthesia care unit, intraoperative awareness, postoperative dizziness, postoperative delirium and postoperative nausea and vomiting, were assessed and documented.
Statistical Analysis
Statistical analysis was conducted using SPSS 25.0 software. The Shapiro–Wilk test was utilized to assess the normality of the data. The continuous distributed variables were reported as mean ± standard deviation(SD) or median (25th to 75th percentiles), where appropriate, and were analyzed using one-way ANOVA or the non-parametric Kruskal–Wallis H-test. The categorical data were quantified as numerical values (expressed as percentages) and subjected to analysis using the chi-square test.
Comparisons between groups were made using the Bonferroni test. P < 0.05 was considered statistically significant. Probit probability unit regression analysis was employed to determine ED50, ED95 and the 95% confidence interval (CI) of remimazolam tosilate. The comparison of ED50 for each group used by relative median intensity.
Results
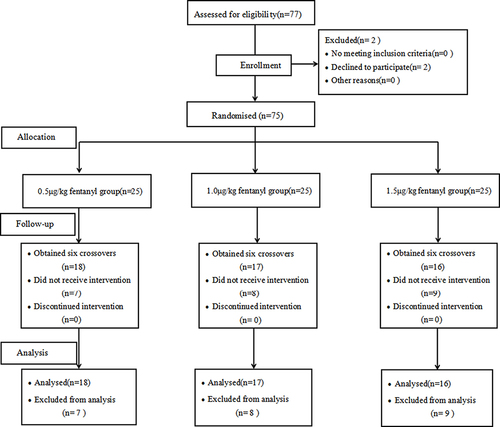
The study recruited a total of 75 patients, with each group consisting of 25 patients. 7, 8, 9 patients in groups F1, F2 and F3 were excluded from the study because six crossover points were achieved in each group (). The study was completed by 18, 17, and 16 patients in groups F1, F2, and F3 respectively. The demographic characteristics did not show any significant differences among the three groups ().
Table 1 Demographic Characteristics for Three Groups
Figure 1 CONSORT flow diagram.
The sequential doses of remimazolam tosilate in combination with fentanyl using up-and-down sequential method are illustrated in . The ED50 and ED95 of remimazolam tosilate is 0.258 mg/kg (95% CI: 0.249–0.266 mg/kg) and 0.272 mg/kg (95% CI: 0.264–0.295 mg/kg) in group F1, 0.162 mg/kg (95% CI: 0.153–0.171 mg/kg) and 0.175 mg/kg (95% CI: 0.167–0.200 mg/kg) in group F2, 0.095 mg/kg (95% CI: 0.088–0.108 mg/ kg) and 0.109 mg/kg (95% CI: 0.101–0.135 mg/kg) in group F3 ().
Figure 2 Individual response to the stimulus of gastroscopy placement in the study groups. Positive response to gastroscopy placement are marked with ●, and negative reaction to gastroscopy placement are marked with ○. The doses of fentanyl in group F1 were 0.5ug/kg (A), in group F2 were 1.0ug/kg (B), in group F3 were 1.5 μg/kg (C), respectively. To get six crossovers, 18, 17 and 16 patients were included individually in groups F1, F2, F3.
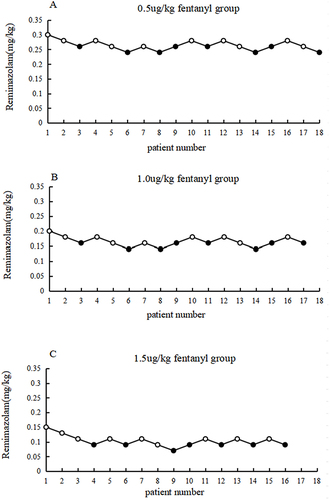
Table 2 ED50 and ED95 of Remimazolam Tosilate and Its 95% CI for the Three Groups
The SBP, DBP, MAP, and HR values did not exhibit any statistically differences among the three groups at various time points (). The total dosage of remimazolam tosilate demonstrated a significant negative correlation with the dosage of fentanyl (p < 0.001). The incidence of injection pain was significantly higher in patients in group F1 than in groups F2 and F3. No statistically difference between groups F2 and F3. There was no statistically difference in the incidence of hypotension between patients in groups F1 and F2. While patients in group F3 had a considerably lower incidence of hypotension than in groups F1 and F2. The three groups did not differ in duration of gastroscopy, time of consciousness recovery, length of recovery room stay, incidence of hiccup. No respiratory depression, intraoperative awareness, postoperative nausea and vomiting, postoperative dizziness, or delirium was observed in either group ().
Table 3 SBP, DBP, HR, SPO2 at Different Time Points for Three Groups
Table 4 Intraoperative and Postoperative Data
Discussion
In our study, we found that the ED50 of remimazolam tosilate in combination with fentanyl are 0.258 mg/kg (with a dosage of 0.5 ug/kg fentanyl) and 0.162 mg/kg (with a dosage of 1.0 ug/kg fentanyl), 0.095 mg/kg (with a dosage of 1.5 ug/kg fentanyl), respectively. The administration of intravenous fentanyl results in a dose-dependent decrease in the ED50 of remimazolam tosilate undergoing painless gastroscopy in elderly patients. It is suggested that fentanyl and remimazolam tosilate have a strong synergistic effect, and this synergistic effect can reduce the dose of sedatives and the risk of hypotension and injection pain, consistent with Kops study.Citation24 Tan et al found that when combined with a dosage of 0.1ug/kg sufentanil, the ED50 of remimazolam besylate in the procedural sedation was 0.196 mg/kg during endoscopic retrograde cholangiopancreatography (ERCP).Citation25 These results are larger than the ED50 of remimazolam tosilate combined with 1 ug/kg fentanyl in our study, which may be attributed the milder stimulation of gastroscopy compared with ERCP.Citation26 Another reason is that elderly patients exhibit heightened sensitivity to sedative drugs and opioids.Citation27 Cao et al observed that ED50 of remimazolam tosilate was 0.097 mg/kg in combination with 0.15 ug/kg sufentanil for sedation in patients aged from 18–65 years old undergoing oesophagogastric varices screening endoscopy with liver cirrhosis.Citation28 The results are similar to our study. However, considering the potential impact of both age and liver function on drug sensitivity. Future studies will focus on investigating the optimal dosage of remimazolam tosilate in combination with opioids for painless gastroscopy in elderly patients with cirrhosis.
There are 27.7% patients in the F1 group who experienced injection pain. The injection pain of remimazolam tosilate was significantly reduced compared with propofol,Citation29 which can be attributed to the water-solubility of remimazolam tosilate, and consequently, there is less injection pain than fat-soluble agents. However, the mechanism of injection pain caused by remimazolam tosilate in our study remains unclear and needs further study. Fortunately, we also found that the administration of 1 ug/kg or 1.5 ug/kg fentanyl significantly reduced the occurrence of injection pain, which may be due to the appropriate dose of opioid preconditioningCitation30 and lower doses of remimazolam tosilate.Citation27 The incidence of hypotension gradually decreased with increasing doses of fentanyl in our study, which may be attributed to a reduction in remimazolam tosilate doses. Dai et al have shown that the hypotension incidence increased with higher doses of remimazolam tosilate.Citation31
Our investigation demonstrated that the rates of intraoperative hiccups were 33.3% in group F1, 23.5% in group F2, and 18.7% in group F3. The incidence of hiccups showed a decreasing trend although there was no clinical significance among three groups. According to Liu et al, midazolam was also found to be strongly linked to an increased risk of hiccups.Citation32 Additionally, they discovered that individuals who were given 2 mg of midazolam experienced hiccups more frequently than those who were given 1 mg. Davis et al thought that the hiccups may be due to the effect of benzodiazepines on the supraspinal hiccup centers located in the brainstem.Citation33 Another factor causing benzodiazepines-induced hiccups could be a direct stimulation of the diaphragm contractility.Citation34 In our study, complications such as reflux aspiration and gastric injury did not increase in patients with hiccups during gastroscopy, nor did they affect the doctor’s operation of gastroscopy. However, according to Vanner’s study, about 40% of patients with hiccups after induction of anesthesia have detectable gastroesophageal reflux.Citation35 So, in future study, we will focus on how to prevent or inhibit the adverse reactions of remimazolam tosilate - induced hiccups.
The present study has several potential limitations. Firstly, we utilize the MOAA/S score as a means of assessing the level of sedation depth in all patients. However, due to the absence of objective monitoring techniques such as bispectral indices or narcotrend, this approach may introduce potential biases into the evaluation process of sedation. Secondly, our study only includes elderly patients with a normal BMI, thus limiting the generalizability of our findings to other patients. Thirdly, this study is a single-center design and small sample size. Therefore, the subsequent trials necessitate a larger sample size and multi-centre studies to further investigate the adverse effects and recovery time of different dose of fentanyl in combination with varying appropriate doses of remimazolam tosilate in painless gastroscopy for elderly patients.
Conclusion
The administration of fentanyl results in a dose-dependent reduction in the ED50 of remimazolam tosilate undergoing painless gastroscopy in elderly patients. Moreover, the administration of 1.5 ug/kg fentanyl resulted in a reduction in the occurrence of hypotension and injection pain.
Abbreviations
ED50, median effective dose; ED95, the 95% effective dose; ASA, American Society of Anesthesiologists; GABAA, gamma-aminobutyric acid A; SpO2, pulse oxygen saturation; MOAA/S score, Modified Observer’s Assessment of Alertness/Sedation Scale; SBP, Systolic blood pressure; DBP, diastolic blood pressure; MAP, Mean arterial pressure; HR, heart rate; ERCP, endoscopic retrograde cholangiopancreatography; SD, standard deviation; CI, confidence interval.
Ethics Approval and Informed Consent
The study was approved by the Institutional Ethics Committee of the Affiliated Hospital of North Sichuan Medical College, China (Approved No. 2023ER368-1) and was registered on the Chinese Clinical Trials. gov (No. ChiCTR2300077778). All participants provided their written informed consent. We confirm our study complies with the Declaration of Helsinki.
Disclosure
All authors declare that they have no conflicts of interest in this work.
Acknowledgments
Yanxia Guo and Zhihua Yao are co-first authors for this study. We would like to thank Dr. Yalan Li for her technical guidance.
Data Sharing Statement
The data supporting the study findings are available from the corresponding author upon request.
References
- Travis AC, Pievsky D, Saltzman JR. Endoscopy in the elderly. Am J Gastroenterol. 2012;107(10):1495–501 quiz 4.
- Shen XC, Ao X, Cao Y, et al. Etomidate-remifentanil is more suitable for monitored anesthesia Care during gastroscopy in older patients than propofol-remifentanil. Med Sci Monit. 2015;1(21):1–8. doi:10.12659/MSM.891183
- Liu F, Cheng XY, Wang YJ, et al. Effect of remimazolam tosilate on the incidence of hypoxemia in elderly patients undergoing gastrointestinal endoscopy: a bi-center, prospective, randomized controlled study. Front Pharmacol. 2023;18(14):1131391. doi:10.3389/fphar.2023.1131391
- Wang SL, Shen N, Wang YL, et al. Bilevel positive airway pressure for gastroscopy with sedation in patients at risk of hypoxemia: a prospective randomized controlled study. J Clin Anesth. 2023;85:111042. doi:10.1016/j.jclinane.2022.111042
- Wu XY, Wang CH, Gao H, et al. Comparison of remimazolam and propofol about safety outcome indicators during general anesthesia in surgical patients: a systematic review and meta-analysis. Minerva Anestesiol. 2023;89(6):553–564. doi:10.23736/S0375-9393.23.17034-9
- Chang Y, Huang YT, Chi KU, et al. Remimazolam versus propofol for procedural sedation: a meta-analysis of randomized controlled trials. PeerJ. 2023;12(11):e15495. doi:10.7717/peerj.15495
- Liu XW, Ding BF, Shi F, et al. The efficacy and safety of remimazolam tosilate versus etomidate-propofol in elderly outpatients undergoing colonoscopy: a prospective, randomized, single-blind, non-inferiority trial. Drug Des Devel Ther. 2021;16(15):4675–4685. doi:10.2147/DDDT.S339535
- Keam SJ. Remimazolam: first approval. Drugs. 2020;80(6):625–633. doi:10.1007/s40265-020-01299-8
- Lee A, Shirley M. Remimazolam: a Review in Procedural Sedation. Drugs. 2021;81(10):1193–1201. doi:10.1007/s40265-021-01544-8
- Sheng XY, Liang Y, Yang XY, et al. Safety, pharmacokinetic and pharmacodynamic properties of single ascending dose and continuous infusion of remimazolam besylate in healthy Chinese volunteers. Eur J Clin Pharmacol. 2020;76(3):383–391. doi:10.1007/s00228-019-02800-3
- Chen S, Wang J, Xu X, et al. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, Phase III clinical trial. Am J Transl Res. 2020;12(8):4594–4603.
- Sneyd JR, Gambus PL, Rigby-Jones AE. Current status of perioperative hypnotics, role of benzodiazepines, and the case for remimazolam: a narrative review. Br J Anaesth. 2021;127(1):41–55. doi:10.1016/j.bja.2021.03.028
- Chen X, Sang N, Song K, et al. Psychomotor recovery following remimazolam-induced sedation and the effectiveness of flumazenil as an antidote. Clin Ther. 2020;42(4):614–624. doi:10.1016/j.clinthera.2020.02.006
- Tan YJ, Wen OY. Effect of remimazolam tosilate on early cognitive function in elderly patients undergoing upper gastrointestinal endoscopy. J Gastroenterol Hepatol. 2022;37(3):576–583. doi:10.1111/jgh.15761
- Liu M, Sun Y, Zhou LX, et al. The median effective dose and bispectral index of remimazolam tosilate for anesthesia induction in elderly patients: an up-and-down sequential allocation trial. Clin Interv Aging. 2022;20(17):837–843. doi:10.2147/CIA.S364222
- Chen JJ, Zou XH, Hu BL, et al. Remimazolam vs etomidate: haemodynamic effects in hypertensive elderly patients undergoing non-cardiac surgery. Drug Des Devel Ther. 2023;27(17):2943–2953. doi:10.2147/DDDT.S425590
- Borkett KM, Riff DS, Schwartz HI, et al. A Phase IIa, randomized, double-blind study of remimazolam (CNS 7056) versus midazolam for sedation in upper gastrointestinal endoscopy. Anesth Analg. 2015;120(4):771–780. doi:10.1213/ANE.0000000000000548
- Wang P, Chen Y, Guo Y, et al. Comparison of propofol-nalbuphine and propofol-fentanyl sedation for patients undergoing endoscopic retrograde cholangiopancreatography: a double-blind, randomized controlled trial. BMC Anesthesiol. 2022;22(1):47. doi:10.1186/s12871-022-01578-9
- Hu BL, Jiang K, Shi WY, et al. Effect of remimazolam tosilate on respiratory depression in elderly patients undergoing gastroscopy: a multicentered, prospective, and randomized study. Drug Des Devel Ther. 2022;5(16):4151–4159. doi:10.2147/DDDT.S391147
- Guo J, Qian YT, Zhang XJ, et al. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: a prospective, randomized and controlled study. BMC Anesthesiol. 2022;22(1):180. doi:10.1186/s12871-022-01713-6
- Zhou ZY, Zhao YL, Yang XL, et al. Effects of different remifentanil target concentrations on MACBAR of sevoflurane in gynaecological patients with CO2 pneumoperitoneum stimulus. Br J Anaesth. 2015;114(4):634–639. doi:10.1093/bja/aeu400
- Albertin A, Casati A, Bergonzi P, et al. Effects of two target-controlled concentrations (1 and 3 ng/mL) of remifentanil on MAC(BAR) of sevoflurane. Anesthesiology. 2004;100(2):255–259. doi:10.1097/00000542-200402000-00012
- Yamaguchi D, Morisaki T, Sakata Y, et al. Usefulness of discharge standards in outpatients undergoing sedative endoscopy: a propensity score-matched study of the modified post-anesthetic discharge scoring system and the modified Aldrete score. BMC Gastroenterol. 2022;22(1):445. doi:10.1186/s12876-022-02549-7
- Wang CY, Gao YZ, Li J, et al. Safety and effectiveness of the combination of remimazolam tosilate and propofol in gastroscopy: a multicenter, randomized controlled, single-blind clinical trial. Front Pharmacol. 2023;31(14):1124667. doi:10.3389/fphar.2023.1124667
- Tan DD, Gu J, Li J, et al. The effective doses of remimazolam besylate in the procedural sedation of endoscopic retrograde cholangiopancreatography. Ibrain. 2022;9(3):290–297. doi:10.1002/ibra.12072
- Haytural C, Aydınlı B, Demir B, et al. Comparison of propofol, propofol–remifentanil, and propofol–fentanyl administrations with each other used for the sedation of patients to undergo ERCP. BioMed Res Int. 2015;2015:1‐5.
- Zhao TYM, Chen D, Sun H, et al. Moderate sedation with single-dose remimazolam tosilate in elderly male patients undergoing transurethral resection of the prostate with spinal anesthesia: a prospective, single-arm, single-centre clinical trial. BMC Anesthesiol. 2022;22(1):247. doi:10.1186/s12871-022-01788-1
- Cao YH, Chi P, Zhou Z, et al. The 50% and 95% effective doses of remimazolam tosilate with adjuvant sufentanil for sedation in patients with liver cirrhosis undergoing oesophagogastric varices screening Endoscopy. J Clin Pharm Ther. 2022;47(12):2068–2073. doi:10.1111/jcpt.13751
- Jalota L, Kalira V, George E, et al. Prevention of pain on injection of propofol: systematic review and meta-analysis. BMJ. 2011;15(342):d1110. doi:10.1136/bmj.d1110
- Lee SH, Lee SE, Chung SY, et al. Impact of time interval between remifentanil and propofol on propofol injection pain. J Clin Anesth. 2016;34:510–515. doi:10.1016/j.jclinane.2016.06.029
- Dai G, Pei L, Duan F, et al. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021;87(10):1073–1079. doi:10.23736/S0375-9393.21.15517-8
- Liu CC, Lu CY, Fang CJ, et al. Sedation-associated hiccups in adults undergoing gastrointestinal endoscopy and colonoscopy. World J Gastroenterol. 2012;18(27):3595–3601. doi:10.3748/wjg.v18.i27.3595
- Davis JN. An experimental study of hiccup. Brain. 1970;93(4):851–872. doi:10.1093/brain/93.4.851
- Aldrich TK, Prezant DJ. Adverse effects of drugs on the respiratory muscles. Clin Chest Med. 1990;11(1):177–189.
- Vanner RG. Gastro-oesophageal reflux and hiccup during Anaesthesia. Anaesthesia. 1993;48(1):92–93. doi:10.1111/j.1365-2044