
Abstract
Background
Causative treatment of patients with wild-type transthyretin amyloid cardiomyopathy (wtATTR-CM) is lacking. Recent reports indicate the potential use of epigallocatechin-3-gallate (EGCG), the most abundant catechin in green tea, to inhibit amyloid fibril formation. We sought to investigate changes of cardiac function and morphology in patients with wtATTR-CM after consumption of green tea extract (GTE).
Methods
Twenty-five male patients (71 [64; 80] years) with wtATTR-CM were submitted to clinical examination, echocardiography, cardiac magnetic resonance imaging (cMRI) (n=14), and laboratory testing before and after daily consumption of GTE capsules containing 600 mg epigallocatechin-3-gallate for at least 12 months.
Results
A significant decrease of left ventricular (LV) myocardial mass by 6% (196 [100; 247] vs 180 [85; 237] g; P=0.03) by cMRI and total cholesterol by 8.4% (191 [118; 267] vs 173 [106; 287] mg/dL; P=0.006) was observed after a 1-year period of GTE consumption. LV ejection fraction by cMRI (53% [33%; 69%] vs 54% [28%; 71%]; P=0.75), LV wall thickness (17 [13; 21] vs 18 [14; 25] mm; P=0.1), and mitral annular plane systolic excursion (10 [5; 23] vs 8 [4; 13] mm; P=0.3) by echocardiography remained unchanged.
Conclusion
This study supports LV mass stabilization in patients with wtATTR-CM consuming GTE potentially indicating amyloid fibril reduction.
Introduction
Transthyretin (TTR) is the most common precursor protein of hereditary amyloidosis. Its phenotype is predominantly characterized by sensorimotor polyneuropathy and/or infiltrative cardiomyopathy (CM).Citation1,Citation2 Moreover, TTR causes a nongenetic disease with deposition of wild-type (wt) TTR amyloid (ATTR) mainly in the heart of elderly males.Citation2 In contrast to the hereditary form, no typical mutation in the TTR gene can be found in wtATTR patients, and the pathogenic mechanisms are a subject of ongoing research.Citation3 Cardiac involvement is by far the most relevant predictor of outcome in both hereditary and wtATTR amyloidosis. Median survival ranged between 4 and 6 years.Citation4,Citation5 Cardiac wtATTR deposition was found postmortem in 25% of patients above 85 years of age.Citation4 A recent analysis of skeletal scintigraphy revealed a prevalence of wtATTR-CM near 1.4% among males in the ninth decade of life.Citation6
Currently, causative treatment of wtATTR-CM is lacking. Diuretics are capable of reducing dyspnea, but standard heart failure medication does not affect amyloid deposition itself.Citation7 During the course of 1 year, wtATTR-CM usually worsens, as indicated by an increase of the left ventricular (LV) wall thickness by 0.2 mm, an increase of NT-proBNP by 1,487 pg/mL, and a decline of LV ejection fraction by 11%.Citation8
Recently, in vitro experiments have shown that epigallocatechin-3-gallate (EGCG), the most abundant catechin in green tea, inhibits fibril formation of diverse amyloidogenic proteins.Citation9–Citation11 Disruption of ATTR fibrils was observed after a daily oral administration of 100 mg/kg EGCG for 6 weeksCitation12 using a transgenic mouse model of familial amyloidotic polyneuropathy carrying the human amyloidogenic Val30Met TTR variant. In a recent study, we demonstrated a decrease of LV mass in a small cohort of patients with hereditary ATTR-CM and wtATTR-CM after a daily consumption of green tea for 12 months.Citation13 In the present study, we report on our findings in a larger, more homogenous cohort of patients with exclusively wtATTR-CM.
Materials and methods
Study subjects
Twenty-five male patients (71 [64; 80] years) were recruited at the Heidelberg Amyloidosis Center (Heidelberg, Germany) between 2008 and 2012. All patients underwent myocardial biopsy and diagnosis of wtATTR was confirmed by immunohistochemistry and molecular genetic testing. Patients started green tea consumption on their own initiative due to the rather widespread knowledge of the effects of EGCG on the disease among patients.
Two patients died during the study period, and follow-up data were not available for two further patients. Data from seven patients had already been reported in our previous study.Citation13 All patients had stable heart failure for at least 3 months prior to study inclusion. Echocardiography, cardiac magnetic resonance imaging (cMRI) (n=14), and laboratory testing, including total cholesterol, troponin-T, and NT-proBNP, were performed before and after 12 months of daily consumption of 1,200 mg green tea extract (GTE) containing 600 mg EGCG in four capsules of praevent-loges® (Dr. Loges & Co GmbH [Winsen, Germany]). Routine medication was continued during this period.
Ethics statement
The study was conducted according to the principles expressed in the Declaration of Helsinki and was approved by the institutional review board of the medical faculty of the University of Heidelberg, Germany (vote number S-024/2008). Written informed consent was obtained from all participants.
Echocardiography
Transthoracic echocardiograms were performed using commercially available ultrasound diagnostic systems (Vivid 7; GE Healthcare, Milwaukee, WI, USA). Examinations were analyzed blindfolded offline on a commercially available workstation (Centricity Cardiology CA1000 2.0; GE Medical Systems, Milwaukee, WI, USA) by two experienced sonographers (MA and RB) who were unaware of all other clinical data. Thickness of interventricular septum (IVS) and posterior wall were measured in late diastole; LV cavity diameter was scaled in end diastole and end systole. Longitudinal myocardial function was quantified by mitral (MAPSE) and tricuspid (TAPSE) annular plane systolic excursion obtained from the apical four-chamber view using M-mode imaging.
cMRI protocol
All cMRI exams were performed on a 1.5 T scanner (Achieva; Philips, Best, the Netherlands) with a 32-element cardiac receiver coil and analyzed by two experienced investigators (FS and HS), both being unaware of the remaining clinical data. Vector electrocardiogram-gated standard steady-state free precession cine sequences were acquired in short axes covering the whole LV and in three long-axis views (two-, three-, and four-chamber views).
Cardiac volumes, LV ejection fraction, and myocardial mass were measured in late diastole from short-axis image stacks by manual delineation of endocardial and epicardial borders excluding papillary muscles using a commercially available workstation (Viewforum, version 3.4; Philips).
Statistical analysis
Continuous data were expressed as median (range). Categorical variables were expressed as absolute number (percent). All analyses were performed using SPSS (version 20.0, IBM Corporation, Armonk, NY, USA). Statistical significance was defined if P-values were <0.05. Differences between the nonparametric, continuous parameters assessed at study inclusion and at 12-month follow-up were compared by the Wilcoxon matched-pairs signed-rank test.
Results
Study cohort
Clinical demographics of the study cohort including the subgroup of cMRI are given in . None of the patients discontinued green tea consumption and no serious side effects were reported during the study period. No changes in New York Heart Association (NYHA) class could be observed, and no significant change in surface electrocardiogram parameters (rhythm, heart rate, PQ, QRS, QTc) occurred. Two patients were lost during follow-up. One patient died due to sepsis, another due to spontaneous retroperitoneal hematoma requiring a prolonged stay in the intensive care unit with artificial ventilation and recurrent infections, resulting in multiorgan failure and, finally, death. Follow-up over periods of 44, 25, and 30 months, respectively, was achieved in three patients.
Table 1 Baseline characteristics
Blood analysis
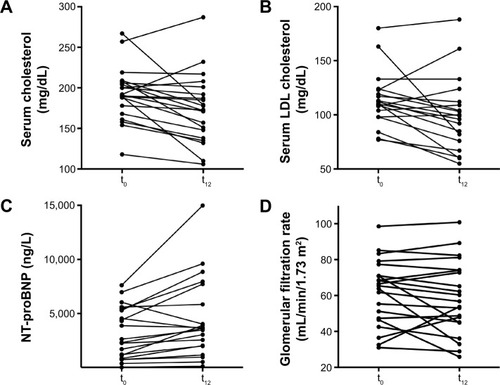
In 18 (85.7%) patients, a significant decrease of total serum cholesterol by 8.4% was observed (191 [118; 267] vs 173 [106; 287] mg/dL; P=0.006) during the 12-month study period. In three patients, an increase of cholesterol by 3% was observed. In 16 (76.2%) patients, low-density lipoprotein (LDL) cholesterol decreased by 8.0% (110 [60; 180] vs 99 [55; 188] mg/dL; P=0.02]). In four patients, LDL cholesterol increased by 7%.
Median NT-proBNP levels remained stable (3,681 vs 3,617 ng/L) in the whole study group during the observation period. Glomerular filtration rate calculated by the modified diet in renal disease (MDRD) formula (62 [31; 99] vs 57 [26; 101] mL/min; P=0.23), GOT (30 [16; 56] vs 33 [17; 74] U/L; P=0.90), and GPT (29 [10; 57] vs 29 [10; 74] U/L; P=0.95) remained unchanged. TTR plasma levels remained stable during the study period (0.28 [0.14; 0.90] vs 0.26 [0.18; 0.50] mg/dL; P=0.64; n=16). Results of laboratory testing are shown in and .
Table 2 Blood analysis
Figure 1 Laboratory testing.
Abbreviations: cMRI, cardiac magnetic resonance imaging; LDL, low-density lipoprotein; MDRD, modified diet in renal disease; t0, baseline; t12, at 12 months; wtATTR-CM, wild-type transthyretin amyloid cardiomyopathy; NT-proBNP, N-terminal prohormone of brain natriuretic peptide.
Echocardiography analysis
Mean thickness of IVS (17 [13; 28] vs 18 [14; 25] mm; P=0.1) and posterior wall (16 [11; 24] vs 17 [12; 19] mm; P=0.4) remained unchanged during the study period ().
Figure 2 Echocardiography findings.
Abbreviations: t0, baseline; t12, at 12 months; wtATTR-CM, wild-type transthyretin amyloid cardiomyopathy.
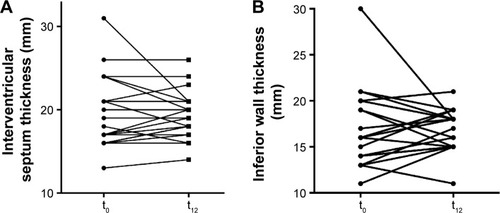
In seven (33.3%) patients, an increase of either 1) both IVS and posterior wall thickness (n=4) or 2) isolated posterior wall thickness or IVS thickness (n=3) occurred, by an average of 1.9 mm (13%).
MAPSE (10 [5; 23] vs 8 [4; 13] mm; P=0.3), TAPSE (14 [8; 23] vs 15 [2; 20] mm; P=0.4), and passive mitral inflow/lateral early diastolic mitral annular velocity (E/E’) ratio (11 [7; 28] vs 14 [4; 31]; P=0.8) remained unchanged. Results of echocardiography are shown in .
Table 3 Echocardiography
cMRI analysis
In the subgroup of patients assessed by cMRI (n=14) (; ), in 12 (86%) patients, a decrease of LV myocardial mass by 5.9% was observed during follow-up (196 [100; 247] vs 180 [85; 237] g; P=0.03). In the remaining two patients, an increase by 11% and by 15% was observed, respectively.
Table 4 Cardiac magnetic resonance imaging
Figure 3 cMRI findings.
Abbreviations: cMRI, cardiac magnetic resonance imaging; LV, left ventricular; LVEF, LV ejection fraction; t0, baseline; t12, at 12 months; wtATTR-CM, wild-type transthyretin amyloid cardiomyopathy.
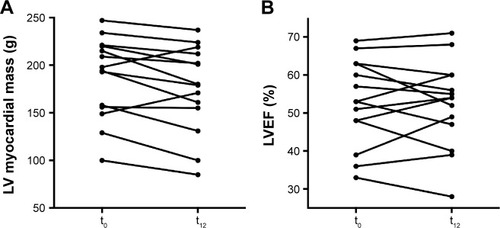
LV ejection fraction (53% [33%; 69%] vs 54% [28%; 71%]; P=0.75) and longitudinal function (MAPSE: 6.5 [3; 10] vs 6 [3;9] mm; P=0.08 and TAPSE: 12 [4; 17] vs 11 [5; 16] mm; P=0.28) remained unchanged.
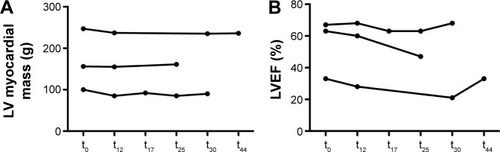
LV mass of the three patients with long-term observation are shown in . Patient 1 showed a reduction of 11 g (4.4%) after 44 months, patient 2 an increase of 5 g (3.2%) after 25 months, and patient 3 a reduction of 10 g (10%) after 30 months.
Figure 4 LV myocardial mass (A) and LVEF (B) of patients with wtATTR-CM who underwent assessment by cMRI with green tea extract consumption for longer than 1 year.
Discussion
We report on a cohort of wtATTR-CM patients consuming GTE for at least 1 year to demonstrate potential effects on inhibition of amyloid fibril formation.Citation10,Citation14 A significant decrease of LV myocardial mass was observed by cMRI while no change of LV wall thickness was detected by echocardiography. A decrease of LV mass was found in two of three patients after 30 and 44 months of observation, while there was an increase by 3% in the third patient after 25 months of treatment. No side effects were reported during the study period. Within a time span of 1 year, ATTR-CM was found to be associated with a significant increase of LV myocardial mass and IVS thickness as well as a reduction of LV ejection fraction.Citation8,Citation15 Thus, we concluded that EGCG may halt progression of this fatal disease.
wtATTR-CM is characterized by predominantly cardiac deposition of wtATTR. According to more recent data achieved by skeletal scintigraphy, it appears to cause LV infiltration in up to 1% of patients above 60 years of age.Citation6 Without treatment, ATTR-CM was found to be associated with an increase of LV mass by 8% within a 1-year periodCitation15 and a decrease of LV ejection fraction by 3.2% during 6 months.Citation8 An association between amyloid load and myocardial mass could be demonstrated in a mouse model by Ogawa.Citation16 Causative treatment options are lacking. In other studies, prognosis of patients with ATTR-CM remained poor, with median survival of 4–6 years.Citation5,Citation17 Diverse in vitro and in vivo strategies have been aimed to stop amyloid fibril formation by stabilization of TTR protein (tafamidis [Vyndaqel®], EGCG) and by RNA interference using ALN-TTRsc (Revusiran®) or ALN-TTR02 (Patisiran®) or to dissolve amyloid fibrils by EGCG. The health benefit of green tea, in particular EGCG, has been reported for many years,Citation18 and only rarely were adverse effects ascribed to the consumption of GTE.Citation19 Actually, two clinical Phase III studies using tafamidis and RNA interference drugs are recruiting patients, but high costs and lack of long-term data on toxicity have to be considered as limitations so far.Citation20
Green tea is considered to positively affect cardiovascular and metabolic complicationsCitation21 and to improve lipid profile.Citation12 Thus, decrease of LDL cholesterol appears to be an indicator of GTE bioavailability. To assure a daily constant intake dose of EGCG, and to facilitate fluid restriction in those patients with severe heart failure, we administered capsules containing EGCG and vitamin C. Vitamin C improves the intestinal stability of EGCG.Citation22,Citation23
Hunstein’s experiment to treat his light-chain amyloidosis with green teaCitation14 was stimulated by the experiments of Bieschke J et alCitation9 and Ehrnhoefer DE et al,Citation10 who demonstrated amyloid fibril disruption incubated with EGCG. In a retrospective analysis of a larger cohort of patients with light-chain amyloidosis, a significant reduction of myocardial mass and an improvement of LV ejection fraction and NYHA functional class were reported in patients consuming green tea, while no changes were observed in patients without intake of green tea.Citation24
Recently, we demonstrated by cMRI an average reduction of LV myocardial mass by 12.5% in a heterogeneous cohort of patients with mutant ATTR (n=8) and wtATTR (n=6).Citation13 This study was focused on patients with wtATTR-CM to avoid modifying effects from inherited forms of ATTR-CM. It remains unclear why some patients did not respond to GTE. Different individual metabolic conditions and renal excretion might have an impact on EGCG plasma concentration. Up to now, no standardized test has been validated that allows reproducible quantification of EGCG plasma concentration.
We observed a disagreement between echocardiography and cMRI data. We assumed that the higher inter- and intraobserver variability of echocardiography within a small sample size could be a reasonable explanation.Citation25 cMRI is considered as the gold standard for analysis of cardiac morphology and function.Citation26,Citation27
Compared with other types of cardiac amyloidosis, wtATTR-CM progresses slowly. Demonstration of a long-term benefit of EGCG requires a longer follow-up beyond 1 year. According to the mechanism of action, it is proposed that EGCG has an additional effect on amyloid fibril formation and disruption to novel drugs that have been reported to inhibit fibril formation from TTR. Tafamidis, a novel stabilizer of human TTR,Citation28 has been shown to stop progression of ATTR V30M polyneuropathy in two-thirds of patients.Citation29,Citation30 It was approved by the European Medicines Agency in December 2011 and by the Japanese Pharmaceuticals and Medical Devices Agency in September 2013 for treatment of stage 1 polyneuropathy in patients with hereditary ATTR amyloidosis. ATTR-ACT, a Phase III study on the impact of tafamidis on cardiac ATTR amyloidosis, started in December 2013.Citation31 The well-known different binding sites of tafamidis and EGCG suggest a synergistic effect.
This is an observational report on a relatively small, but well-sized, study cohort with respect to the prevalence of this disease. As green tea is widely available, of low cost, and, importantly, appears to have only minor side effects with long-term use, the potential for a placebo-controlled clinical trial is limited. Furthermore, EGCG capsules are over-the-counter products, and the broad spectrum of effects of EGCG, including amyloid fibril inhibition, has been well known for many years to most ATTR amyloidosis patients. Thus, we were not able to recruit a control group for the present study. None of the fatal events appeared to be associated with intake of GTE.
We assumed that the observed reduction of myocardial mass was due to reduction of amyloid load. Nevertheless, cell atrophy or hypotrophy might explain these findings as well. Further MRI studies demonstrated the use of a novel technique for tissue characterization, T1 mapping, for early diagnosisCitation32–Citation34 and prognosisCitation35 in different forms of cardiac amyloidosis. T1 mapping allows quantification of the extracellular volume fraction. Recently, reduction of extracellular volume by T1 mapping indicative of reduction of amyloid load has been demonstrated in a small cohort of patients with ATTR amyloidosis.Citation36 However, histopathological validation of this technique is lacking.
Conclusion
This study supports evidence for the benefit of EGCG to stabilize myocardial mass in wtATTR-CM patients. A reduction of myocardial mass was observed by cMRI, while echocardiographic data and cardiac biomarkers, however, remained unchanged during the study period of 1 year.
Acknowledgments
This study was financially supported by Dr. Loges & Co GmbH (Winsen, Germany) by providing the green tea capsules for the patients.
Disclosure
The authors report no conflicts of interest in this work. No payments were received. Dr. Loges & Co GmbH (Winsen, Germany) provided capsules of green tea extract and support to conduct the study, but were not involved in the study design, the analysis, or the interpretation of the results.
References
- ConnorsLHDorosGSamFBadieeASeldinDCSkinnerMClinical features and survival in senile systemic amyloidosis: comparison to familial transthyretin cardiomyopathyAmyloid201118Suppl 115715921838471
- PomeranceASenile cardiac amyloidosisBr Heart J19652757117185829755
- PolimantiRDi GirolamoMManfellottoDFuciarelliMIn silico analysis of TTR gene (coding and non-coding regions, and interactive network) and its implications in transthyretin-related amyloidosisAmyloid201421315416224779883
- CornwellGG3rdMurdochWLKyleRAWestermarkPPitkänenPFrequency and distribution of senile cardiovascular amyloid. A clinicopathologic correlationAm J Med19837546186236624768
- PinneyJHWhelanCJPetrieASenile systemic amyloidosis: clinical features at presentation and outcomeJ Am Heart Assoc201322e00009823608605
- LonghiSGuidalottiPLQuartaCCIdentification of TTR-related subclinical amyloidosis with 99mTc-DPD scintigraphyJACC Cardio-vasc Imaging201475531532
- MohtyDDamyTCosnayPCardiac amyloidosis: updates in diagnosis and managementArch Cardiovasc Dis20131061052854024070600
- RubergFLMaurerMSJudgeDPProspective evaluation of the morbidity and mortality of wild-type and V122I mutant transthyretin amyloid cardiomyopathy: the Transthyretin Amyloidosis Cardiac Study (TRACS)Am Heart J20121642222228.e122877808
- BieschkeJRussJFriedrichRPEGCG remodels mature alpha-synuclein and amyloid-beta fibrils and reduces cellular toxicityProc Natl Acad Sci U S A2010107177710771520385841
- EhrnhoeferDEBieschkeJBoeddrichAEGCG redirects amyloidogenic polypeptides into unstructured, off-pathway oligomersNat Struct Mol Biol200815655856618511942
- FerreiraNCardosoIDominguesMRBinding of epigallocatechin-3-gallate to transthyretin modulates its amyloidogenicityFEBS Lett2009583223569357619861125
- FerreiraNSaraivaMJAlmeidaMREpigallocatechin-3-gallate as a potential therapeutic drug for TTR-related amyloidosis: “in vivo” evidence from FAP mice modelsPLoS One201271e2993322253829
- KristenAVLehrkeSBussSGreen tea halts progression of cardiac transthyretin amyloidosis: an observational reportClin Res Cardiol20121011080581322584381
- HunsteinWEpigallocathechin-3-gallate in AL amyloidosis: a new therapeutic option?Blood20071106221617785589
- BensonMDTeagueSDKovacsRFeigenbaumHJungJKincaidJCRate of progression of transthyretin amyloidosisAm J Cardiol2011108228528921550574
- OgawaHSenile cardiac amyloidosis in senescence accelerated mouse (SAM)Jpn Circ J19885212137713833241319
- RapezziCMerliniGQuartaCCSystemic cardiac amyloidoses: disease profiles and clinical courses of the 3 main typesCirculation2009120131203121219752327
- KhuranaSVenkataramanKHollingsworthAPicheMTaiTCPolyphenols: benefits to the cardiovascular system in health and in agingNutrients20135103779382724077237
- SarmaDNBarrettMLChavezMLSafety of green tea extracts: a systematic review by the US PharmacopeiaDrug Saf200831646948418484782
- ObiciLMerliniGAn overview of drugs currently under investigation for the treatment of transthyretin-related hereditary amyloidosisExpert Opin Investig Drugs201423912391251
- KeskeMANgHLPremilovacDVascular and metabolic actions of the green tea polyphenol epigallocatechin gallateCurr Med Chem2015221596925312214
- ChungJHKimSLeeSJChungJOOhYJShimSMGreen tea formulations with vitamin C and xylitol on enhanced intestinal transport of green tea catechinsJ Food Sci2013785C685C69023551173
- PetersCMGreenRJJanleEMFerruzziMGFormulation with ascorbic acid and sucrose modulates catechin bioavailability from green teaFood Res Int20104319510220161530
- MerelesDBussSJHardtSEHunsteinWKatusHAEffects of the main green tea polyphenol epigallocatechin-3-gallate on cardiac involvement in patients with AL amyloidosisClin Res Cardiol201099848349020221615
- PerdrixLMansencalNCocheteuxBHow to calculate left ventricular mass in routine practice? An echocardiographic versus cardiac magnetic resonance studyArch Cardiovasc Dis2011104534335121693371
- BellengerNGBurgessMIRaySGComparison of left ventricular ejection fraction and volumes in heart failure by echocardiography, radionuclide ventriculography and cardiovascular magnetic resonance; are they interchangeable?Eur Heart J200021161387139610952828
- BellengerNGDaviesLCFrancisJMCoatsAJPennellDJReduction in sample size for studies of remodeling in heart failure by the use of cardiovascular magnetic resonanceJ Cardiovasc Magn Reson20002427127811545126
- BulawaCEConnellySDevitMTafamidis, a potent and selective transthyretin kinetic stabilizer that inhibits the amyloid cascadeProc Natl Acad Sci U S A2012109249629963422645360
- CoelhoTMaiaLFMartins da SilvaATafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trialNeurology201279878579222843282
- MerkiesISTafamidis for transthyretin familial amyloid polyneuropathy: a randomized, controlled trialNeurology201380151444144523569001
- UedaMAndoYRecent advances in transthyretin amyloidosis therapyTransl Neurodegener201431925228988
- BrooksJKramerCMSalernoMMarkedly increased volume of distribution of gadolinium in cardiac amyloidosis demonstrated by T1 mappingJ Magn Reson Imaging20133861591159523450747
- FontanaMBanypersadSMTreibelTANative T1 mapping in transthyretin amyloidosisJACC Cardiovasc Imaging20147215716524412190
- KaramitsosTDPiechnikSKBanypersadSMNoncontrast T1 mapping for the diagnosis of cardiac amyloidosisJACC Cardiovasc Imaging20136448849723498672
- MaceiraAMPrasadSKHawkinsPNRoughtonMPennellDJCardiovascular magnetic resonance and prognosis in cardiac amyloidosisJ Cardiovasc Magn Reson2008105419032744
- aus dem SiepenFBussSJAndreFExtracellular remodeling in patients with wild-type amyloidosis consuming epigallocatechin-3-gallate: preliminary results of T1 mapping by cardiac magnetic resonance imaging in a small single center studyClin Res Cardiol2015104864064725855392