
Abstract
Background
Kratom, known botanically as Mitragyna speciosa (Korth.), is an indigenous tree in Southeast Asia. Kratom is currently easily available worldwide via special shops and the Internet to use as a drug of abuse, opioid alternative, or pain killer. So far, the pharmacokinetics of this plant has been studied only in animals, and there is no such study in humans. The major abundant active alkaloid in Kratom, mitragynine, is one of the promising new chemical substances to be developed as a new drug. The aim of this study was to examine the pharmacokinetics of mitragynine and assess the linearity in pharmacokinetics in chronic users.
Methods
Since Kratom is illegal in Thailand, studies in healthy subjects would be unethical. We therefore conducted a prospective study by enrolling ten chronic, regular, healthy users. We adjusted the steady state in each subject by giving a known amount of Kratom tea for 7 days before commencement of the experiment. We admitted and gave different oral doses to subjects to confirm linearity in pharmacokinetics. The mitragynine blood concentrations at 17 times points and the urine concentrations during the 24-hour period were collected and measured by liquid chromatography-tandem mass spectrometry method.
Results
Ten male subjects completed the study without adverse reactions. The median duration of abuse was 1.75 years. We analyzed one subject separately due to the abnormal behavior of blood concentration. From data of nine subjects, the pharmacokinetic parameters established were time to reach the maximum plasma concentration (0.83±0.35 hour), terminal half-life (23.24±16.07 hours), and the apparent volume of distribution (38.04±24.32 L/kg). The urine excretion of unchanged form was 0.14%. The pharmacokinetics were observed to be oral two-compartment model.
Conclusion
This was the first pharmacokinetic study in humans, which demonstrated linearity and was consistent with the oral two-compartment model with a terminal half-life of about 1 day. The pharmacokinetic linearity and parameters reported are necessary pharmacological information of Kratom, and there is a possibility for it to be developed medically as a pain killer or better opioid substitute in the future.
Keywords:
Introduction
Kratom, the botanical name of Mitragyna speciosa (Korth.), also known as Ketum in Malaysia, belongs to the Rubiaceae family, which can grow in tropical and subtropical regions of Asia.Citation1,Citation2 It is a native tree indigenous to Southeast Asia, especially in Thailand and Malaysia.Citation2,Citation3 It contains many alkaloids such as mitragynine, paynantheine, speciogynine, and 7-hydroxymitragynine.Citation2 Mitragynine is the most abundant active alkaloid isolated from Kratom.Citation2,Citation4 Mitragynine has an antinociceptive effect, similar to 7-hydroxymitragynine, one of alkaloids, which is a significantly more potent analgesic than mitragynine and morphine.Citation2,Citation4 Kratom possesses dose-dependent pharmacological effects, with stimulant effects in lower doses and opiate-like effects in higher doses.Citation4 Other clinical effects include antinociceptive, antiinflammatory, antidiarrheal, antitussive, antipyretic, euphoric, antidepressant, anxiolytic, blood pressure lowering, antidiabetic, and appetite suppressing as previously described.Citation2,Citation4 Kratom is also reported to be used as an opioid substitute.Citation5–Citation7
There were studies performed to observe the effect of mitragynine several years ago.Citation8,Citation9 The acute toxicities studied in rats include increasing blood pressure, hepatotoxicity, and nephrotoxicity.Citation10 In another rat study, it was found that the aqueous extract, even very high dose, did not cause death and any significant toxicity.Citation11 In humans, the adverse effects or the toxicities include dry mouth, changes in urination, nausea, vomiting, anorexia, weight loss, constipation, nystagmus, and tremor.Citation4,Citation12 In addition, seizure has been reported in previous literature.Citation5,Citation13,Citation14 Primary hypothyroidismCitation15 and intrahepatic cholestasisCitation16 are also reported in a number of cases to be associated with Kratom. For chronic toxicity, impairment of cognitive behavioral function is found in mice fed mitragynine for a long period.Citation17 In humans, anorexia, weight loss, hyperpigmentation, and psychosis are described in chronic abusers.Citation4 Kratom alone, or in combination with other substances, has been shown to cause dependence and withdrawal symptoms following repeated consumption.Citation2,Citation18–Citation21 Kratom has the potential herb–drug interaction on cytochrome P450 (CYP) enzyme activity. This was shown in one study, with potent inhibitory effect for CYP3A4 and CYP2D6, moderate effect for CYP1A2, and weak effect for CYP2C19,Citation22 whereas in another study, mitragynine and 7-hydroxymitragynine also showed the inhibitory effect on P-glycoprotein.Citation23 However, there were a few reports of Kratom-related fatalities.Citation24,Citation25
In Thailand, Kratom is used by manual laborers to enhance physical endurance and productivity and to elicit euphoric effects. It is also used as a folk medicine to treat several diseases or in the past as an opioid alternative by chewing fresh leaves, smoking dried leaves, or brewing as a tea.Citation2–Citation4,Citation12 In the south of Thailand, Kratom is not considered to be a drug of abuse, and it is a part of the way of life, embedded in local custom and tradition. Nevertheless, now it is causing concern, emerging as drug of abuse known as “4×100 cocktail” and one of the most popular illicit substances used,Citation2,Citation14 particularly in the southern part of Thailand. Although, Kratom, a schedule 5 drug in Thai Narcotic Act, is banned in some countries such as Malaysia, it is still legal in Indonesia and the United States and some countries in Europe.Citation2
Kratom has become increasingly trendy in several countries, especially in Europe and USA. Currently, it is available through special shops or online market known as “Legal highs.” Therefore, it is used by the online community and made available by many online vendors.Citation2 It is important to note that Kratom is sometimes used as a drug of abuse alone or in combination with other substances and for medicinal purposes such as to relieve pain.Citation2,Citation4,Citation26–Citation34 Kratom is used to alleviate opioid withdrawal symptoms and is an economical alternative to other opioid-replacement medications without a prescription. There are an increasing number of reports, studies, and reviews about Kratom use for opioid substitution.Citation2,Citation5–Citation7,Citation35 Despite increasing reports and studies on Kratom, to our knowledge, respiratory depression or significant opioid toxic syndrome have not been reported as the toxicity from Kratom.Citation7,Citation14,Citation35 Even if Kratom is mainly available as a drug of abuse, it may yet provide insight into the possibility for its medicinal development as a new and more effective opioid substitute or pain killer in the future, with fewer lethal side effects.
To date, current knowledge of Kratom is limited, and many questions remain regarding its basic safety and the potential toxicities.
Hence, the pharmacology and pharmacokinetics are very important and necessary data to understand in managing poisoning or even widening the medical scope of Kratom in the future. Currently, the pharmacokinetics of Kratom has been derived only from animal studies,Citation36–Citation38 which employed only the rat model and produced variable results. There is no pharmacokinetic study in humans. Thus, the objective of this study was to look for the first time at the pharmacokinetics in humans and to assess the linearity of the pharmacokinetics of mitragynine, the most prevalent alkaloid in Kratom. This active alkaloid is a promising new chemical for new drug development.
Methods
Study design and subjects
The study was approved by Institutional Review Board of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University. Since Kratom is an illegal substance in Thailand, performing the study in healthy subjects is unethical; therefore, we performed the prospective experimental study in chronic regular users. We asked for permission to possess Kratom leaves from the Thai Food and Drug Administration to be used in this study.
The primary outcome was the pharmacokinetics of mitragynine. The secondary outcomes were blood pressure and pulse rate change after taking Kratom. We used different doses of Kratom to observe the dose responses in our study.
Inclusion criteria for recruiting subjects in this study included healthy participants, without any underlying diseases, using Kratom regularly for more than 6 months, having positive urine or blood test for mitragynine at the first hospital visit. We excluded subjects who refused to participate in the study. All subjects provided written informed consents.
Study protocol
Preparation of Kratom tea
Kratom tea for this study was prepared from leaves collected from Phatumthani province, Thailand during 2012–2013. Ramathibodi Poison Center, Faculty of Medicine Ramathibodi Hospital was certified to handle the plant material. First, fresh or dried leaves of Kratom and different times for boiling the Kratom tea (30 minutes or 1 hour) were compared to find the most proper conditions. Fresh leaves and a 1-hour boiling time were selected for preparing the tea. In detail, 40 g of fresh Kratom leaves were cut and mixed together with 2 L of distilled water, and the leaves were boiled for 1 hour. Three mitragynine concentrations of tea were prepared: 0.1042, 0.166, and 0.1917 mg/mL. Then, the tea was kept in sterile 60 mL bottles and at 4°C for stability testing, which was performed at 3, 5, 7, and 14 days.
Prestudy period
On the first day, subjects were interviewed and underwent medical, physical, and basic psychological evaluations at Ramathibodi Hospital. The baseline mitragynine concentration and blood chemistry were also checked.
Since the subjects were chronic, regular users, and did not need to stop their Kratom use, we considered them adjusted to the steady state of Kratom levels by ingesting a known amount of Kratom tea (60 mL) every day for 7 days.
Study period
The pharmacokinetic study was performed on day 8. All subjects were admitted and resided in a ward for 24 hours. They were randomly assigned to take either 60 mL or 120 mL of the tea defined as loading doses or the 8th dose added in the study day. Forearm venous blood was collected from subjects through a heparin lock at 17 times points during the 24-hour period at time 0 (before the loading dose was given), 15, 30, and 45 minutes; 1, 1.25, 1.5, 1.75, 2, 2.5, 3, 4, 6, 9, 12, 19, and 24 hours. Urine samples were collected during the period of study to measure Kratom concentrations.
For physiologic changes and safety, vital signs as well as any abnormal signs and symptoms were also observed during the study period.
Specimen analysis
Chemicals
Mitragynine was purchased from Cerilliant Corporation (Round Rock, Texas, USA), 7-methyltestosterone from Fluka Chemie GmBH (Buchs, Switzerland), ethyl acetate from Thermo Fisher Scientific (Waltham, MA, USA), and acetic acid and methanol were from Merck KGaA (Darmstadt, Germany). All chemicals were of analytical grade.
Analysis of plasma and urine samples
A 0.5 mL aliquot of each subject’s plasma and urine samples (indicate period of collection) was spiked with 25 μL of 2.0 μg/mL 7-methyltestosterone (internal standard) to achieve final concentration 100 ng/mL. A 2 mL aliquot of 0.1 M phosphate buffer, pH 6.0, was added and briefly mixed. The solid phase extraction (SPE) column (C18; Agilent Technologies, Santa Clara, CA, USA) was conditioned with 2 mL of methanol and a 2 mL aliquot of 0.1 M phosphate buffer, pH 6.0. The plasma or urine sample then was loaded onto a conditioned SPE column, and 1 mL of deionized water and 1 mL of 10 mM acetic acid were added to the SPE column, which was dried for 5 minutes under vacuum (<20 mmHg). Analytes were eluted with 3 mL of ethyl acetate and dried under a flow of nitrogen gas below 40°C. This residue was reconstituted with 100 μL of 20% acetonitrile.
Analysis of Kratom tea
A 10 μL aliquot was added to 990 μL of 20% (v/v) acetonitrile, mixed, and centrifuged at 13,800× g for 5 minutes at room temperature. The supernatant was used for subsequent analysis.
Liquid chromatography-tandem mass spectrometry analysis
The sample volume of 5 μL (for plasma or urine) or 2 μL (of Kratom tea) were analyzed using an Amazon SL LC-MS/MS system. Liquid chromatography was performed in an UltiMate 3000 UHPLC system (Thermo Fisher Scientific) equipped with a Luna-C18 separation column (100 mm ×2.1 mm; 3 μm particle size) and a same phase guard column (10 mm ×2.1 mm; 3 μm particle size). All samples were kept at 10°C in autosampler trays during the analysis cycle. Mobile phase A was composed of 5 mM ammonium acetate together with 0.1% formic acid, and mobile phase B was acetonitrile with 0.1% formic acid. After introduction of the sample, the mobile phase was initiated at 10% B (90% A) and linearly increased to 40% B within 10 minutes, then to 75% B within 13.5 minutes, and finally to 80% B within 16 minutes and maintained for 5 minutes.
Mass spectrometry was performed in an amaZon SL Ion Trap spectrometer (Bruker Daltonics, GmbH, Germany). A standard electrospray ionization source was operated in positive ion mode with the nebulizer at a gas flow rate of 8.0 L/minute and drying temperature of 250°C. End plate offset and capillary voltage was 500 V and 4,500 V, respectively. Multiple reaction monitoring transition was 399.20→238.20 and 303.20→285.20 for mitragynine (retention time 9.10 minutes) and 7-methyltestosterone (retention time 13.74 minutes), respectively. Line spectra were collected in full scan mode from 50 to 1,000 Da. The validation of the analytical method was performed and will be published separately (Auparakkitanon, unpublished, 2015).
Pharmacokinetics and statistical analysis
The pharmacokinetics of mitragynine was evaluated by use of computer software, WinNonlin® version 3.0 (Pharsight Corporation, Mountain View, CA, USA). Noncompart-mental analysis included determination of the following parameters: the maximum or peak plasma concentration (Cmax); the time to maximum observed concentration or time to reach Cmax (tmax); terminal half-life (t1/2), estimated via linear regression of time and the log terminal end portion of the curve; and the area under the time–concentration curve from the time of dosing to the time of the last observable concentration (AUC0−tlast), calculated by the log linear trapezoidal rule. The area under the curve (AUC) extrapolated to time to infinity (AUC0–∞) can be calculated by adding AUC0−tlast with the last observable concentration (Clast) divided by linear regression-fitted terminal slope (λZ). The apparent total clearance (CL/F) was calculated by dose/AUC0–∞. The apparent volume of distribution (Vd/F) values were calculated in L/kg of body weight and were computed based on the terminal elimination phase and the apparent CL/F. Data were reported as the mean ± standard deviation (SD) unless otherwise defined. Repeated measures ANOVA were tested for continuous data of mean blood pressure, pulse rate, and capillary blood glucose. The mean and SD were for continuous data, and the frequency and percentage were for categorical data.
Results
There were ten subjects recruited in this study. All were healthy men who had no preexisting diseases. The demographic data is shown in . The liver and kidney function values were within acceptable limit.
Table 1 The demographic data of ten subjects
The data from our laboratory analysis showed that mitragynine concentration in the tea was stable during storage at the subjects’ homes, and this meant that the subjects actually received the same dose every day.
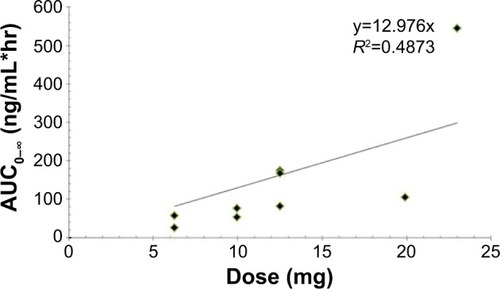
The daily doses and loading doses were different and divided into five groups, as shown in . The normal and semilogarithmic plot of plasma mitragynine concentration against time curve of every subject after the administration of a loading dose are shown in . We found the abnormal behavior of blood concentration in one subject, which was clearly far different from that of the other subjects. This subject’s parameter was analyzed separately. The highest Cmax, 0.105 μg/mL, and the highest AUC0−tlast, 0.67 μg h/mL, were found in the subject taking the highest loading dose, 23 mg. The lowest Cmax was 0.0185 μg/mL, found in the subject with the low loading dose 9.96 mg. The lowest AUC0−tlast was 0.062 μg h/mL, found in the subject with the lowest loading dose, 6.25 mg. The Tmax was 0.83±0.35 hours and the average apparent Vd/F and CL/F of mitragynine were 38.04±24.32 L/kg and 98.1±51.34 L/h kg, respectively, as shown in . The semilog plot of pharmacokinetics time profiles in nine out of all ten subjects demonstrated biexponential decline, which suggested the pharmacokinetic behavior of mitragynine followed the oral two-compartment model, as shown in . The correlation between the loading dose and Cmax, as well as the loading dose and AUC0–∞ were linear ( and ). When the dose increased, the Cmax and AUC0–∞ increased proportionally with dose. We found that the CL/F was quite constant and not increased when the loading dose increased. Altogether, it was suggested that the pharmacokinetics of mitragynine was linear or first order kinetics. The urine excretion of unchanged mitragynine was very limited, as it was only 0.14%.
Table 2 The number of subjects, the daily mitragynine doses to adjust for the steady state, and the loading doses in each subject
Table 3 The summary on the pharmacokinetic parameters of mitragynine
Figure 1 Plasma mitragynine concentration–time curve of every subject after the administration of a loading dose: the normal plot (A) and semi-logarithmic plot (B).
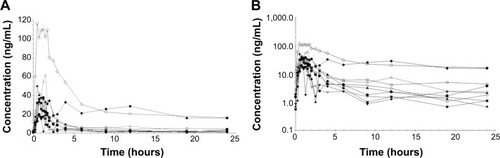
Figure 2 The relationship between the maximum plasma concentration (Cmax) and loading dose.
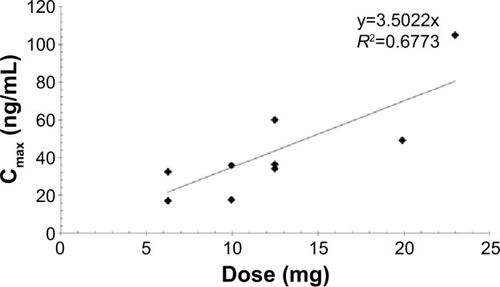
Figure 3 The relationship between the area under the curve extrapolated to time to infinity (AUC0–∞) and loading dose.
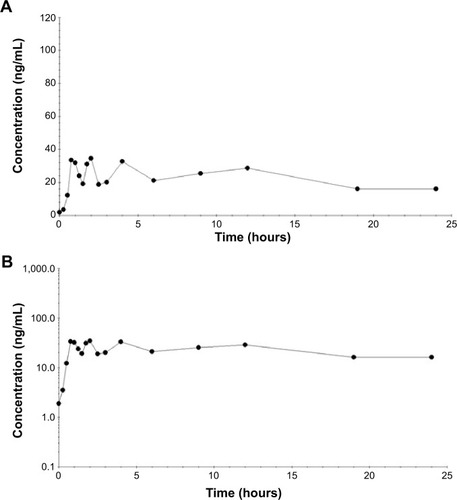
For one subject who took 9.96 mg for both daily and loading doses and had the abnormal behavior of blood concentration, his normal and semilogarithmic plots are shown in . There was no distribution phase because no sharp decrease of the blood concentration was seen. The possible errors were excluded by reevaluation. His blood samples were collected for other investigation in this regard.
Figure 4 Plasma mitragynine concentration – time curve of one subject with abnormal behavior of blood concentration after the administration of a loading dose: the normal plot (A) and semi-logarithmic plot (B).
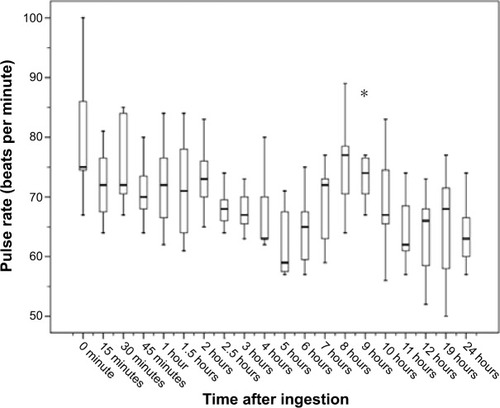
The blood pressure and pulse rate of every subject increased at the 8th hour of study and then returned to normal, as shown in and . Capillary blood glucose levels were normal during the period of the study. All subjects described tongue numbness after they finished drinking Kratom tea. No abnormal signs and symptoms were detected during this period of the study.
Figure 5 Blood pressures (BP) of every subject during the day of the study.
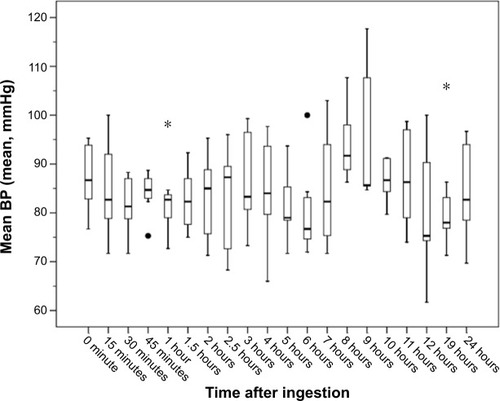
Figure 6 Pulse rates of every subject during the day of the study.
Discussion
The pharmacokinetic parameters are important and essential information for the pharmacologic study of any substance of interest. To our knowledge, this study was the first pharmacokinetic study of Kratom in human. In our study, the pharmacokinetic parameters were different from those of animal studies. As we used different doses, more information was added, showing the pharmacokinetics were linear and followed an oral two-compartment model. Information on the bioavailability of oral mitragynine is not currently available in humans. The Vd and CL in our study were apparent Vd and CL. According to this apparent Vd, it would be considered as a large Vd, unless the bioavailability was less than 2%. For example, we applied the oral bioavailability of mitragynine from the rat study, which was 3.03±1.47%Citation29 in our pharmacokinetic analysis. The estimated Vd and CL would be 1.15 L/kg and 2.97 L/h kg, respectively. We hypothesize that mitragynine has a large Vd and is mainly distributed out of the circulation.
As urine excretion of the unchanged mitragynine form was as low as 0.14%, this suggests that renal excretion should not be a significant route of excretion, even when its bioavailability was taken into account. Based on our findings, we propose that mitragynine is mainly metabolized by hepatic metabolism to other metabolites. This is consistent with another study on mitragynine.Citation39
As for the clinical and safety aspects, no serious adverse effect was found during the study. This is probably because the doses used in our study were less than 30 mg. However, the daily intake dose of regular abusers was reported to be as high as 276.5 mg in Malaysia.Citation16 Every subject in our study developed tongue numbness after having finished drinking Kratom tea. All of the participants also confirmed that it was the same experience as when they took Kratom. Thus, tongue numbness would be one of the symptoms of Kratom effect that was supported by these studies.Citation8,Citation40
Our study also found that all subjects had increasing blood pressure and heart rate, but the onset was delayed to 8 hours after drinking Kratom tea. The time was later than Tmax; therefore, this finding needs further investigation.
For clinical applications, the beneficial effects of Kratom on opioid withdrawal have been reported in various studies. Our study showed that it had a long elimination t1/2 and linear pharmacokinetics. Taken together, Kratom would be a good candidate for opioid substitute in patients who are addicted to these substances. As it had very low renal clearance, in patients with impaired renal function, dose adjustment might not be needed.
However, based on the finding that the pharmacokinetics of mitragynine is linear, if dose adjustment is needed, it can be easily implemented. Extracorporeal techniques such as hemodialysis or hemoperfusion might not be able to remove mitragynine from the circulation as it would have high Vd/F.
In conclusion, pharmacokinetics of mitragynine, a major and active metabolite of Kratom, is linear and follows the two-compartment model. It has a long terminal t1/2, extending for hours, and high apparent Vd. Renal excretion of unchanged mitragynine is very low. The pharmacokinetics of Kratom in human was different from animals, thus applying the animal data to humans should be used with caution. Numbness of tongue would be a clinical marker of Kratom ingestion. Abnormal pharmacokinetics in some patients and delayed onset of increasing blood pressure and heart rate require further investigation.
Kratom has been an emerging substance of abuse, available worldwide. In the future, Kratom may merit further scientific study to develop its medical benefits, as a better opioid substitute, with fewer lethal side effects, or as an effective pain killer.
Limitation
This study was done in chronic users. Therefore, the pharmacokinetic parameters would not apply for healthy subjects since the metabolism in chronic users might differ from that of naïve persons. Further studies in healthy subjects and population pharmacokinetics should be carried out.
Acknowledgments
We wish to express our sincere thanks to Professor Amnuay Thithapandha for his help with English editing and comments on the manuscript and Mrs Umaporn Udomsubpayakul for the statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
- PuffCChayamaritKChamchumroonVRubiaceae of Thailand: A Pictorial Guide to Indigeneous and Cultivated GeneraBangkokForest Herbarium, National Park, Wildlife and Plant Conservation Department2005
- HassanZMuzaimiMNavaratnamVFrom Kratom to mitragynine and its derivatives: physiological and behavioural effects related to use, abuse, and addictionNeurosci Biobehav Rev201337213815123206666
- SuwanlertSA study of kratom eaters in ThailandBull Narc197527321271041694
- BabuKMMcCurdyCRBoyerEWOpioid receptors and legal highs: Salvia divinorum and KratomClin Toxicol (Phila)200846214615218259963
- BoyerEWBabuKMAdkinsJEMcCurdyCRHalpernJHSelf-treatment of opioid withdrawal using kratom (Mitragynia speciosa korth)Addiction200810361048105018482427
- BoyerEWBabuKMMacalinoGEComptonWSelf-treatment of opioid withdrawal with a dietary supplement, KratomAm J Addict200716535235617882605
- VicknasingamBNarayananSBengGTMansorSMThe informal use of ketum (Mitragyna speciosa) for opioid withdrawal in the northern states of peninsular Malaysia and implications for drug substitution therapyInt J Drug Policy201021428328820092998
- GrewalKSObservations on the pharmacology of mitragynineJ Pharmacol Expr Ther1932463251271
- MackoEWeisbachJADouglasBSome observations on the pharmacology of mitragynineArch Int Pharmacodyn Ther197219811451614626477
- HarizalSNMansorSMHasnanJTharakanJKAbdullahJAcute toxicity study of the standardized methanolic extract of Mitragyna speciosa Korth in rodentJ Ethnopharmacol2010131240440920643198
- KamalMSAGhazaliARYahyaNAWasimanMIIsmailZAcute toxicity study of standardized Mitragyna speciosa Korth aqueous extract in Sprague Dawley ratsJ Plant Stud201212120129
- UlbrichtCCostaDDaoJAn evidence-based systematic review of kratom (Mitragyna speciosa) by the Natural Standard Research CollaborationJ Diet Suppl201310215217023725528
- NelsenJLLapointJHodgmanMJAldousKMSeizure and coma following Kratom (Mitragynina speciosa Korth) exposureJ Med Toxicol20106442442620411370
- TrakulsrichaiSTongpoASriaphaCKratom abuse in Ramathibodi Poison Center, Thailand: a five-year experienceJ Psychoactive Drugs201345540440824592666
- ShelegSVCollinsGBA coincidence of addiction to “Kratom” and severe primary hypothyroidismJ Addict Med20115430030121817918
- KappFGMaurerHHAuwärterVWinkelmannMHermanns-ClausenMIntrahepatic cholestasis following abuse of powdered kratom (Mitragyna speciosa)J Med Toxicol20117322723121528385
- ApryaniEHidayatMTMoklasMAFakuraziSIdayuNFEffects of mitragynine from Mitragyna speciosa Korth leaves on working memoryJ Ethnopharmacol2010129335736020371280
- McWhirterLMorrisSA case report of inpatient detoxification after kratom (Mitragyna speciosa) dependenceEur Addict Res201016422923120798544
- SinghDMüllerCPVicknasingamBKKratom (Mitragyna speciosa) dependence, withdrawal symptoms and craving in regular usersDrug Alcohol Depend201413913213724698080
- SaingamDAssanangkornchaiSGeaterAFBalthipQPattern and consequences of krathom (Mitragyna speciosa Korth.) use among male villagers in southern Thailand: a qualitative studyInt J Drug Policy201324435135823083922
- SaingamDAssanangkornchaiSGeaterAFLerkiatbunditSValidation of Krathom (Mitragyna speciosa Korth.) Dependence Scale (KDS): a dependence screen for internationally emerging psychoactive substanceSubst Abus201435327628324853660
- KongWMChikZRamachandraMSubramaniamUAziddinREMohamedZEvaluation of the effects of Mitragyna speciosa alkaloid extract on cytochrome P450 enzymes using a high throughput assayMolecules20111697344735621876481
- MandaVKAvulaBAliZKhanIAWalkerLAKhanSIEvaluation of in vitro absorption, distribution, metabolism, and excretion (ADME) properties of mitragynine, 7-hydroxymitragynine, and mitraphyllinePlanta Med201480756857624841968
- NeermanMFFrostREDekingJA drug fatality involving KratomJ Forensic Sci201358Suppl 1S278S27923082895
- KarinenRFosenJTRogdeSVindenesVAn accidental poisoning with mitragynineForensic Sci Int2014245Ce29e3225453780
- AhmadKAzizZMitragyna speciosa use in the northern states of Malaysia: a cross-sectional studyJ Ethnopharmacol2012141144645022440259
- Burillo-PutzeGLópez BrizECliment DíazB[Emergent drugs (III): hallucinogenic plants and mushrooms]An Sist Sanit Navar2013363505518 Spanish24406363
- ForresterMBKratom exposures reported to Texas poison centersJ Addict Dis201332439640024325774
- ProzialeckWCJivanJKAndurkarSVPharmacology of kratom: an emerging botanical agent with stimulant, analgesic and opioid-like effectsJ Am Osteopath Assoc20121121279279923212430
- RosenbaumCDCarreiroSPBabuKMHere today, gone tomorrow… and back again? A review of herbal marijuana alternatives (K2, Spice), synthetic cathinones (bath salts), kratom, Salvia divinorum, methoxetamine, and piperazinesJ Med Toxicol201281153222271566
- SchmidtMMSharmaASchifanoFFeinmannC“Legal highs” on the net-Evaluation of UK-based Websites, products and product informationForensic Sci Int20112061–3929720650576
- UjváryIPsychoactive natural products: overview of recent developmentsAnn Ist Super Sanita2014501122724695249
- ArndtTClaussenUGüssregenBKratom alkaloids and O-desmethyltramadol in urine of a “Krypton” herbal mixture consumerForensic Sci Int20112081–3475221112167
- RechMADonaheyECappiello DziedzicJMOhLGreenhalghENew drugs of abusePharmacotherapy Epub2014124
- WardJRosenbaumCHernonCMcCurdyCRBoyerEWHerbal medicines for the management of opioid addiction: safe and effective alternatives to conventional pharmacotherapy?CNS Drugs20112512999100722133323
- de MoraesNVMorettiRAFurrEBMcCurdyCRLanchoteVLDetermination of mitragynine in rat plasma by LC-MS/MS: application to pharmacokineticsJ Chromatogr B Analyt Technol Biomed Life Sci20098772425932597
- JanchaweeBKeawpradubNChittrakarnSPrasetthoSWararatananurakPSawangjareonKA high-performance liquid chromatographic method for determination of mitragynine in serum and its application to a pharmacokinetic study in ratsBiomed Chromatogr200721217618317221920
- ParthasarathySRamanathanSIsmailSAdenanMIMansorSMMurugaiyahVDetermination of mitragynine in plasma with solid-phase extraction and rapid HPLC-UV analysis, and its application to a pharmacokinetic study in ratAnal Bioanal Chem201039752023203020454783
- PhilippAAWissenbachDKZoerntleinSWKleinONKanogsunthornratJMaurerHHStudies on the metabolism of mitragynine, the main alkaloid of the herbal drug Kratom, in rat and human urine using liquid chromatography-linear ion trap mass spectrometryJ Mass Spectrom20094481249126119536806
- ChittrakarnSKeawpradubNSawangjaroenKKansenalakSJanchaweeBThe neuromuscular blockade produced by pure alkaloid, mitragynine and methanol extract of kratom leaves (Mitragyna speciosa Korth.)J Ethnopharmacol2010129334434920371282