Abstract
Sildenafil is an orally administered phosphodiesterase type 5 inhibitor that is approved for the treatment of pulmonary arterial hypertension (PAH). The hemodynamic effects of sildenafil are mitigated primarily via potentiating the effects of endogenous nitric oxide, leading to smooth muscle cell relaxation and reductions in pulmonary arterial pressures and pulmonary vascular resistance. When added to standard background therapy in patients with idiopathic or associated PAH from congenital heart disease, anorexigen use, or connective tissue disease, sildenafil treatment results in improved exercise capacity as measured by 6 minute walk distance, improved hemodynamics, and favorable changes in quality of life. Sildenafil use is contraindicated with concomitant nitrate administration, and caution should be exercised when used in combination with antihypertensive agents due to risks of precipitating hypotension. Side effects are generally mild, and include flushing, headaches, and epistaxis. The combination of sildenafil with intravenous epoprostenol is safe and well tolerated, and further improves exercise capacity. Sildenafil is approved only for treatment of PAH, and although emerging data suggest a potential role in treating other types of pulmonary hypertension, larger trials are required to confirm these findings.
Introduction
Pulmonary arterial hypertension (PAH) is a life-threatening disorder characterized by progressive remodeling of the pulmonary vasculature, leading to a rise in pulmonary arterial pressures and pulmonary vascular resistance that often culminates in right ventricular (RV) failure. Despite regional variations in disease epidemiology, a recent European registry estimates the prevalence PAH at approximately 15.0 cases/million.Citation1 Worldwide, prevalence of PAH is likely to rise, given increased awareness among physicians, salutatory effects of treatment, increased use of amphetamine stimulants, recognition of schistosomiasis as a common etiologic agent in certain regions, and greater appreciation for the role of hemoglobinopathies in PAH.Citation2 Prior to the widespread use of disease-specific pharmacotherapy, mortality was high, with a median survival of 50% at 2.8 years.Citation3 Although few randomized trials have been designed to assess survival, observational data suggest improved outcome in the pharmacotherapy era, with 2-year survival estimated at 89%.Citation4
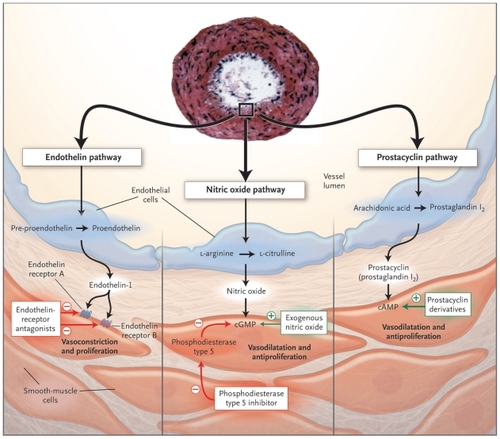
Treatment of PAH has evolved dramatically over the past 15 years. Prior to 1996, treatment was focused upon symptom control which included management of RV failure with diuretics and digoxin, supplemental oxygen therapy to correct hypoxemia, and judicious use of calcium channel blockers. The recognition that PAH progression was characterized by vascular remodeling and an imbalance between proliferative and anti-inflammatory mediators led to the identification of the importance of endothelin, prostacyclin, and nitric oxide (NO) in disease initiation and progression (). These key pathways currently serve as targets for disease-specific treatment modalities that have revolutionized PAH management, by improving functional capacity, hemodynamics, and patient well being.Citation5 In PAH, the ideal pharmacologic agents should facilitate vasorelaxation and restoration of the balance between apoptosis and cellular proliferation, ultimately preserving RV function and delaying the onset of right heart failure.Citation6
Figure 1 Cellular mechanisms of sildenafil actions.
Reproduced with permission from Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004;351:1425–1436.Citation68 Copyright © 2004 Massachusetts Medical Society. All rights reserved.
Sildenafil, an orally administered a phosphodiesterase type 5 (PDE-5) inhibitor, targets the NO pathway. The drug was first approved for the treatment of erectile dysfunction in 1998, and approved for treatment of PAH in 2005.Citation7,Citation8 This review will summarize the mechanisms behind the therapeutic efficacy of sildenafil, review the role for sildenafil in the treatment of PAH, and highlight emerging roles for sildenafil in heart failure and other cardiopulmonary conditions.
Sildenafil background and mechanisms of action
The effects of sildenafil in treating both erectile dysfunction and PAH are accomplished by enhancing the downstream effects of NO mediated vasorelaxation (). NO is a labile gas produced by NO synthases located in the vascular endothelial and airway epithelial cells that freely diffuses across capillary membranes. On a cellular level, NO stimulates conversion of guanosine triphosphate (GTP) to cyclic guanosine monophosphate (cGMP). Intracellular cGMP has multiple effects on cellular physiology mediated by activation of protein kinases, specifically regulation of ion channels and alteration of intracellular cyclic nucleotide concentrations.Citation9 From a physiological standpoint, NO stimulates dilatation of vascular smooth muscle at both the arterial and venous levels. Antiproliferative effects of NO have been well described.Citation10,Citation11 The importance of NO in PAH is magnified because PAH is intrinsically associated with reduced endogenous NO production. The ability to maintain NO production in the setting of hypoxia may play a role in delaying the onset of pulmonary hypertension (PH).Citation12,Citation13
Figure 2 Endothelial cell.
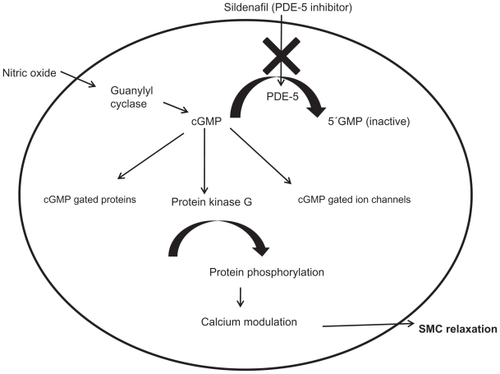
Reduced levels of cGMP have deleterious effects, leading to altered calcium handling and subsequent vasoconstriction and smooth muscle cell proliferation.Citation6,Citation14 cGMP levels are regulated by PDE enzymes. Currently, 11 different families of PDE isoenzymes have been identified, which vary in substrate selectivity, tissue location, and mechanism of action (). PDE-5 has been the focus for PAH because the PDE-5 enzyme is highly expressed in lung tissue compared to other vascular beds, with minimal expression in the systemic circulation.Citation15,Citation16 PDE-5 expression is upregulated in PAH, leading to increased metabolism of NO-derived cGMP. For these reasons, inhibition of PDE-5 was hypothesized to serve as a viable target to enhance NO-mediated physiologic effects.Citation17 The utility of PDE-5 inhibition in PAH was first demonstrated in 1991, when investigators successfully used the PDE-5 inhibitor zaprinast to mitigate alveolar induced hypoxia.Citation18 Sildenafil, the first commercially available oral PDE-5 inhibitor, was studied in 2001 and demonstrated to prevent development of PH in hypoxic mouse models.Citation19
Table 1 Phosphodiesterase isoenzymes
Targeting of the NO pathway with exogenous oral nitrates is limited by the rapid development of tachyphylaxis.Citation20 Treatment with PDE-5 inhibitors indirectly modulates the NO pathway by acting on a downstream site, thereby obviating this problem.
Additional pleotropic mechanisms may contribute to the beneficial effects of sildenafil in PAH. Antioxidant properties have been described in other tissue beds.Citation21,Citation22 Controversy exists about the presence of a direct RV inotropic effect of sildenafil. The hypertrophied RV demonstrates increased tissue expression of PDE-5.Citation23 In healthy individuals, PDE-5 is expressed in the coronary arteries, but is not typically found in cardiac myocytes. One study comparing sildenafil to inhaled NO (iNO) demonstrated comparable reductions in PA pressures and pulmonary vascular resistance (PVR), but increased cardiac index (CI) was seen only with sildenafil treatment, consistent with an inotropic effect.Citation24 However, other investigators, examining load-independent measures of myocardial performance, found no changes in systolic or diastolic function with sildenafil treatment.Citation25 Circulating endothelial progenitor cells are reduced in idiopathic PAH and congenital PAH, and treatment with sildenafil has been shown to increase these cells to levels consistently higher than other PAH therapies.Citation26 Sildenafil also inhibits PDE-1, which is expressed in low levels in the pulmonary circulation under baseline conditions but is upregulated in the disease state.Citation27 The clinical significance of these findings remains uncertain. Ultimately, modulation of cGMP leads to improved calcium handling and restoration of the balance between apoptosis and smooth cell proliferation, resulting in vascular reverse remodeling.
Drug pharmacokinetics and interactions
Maximum plasma concentrations of sildenafil dosed at the Food and Drug Administration (FDA) approved schedule of 20 mg 3 times daily are achieved 1 hour after administration, with a half-life of approximately 4 hours. Bioavailability is approximately 40%, which is reduced to 29% following a large meal.Citation28 In the elderly (age >65 years) the clearance of sildenafil is impaired, with increased drug half-life and maximum serum concentrations.Citation29 The pharmacokinetics of sildenafil are not altered in the setting of mild to moderate renal insufficiency. Although serum levels can rise in severe impairment, dosing changes are usually not required.Citation29 Similarly, in patients with Child’s A or B cirrhosis, despite increased drug levels, dose adjustments are rarely necessary.Citation29
Sildenafil is metabolized primarily by the hepatic cytochrome P450 (CYP) 3A4 enzymes and to a lesser extent by CYP2C9 enzymes. The primary metabolite, N- desmethylsildenafil, maintains PDE-5 specificity, but with reduced potency, and plasma levels approaching 40% of primary compound.Citation28 Careful monitoring is advisable with coadministration with CYP3A4 inducers (carbamazepine, phenytoin, nevirapine), as sildenafil dose increases may be necessary. Bosentan is an inducer of the CYP3A4 pathway, and the use of these drugs in combination will be discussed later in this review. Sildenafil is currently listed by the FDA as a category B drug in pregnancy.Citation30 There are only small case series examining drug safety in pregnancy, and caution is advised in this regard.Citation31
Drug side effects
Review of the pivotal SUPER 1 study demonstrate that the most frequent placebo subtracted side effects were epistaxis (8%), headache (7%), and flushing (6%).Citation8 There was a dose-dependent increase in the incidence of drug-related side effects, including flushing, headache, and blurry vision. No significant laboratory abnormalities were identified. Retinal hemorrhage occurred more commonly in the sildenafil-treated group (1.4% vs 0%), but most patients who developed this condition were taking oral anticoagulants. Because of a shared and common pathway of increased NO-mediated effects, concomitant administration with oral nitrate medications can potentiate the effects of either agent, and their use together is contraindicated.Citation32 Administration of sildenafil to patients taking nitrate medications can produce dramatic reductions in blood pressure (systolic blood pressure drop in excess of 50 mmHg) and syncope.Citation33 Sildenafil should not be administered to patients who have taken any oral or sublingual preparation within the previous 24 hours. While larger doses of sildenafil have been associated with significant reduction in systolic blood pressure approaching 10 mmHg, the FDA-approved dose of 20 mg by mouth 3 times daily has not been shown to significantly affect blood pressure.Citation34 Blurry vision has been described at higher doses, primarily due to minor inhibition of PDE-6 located in the eyes.
Nonarteritic anterior ischemic optic neuropathy (NAION) is a common cause of acute optic neuropathy in the elderly. Anecdotal reports and cases series suggested increased risks of NAION in sildenafil-treated patients. However, pooled data from clinical trials of all three commercially available PDE-5 inhibitors (sildenafil, tadalafil, vardenafil) suggested no increased risk of NAION.Citation35 Patients at highest risk for development of NAION are those who have previously suffered NAION in one eye, and those with other risk factors for vascular disease, including diabetes mellitus. Although these findings are reassuring to health care providers, it remains advisable to monitor for visual changes, and to seek prompt medical attention for sudden vision loss. Uncommon drug effects, including a case report of thrombocytopenia, have been described.Citation36
Clinical trial experience
The first case report demonstrating a clinical benefit of sildenafil in PAH was published in 2000.Citation37 Earlier work had suggested utility of sildenafil in other cardiopulmonary conditions, including weaning mechanically ventilated patients with iNO-dependent respiratory failure.Citation38 Building on this promising early experience, single-center studies were completed that suggested significant clinical efficacy and both functional and hemodynamic improvement in PAH.Citation39 Taken together these studies suggested that sildenafil, in a dose-dependent manner, had durable and sustained pulmonary vasodilator effects.
The SUPER-1 trial (Sildenafil Use in PUlmonary hypertension) commenced enrollment in 2002, and randomized patients with PAH to treatment with either sildenafil (20 mg, 40 mg, 80 mg) 3 times daily or placebo.Citation8 The primary endpoint in this study, similar to most PAH trials, was assessing exercise capacity as measured by changes in 6 minute walk distance (6MWD) at 12 weeks. Secondary endpoints included changes in invasive hemodynamic parameters, BORG dyspnea score, clinical worsening, and health related quality of life (QoL). The study was restricted to patients with idiopathic PAH, and acquired PAH from connective tissue disease (CTD), congenital heart disease (CHD), or previous anorixegen use, and composed of patients with moderate disease severity (), who were predominantly World Health Organization (WHO) functional class II (39%) and III (58%), and had a mean 6MWD of 344 m. The mean age of patients included in the study was 49 years, and approximately three-fourths of patients were female.
Table 2 WHO functional classification of pulmonary hypertension
After 12 weeks, the mean placebo corrected increase in 6MWD was 45 m. A trend towards improved exercise capacity was detected as early as 4 weeks. Sildenafil treatment was associated with a statistically significant number of patients who improved by at least one functional class (21%, P = 0.003). There were no significant differences between the sildenafil- and placebo-treated groups in BORG dyspnea score, or the incidence of clinical worsening, defined as a combined endpoint of death, lung transplantation, hospitalization for PAH or need to institute combination therapy.
Patients who completed the study were eligible to enroll in an extension study, where doses were uptitrated to 80 mg by mouth 3 times daily. The results of the extension study have not yet been published. Subgroup analysis from the SUPER-1 study in 84 patients with CTD demonstrated that the drug was equally safe and efficacious this patient population. Citation40 Analysis of QoL measures demonstrated that treatment with sildenafil significantly improved physical functioning, and general health, vitality, and well-being.
Based primarily upon the results of SUPER-1 study, in 2005, sildenafil was approved for the treatment of PAH in both the United States and Europe at the 20 mg 3 times daily dose. Although there were no differences in 6MWD between the three doses during the pivotal trial period, dose-dependent changes in hemodynamic parameters, particularly mean pulmonary arterial pressure (mPAP) and PVR, were identified. Additional small studies have suggested safety and efficacy of higher doses of sildenafil, but obtaining insurance approval for these higher doses remains challenging.Citation41
Clinical use of sildenafil
Sildenafil is indicated in patients with mild to moderate pulmonary hypertension (WHO FC II–III).Citation42 There are no data to support treatment in asymptomatic individuals, and the drug should not be used as a first-line agent in markedly symptomatic patients (WHO FC IV, 6MWD <100 m). When considering initiating treatment with sildenafil, the physician must carefully examine the existing medication list, monitor for drugs that may potentiate an interaction (alpha-blockers, nitrates) and assess for systemic hypotension that may worsen with treatment.
Currently, sildenafil is one of nine FDA-approved pharmacologic therapies for PAH. These include treatments involving continuous infusions, using hand-held inhaled devices, and pills. Before choosing an agent, several factors should be assessed, including disease severity, existing comorbidities, patient compliance, family support, and drug side effects–interactions. Regardless of chosen pharmacotherapy, regular follow up, and surveillance for disease progression and development of RV failure are critical in disease management.
There are very few head to head trials comparing different agents. One small study comparing high dose sildenafil (dose titration to 50 mg 3 times daily) to bosentan dosed at 125 mg by mouth twice daily, demonstrated no significant change in the primary endpoint (RV mass), or secondary endpoints, including 6MWD and B-type natriuretic peptide levels.Citation43 In patient with WHO FC II–III disease, most experts recommend initial therapy with an oral agent with careful follow up for disease progression.Citation42 These recommendations stem primarily from the efficacy of the oral agents, coupled with desire to avoid potential infectious complications with continuous infusion therapy and the cumbersome nature of inhaled therapy, which requires 4 to 9 treatments daily. An advantage of PDE-5 inhibitor over the endothelin receptor antagonists ambrisentan and bosentan, is that therapy with PDE-5 inhibitors does not require safety monitoring with monthly liver function tests.
Sildenafil in other acquired PAH
Smaller studies have been completed in patients who were not eligible for the larger scale phase III clinical trials. Patients with end-stage liver disease are susceptible to development of portopulmonary hypertension, which, if untreated, is a contraindication for liver transplantation. While epoprostenol has long been the gold standard for treatment of portopulmonary hypertension, smaller studies suggest that in milder cases, sildenafil treatment can be safely used as a bridge to liver transplantation.Citation44
Combination therapy
The rational for combination therapy stems from using different classes of medications target the disease from multiple mechanisms. As a general rule, efficacy should be maximized, while minimizing drug toxicity. Despite the number of agents available, limited published data are available to guide decision making in this regard. Given the costs associated with PAH therapy and potential for drug interactions and side effects, caution is advised when attempting combination therapy. The largest clinical trial evaluating combination therapy studied adding sildenafil, at doses ranging from 40 mg 3 times daily to 80 mg 3 times daily, to patients on stable doses of intravenous epoprostenol.Citation45 The study included 267 patients with predominantly idiopathic PAH (79%), and those with WHO FC II (26%) and WHO FC III (66%) symptoms. Addition of sildenafil was associated with a significant placebo-adjusted increase in 6MWD of 26 m (P = 0.0009) and increased time to clinical worsening. Hemodynamic improvements were noted with addition of sildenafil, including a reduction in mPAP of 3.9 mm mg (P = 0.00003). Health-related QoL was improved with sildenafil treatment, despite no significant changes in the Borg dyspnea score.
A few small single center studies have reported safety in adding sildenafil in combination with inhaled iloprost. The study with the longest follow up evaluated patients who experienced clinical worsening after treatment with iloprost. Fourteen patients were randomized to treatment with sildenafil or placebo, and the sildenafil-treated group experienced significant and durable improvements in 6MWD.Citation46 The timing for introduction of a second agent remains unresolved. Based upon available literature, most therapies require 12 to 16 weeks for a maximal response. Additional improvements in exercise capacity as measured by 6MWD have not been demonstrated in nonblinded extension studies of the pivotal drug trials. Whether to initiate combination therapy prior to clinical deterioration in monotherapy, or earlier on in the course of disease, has not been established.
Coadministration of bosentan (a hepatic enzyme inducer) and sildenafil reduces plasma levels of sildenafil and increases bosentan concentrations, though the clinical significance of this remains uncertain.Citation47 As described earlier, bosentan induces expression of CYP2C9 and CYP3A4, which are involved with metabolism of sildenafil, and can decrease the pharmaceutical area under the curve by approximately 55%.Citation47 To determine if any clinically relevant interaction existed, the COMPASS I study investigated the acute hemodynamic effects of sildenafil addition to patients on long-term bosentan therapy.Citation48 Sildenafil administration reduced PVR by 15%, comparable to that seen with sildenafil montherapy in treatment-naïve patients. Despite the pharmacokinetic interaction between the agents, most experts believe that alterations in treatment effects of either drug are not apparent with the combination, and dose adjustment are usually not required. There are no clinically relevant interactions between ambrisentan and sildenafil.Citation49
Broad treatment guidelines apply to all patients with PAH. Hypoxemia is a potent pulmonary vasoconstrictor, and it is advisable for oxygen to be administered to maintain saturations above 90%. Right heart failure and symptoms of congestion are common, and therapy with diuretics is often required to maintain an optimal volume state. Calcium channel blocker use should be restricted to patients with WHO FC I–III patients with idiopathic PAH who demonstrate a positive response to a vasodilator challenge at the time of right heart catheterization. A positive response is defined as a decline in the mean pulmonary artery pressure of >10 mmHg and to a level less than 40 mmHg, with an unchanged or improved cardiac index. Oral digoxin has not been studied in a controlled fashion, but in patients with advanced disease exhibiting signs and symptoms of RV failure, or those with atrial tachyarrhythmias who may not tolerate beta blockers, therapy with digoxin may be beneficial. In patients with IPAH, anticoagulation with coumadin is recommended in absence of contraindications.
Costs of PAH therapy
Society is becoming increasingly aware of the costs of health care. Of the nine FDA-approved therapies, only epoprostenol is available in the generic from. Compared to drugs routinely used to treat common cardiopulmonary conditions (hypertension, dyslipidemia, obstructive lung disease) PAH pharmacotherapy is considerably more costly. Uninsured or underinsured patients will be unable to afford the costs of PAH pharmacotherapy in the absence of other financial support. It is therefore incumbent upon the physician to perform a thorough diagnostic evaluation to confirm the diagnosis of PAH, and exclude more common conditions, including obstructive lung disease, obstructive sleep apnea, and pulmonary venous hypertension from systolic or diastolic dysfunction. A recent study examined the costs of PAH pharmacotherapy. The investigators obtained cost information from US medicare and medicaid data, and utilizing a Markov-type model, determined that in medically comparable patients, treatment with sildenafil was less costly and associated with a net increase in quality adjusted life-years. Citation50 In insured patients who have adequate prescription drug coverage, we feel that the factors described previously, and not the cost of therapy, should drive decisions on pharmacotherapy.
Other PDE-5 inhibitors
Tadalafil is an orally administered PDE-5 inhibitor currently approved for treatment erectile dysfunction and PAH. A 16-week randomized, placebo-controlled study comparing tadalafil at doses ranging from 2.5 mg to 40 mg to placebo in patients with PAH was recently published.Citation51 Similar to the SUPER-1 Study, the primary endpoint in this trial was change in functional capacity as estimated by 6MWD. The mean placebo-corrected improvement in 6MWD was 33 m. When patients on background therapy with bosentan were removed, and only PAH treatment-naïve patients analyzed, the treatment effect was 44 m, comparable to that noted with sildenafil in the SUPER-1 study. Additionally, the drug improved QoL, and was associated with comparable improvements in hemodynamic patterns. Tadalafil levels are reduced with coadministration with bosentan,Citation52 and the FDA-approved dose of tadalafil is 40 mg daily. Vardenafil is a commercially available PDE-5 inhibitor used for the treatment of erectile dysfunction that is not FDA approved for the treatment of PAH.
Non-WHO group-1 pulmonary hypertension
Multiple conditions result in development of pulmonary hypertension, but are not characterized as PAH (). Phase III clinical trials have excluded these patients, and therefore, sildenafil is not FDA approved for treatment in these conditions. Smaller studies have suggested potential utility in several populations. In patients with chronic thromboembolic pulmonary hypertension (CTEPH), where anatomy is not favorable for surgical pulmonary arterial thromboendarterectomy, a potential beneficial effect to long-term sildenafil treatment has been suggested.Citation53 Sildenafil may have a useful role in management of post-heart transplant RV dysfunction and to expedite weaning from inotropes.Citation54 A small single-center study investigated high-dose sildenafil treatment in patients with pulmonary sarcoidosis (WHO Group V PH) where sildenafil treatment was associated with reductions in PA pressures, PVR, and improved cardiac index, but no change in 6MWD.Citation55 In chronic obstructive pulmonary disease, single-dose treatment with sildenafil has been shown to reduce PA pressure, irrespective of baseline, but have no impact on cardiac output, stroke volume, or exercise capacity.Citation56 In patients at high altitudes who are continuously exposed to hypoxic conditions, sildenafil has demonstrated beneficial effects in reducing PA pressures.Citation57 In one study of patients with pulmonary fibrosis, sildenafil usage at 50 mg daily reduced pulmonary vascular resistance, improved V/Q mismatch, and increased partial pressure of oxygen.Citation58 In patients with systemic sclerosis, sildenafil treatment in patient with refractory Raynaud’s with digital ulcers was associated with reduced frequency and duration of Raynaud’s attacks, and improved capillary flow.Citation59 Despite these promising initial data, larger clinical trials, with better delineation of the target populations and study endpoints, are warranted. Given the costs, unproven benefits, and potential side effects of therapy, it is generally not advisable to use sildenafil for conditions other than WHO Group I PH.
Table 3 WHO classification of pulmonary hypertension
Sildenafil in heart failure
The most common cause of right heart failure is longstanding left heart failure and development of pulmonary venous hypertension. Over time, if left untreated, some patients can develop structural changes in the pulmonary arteries with resultant increase in pulmonary vascular resistance.Citation60 Sildenafil has been shown to be well tolerated among severe end-stage heart failure patients undergoing transplant evaluation and as an acute screening agent for fixed pulmonary hypertension that would otherwise be a contraindication to heart transplantation.Citation61 Impaired NO generation and utilization contributes to the abnormal cardiovascular phenotype in congestive heart failure. Based upon these observations, sildenafil is receiving increasing attention from the heart failure community.
From a historical perspective, PDE inhibitors were used with great caution in heart failure, because the PDE-3 inhibitor milrinone, which increases myocellular cyclic adenosine monophosphate (cAMP) levels, is associated with increased mortality in heart failure.Citation62 However, sildenafil, through its high specificity for PDE-5, is believed to be far safer in this regard. From a safety standpoint, sildenafil has been studied in doses ranging from 25 to 100 mg in patients with erectile dysfunction and heart failure and appears to be safe and well tolerated.Citation61
Melonovsky et al studied the acute hemodynamic effects of sildenafil administration in heart failure.Citation63 Following dosing with 40 mg sildenafil, reductions in PVR and improvements in PA compliance were noted. Increased intracellular levels of cGMP were reported, suggesting that PDE5 inhibition restores sensitivity of pulmonary vascular to endogenous cGMP-dependent vasodilators. Additional studies of patients with heart failure and pulmonary hypertension demonstrated that sildenafil treatment was associated with improved ventilator efficiency, as determined by Ve/VCO2 slope by cardiopulmonary stress testing, and correlated with drops in pulmonary vascular resistance and improvement in RV ejection fraction.Citation64 Sildenafil may improve RV systolic function in patients with heart failure complicated by PH.Citation64 A small, placebo-controlled randomized study in congestive heart failure patients demonstrated that 4 weeks of sildenafil administration improved functional capacity, ventilator efficiency, and pulmonary hypertension.Citation65 In stable heart failure patients, sildenafil treatment improves mVO2 max and improves endothelial function as measured by brachial artery flow-mediated dilation, suggesting endothelium-mediated attenuation of exercising muscle oversignaling.Citation66 Nitrates are commonly used in heart failure, and are contraindicated with sildenafil administration. However, a small study demonstrated safety and efficacy of combing nitrates with sildenafil to further reduce PA pressures in advanced heart failure.Citation67 Taken together, the experience of sildenafil in heart failure appears promising and provocative, and a potential novel application.
Conclusions
Sildenafil has emerged as a safe and efficacious pharmacotherapy for PAH. Longer-term studies, examining the effects of therapy on disease remodeling overall survival have yet to be completed. Combination therapy is an exciting development in the treatment of PAH. A favorable side effect profile and acceptable dosing regimen make sildenafil an attractive option for combination therapy, and studies are underway examining multiple drug combinations. By enhancing downstream effects of NO, there is potential for sildenafil to have utility in treating various conditions with endothelial dysfunction and regional alterations in blood flow.
Disclosures
Gautam Ramani has served as a consultant to United Therapeutics, Actelion, and Gilead. Myung Park has served as a consultant to United Therapeutics, Actelion, Gilead and Pfizer.
References
- HumbertMSibtonOChaoutAPulmonary arterial hypertension in France: Results from a national registryAm J Respir Crit Care Med20061731023102616456139
- ButrousGGhofraniHAGrimmingerFPulmonary vascular diseases in the developing worldCirculation20081181758176618936338
- D’AlonzoGEBarstRJAyresSMSurvival in patients with primary pulmonary hypertension: results from a national prospective registryAnn Intern Med19911153433491863023
- McLaughlinVVSibtonOBadeschDBSurvival with first-line bosentan in patients with primary pulmonary hypertensionEur Respir J200525244249 Erratum in Eur Respir J. 2005;25:94215684287
- MichelakisEDWilkinsMRRabinovitchMEmerging concepts and translational priorities in pulmonary arterial hypertensionCirculation20081181486149518824655
- ArcherSLMichelakisEDPhosphodiesterase type 5 Inhibitors for pulmonary arterial hypertensionN Engl J Med20093611864186119890129
- GoldsteinILueTFPadma-NathanHOral sildenafil in the treatment of erectile dysfunctionN Engl J Med1998338139714049580646
- GalieNSildenafil citrate therapy for pulmonary arterial hypertensionN Engl J Med20053532148215716291984
- LucasKAPitariGMKazerounianSGuanyl cyclases and signaling by cyclic GMPPharmacol Rev20005237541310977868
- MoncadaSPalmerRMHiggsEANitric oxide: physiology, pathophysiology and pharmacologyPharmacol Rev1991431091421852778
- TantiniBManesAFiumanaEAntiproliferative effect of sildenafil on human pulmonary artery smooth muscle cellsBasic Res Cardiol200510013113815739122
- GirgisREChampionHCDietteGBDecreased exhaled nitric oxide in pulmonary arterial hypertension: response to bosentan therapyAm J Respir Crit Care Med200517235235715879413
- BeallCMLaskowskiDStrohlKPPulmonary nitric oxide in mountain dwellersNature200141441141211719794
- WangCWangJZhaoLSildenafil inhibits human pulmonary artery smooth muscle cell proliferation by decreasing capacitative Ca2+ entryJ Pharmacol Sci2008108717818818482
- FrancisSHCorbinJDSildenafil: efficacy, safety, tolerability and mechanism of action in treating erectile dysfunctionExpert Opin Drug Metab Toxicol2005128329316922643
- WhartonJAntiproliferative effects of phosphodiesterase type 5 inhibition in human pulmonary artery cellsAm J Respir Crit Care Med200517210511315817798
- CorbinJDBeasleyABlountMAHigh lung PDE5: a strong basis for treating pulmonary hypertension with PDE5 inhibitorsBiochem Biophys Res Commun200533493093816023993
- HaynesJKithasPATaylorAESelective inhibition of cGMPinhibitable cAMP phosphodiesterase decreases pulmonary vasore-activityAm J Physiol1991261H487H4921652213
- ZhaoLSildenafil inhibits hypoxia-induced pulmonary hypertensionCirculation200110442442911468204
- KosmickiMALong-term use of short and long-acting nitrates in stable angina pectorisCurr Clin Pharmacol2009413214119442078
- AbdollahiMFooladianFEmaniBProtection by sildenafil and theophylline of lead acetate-induced oxidative stress in rat submandibular gland and salivaHum Exp Toxicol20032258759214686481
- PerkHArmaganANazirogluMSildenafil citrate as a phosphodiesterase inhibitor has an antioxidant effect in the blood of menJ Clin Pharm Ther20083363564019138241
- NagendranJArcherSLSolimanDPhosphodiesterase type 5 is highly expressed in the hypertrophied human right ventricle, and acute inhibition of phosphodiesterase type 5 improves contractilityCirculation200711623824817606845
- MichelakisETymchakWLienDOral sildenafil is an effective and specific pulmonary vasodilator in patients with pulmonary arterial hypertension: comparison with inhaled nitric oxideCirculation20021052398240312021227
- LeporeJJMarooABigatelloLMHemodynamic effects of sildenafil in patients with congestive heart failure and pulmonary hypertension: combined administration with inhaled nitric oxideChest20051271647165315888841
- DillerGPvan EijlSOkonkoDoCirculation endothelial progenitor cells in patients with Eisenmenger syndrome and idiopathic pulmonary arterial hypertensionCirculation20081173020303018519847
- SchermulyRTPullamsettiSSKwapiszewskaGPhosphodiesterase 1 upregulation in pulmonary arterial hypertension: target for reverse-remodeling therapyCirculation20071152331233917438150
- NicholsDJMuirheadGJHarnessJAPharmacokinetics of sildenafil after single oral doses in healthy male subjects: absolute bioavailability, food effects and dose proportionalityBr J Clin Pharmacol200253Suppl 15S12S11879254
- MuirheadGJWilnerKColburnWThe effects of age and renal and hepatic impairment on the pharmacokinetics of sildenafilBr J Clin Pharmacol200253Suppl 121S30S11879256
- Revatio.com [Home page on the internet] Updated 11/2009. http://www.revatio.com/intermediateLaunch.aspxAccessed 12/27/2009. Accessed Dec 2009
- HuangSHermesDeSantisEvelynRTreatment of pulmonary arterial hypertension in pregnancyAm J Health Syst Pharm2007641922192617823103
- WebbDJFreestoneSAllenMJSildenafil citrate and blood-pressure-lowering drugs: results of drug interaction studies with an organic nitrate and a calcium antagonistAm J Cardiol19998321C28C10073779
- WebbDJMuirheadGJWulffMSildenafil citrate potentiates the hypotensive effects of nitric oxide donor drugs in male patients with stable anginaJ Am Coll Cardiol200036253110898408
- JacksonGBenjaminNJacksonNEffects of sildenafil citrate on human hemodynamicsAm J Cardiol19998313C20C
- LatiesAMVision disorders and phosphodiesterase type 5 inhibitors: a review of the evidence to dateDrug Saf20093211819132801
- PhilipARamachandaniSDorranceKSildenafil-induced thrombocytopeniaAnn Intern Med200814943743918794570
- PrasadSWilkinsonJGatzoulisMASildenafil in primary pulmonary hypertensionN Engl J Med2000343134211183578
- AtzAMWesselDLSildenafil ameliorates effects of inhaled nitric oxide withdrawalAnesthesiology19999130731010422958
- SastryBKNarasimhanCReddyNKClinical efficacy of sildenafil in primary pulmonary hypertension: a randomized, placebo-controlled, double-blind, crossover studyJ Am Coll Cardiol2004431149115315063421
- BadeschDBHillNSBurgessGSildenafil for pulmonary arterial hypertension associated with connective tissue diseaseJ Rheumatol2007342417242217985403
- MichelakisEDTymchakWNogaMLong-term treatment with oral sildenafil is safe and improves functional capacity and hemodynamics in patients with pulmonary arterial hypertensionCirculation20031082066206914568893
- McLaughlinVVArcherSLBadeschDBACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension AssociationJ Am Coll Cardiol2009531573161919389575
- WilkinsMRPaulGAStrangeJWSildenafil versus Endothelin Receptor Antagonist for Pulmonary Hypertension (SERAPH) StudyAm J Respir Crit Care Med20051711292129715750042
- HemmesARRobbinsIMSildenafil monotherapy in portopulmonary hypertension can facilitate liver transplantationLiver Transpl200915151919109843
- SimonneauGRubinLJGalieNAddition of sildenafil to long-term intravenous Epoprostenol therapy in patients with pulmonary arterial hypertensionAnn Intern Med200814952153018936500
- GhofraniHARoseFSchermulyRTOral sildenafil as long-term adjunct therapy to inhaled iloprost in severe pulmonary arterial hypertensionJ Am Coll Cardiol20034215816412849677
- BurgessGHoogkamerHCollingsLMutual pharmacokinetic interactions between steady-state bosentan and sildenafilEur J Clin Pharmacol200864435018040672
- GruenigEMichelakisEVachieryJLAcute hemodynamic effects of single-dose sildenafil when added to established bosentan therapy in patients with pulmonary arterial hypertension: results of the COMPASS-1 studyJ Clin Pharmacol2009491343135219755415
- SpenceRMandagereADuftonCPharmacokinetics and safety of ambrisentan in combination with sildenafil in healthy volunteersJ Clin Pharmacol2008481451145918832294
- GannMCClarkLChumneyECCost-utility of treatment for pulmonary arterial hypertension: a Markov state-transition decision analysis modelClin Drug Investig200929635646
- GalieNBundageBHGhofraniHATadalafil therapy for pulmonary arterial hypertensionCirculation20091192894290319470885
- WrishkoREDingemanseJYuAPharmacokinetic interaction between tadalafil and bosentan in healthy male subjectsJ Clin Pharmacol20084861061818305126
- ReichenbergerFLong-term treatment with sildenafil in chronic thromboembolic pulmonary hypertensionEur Respir J20073092292717690123
- DeSantoLSMastroianniCRomanoGRole of sildenafil in acute posttransplant right ventricular dysfunction: successful experience in 13 consecutive patientsTransplant Proc2008402015201818675118
- MilmanNBurtonCMIversenMPulmonary hypertension in end stage pulmonary sarcoidosis: therapeutic effect of sildenafil?J Heart Lung Transplant20082732933418342757
- HolverdaSRietemaHBogaardHJAcute effects of sildenafil on exercise pulmonary hemodynamics and capacity in patients with COPDPulm Pharmacol Ther20082155856418342559
- RichaletJPGratadourPRobachPSildenafil inhibits altitude-induced hypoxemia and pulmonary hypertensionAm J Respir Crit Care Med200517127528115516532
- GhofraniHAWiedemannRRoseFSildenafil for treatment of lung fibrosis and pulmonary hypertension: a randomized controlled trialLancet200236089590012354470
- FriesRShariatKvon WilmowskyHSildenafil in the treatment of Raynaud’s phenomenon resistant to vasodilatory therapyCirculation20051122980298516275885
- HoeperMMBarberaJAChannickRNDiagnosis, assessment, and treatment of non-pulmonary arterial hypertension pulmonary hypertensionJ Am Coll Cardiol200954S85S9619555862
- KatzSDParkerJDGlasserDBEfficacy and safety of sildenafil citrate in men with erectile dysfunction and chronic heart failureAm J Cardiol200595364215619391
- PackerMCarverJRRodehefferRJfor the PROMISE study research groupEffect of oral milrinone on mortality in severe chronic heart failureN Engl J Med1991325146814751944425
- MelenovskyVAl-HitiHKazdovaLTranspulmonary B-type natriuretic peptide uptake and cyclic guanosine monophosphate release in heart failure and pulmonary hypertension: the effects of sildenafilJ Am Coll Cardiol20095459560019660688
- LewisGDShahRVPappagianopolasPPDeterminants of ventilator efficiency in heart failure: the role of right ventricular performance and pulmonary vascular toneCirc Heart Fail2008122723319808296
- BehlingARohdeLEColomboFCEffect of 5′-phosphodiesterase four-week long inhibition with sildenafil in patients with chronic heart failure: a double-blind placebo-controlled clinical trialJ Card Fail20081418919718381181
- GuazziMSamajaMArenaRLong-term use of sildenafil in the therapeutic management of heart failureJ Am Coll Cardiol2007502136214418036451
- StehlikJMovsesianMACombined use of PDE5 inhibitors and nitrates in the treatment of pulmonary arterial hypertension patients with heart failureJ Card Fail200915313419181291
- HumbertMSitbonOSimonneauGTreatment of pulmonary arterial hypertensionN Engl J Med20043511425143615459304
- BarstRJPulmonary Arterial Hypertension: Diagnosis and Evidence-Based TreatmentWest Sussex, EnglandJohn Wiley & Sons2008
- McLaughlinVVMcGoonMDPulmonary arterial hypertensionCirculation20061141417143117000921