Abstract
Background
Drug therapy is the most often used intervention for treatment and prevention of disease. However, if used inappropriately, drugs can cause more harm than good. Improper drug storage and disposal can have a direct impact on public safety, the environment, and the health care services. The purpose of this study was to characterize medications stored in Qatar homes and to explore their methods of storage and disposal, and to identify the public’s source of information related to medicines.
Methods
For the purpose of this cross-sectional exploratory study, a list of telephone numbers was generated from Qatar’s telephone directory using a systematic sampling method. Individuals consenting to participate were interviewed using a multipart pretested survey instrument.
Results
Data were collected from a total of 49 homes. Most respondents did not have a designated compartment or box specifically for storing medications. The majority of drugs (48%) were kept in bedrooms and a number of respondents were keeping their drugs in the fridge and in the kitchen. The most often stored classes of medicines were analgesics, antihistamines, nutritional supplements, and medications used for the respiratory system. Most respondents disposed of unwanted medicines by throwing them in the trash. In about 15% of cases, the dosage of drug taken was different from the instructions on the label. Sharing of prescription medicines was not uncommon. The majority of respondents sought information related to drugs from doctors.
Conclusion
These findings raise concerns about how medications are stored and disposed of in the community. The fact that no household routinely returned unwanted medications to a pharmacy for proper disposal places the environment at risk. There is a need for more societal awareness about the safe handling and storage of drugs in the home, and about the professional role of the pharmacist.
Keywords:
Introduction
Drug therapy is often associated with adverse effects and other drug-related problems that can generate increased health care costs, including a need for new consultations with other health care professionals, use of additional drugs, need for more laboratory tests, hospitalization, and even death.Citation1 It has been estimated that for each dollar spent on drugs, one dollar is needed for the treatment of problems related to drugs.Citation2 All this means that medicines can have significant adverse consequences at a societal level, in addition to having an economic impact on the health care system.Citation3
Studies conducted in Spain, the UK, and the US have reported that elderly patients tend to have more medications in their homes, and a larger household size was found to be predictive of storage of more medications.Citation4–Citation6 A study conducted in Saudi Arabia found a mean of eight drugs per household, and up to 30% had at least 10 medications.Citation7
Medications stored in the home are sometimes taken by someone other than the person for whom they are prescribed. A study conducted in 2001 found that 3%–12.7% of people had shared their medications with someone else.Citation8 The same study reported high use of nonprescription medications and dietary supplements among households, and reported simultaneous use of multiple products with the same active ingredient (duplicate therapy).
Hoarding of old medications is not uncommon. It was reported that around 40% of patients had prescription medications that they no longer used.Citation9 Storage of large quantities of medications in the home increases the risk of a wide range of potential drug-related problems, including errors in taking medications, accidental poisoning, adverse drug reactions, and is also a waste of resources.Citation10 While historically patients may have been advised to flush unwanted medications down the toilet, many studies have shown that chemicals are increasingly present in waterways, eg, streams, rivers, and lakes. Pharmaceuticals inappropriately discarded in this manner could contaminate water supplies and threaten aquatic ecosystems.Citation11
No previous study has examined what and how medications are stored in Qatar homes. A number of key issues must be considered before trying to apply the findings of studies conducted overseas to Qatar, a multiethnic country with a population of around 1,600,000, as per Qatar’s Statistics Authority website (http://www.qsa.gov.qa/eng/index.htm). One such issue is the pharmacy regulations governing the sale, classification, prescribing, and dispensing of medications (and ultimately public access to medications and the potential hazards associated with that access). In most countries, drugs are classified mainly according to whether they are available on prescription only and are sold over-the-counter (OTC). Classification to prescription or OTC is mainly based on the safety and efficacy of the product and its potential for abuse by the patient. This classification has direct implications for the level of access to medications and subsequently the potential impact on public safety. Many countries limit the list of OTC medicines to those with a proven safety profile, while extending the prescription only list to include all medications that could be potentially harmful. Other countries limit the prescription medication list, while making a longer list of OTC products available. This reflects the current situation in Qatar, which is not helped by the public’s poor understanding of the role of the community pharmacist in providing drug information and by insufficient pharmacist–patient time, as reported by a recent study in Qatar.Citation12 This study seeks to explore these relationships by characterizing medications kept in Qatar homes, specifically drug quantity, therapeutic class, sale class, usage, method of storage, method of disposal, and expiry status.
Materials and methods
This was a cross-sectional, exploratory descriptive study. To identify households for inclusion in the study, a list of home telephone numbers was selected randomly from the telephone directory maintained by Qtel®, Qatar’s national telephone company. Random telephone numbers were dialed and all adults responding to the call and identifying themselves as the person most involved with the household medicine stock or cabinet were invited to take part in this voluntary anonymous survey. In the absence of an institutional review board in Qatar at the time of conducting this study, verbal consent was obtained from participants prior to administering the interviews.
Questionnaire design
Several meetings were held and the literature was searched to help in developing a comprehensive survey tool for collecting the necessary data from the sample. A literature search was conducted using the Medline, Embase, and Cinahl databases and the search engines of relevant journals. Search terms included: “medicine”, “drug”, “medication”, “pharmaceutical preparations”, “prescription”, “over the counter”, “non-prescription”, “medicine cabinet”, “medicine cupboard”, “home”, “storage”, “self-medication”, “drug stability”, “drug wastage”, “expiry”, and “brown bag”. Limits used to narrow down the number of studies returned included human and English language studies only. Articles that had reviewed the storage of medicines in homes were identified, and their findings were examined. Where possible, their methods were looked at to determine how the research had been conducted. Following the literature review, the interview format was determined and a set of forms was assembled. The forms were designed to enable gathering of information that addressed the specific aims of the research and included common questions drawn from the literature. Areas that were targeted by the survey included the types of medicine that were stored, their quantities, what condition they were in, how they were used and who they were used by, whether they were stored and used safely and correctly, and how they were disposed of. Other information gathered included usage of the medicines in relation to the instructions for use on their label, the source of most information related to drugs, and degree of satisfaction with the information received. The knowledge people had regarding their medicines was also briefly examined.
The method of data collection was a 25–30-minute structured telephone interview carried out by two research assistants. The forms were piloted with a small sample of participants, and minor modifications to the structure and wording of the questionnaires were made as a result. Face validity and comprehension of the questionnaire were tested (time taken to respond to the questionnaire, comprehension, and response to questions of a “personal” nature).
Data collection
For the purpose of the study, randomly selected telephone numbers were dialed, and individuals answering calls were provided with the study objectives, and asked if they (or someone else whom they identified as someone with the best knowledge about medicines at the house) wished to participate. Those who gave their verbal consent were interviewed at a second call after giving them time to prepare all the medications stored at the house, including vitamins, minerals, and herbal products. A semistructured interview was conducted in Arabic or English using the multipart pretested survey instrument. Questions were asked in lay language and in Arabic or English depending on the language preferred by the respondent. Medication names were collected by asking the respondent to read or spell out the name written on the packaging or container, and if necessary, the interviewer assisted the respondent until the interviewer was satisfied that the correct name of the medicine was collected. In the event of the availability of commercial names only, the generic name or composition was identified by referring to drug information sources available throughout the data collection process, including text books (British National Formulary, Drug Information Handbook) or online software (Micromedex, http://www.thomsonhc.com/home/dispatch). After identifying the medication, a member of the research team placed the medicines under its appropriate drug class (as per the British National Formulary classification) for further analysis.Citation13
Statistical analysis
The data collected were entered into Excel® (Microsoft Corporation, Redmond, WA) then exported to SPSS (v 17.0; SPSS® Inc, Chicago, IL). Data were entered by two independent junior researchers for validation and accuracy purposes. Descriptive statistical analyses and group comparisons were carried out using correlation statistics and multiple regression analysis. The Pearson correlation coefficient was used to determine any association between demographic data and other variables identified a priori (like the association between household size, annual income, level of education, age, ethnicity, and the method used to dispose of unwanted medications or how and where medications were stored in the home). Student’s t-test was used to assess statistical significance (P ≤ 0.05).
Results
Household characteristics
Four hundred and thirty-two phone calls were made to invite respondents to take part in the study. Eighty-one household representatives initially expressed interest in being part of the research during the first call, of whom 49 participants (18% of the targeted sample size) answered all survey questions.
Demographics of respondents
Eighteen percent of the respondents (n = 9) were of Qatari nationality. Respondents from other Arabic origins were the highest group (39%), followed by people of Asian background (35%). Those of European background comprised only 2% of the sample. Eighty percent of those responding to phone calls and ultimately responding to the survey were females. The majority of people living in the surveyed homes were in the 19–59-year age bracket (). Around 13% (35/262) of the sample living in the houses surveyed were aged 5 years or younger. There were only three individuals aged 60 years or older. Fifty-one percent of the households accommodated 2–4 persons, while 41% had fewer than ten persons living in them. The rest of the households had ten persons or more living in them (). Around 37% of respondents were unemployed (eg, housewives or retired persons). There was no statistical association between household income and quantity of drugs kept in the home (P = 0.08).
Figure 1 Age distribution of the residents in all houses surveyed (n = 265).
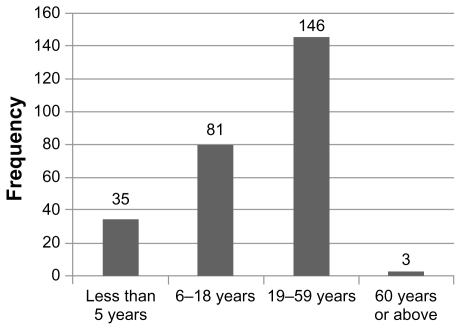
Table 1 Number of people living in the household (n = 49)
Drugs in home
Pharmacological class
Participants were asked to answer questions related to each drug stored in the household. The average (± standard deviation) number of medicines per household was 6.0 ± 4.1. The total number of drugs stored in the home was greater as the number of people living in the house increased (P < 0.05). The majority of the drugs stored (n = 58; 21%) in the participating homes were analgesics. Nonsteroidal anti-inflammatory drugs were the second most commonly stored drugs, representing 16% of all the drugs (). There were 86 prescription drug products and 167 OTC drug products. summarizes the distribution of drugs as per their sale category.
Table 2 Drug distribution by class (n = 278)
Table 3 Drugs per sale category (n = 278)
Participants were also asked about whether medicinal products were shared amongst residents in the same house. Sharing occurred with antidiabetic medicines (two households; 4%), anti-infective medications (seven households; 14%), inhaled bronchodilators (three households; 6%), inhaled corticosteroids (one household; 2%), and oral corticosteroid medication (two households; 4%). In around 15% of cases, medicines were used in dosage regimens that were different from that in the labeling on the medicine’s containers.
Child-resistant closures
When participants were asked about whether the bottles containing liquid dosage forms (eg, syrups and suspensions) or solid dosage forms (eg, loose tablets or capsules) were fitted with child-resistant closures, only 29% confirmed that the drug containers had a child-resistant closure. The rest were in containers with bottles fitted with normal screw caps or in paper or plastic envelopes.
Storage
Participants were asked about where each of their household drugs was stored. The majority of drugs (48.2%) were kept in bedrooms. Most respondents did not have a designated compartment or box specifically for storing medications. A number of respondents kept their drugs in the fridge or kitchen. summarizes drug storage sites in the home.
Table 4 Drug storage sites in the home (n = 253)
Disposal
When participants were asked about how they disposed of their unwanted or leftover medicines, the majority (65%) reported that they threw them in the general rubbish. Around 12% said they usually threw their unused medicines in the rubbish or kept them. Only 4% reported that they kept unused medicines indefinitely, and 6% flushed them down the toilet. The answers of the remaining participants varied between returning the drug to the pharmacy, or using a combination of methods to dispose of their unused medicines. No expired medications were reported.
Sources of satisfaction with drug-related information
Physicians were cited as the most important source of drug-related information for the participants (49%). Only 6.1% and 4.1% of the participants reported pharmacists and nurses as their main source of drug-related information, respectively.
Discussion
The research question addressed in this project (ie, how medicines are stored in the home) is not novel, but is an important one that relates directly to issues of public safety. What makes this an even more important issue to be addressed in the State of Qatar is the fact that regulations that organize pharmaceutical products in terms of approval, classification, provision, and use (in other words the drug use process) are still in a stage of development and evolution. Therefore, the focus of community and other pharmacists is still on instructing patients on how to take the prescribed drug at the prescribed dose for the prescribed time. What is often overlooked is what the patient and caregivers, who have the ultimate responsibility for proper drug use, do with these medications at home.Citation14
It had been reported that the public is generally dissatisfied with current medication use conditions in Qatar, particularly the availability and cost of medications in the private sector.Citation13 These findings might have implications, in our opinion, for the types, range, and quantities of medications stored in private homes in Qatar, and on how people dispose of their unused medicines and where (and how) they store them. Therefore, this exploratory study looked at the status of medicines in a cross-sectional sample of homes in Qatar with the intention of making some inferences about the possible overall impact on public safety and on potential roles of health care workers, including pharmacists, in health promotion and health education.
A telephone interview strategy was adopted in this study. We have had other options that included face-to-face interviews and distributing the questionnaires to parents through their children in schools. Both of these methods were disregarded for different reasons. For example, home visits to collect information were excluded on the grounds of cultural sensitivity and school visits would miss potential participants with no children of school age. The utilization of Qatar’s national telephone directory as the source for our sample seemed logical because it included an updated list of all telephone numbers, and it allowed adequate randomization. However, of all the telephone calls made, only a small fraction of those who answered our calls in which we explained the aim of the study agreed to participate, and finally 11% of all those who were invited to participate (which translates to 18% of the target sample size) did complete the phone survey. This response rate illustrates the difficulty of conducting population-based surveys in Qatar, especially surveys that utilize telephone calls and probably also postal questionnaires. One would be justified in expecting better response rates with surveys that target professional groups or similar defined groups of candidates than those targeting the general population.
In our case, one reason for the poor response rate may have been a reluctance to answer questions related to medications or medical conditions of a sensitive and private nature. Also, there might have been a reluctance to participate in a telephone interview that might take too long, which again may have deterred some individuals. O’Toole et al advocated the use of a combination of approaches to maximize telephone response rates.Citation15 Factors like reduced telephone number listings and people’s increasing resistance to unwanted phone calls could also compromise the response rate to telephone interviews. However, for an exploratory study like this one, sample size is not an issue because the aim in this case is not to provide results that could be generalizable, but to provide a snapshot in time and some insight into the phenomenon of home drug storage.Citation16
Participant demographics
Analysis of respondent demographics reveals a multiethnic mixture including different proportions of the main ethnicities that form Qatar’s population, and bears a close resemblance to the actual situation in Qatar. The sample population also showed reasonable diversity with respect to age, gender, and ethnicity. However, because of the small sample size, we cannot claim that the data generated is representative of the whole population in Qatar. Indeed, as stated above, generalizability was not our main objective in this work.
The majority of those who responded to the survey were female, which is not surprising given that phone calls were often made at a time of the day when employed spouses or other individuals were not at home. Over 40% of respondents lived in houses with 5–10 other members in the same household. This could be a reflection of the social makeup and living arrangements involving extended family in this part of the world. This is an important finding with relevance to the core of this study, whereby we found an association between number of members in the household and quantity of medicines stored. While this is to be expected, it could also raise concern about the increased potential for drug-related risks.
Some participants did not feel comfortable answering questions about income, which is not surprising because this could justifiably be perceived as sensitive and personal information. Reluctance to answer the income question might have been driven by the nature of the survey provision strategy, where a phone call could be seen as somewhat intrusive and the respondent could be feeling “exposed”, unlike a postal questionnaire that carries no personal information, address, contact number, or a human voice.
Quantities of medicines in homes
The mean number of medications stored in the home was six per household. This number is comparable with the average number of medications stored at home in other countries, like Sudan, where the mean number of medications reported per household unit is 4.4, and like Saudi Arabia, where the mean number of reported medications is 8.0 per family.Citation7,Citation17 Household income does not appear to have an association with quantity of medicine stored in the household. This simply suggests that people do not seem to keep or purchase more medications as their income increases. However, due to the perceived sensitivity of the information, these results should be considered with caution.
The most frequently stored medications at home in this country were analgesics (21%) followed by nonsteroidal anti-inflammatory drugs (16%), and allergy, cough, and cold medications (14%). This finding is consistent with the results of some studies conducted in other countries but is in contrast with others. For example, De Bolle et al reported that the most commonly encountered categories of medicines in Belgium are nonopioid analgesics (7.2%), nonsteroidal anti-inflammatory drugs (6.9%), and nasal decongestants (3.5%).Citation18 In the Sudanese study cited earlier, the most commonly stored medicines found at home in Sudan were antibiotics (22%) followed by analgesics (12%).Citation17 Abou-Auda found that respiratory drugs, followed closely by central nervous system agents, and antibiotics, were the most common medicines in Saudi Arabian households (16.8%, 16.4%, and 14.3%, respectively).Citation7 In Iran, drugs acting on the central nervous system were the most commonly encountered medications (23.7%) followed by anti-infectives (14%) and gastrointestinal agents (13%).Citation19 We have intentionally considered analgesics (eg, paracetamol, opioids) as a category distinct from nonsteroidal anti-inflammatory drugs because the latter class is considered especially problematic due to the potential for causing gastrointestinal bleeding, ulcers, and several cardiovascular complications.Citation20–Citation22
The low percentage of anti-infectives (6%) found in Qatar’s households could be explained by the fact that Qatar’s drug regulations prohibit the dispensing of anti-infectives without a prescription which would limit public access to this category of medications.
In spite of the fact that cardiovascular disease accounts for a significant percentage of hospital admissions in Qatar and is the leading cause of death in that country, only 6% of stored medications were cardiovascular agents.Citation21 This could be explained by the relatively young age of people living in the homes surveyed (only three individuals were above 60 years of age). Another explanation could be that people are not likely to self-medicate with cardiovascular medicines. Noteworthy is the fact that access to these medicines is so far not restricted in Qatar (medicines for cardiovascular health problems can be sold freely in community pharmacies). However, most patients are prescribed these medicines at health care centers and hospitals.
The high number of allergy, cough, and cold products found in Qatar’s households (14% of the total number of medicinal products) could be due to the high prevalence of allergic disorders in this country, especially among school-aged children.Citation23
Safety of packaging
Safety of medicine packaging is a universal problem and concern had been expressed over accidental poisoning as a result of poor packaging. It has been suggested that education does not reduce accidental poisoning as safety packaging does, which could explain why it is most prevalent among children, especially those without adult supervision.Citation24 Only one-third of the drug products stored in the households surveyed were fitted with a child-resistant closure. We asked specifically about child-resistant closures if the medication was a solid dosage form (tablets, capsules) or a liquid (syrup, suspension, elixir). The fact that 13% of all residents in the houses surveyed were children (5 years or younger) makes this finding of considerable importance and raises concerns about the potential for accidental child poisoning. The problem is compounded by our other finding related to the manner in which medications were stored in the homes we surveyed.
Place of storage
Previous studies have identified a link between where people store their medicine and how frequently the drug is used.Citation25,Citation26 They found that medicines for everyday use are often kept in places where they can be seen, such as the kitchen bench, while the “when required” medicines are usually kept out of the way in a bathroom cabinet. Storage of medicines in homes under damp and humid conditions, as well as exposure to light or high temperatures, can cause medicines to degrade more quickly than expected.
The majority of drugs in our study were kept in the bedroom, which makes them accessible, especially to children living in or visiting the house. Some medications were kept in the kitchen, and in around 25% of the cases in the fridge, where heat and humidity, respectively, could be problematic, especially for solid formulations, eg, tablets. In 19 cases, medications were stored in the living room or in the bathroom. Lack of a single storage place for regular medications leads to a greater chance of missed doses, except if the medications are stored in different locations because of time of administration (eg, morning medications on the kitchen table and bedtime medications at the bedside).Citation15 Considering that the ideal place to keep medicines is in a locked container in a cool, dark, and dry place out of reach of children, these results indicated poor and sometimes hazardous medicine storage conditions.
Hoarding and disposing of medicines
Little evidence of drug hoarding was found in our sample because only three households reported retention of discontinued medication. This is important given the concerns we expressed regarding the status of medication storage and packaging in the households surveyed. We did not explore reasons why only a minority of households disposed of medications through plumbing (8%) compared with throwing them in the trash (81%). Low rates of medication return to pharmacies are not surprising given that it is not widely promoted by pharmacists in the country and Qatar does not currently have laws or regulations on recycling of any other products (eg, plastic, paper, aluminum).Citation12,Citation27
Sharing and use of medicines
Of concern was the fact that sharing of prescription medications was not uncommon in this sample. In seven cases, anti-infectives were shared, and in other cases inhaled bronchodilators, antidiabetic medication, and oral corticosteroids were shared as well. In countries where pharmacy regulations and standards are well developed, all of these medications would be categorized as prescription medicines used by specific patients to treat a specific health condition and for a specific duration of time. Anti-infective preparations (like antibiotics) are one of few classes of medications that are classified as prescription medicines in Qatar. This classification is in an effort to avoid irrational antibiotic use. Sharing of prescription medicines with individuals for whom the drug product was not intended may compound the problem of drug-related illnesses and may increase hospitalization rates and associated morbidity and mortality.Citation28 In previous studies, it had been reported that antibiotics were found as “leftovers” in drug cabinets, hence our finding in this respect was not unique.Citation29 In a large proportion of cases, drugs were used in a dosage regimen (dose, frequency, duration) that was different from the instructions on the drug label. This is also a risky practice that could lead to adverse effects as a result of overdosing or underdosing.
Sources of drug information
Most participants in this study reported that they were satisfied with the level of information they received regarding their medicines. In response to the question about what drugrelated information they would like provided, adverse effects of drugs topped the list. This might suggest that patients are not routinely provided with information about adverse effects, a finding that is similar to previously report findings.Citation30,Citation31 However, and of interest, respondents considered the physician to be the primary source for information related to drugs and their use. This same assertion was made by New Zealand respondents in a study conducted in Auckland in 2003.Citation32
Limitations
There was potential in this study for selection and social desirability bias as a result of the strategy of using the telephone to conduct an interview. Also, interviews which were conducted during working hours could run the risk of excluding highly educated young subjects. Due to the small sample size, the results of this exploratory study should be considered with caution. However, the findings do provide insight into aspects that should be further investigated as part of a larger study in the future.
Conclusion
This study raises several issues of concern in relation to medicines stored inside homes that warrant addressing. It also sheds some light on the potential role played by pharmacists regarding public education in relation to drug therapy that goes beyond the dispensing process. Judging by the finding that pharmacists were not considered primary sources of drug-related information, there seems to be a gap in the public understanding of the pharmacist’s role, and their acceptance of this. Pharmacists in Qatar must take advantage of the opportunities provided by the currently evolving health system to forge new roles for themselves. The benefits of this course of action will be both a stronger pharmacy profession and better health outcomes for the community.
Acknowledgment
This work was made possible by a grant from the Qatar National Research Fund under its Undergraduate Research Experience Program. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Qatar National Research Fund.
Disclosure
The author reports no conflict of interest in this work.
References
- HarrisonDLBootmanJLCoxERCost-effectiveness of consultant pharmacists in managing drug-related morbidity and mortality at nursing facilitiesAm J Health Syst Pharm19985515158815949706185
- BootmanJLHarrisonDLCoxEThe health care cost of drug-related morbidity and mortality in nursing facilitiesArch Intern Med199715718208920969382665
- FinkersFMaringJGBoersmaFTaxisKA study of medication reviews to identify drug-related problems of polypharmacy patients in the Dutch nursing home settingJ Clin Pharm Ther200732546947617875113
- SmithNLPsatyBMHeckbertSRTracyRPCornellESThe reliability of medication inventory methods compared to serum levels of cardiovascular drugs in the elderlyJ Clin Epidemiol199952214314610201655
- LeachRHWhitePLUse and wastage of prescribed medicines in the homeJ R Coll Gen Pract1978281863236553167
- Vacas RodillaECastellà DagàISánchez GiraltMPujol AlguéAPallarés ComaladaMCBalagué CorberaMSelf-medication and the elderly. The reality of the home medicine cabinetAten Primaria2009415269274 Spanish19443087
- Abou-AudaHSAn economic assessment of the extent of medication use and wastage among families in Saudi Arabia and Arabian Gulf countriesClin Ther20032541276129212809973
- LamABradleyGUse of self-prescribed nonprescription medications and dietary supplements among assisted living facility residentsJ Am Pharm Assoc (2003)200646557458117036643
- RobinsonAFPrescription medication practices of the elderlyContemp Pharm Pract19803313113610247868
- WasserfallenJBBourgeoisRBulaCYersinBBuclinTComposition and cost of drugs stored at home by elderly patientsAnn Pharmacother200337573173712708953
- FocazioMJKolpinDWBarnesKKA national reconnaissance for pharmaceuticals and other organic wastewater contaminants in the United States – II) untreated drinking water sourcesSci Total Environ20084022–320121618433838
- El HajjMSSalemSMansoorHPublic’s attitudes towards community pharmacy in Qatar: a pilot studyPatient Prefer Adherence2011540542221949604
- British Medical AssociationBritish National Formulary Available at: http://bnf.org/bnf/index.htmAccessed November 2, 2011
- CameronKMedication safety in the home: The need for pharmacist involvementCan Pharm J200714014749
- O’TooleJSinclairMLederKMaximising response rates in household telephone surveysBMC Med Res Method2008871
- MyersMQualitative research and the generalizability question: standing firm with Proteus2000 Online serial. Available from: http://www.nova.edu/ssss/QR/QR4-3/myers.htmlAccessed October 30, 2011
- YousifMAIn-home drug storage and utilization habits: a Sudanese studyEast Mediterr Health J200282–342243115339133
- De BolleLMehuysEAdriaensERemonJPVan BortelLChristiaensTHome medication cabinets and self-medication: a source of potential health threats?Ann Pharmacother200842457257918364405
- ZulloAHassanCCampoSMMoriniSBleeding peptic ulcer in the elderly: risk factors and prevention strategiesDrugs Aging2007241081582817896831
- LanasANonsteroidal antiinflammatory drugs and cyclooxygenase inhibition in the gastrointestinal tract: a trip from peptic ulcer to colon cancerAm J Med Sci200933829610619680014
- PengSDugganAGastrointestinal adverse effects of non-steroidal anti-inflammatory drugsExpert Opin Drug Saf20054215716915794710
- KolarzGMayrhoferFNeumannKSingerFAdverse effects of non-steroidal anti-inflammatory drugs. A prevalence study in AustriaWien Klin Wochenschr20031151–24146 German12658910
- JanahiIABenerABushAPrevalence of asthma among Qatari schoolchildren: International Study of Asthma and Allergies in Childhood, QatarPediatr Pulmonol2006411808616283628
- McIntireMSAngleCRGrushMLHow effective is safety packaging?Clin Toxicol197693419425954370
- PoirierSBarbeauGAn in-home medication inventory among elderly receiving home care servicesJ Geriatr Drug Ther19991234354
- ThompsonSStewartKPrescription medication use practices among non-institutionalised older personsInt J Pharm Pract200193141151
- QaziSQatar yet to take recycling seriouslyGulf Times2008 Available from: http://www.gulf-times.com/site/topics/article.asp?cu_no=2&item_no=262190&version=1&template_id=36&parent_id=1Accessed October 30, 2011
- KiyingiKSLauwoJADrugs in the home: danger and wasteWorld Health Forum19931443813848185788
- CeaserSWurtzR“Leftover” antibiotics in the medicine cabinetAnn Intern Med200013317410877746
- DeBLMehuysEAdriaensERemonJPVanBLChristiaensTHome medication cabinets and self-medication: a source of potential health threats?Ann Pharmacother200842457257918364405
- McMahonTClarkCMBailieGRWho provides patients with drug information?Br Med J (Clin Res Ed)19872946568355356
- PlantMHannaNChiTGoundenMKNA Review of Medicines Stored in Auckland HomesAuckland, New ZealandSchool of Pharmacy, University Of Auckland2010