
Abstract
Anaphylaxis is a serious, potentially fatal allergic reaction. Guidelines recommend prompt intramuscular injections of epinephrine as the first-line therapy for anaphylaxis. Delayed epinephrine treatment may cause undesirable clinical outcomes, including death. In the community, epinephrine auto-injectors (EAIs) are commonly used to treat anaphylaxis. This literature review examines several recent concerns regarding the safety of EAIs that may prevent the timely administration of epinephrine. Reports of cardiovascular complications are linked with epinephrine administration, although recent studies suggest that these events are much more commonly associated with intravenous epinephrine rather than with EAIs. Recent studies have also highlighted accidental injections of EAIs in patients’ or caregivers’ fingers and lacerations associated with the use of EAI in children. However, the data suggest that both accidental injections and lacerations are rare and require limited medical intervention. In addition, patients may receive conflicting information on the safety and efficacy of using expired EAIs. Overall, it is believed that the benefits of using EAIs far outweigh the potential risks of not administering an EAI. Although legitimate safety concerns are associated with EAIs, adverse events are rare. Continued training of medical providers, caregivers, and patients may be beneficial to address these concerns and reduce EAI-associated injuries while ensuring that patients receive necessary medical care.
Keywords:
Background
Anaphylaxis is a severe, acute, and potentially fatal allergic reaction that can develop within minutes of exposure to an immunologic trigger.Citation1,Citation2 Major medical groups recommend prompt intramuscular (IM) injection of epinephrine as the first-line therapy for anaphylaxis.Citation2–Citation5 Epinephrine auto-injectors (EAIs) can be used in the community for prompt delivery of epinephrine,Citation2 which is known to significantly improve outcomes in individuals experiencing anaphylaxis.Citation6–Citation8 Despite the potentially life-saving benefits of using EAIs, epinephrine is not used to treat the majority of anaphylactic reactions.Citation9 There are several reasons why EAIs are not administered, including lack of availability and concerns over safety.Citation9 Many parents have reservations about potentially using an EAI to administer epinephrine to their children due to concerns over injury, incorrect use, and poor outcomes.Citation10 Prevalent safety concerns regarding the use of EAIs include cardiovascular (CV) complications,Citation11–Citation13 accidental injections,Citation14–Citation16 laceration injuries,Citation17,Citation18 and the use of expired EAIs.Citation19 The present literature review provides an overview of anaphylaxis and discusses the safety concerns, highlighting the recent developments on their frequency, severity, and prevention.
Overview of anaphylaxis
Anaphylaxis is a serious allergic reaction that is rapid in onset and, in rare cases, may cause death.Citation1 Many immunologic triggers can induce an anaphylactic reaction, the most common being food, insect venom, and medication.Citation5,Citation20–Citation22 The rate of anaphylaxis appears to be increasing dramatically in the developed countries,Citation23,Citation24 which may partially be due to an increase in the prevalence of food allergies.Citation25 Individuals with a previous history of allergic reactions and asthma are at the greatest risk.Citation7,Citation22 However, anaphylaxis can commonly occur in those with no known history of allergy,Citation22 and triggers are never identified in many cases.Citation20–Citation22 Results from one study on a private allergy practice suggest that more than half of all the cases are idiopathic.Citation26 Accordingly, predicting who is at the greatest risk of a fatal reaction has been proven to be very difficult.Citation27
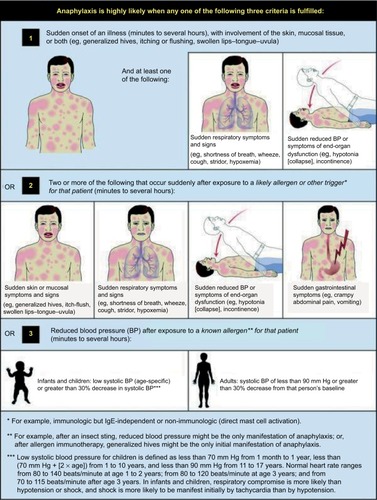
Anaphylactic reactions often occur within minutes of exposure to a trigger.Citation2 Triggers can induce reactions affecting multiple organs, including the skin, lungs, heart, and gastrointestinal system.Citation2,Citation21 Symptoms are diverse, including pruritus, hives, angioedema, breathing difficulties, abdominal pain, tachycardia, hypotension, and, potentially, cardiac arrest. Anaphylaxis is likely when one of three combinations of symptoms is observed ().Citation1,Citation2 Symptoms affecting the skin are the most common and easy to recognize but might not always be present.Citation2 As a wide range of organ systems are affected, the best therapies for anaphylaxis are those that can be used to treat all of the most serious symptoms.
Figure 1 Criteria that increase the likelihood of anaphylaxis.
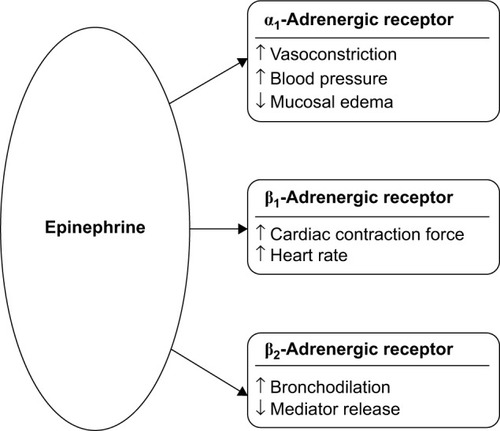
Guidelines from the World Allergy Organization and other major medical groups recommend prompt IM injection of epinephrine as the first-line therapy for anaphylaxis.Citation2–Citation5 Epinephrine is a naturally occurring ligand of adrenergic receptors, a broadly expressed class of G-protein-coupled receptors with distinct functions.Citation28 Through adrenergic receptor signaling, epinephrine has a variety of physiological effects ().Citation2,Citation29 Epinephrine induces vasoconstriction, increases blood pressure, and decreases mucosal edema through action on the α1-adrenergic receptor. Activation of the β1-adrenergic receptor increases cardiac output, whereas activation of the β2-adrenergic receptor increases bronchodilation and reduces immune mediator release. Thus, the administration of exogenous epinephrine can counteract some of the most severe symptoms of anaphylaxis.
Figure 2 Pharmacological effects of epinephrine in the treatment of anaphylaxis.
However, epinephrine may still be used less frequently than other medications for the treatment of anaphylaxis. Although the prehospital use of epinephrine for anaphylaxis is increasing,Citation30 a 2010 multicenter study of emergency departments found that half of the children with food-related anaphylaxis were never treated with epinephrine, and the majority were treated with antihistamines.Citation31 Similarly, results from a survey on anaphylaxis survivors treated in a community setting demonstrated that epinephrine was not administered in the majority of cases, and the use of antihistamines was listed as the most common reason for why epinephrine was not administered.Citation9 In contrast to epinephrine, antihistamines do not treat some of the most severe symptoms of anaphylaxis.Citation2,Citation29 H1-antihistamines (eg, diphenhydramine) can help relieve some of the skin and nasal symptoms of anaphylaxis, whereas H2-antihistamines (eg, ranitidine) may be effective in treating tachycardia and hives. However, antihistamines fail to treat many of the critical CV or pulmonary effects in a sufficiently timely manner. Antihistamines also have a relatively long time to onset of activity (0.7–3 h)Citation32 and time to peak plasma concentration (0.8–2.8 h)Citation33 and as such are not recommended as a first-line therapy for anaphylaxis.
Early use of epinephrine is associated with prevention of hypotension, decreased rates of hospitalization, and increased survival.Citation6–Citation8 In the community, epinephrine can be promptly delivered via an EAI.Citation2 EAIs can be self-administered or administered by another individual upon onset of symptoms. A report from a Chicago-area hospital suggests that prescriptions for EAIs are increasing,Citation30 as patients and providers are realizing the life-saving benefits of EAIs and importance of preparedness. Several brands of EAIs are currently available, with the EpiPen® Auto-Injector devices (Mylan Specialty L.P., Canonsburg, PA, USA) being the most widely prescribed, with a 90% EAI market share in the US.Citation18,Citation34,Citation35 Patients admitted in emergency departments for anaphylaxis were less likely to be hospitalized if they had filled an EAI prescription in the prior year. This suggests that prescribing EAIs may prevent hospitalizations in patients with anaphylactic reactions.Citation36 However, predicting who is at a risk of fatal anaphylactic reactions is difficult as the severity of previous reactions is not indicative of the severity of subsequent reactions.Citation27 Although epinephrine is an important, potentially life-saving, first-line therapy for anaphylaxis, there are several obstacles that may prevent someone from receiving timely epinephrine.
Major obstacles to prompt the administration of epinephrine in the community setting include both the availability of an EAI and accessibility of someone who has been trained to use an EAI. Results from a 2012 survey of US paramedics indicated that <40% of emergency response vehicles stocked EAIs.Citation37 In addition, many of these paramedics were unprepared to properly treat anaphylaxis, as 54% of patients were unable to correctly identify epinephrine as the first-line drug of choice for anaphylaxis. Similarly, severe allergic reactions can occur on commercial aircraft, sometimes requiring diversion.Citation38 Currently, the Federal Aviation Administration (FAA) does not require that airplane emergency medical kits contain epinephrine for the treatment of anaphylaxis, and the FAA recommends the use of oral antihistamines for the treatment of anaphylaxis.Citation39,Citation40 Ready availability of EAIs in school settings is also a major public health concern, as the prevalence of food allergies among children is increasing.Citation25 Anaphylactic events do occur in schools and have been frequently documented in students with no history of prior allergic reactions.Citation22,Citation41 However, some schools may not have stock EAIs available to students.Citation22
As accessibility in the community is lacking, important steps have been taken on multiple levels to make life-saving epinephrine more widely available. Currently, the National Association of Emergency Medical Services (EMS) physicians recommends that EMS providers be trained to recognize anaphylaxis and permitted to administer epinephrine in the field.Citation42 Recently, the US Senate introduced the Airline Access to Emergency Epinephrine Act, which, if passed, would require airlines to stock EAIs in their emergency medical kits.Citation43 Similarly, in 2013, the US Federal Government enacted the School Access to Emergency Epinephrine Act, which provides funding incentives to states that require schools to stock EAIs and to train staff to administer epinephrine.Citation44 State- and district-level policies are also being put into place to make stock epinephrine more widely available.Citation45,Citation46 In addition, the manufacturer of the EpiPen Auto-Injector, Mylan Specialty L.P., provides free EAIs to schools participating in the EpiPen4Schools® program.Citation22 More than 60,000 US public and private schools have participated in this program. Altogether, these legislative changes, policy implementations, and EAI stocking programs are working toward improving the treatment of anaphylaxis in the community and increasing access to EAIs.
However, even if EAIs are available, safety concerns may prevent them from being administered in some situations. Parents still have reservations about using EAIs to administer epinephrine to their children, citing concerns over injury, incorrect use, and poor outcomes.Citation10 These can include CV complications,Citation11–Citation13 accidental injections,Citation14–Citation16 laceration injuries,Citation17,Citation18 and the use of expired epinephrine.Citation19 The following sections discuss these safety concerns, highlighting the recent developments on their frequency, severity, and prevention.
CV complications
For decades, there have been reports on epinephrine administration resulting in severe, and sometimes fatal, CV complications.Citation11–Citation13 Epinephrine increases cardiac output through action on the β1-adrenergic receptors in the heart.Citation2 In addition, epinephrine induces vasoconstriction through the activation of the α1-adrenergic receptor. Due to the combination of vasoconstriction and increased cardiac output, several CV adverse events (AEs) could potentially occur after the administration of exogenous epinephrine, including myocardial ischemia, ventricular tachycardia, and myocardial infarction.Citation13
A recent literature review suggested that the majority of CV AEs seem to occur when epinephrine is administered via the intravenous (IV) route.Citation13 These results were subsequently supported by a study on emergency department patients that demonstrated that CV AEs occurred in 10% of patients with anaphylaxis who received epinephrine as an IV bolus.Citation12 In contrast, only 1.3% of patients presented with CV AEs when epinephrine was administered via IM injection, none of which were considered major. It is notable that the majority of serious CV AEs due to IV administration of epinephrine occurred in adults,Citation12,Citation13 suggesting that these events may be less common in children than in adults. Many of these CV complications occur when an excessive dose of epinephrine is administered.Citation12,Citation47 Epinephrine overdoses may result from confusion between the IM dose recommended for the treatment of anaphylaxis (0.3–0.5 mg of 1 mg/mL concentration [1:1,000]), the IV dose used for the treatment of anaphylactic shock (0.1 mg of 0.1 mg/mL concentration [1:10,000]), and the IV dose used for the treatment of cardiac arrest (1 mg of 0.1 mg/mL concentration [1:10,000]).Citation47 When tested, only 61% of doctors could correctly determine the volume of epinephrine required when the concentration and desired mass were given,Citation48 demonstrating how simple math miscalculations could result in a fatal dosing error. Results from an informal survey suggested that nearly all hospitals carried prefilled syringes of high dose of epinephrine appropriate for treating cardiac arrest while not carrying prefilled syringes of the dose used for the treatment of anaphylaxis.Citation47 In addition, confusion may arise from the use of ratios (eg, 1:1,000), percentages (eg, 0.1%), and metric units (eg, 1 mg/mL) to express concentrations of various drugs.Citation49 In order to help alleviate this uncertainty, the US Pharmacopeia and the National Formulary have issued new regulations no longer allowing the use of ratios to express concentrations of single-entity drug products, such as epinephrine. Accordingly, epinephrine concentrations are now to be expressed only in metric units. Although these changes may lead to fewer dosing errors in the long term, there is a concern that they may actually generate more confusion in the short term as providers adjust.Citation49 Thus, administration of epinephrine via a stock EAI, containing the correct dose, may help prevent CV complications resulting from dosing errors associated with IV delivery.
In addition to being recognized as generally safe, IM administration of epinephrine is regarded as an effective therapy for anaphylaxis.Citation2 Accordingly, guidelines indicate that IM administration of epinephrine should be used in all settings, except under extreme circumstances.Citation2–Citation5 It is even recommended that patients with underlying ischemic heart disease be administered epinephrine to treat an anaphylactic reaction as a decrease in filling pressure due to anaphylaxis can occur and result in the progression of ischemia.Citation50 However, a 2013 survey showed that although >90% of pediatric emergency physicians correctly identified epinephrine as the drug of choice for the treatment of anaphylaxis, only two-thirds correctly identified IM injection as the preferred route of administration.Citation51 Therefore, even in an emergency setting, there appears to be some lack of awareness of how to properly and safely treat anaphylaxis. The use of clearly labeled stock EAIs (“use only for anaphylaxis”) and prefilled syringes (“use only for cardiac arrest”) coupled with the circulation of a memo on proper administration of epinephrine has been successful in reducing AEs in a hospital setting.Citation47 Thus, simple policy changes and training may help reduce CV complications and overdoses when using epinephrine to treat anaphylaxis.
Accidental injections
Accidental injections of EAIs are a known concern that can occur under a variety of circumstances, such as when someone holds an EAI upside down and places his or her thumb on the tip during administration.Citation14–Citation16 A recent report shows that accidental injections can also occur when a child is playing with an EAI or confuses an actual EAI with a trainer device.Citation52 How commonly accidental injections of EAIs occur is unknown, but several reports suggest that the incidence of such events is increasing.Citation53,Citation54 In addition, the potential severity of these events has, until recently, been unclear.
As an agonist of the α1-adrenergic receptor in vascular smooth muscle, epinephrine induces vasoconstriction.Citation2 Through this mechanism, it is possible that accidental digital injection of epinephrine may cause local ischemia and subsequent tissue necrosis. There have been reports of accidental injections resulting in severe vasoconstriction, leading to amputation of a digit.Citation54 However, the frequency of digital tissue necrosis and permanent damage from accidental EAI injection has been called into question, as published reports of such events have been notably rare.Citation55 A 6-year retrospective study from the Texas Poison Center Network of 365 accidental injections showed that ischemia occurred in only 3.1% of the cases and completely resolved within 24 h in all the cases, without any complications (no patients were hospitalized, required surgery, or developed necrosis).Citation56 A systematic review also indicated that >99% of patients with accidental injections made a full recovery.Citation57 When necessary, the most frequently administered treatments for those requiring medical intervention included topical administration of nitroglycerin and subcutaneous administration of the α1-adrenergic receptor antagonist phentolamine.Citation16,Citation55,Citation56
Although the direct effects of accidental EAI injection are not usually serious, the loss of the dose required to treat the anaphylactic attack could be fatal.Citation53 Approximately 10% of accidental injections occurred while administering an EAI to another person.Citation53 In these cases, the person experiencing the anaphylactic attack may suffer delayed epinephrine administration. Although the scientific literature fails to provide much insight into the potential significance of the “lost dose hazard”, there was a media report of a child dying after a caregiver accidentally injected herself with an EAI.Citation58 An EAI 2 pack would allow for multiple doses to be on hand,Citation59,Citation60 which may help offset lost dose concerns.
The best way to alleviate safety concerns associated with accidental injection of EAIs is to ensure proper administration. Appropriate technique dictates that an EAI be held in the palm with the thumb covering the index finger ().Citation60,Citation61 If the thumb is placed on a tip, an accidental injection could occur, especially if the device is being held upside down. Patients and caregivers may think that the needle of an EAI will be located under the safety cap, but in some EAIs, the needle is located on the opposite end, which may cause users to hold the device upside down.Citation62,Citation63 Unfortunately, proper EAI administration technique is lacking at all levels. Among both food-allergic teenagers and parents of younger food-allergic children, only 38% were able to correctly demonstrate how to administer an EAI.Citation35 The pharmacists who dispense EAIs are often tasked with instructing patients on the use of EAIs. However, 35% of Australian pharmacists were unable to correctly demonstrate the most important steps in EAI administration, with 12% incorrectly placing their thumb over the end of the device.Citation64 Similarly, the majority of medical professionals in metropolitan Toronto did not hold an EAI correctly when demonstrating its use.Citation61 A study on general pediatric physicians in Turkey showed that when asked to simulate the administration of an EAI with a trainer device, 36% of them used a technique that may have caused self-injection into their own thumb.Citation65 However, after theoretical and practical training, the potential self-injection rate was reduced to 7%,Citation65 demonstrating the value of such training. Results from a study of interns with no prior EAI training demonstrated that EAI usage skills significantly decreased 6 months after initial training.Citation66 Thus, it is important that regular retraining of all those who may need to administer an EAI be emphasized, especially for medical providers who train patients and caregivers on appropriate techniques. In addition, advances in EAI technology may help prevent accidental injections. While older EAIs had exposed needles, some modern EAIs, like the recently redesigned EpiPen Auto-Injector, have been modified to help prevent accidental injections.Citation18,Citation67 These modifications include an orange needle sheath and a “needle end” label with a prominent arrow indicating proper orientation ().Citation60 Together, improved training and further device enhancements may prove beneficial in the prevention of accidental injections.
Figure 3 Self-administration of an epinephrine auto-injector.
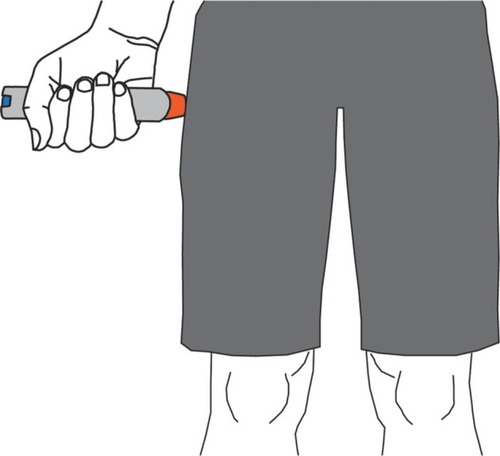
Figure 4 Comparison of the (A) old-look and (B) new-look (right) EpiPen® Auto-Injector (Mylan Specialty L.P., Canonsburg, PA, USA).

Laceration injuries
Recent publications by Brown et al have raised concerns over laceration and embedded-needle injuries resulting from the use of EAIs.Citation17,Citation18 These studies used social media and e-mail discussion groups to identify cases of injuries resulting from EAI use that occurred in North America. Together, they reported a total of 26 cases of laceration and embedded-needle injuries, 25 of which occurred when an adult was administering an EAI to a child under the age of 11.Citation17,Citation18 Of the reported incidents, only 12% required wound repair with sutures.Citation17,Citation18 Although images of such injuries may be startling, they are believed to be rare events, and the authors emphasized that they should not discourage the use of an EAI.Citation18 However, these reports provide helpful insight into the steps caregivers can take to prevent laceration and embedded-needle injuries when administering an EAI.
The majority of reported laceration injuries are the result of a child moving or jerking while epinephrine is being administered.Citation17,Citation18 This demonstrates the importance of properly restraining a child while administering an EAI. Recent studies have emphasized the importance of restraint and immobilization techniques ().Citation17 In addition, the prescribing information for the EpiPen Auto-Injector was recently updated to recommend that the caregiver hold the child’s leg firmly in place both before and during the injection.Citation60 In order to help prevent laceration injuries, it may be important to identify the most effective methods of restraint and communicate these techniques to those who may have to administer an EAI to an uncooperative child.
Figure 5 Proposed child restraint options for the administration of an epinephrine auto-injector.

Some laceration injuries could also be the result of a physician or caregiver trying to reinsert the needle after a child jerked free.Citation18 The EAIs available in North America have been prescribed with directions to insert the needle into the thigh and hold for 10 s to ensure full dose delivery.Citation18 Very recently, the prescribing information for the EpiPen Auto-Injector was changed to shorten the time of insertion to 3 s and to massage the injection site for an additional 10 s.Citation60 Epinephrine absorption should not be affected by this recommendation, as suggested by a study that used EAIs to inject epinephrine into beef.Citation68 This study indicated that there may not be an increase in epinephrine absorbed or dispensed past 1 s of injection. Thus, the new shortened injection time should improve the safety profile of EAIs, as laceration injuries have occurred after trying to reinsert a needle that has become dislodged in <10 s.Citation18 Another EAI that was formerly available had a needle that automatically retracted after injection to help prevent laceration injuries.Citation18 However, the actual benefits of shortened injection time and retractable needles remain unclear. While laceration injuries may be uncommon, it was agreed that more research and discussion are required on how to further prevent them.
Use of expired epinephrine
Epinephrine is an unstable chemical.Citation69,Citation70 Accordingly, EAIs have a relatively short shelf-life, and prescribing information states that they should be stored at 20°C–25°C (68°F–77°F).Citation59,Citation60 Once the expiration date has passed, the concentration and bioavailability of epinephrine in an EAI decrease over time.Citation69,Citation71 Similarly, epinephrine stored outside the recommended temperature range may not provide the labeled dose.Citation72
Many patients carry expired EAIs, which may be the only source of epinephrine available.Citation35 Recent literature suggests that physicians may give conflicting or inaccurate information regarding the safety and efficacy of expired EAIs. Some physicians highly emphasize the importance of keeping EAIs up to date.Citation73 In contrast, some patients have reported that health care professionals have advised them to ignore the expiration dates and that EAIs are safe to use unless they are cloudy or discolored.Citation19 However, significant degradation of epinephrine in an EAI can occur in the absence of discoloration or precipitation, indicating that appearance alone should not be used to determine whether an EAI is safe to use.Citation74 Other experts have suggested that if an expired EAI is the only source of epinephrine available to treat an anaphylactic event, it may be used as the risk of using a suboptimal dose of epinephrine potentially outweighs the risk of using no epinephrine at all.Citation69 There are instances where patients have died from anaphylactic attacks after having been administered epinephrine from an expired EAI.Citation75 Thus, in order to ensure proper treatment of anaphylaxis, it is believed that EAIs should always be replaced before they expire,Citation2,Citation69 and physicians should emphasize the importance of restocking expired EAIs to patients.
Discussion
Although epinephrine is an important, potentially life-saving, first-line therapy for anaphylaxis, concerns over safety may prevent someone from receiving timely epinephrine. One study revealed, for example, that a majority of parents of children with a peanut allergy and an epinephrine prescription are afraid of administering an EAI.Citation10 Commonly cited concerns included hurting the child, using the EAI incorrectly, and a bad outcome or death. This demonstrates that even parents with some level of training on EAI usage may have lingering concerns that affect their confidence in their ability to safely administer an EAI.
Although important efforts are being made with legislative and policy changes to increase the availability of EAIs,Citation42–Citation46 these alone are not enough, as people also need to be willing and able to safely use them. Multiple reports show that parents who had previously administered an EAI were more comfortable with using an EAI than those who had not.Citation10,Citation76 This suggests that overall familiarity with an EAI makes a parent more comfortable and perhaps more likely to administer an EAI during an emergency. Thus, regular hands-on training, perhaps in conjunction with yearly prescription renewals (which include placebo trainer devices), may be the most beneficial for helping to prevent injuries associated with EAI use, such as accidental injections and lacerations.
Addressing potential knowledge gaps for medical providers is also important. Medical providers need to be able to properly administer epinephrine to prevent CV AEs associated with epinephrine overdose and to train patients on the proper use of EAIsCitation61,Citation65 and the importance of replacing their EAIs before they expire.Citation73 While very basic training methods may be extremely beneficial in preventing epinephrine-associated injuries,Citation47,Citation65 recurring reminders on proper EAI use may also be valuable.Citation66 There are legitimate safety concerns with the administration of EAIs, but recent evidence shows that injuries are rare and typically not serious. Moreover, there is a broad agreement that these safety concerns are far outweighed by the benefits of prompt administration of an EAI to treat anaphylaxis.Citation5,Citation13,Citation18,Citation69
Acknowledgments
Editorial assistance was provided under the direction of the authors by Scott Houck, PhD, and Jennifer Rossi, MA, ELS, MedThink SciCom, and funded by Mylan Specialty L.P.
Disclosure
Dr Posner has served on the scientific advisory board for Mylan Specialty L.P. and Dr Camargo for Mylan Specialty L.P. and Sanofi-Aventis. Dr Posner and Dr Camargo performed investigator-initiated research funded by Mylan Specialty L.P. The authors report no other conflicts of interest in this work.
References
- SampsonHAMuñoz-FurlongACampbellRLSecond symposium on the definition and management of anaphylaxis: summary report–second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposiumAnn Emerg Med200647437338016546624
- SimonsFEArdussoLRBilòMBWorld allergy organization guidelines for the assessment and management of anaphylaxisWorld Allergy Organ J201142133723268454
- MuraroARobertsGWormMAnaphylaxis: guidelines from the European Academy of Allergy and Clinical ImmunologyAllergy20146981026104524909803
- SoarJPumphreyRCantAEmergency treatment of anaphylactic reactions – guidelines for healthcare providersResuscitation200877215716918358585
- NIAID-Sponsored Expert PanelBoyceJAAssa’adAGuidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panelJ Allergy Clin Immunol20101266 SupplS1S5821134576
- KoBSKimJYSeoDWShould adrenaline be used in patients with hemodynamically stable anaphylaxis? Incident case control study nested within a retrospective cohort studySci Rep201662016826837822
- BockSAMuñoz-FurlongASampsonHAFurther fatalities caused by anaphylactic reactions to food, 2001–2006J Allergy Clin Immunol200711941016101817306354
- FlemingJTClarkSCamargoCAJrRuddersSAEarly treatment of food-induced anaphylaxis with epinephrine is associated with a lower risk of hospitalizationJ Allergy Clin Immunol Pract201531576225577619
- SimonsFEClarkSCamargoCAJrAnaphylaxis in the community: learning from the survivorsJ Allergy Clin Immunol2009124230130619540575
- ChadLBen-ShoshanMAsaiYA majority of parents of children with peanut allergy fear using the epinephrine auto-injectorAllergy201368121605160924410784
- CarterBTWestfallVKHeironimusTWAtukNOSevere reaction to accidental subcutaneous administration of large doses of epinephrineAnesth Analg19715021751785102629
- CampbellRLBellolioMFKnutsonBDEpinephrine in anaphylaxis: higher risk of cardiovascular complications and overdose after administration of intravenous bolus epinephrine compared with intramuscular epinephrineJ Allergy Clin Immunol Pract201531768025577622
- WoodJPTraubSJLipinskiCSafety of epinephrine for anaphylaxis in the emergency settingWorld J Emerg Med20134424525125215127
- PeykoVCohenVJellinek-CohenSPPearl-DavisMEvaluation and treatment of accidental autoinjection of epinephrineAm J Health Syst Pharm201370977878123592360
- CarrascosaMFGallastegui-MenéndezATeja-SantamaríaCSalcines CaviedesJRAccidental finger ischaemia induced by epinephrine autoinjectorBMJ Case Rep20132013
- BodkinRPAcquistoNMGunyanHWiegandTJTwo cases of accidental injection of epinephrine into a digit treated with subcutaneous phentolamine injectionsCase Rep Emerg Med2013201358620724024046
- BrownJCTuuriRELacerations and embedded needles due to EpiPen use in childrenJ Allergy Clin Immunol Pract20164354955126897302
- BrownJCTuuriREAkhterSLacerations and embedded needles caused by epinephrine autoinjector use in childrenAnn Emerg Med201667330731526452720
- MoneyAGBarnettJKuljisJLucasJPatient perceptions of epinephrine auto-injectors: exploring barriers to useScand J Caring Sci201327233534422834703
- HuangFChawlaKJärvinenKMNowak-WęgrzynAAnaphylaxis in a New York City pediatric emergency department: triggers, treatments, and outcomesJ Allergy Clin Immunol2012129116216822018905
- WoodRACamargoCAJrLiebermanPAnaphylaxis in America: the prevalence and characteristics of anaphylaxis in the United StatesJ Allergy Clin Immunol2014133246146724144575
- WhiteMVHogueSLBennettMEEpiPen4Schools pilot survey: occurrence of anaphylaxis, triggers, and epinephrine administration in a U.S. school settingAllergy Asthma Proc201536430631225898241
- PoulosLMWatersAMCorrellPKLoblayRHMarksGBTrends in hospitalizations for anaphylaxis, angioedema, and urticaria in Australia, 1993–1994 to 2004–2005J Allergy Clin Immunol2007120487888417931562
- RuddersSAAriasSACamargoCAJrTrends in hospitalizations for food-induced anaphylaxis in US children, 2000–2009J Allergy Clin Immunol2014134496096225109801
- BranumAMLukacsSLFood allergy among children in the United StatesPediatrics200912461549155519917585
- WebbLMLiebermanPAnaphylaxis: a review of 601 casesAnn Allergy Asthma Immunol2006971394316892779
- PumphreyRAnaphylaxis: can we tell who is at risk of a fatal reaction?Curr Opin Allergy Clin Immunol20044428529015238794
- LodishHBerkAZipurskySLMatsudairaPBaltimoreDDarnellJG protein–coupled receptors and their effectorsMolecular Cell Biology4th edNew YorkW.H. Freeman2000 Section 20.3
- FinemanSMOptimal treatment of anaphylaxis: antihistamines versus epinephrinePostgrad Med201412647381
- FuzakJKTrainorJComparison of the incidence, etiology, and management of anaphylaxis over timePediatr Emerg Care201329213113523364374
- RuddersSABanerjiACorelBClarkSCamargoCAJrMulticenter study of repeat epinephrine treatments for food-related anaphylaxisPediatrics20101254e711e71820308215
- SimonsFEFirst-aid treatment of anaphylaxis to food: focus on epinephrineJ Allergy Clin Immunol2004113583784415131564
- SimonsFEAdvances in H1-antihistaminesN Engl J Med2004351212203221715548781
- KuMSRecent trends in specialty pharma business modelJ Food Drug Anal2015234595608
- SichererSHFormanJANooneSAUse assessment of self-administered epinephrine among food-allergic children and pediatriciansPediatrics2000105235936210654956
- ClarkSWeiWRuddersSACamargoCAJrRisk factors for severe anaphylaxis in patients receiving anaphylaxis treatment in US emergency departments and hospitalsJ Allergy Clin Immunol201413451125113024985399
- JacobsenRCToySBonhamAJSalomoneJAIIIRuthstromJGrattonMAnaphylaxis knowledge among paramedics: results of a national surveyPrehosp Emerg Care201216452753422712745
- PetersonDCMartin-GillCGuyetteFXOutcomes of medical emergencies on commercial airline flightsN Engl J Med2013368222075208323718164
- NableJVTupeCLGehleBDBradyWJIn-flight medical emergencies during commercial travelN Engl J Med20153731093994526332548
- Federal Aviation Administration, Department of TransportationEmergency medical equipment. Final ruleFed Regist20016671190281904611708364
- McIntyreCLSheetzAHCarrollCRYoungMCAdministration of epinephrine for life-threatening allergic reactions in school settingsPediatrics200511651134114016264000
- National Association of EMS PhysiciansThe Use of Epinephrine for Out-of-hospital Treatment of AnaphylaxisLenexa, KSNational Association of EMS Physicians2011
- Airline Access to Emergency Epinephrine Act of 2015, S 1972, 114th Cong, 1st Sess (2015).
- US Public LawSchool Access to Emergency Epinephrine Act. Pub L No. 113–48, 127; Statute 57511132013
- ZadikoffEHWhyteSADeSantiago-CardenasLHarvey-GintoftBGuptaRSThe development and implementation of the Chicago Public Schools emergency EpiPen® policyJ Sch Health201484534234724707929
- The Network for Public Health LawSummary Matrix of State Laws Addressing Epi-Pen Use in SchoolsSt Paul, MNThe Network for Public Health Law2015
- KanwarMIrvinCBFrankJJWeberKRosmanHConfusion about epinephrine dosing leading to iatrogenic overdose: a life-threatening problem with a potential solutionAnn Emerg Med201055434134420031267
- RolfeSHarperNJAbility of hospital doctors to calculate drug dosesBMJ19953106988117311747767153
- PaparellaSFSay goodbye to confusing ratio expressionsJ Emerg Nurs201642543143327594076
- McLean-TookeAPBethuneCAFayACSpickettGPAdrenaline in the treatment of anaphylaxis: what is the evidence?BMJ200332774271332133514656845
- GrossmanSLBaumannBMGarcia PeñaBMLinaresMYGreenbergBHernandez-TrujilloVPAnaphylaxis knowledge and practice preferences of pediatric emergency medicine physicians: a national surveyJ Pediatr2013163384184623566384
- SasakiKNakagawaTSugiuraSKandoNItoKAccidental usage of an adrenaline auto-injector in Japanese children with a food allergyAllergol Int201665334935026987410
- SimonsFELiebermanPLReadEJJrEdwardsESHazards of unintentional injection of epinephrine from autoinjectors: a systematic reviewAnn Allergy Asthma Immunol2009102428228719441598
- SimonsFEEdwardsESReadEJJrClarkSLiebeltELVoluntarily reported unintentional injections from epinephrine auto-injectorsJ Allergy Clin Immunol2010125241942320159254
- Fitzcharles-BoweCDenklerKLalondeDFinger injection with high-dose (1:1,000) epinephrine: does it cause finger necrosis and should it be treated?Hand (N Y)20072151118780041
- MuckAEBebartaVSBorysDJMorganDLSix years of epinephrine digital injections: absence of significant local or systemic effectsAnn Emerg Med201056327027420346537
- WrightMTreatment after accidental injection with epinephrine auto-injector: a systematic reviewJ Allergy Ther201453175
- AzziMMother reveals the heartbreaking story of how her son died at school due to his peanut allergy despite it’s ‘nut-free policy’ – and how the teacher stabbed the EpiPen into her own hand instead of little AlexDaily Mail201592 Available from: http://www.dailymail.co.uk/news/article-3219624/Mother-reveals-heartbreaking-moment-called-son-s-kindergarten-told-died-peanut-allergy-despite-school-nut-free.htmlAccessed March 8, 2016
- Adrenaclick® (epinephrine injection USP) auto-injector [package insert]Horsham, PAAmedra Pharmaceuticals LLC2013
- EpiPen® (epinephrine injection) Auto-Injector [package insert]Morgantown, WVMylan Specialty L.P.2016
- GrouhiMAlshehriMHummelDRoifmanCMAnaphylaxis and epinephrine auto-injector training: who will teach the teachers?J Allergy Clin Immunol1999104119019310400860
- LeeJThe role of metaphor in design: impact on health outcomesMedium Available from: https://medium.com/@joyclee/the-role-of-metaphor-in-design-cd6d8f04daab#.yb0oqje6zAccessed December 5, 2016
- FrewAJWhat are the ‘ideal’ features of an adrenaline (epinephrine) auto-injector in the treatment of anaphylaxis?Allergy2011661152420716315
- SalterSMLohRSanfilippoFMCliffordRMDemonstration of epinephrine autoinjectors (EpiPen and Anapen) by pharmacists in a randomised, simulated patient assessment: acceptable, but room for improvementAllergy Asthma Clin Immunol20141014925264449
- ArgaMBakirtasACatalFTraining of trainers on epinephrine autoinjector usePediatr Allergy Immunol201122659059321309857
- TopalEBakirtasAYilmazOKaragolIHArgaMDemirsoyMSTurktasIWhen should we perform a repeat training on adrenaline auto-injector use for physician trainees?Allergol Immunopathol (Madr)201442547247524176470
- GuerlainSWangLHugineAIntelliject’s novel epinephrine auto-injector: sharps injury prevention validation and comparable analysis with EpiPen and TwinjectAnn Allergy Asthma Immunol2010105648048421130387
- BakerTWWebberCMStolfiAGonzalez-ReyesEThe TEN study: time epinephrine needs to reach muscleAnn Allergy Asthma Immunol2011107323523821875542
- SimonsFEGuXSimonsKJOutdated EpiPen and EpiPen Jr autoinjectors: past their prime?J Allergy Clin Immunol200010551025103010808186
- ChurchWHHuSSHenryAJThermal degradation of injectable epinephrineAm J Emerg Med19941233063098179736
- RachidOSimonsFEWeinMBRawas-QalajiMSimonsKJEpinephrine doses contained in outdated epinephrine auto-injectors collected in a Florida allergy practiceAnn Allergy Asthma Immunol2015114435435625707326
- RachidOSimonsFERawas-QalajiMLewisSSimonsKJEpinephrine doses delivered from auto-injectors stored at excessively high temperaturesDrug Dev Ind Pharm20164213113525997362
- BennettJRFromerLHaydenMLAnaphylaxis challenges on the front line: perspectives from community medicineAm J Med20141271 SupplS25S33
- ParishHGBowserCSMortonJRBrownJCA systematic review of epinephrine degradation with exposure to excessive heat or coldAnn Allergy Asthma Immunol20161171798727221065
- PumphreyRSGowlandMHFurther fatal allergic reactions to food in the United Kingdom, 1999–2006J Allergy Clin Immunol200711941018101917349682
- KimJSSinacoreJMPongracicJAParental use of EpiPen for children with food allergiesJ Allergy Clin Immunol2005116116416815990790