Abstract
Smoking is still the most prominent cause of preventable premature death in the United States and an increasing cause of morbidity and mortality throughout the world. Although the current treatments such as nicotine replacement therapy (NRT) and bupropion are effective, long-term abstinence rates are low. Mechanism studies suggest that the pleasurable effects of smoking are mediated predominantly by nicotine, which activates the brain reward system by activation of brain α4β2 nicotinic acetylcholine receptors (nAChRs). Varenicline is a novel α4β2 nAChR partial agonist and has been found to be even more effective than NRT or bupropion in attenuating smoking satisfaction and in relieving craving and withdrawal symptoms after abstinence. Thus, varenicline has been recently approved to be a first-line medication for smoking cessation in the United States and European countries. Varenicline is generally well tolerated in healthy adult smokers, with the most commonly reported adverse effects being nausea, insomnia, and headache. However, growing postmarketing data has linked varenicline to an increase in neuropsychiatric symptoms such as seizures, suicidal attempts, depression, and psychosis as well as serious injuries potentially relating to unconsciousness, dizziness, visual disturbances, or movement disorders. Therefore, new safety warnings are issued to certain high risk populations, such as patients with mental illness and operators of commercial vehicles and heavy machinery. In particular, pilots, air traffic controllers, truck and bus drivers have been banned from taking varenicline.
Introduction
It is estimated that about 1.3 billion people smoke cigarettes worldwide and about 500 million people die annually from tobacco-related diseases.Citation1–Citation3 In the United States (US), about 45 million adults (∼20%) smoke cigarettes or are exposed to secondhand smoking, resulting in about 18% of total mortality and 440,000 annual premature deaths.Citation1,Citation2 The annual economic cost of smoking in the US is about 200 billion dollars. Smoking cessation has shown to significantly reduce the risk of many smoking-related diseases such as lung cancer, chronic lung diseases, myocardial infarction, and stroke as well as decrease morbidity and mortality related to tobacco use.Citation3
However, tobacco dependence is a chronic relapse disorder that is difficult to treat.Citation3 Despite the availability of effective pharmacologic aids, such as nicotine replacement therapy (NRT) and bupropion sustained-release, these treatments only help 5%–15% of people to maintain long-term abstinence from smoking.Citation4–Citation6 Craving and withdrawal symptoms after tobacco cessation are the most important reasons to prevent smokers from achieving long-term tobacco abstinence. For these reasons, novel pharmacotherapies are being developed in an attempt to improve long-term abstinence outcomes. Among the most promising of treatments is varenicline, a novel partial α4β2 nicotinic acctylcholine receptors (nAChR) agonist, which has recently been approved by the US Food and Drug Administration (FDA) as a smoking cessation aid. Varenicline has been found to be even more effective than placebo, NRT or bupropion in clinical trials.Citation5,Citation6 In this article, we review the mechanism-based medication development strategies, preclinical pharmacology, efficacy, and safety profiles of varenicline in the treatment of cigarette smoking in humans.
Mechanism of tobacco dependence
The mechanisms underlying tobacco addiction are not completely understood. Accumulating evidence indicates that nicotine is the major addictive component in tobacco.Citation7 Nicotine binds to central and peripheral nAChRs. Acetylcholine (Ach) is an endogenous neurotransmitter that binds to and activates both nAChRs and muscarinic acetylcholine receptors. Neuronal nAChRs are ligand-gated ion channels with high permeability to Ca++, and are formed from combinations of five subunits.Citation8,Citation9 To date, twelve different neuronal nAChR subunits have been cloned, including nine α-subunits (α2–α10) and three β-subunits (β2–β4). Non-neuronal subunits, α1, β1, γ, δ, and ε, form peripheral nicotinic receptors at the neuromuscular junction.Citation10 The neuronal subunits combine with two α- and three β-, or five α7-subunits to form nAChRs ().Citation10,Citation11 Both the α4β2 and α7 subtypes of nAChRs are the most abundant subtypes in the brain and are localized on presynaptic terminals, somatodendrites, and postsynaptic cells.Citation8,Citation9 Activation of presynaptic nAChRs by ACh or nicotine potentiates neurotransmitter release, while activation of postsynaptic nAChRs increases excitability of postsynaptic cells by increasing influx of Na+ and Ca++ via nAChR channels.Citation10–Citation12
Figure 1 Schematic diagram of the mesolimbic DA projection pathway in human brain, illustrating that nicotine activates α4β2 nAChRs located on DA neurons in the VTA and increases VTA DA neuron activity as well as DA release in the NAc, dorsal striatum, and PFC. Insert: Simplified structure of α4β2 nAChR (ion channel) located on surface of VTA DA neurons. Activation of α4β2 nAChR opens the receptor ion channel, causing influx of Na+ and/or Ca++ and depolarization of VTA DA neuron.
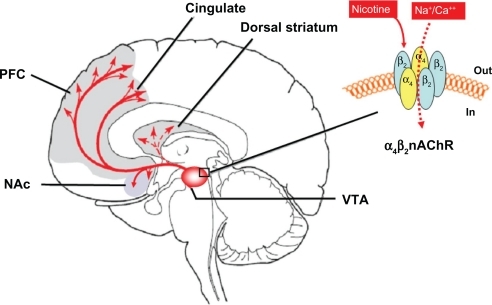
One third of the α4β2 nAChRs are located on the dopamine (DA) cells in the mesolimbic DA system ().Citation13,Citation14 This system originates from DA neurons in the ventral tegmental area (VTA) in the midbrain and projects to the forebrain nucleus accumbens (NAc) and the prefrontal cortex (PFC).Citation15 The α4β2 nAChR subtype has been thought to play a vital role in mediating nicotine reward.Citation8–Citation10 This is supported by the finding that blockade of α4β2 nAChRs by dihydro-β-erythroidine (DHβE) inhibits nicotine self-administration in rats.Citation16 Genetic deletion of α4 or β2 subunits largely abolishes nicotine binding to mouse brain and inhibits nicotine self-administration and nicotine-induced increases in NAc DA.Citation17,Citation18 Similarly, nicotine-mediated currents from VTA (DA) neurons are also inhibited by DHβECitation17,Citation19 or dramatically decreased on midbrain neurons in β2-kockout mice.Citation17,Citation19,Citation20 These data suggest that both the behavioral and DA-releasing effects of nicotine are mediated predominantly by activation of α4β2 nAChRs in the mesolimbic DA system.Citation8,Citation9,Citation17,Citation21 As stated above, the α4β2 nAChR is a receptor ion channel with high affinity to nicotine. High concentrations of nicotine binds to the α4β2 receptor, causing the ion channel opening and Na+ influx, which subsequently depolarizes VTA DA neurons and increases DA release in the NAc ().Citation21
Medication strategies for the treatment of nicotine addiction
Modulating nAChRs can be achieved using nAChR agonists, antagonists, or partial agonists. Full agonists, such as NRT, mimic the effects of nicotine by activating the receptor, therefore reducing withdrawal symptoms during nicotine abstinence.Citation22 NRT is proven effective in smoking cessation,Citation23 although it does not produce complete abstinence because the smoker is still physically dependent on the effects of smoking. Antagonists, such as mecamylamine, compete with nicotine or ACh for occupancy of the receptors.Citation24 Therefore, a full antagonist may fully block the pharmacological action of nicotine, such as nicotine reward. However, antagonists are prone to induce withdrawal symptoms by themselves.Citation22 Surprisingly, mecamylamine in combination with NRT is more effective than NRT alone or mecamylamine alone in smoking cessation.Citation25,Citation26 This could be due to a functional effect of the agonist NRT (reduction of the withdrawal syndromes) in combination with the effect of the antagonist mecamylamine (attenuation of the reinforcing effects of nicotine). This finding suggests that the development of a nicotine partial agonist such as cytisine and varenicline may be optimal in the treatment of nicotine dependence because partial agonists display the properties of both agonists and antagonists. Partial agonists occupy the receptors, but only partially activate them. As a consequence, the action of a partial agonist is dependent on the receptor occupancy.Citation27 In cigarette smokers, a partial agonist would mostly work as an antagonist during smoking (ie, high nicotine occupancy), but as an agonist during abstinence or withdrawal (ie, low nicotine occupancy). Thus, the rewarding effects of smoking would decrease substantially but not disappear completely, whereas withdrawal symptoms and craving episodes would occur less frequently during drug abstinence due to the release of a low-to-moderate level of DA produced by a partial agonist itself.Citation28–Citation30
Cytisine – an unnoticed smoking cessation drug since the 1960s
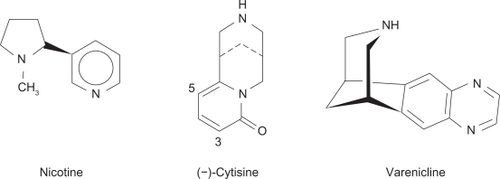
Cytisine has a molecular structure somewhat similar to that of nicotine and varenicline (). Cytisine is a natural insecticide present in plants called Cytisus laburnum (Golfen Rain).Citation28 Cytisine (Tabex®; Sopharma, Sofia, Bulgaria) has been used in Bulgaria, Germany, Poland, and Russia as a smoking cessation aid since the 1960s.Citation29–Citation32 Despite its widespread use in Eastern and Central Europe, cytisine has remained largely unnoticed elsewhere, possibly due to limited access to the non-English literature.Citation32 In addition, the underlying mechanisms have remained unclear until the 1990s when it was reported that cytisine is a partial agonist of nAChRs with high affinity for α4β2 receptors.Citation28,Citation33 Behavioral studies in experimental animals suggest that cytisine produces low-to-moderate behavioral activation,Citation34,Citation35 conditioned place preference,Citation36 and drug discriminative effects.Citation37 In addition, drug-naive mice also self-administer cytisine intravenously, suggesting that cytisine has certain reinforcing effects.Citation38
Figure 2 Chemical structures of nicotine, cytisine, and varenicline.
Preclinical pharmacology of varenicline
Varenicline as a smoke-cessation aid was developed by Pfizer in 1997, largely based on cytisine described above.Citation39,Citation40 In vitro binding assays indicate that varenicline has higher binding affinity (Ki = 0.15 nM) to α4β2 nAChRs than cytisine (Ki = 0.23 nM) or nicotine (Ki = 1.6 nM). It has 500–20,000-fold selectivity for α4β2 receptors over other nAChR subtypes ().Citation39–Citation41 In vitro functional patch clamp studies in HEK cells expressing nAChRs show that varenicline is a partial agonist with 45% of nicotine’s maximal efficacy at α4β2 nAChRs.Citation39 In neurochemical models varenicline has significantly lowered (40%–60%) efficacy than nicotine in stimulating [3H]-DA release from rat brain slices in vitro, and in increasing DA release from rat NAc in vivo.Citation39 When combined with nicotine, varenicline effectively attenuates the nicotine-induced DA release, consistent with partial agonism.Citation39
Table 1 In vitro binding affinity and functional activity of nicotine, cytisine, and varenicline at human brain nAChRsCitation28,Citation29,Citation41
In animal models of addiction (), varenicline significantly inhibits nicotine self-administration,Citation39 nicotine-enhanced brain stimulation reward,Citation42 and nicotine priming, but not nicotine-associated cue-induced reinstatement of drug-seeking behavior.Citation43 Varenicline itself does not induce reinstatement of nicotine seeking when administered as a priming injection.Citation43 Varenicline partially substitutes for nicotine in self-administration testing in animals and partially generalizes to nicotine in the drug discrimination preclinical animal paradigm,Citation39,Citation44 suggesting that it may have some abuse potential, but lower than that of nicotine. In addition, varenicline also enhanced the basal locomotor activity in drug-naive rats by itself, while pretreatment with varenicline attenuated acute nicotine-induced hyperlocomotion and repeated nicotine-induced behavioral sensitization.Citation45
Table 2 Behavioral effects of cytisine and varenicline in animal models related nicotine addiction
In addition to being an α4β2 nAChR partial agonist, varenicline is also a full α7 nAChR agonist.Citation46 To determine which receptor subtype underlies the action of varenicline, we have recently investigated the effects of α4β2 or α7 receptor agonists or antagonists on varenicline-enhanced electrical brain-stimulation reward (BSR). We found that systemic administration of nicotine or varenicline produced significant BSR enhancement, while pretreatment with varenicline dose-dependently attenuated nicotine-enhanced BSR. The BSR-enhancing effect produced by varenicline was blocked by mecamylamine (a full nAChR antagonist) and DHβE (a selective α4-containing nAChR antagonist), but not by methyllycaconitine (a selective α7 nAChR antagonist), suggesting an effect mediated by activation of α4β2 receptors.Citation42 This suggestion is further supported by findings that SIB-1765F, another selective α4β2 nAChR agonist, produced a dose-dependent enhancement of BSR, while pretreatment with SIB-1765F also attenuated nicotine-enhanced BSR. In contrast, the selective α7 receptor agonist, ARR-17779, altered neither BSR itself nor nicotine-enhanced BSR, at any dose tested.Citation42 These findings are consistent with other reports that neither deletion of α7 receptors nor pharmacological blockade of α7 receptors alters the nicotine-produced discriminative stimulus effect.Citation47–Citation49 Together, these data suggest that the pharmacotherapeutic effects of varenicline on nicotine’s action are mediated by activation of the α4β2, rather than the α7 nAChR subtype.
The bioavailability of varenicline is high and is unaffected by the time of dosing or administration with food.Citation50 After serial measurements, varenicline followed first-order kinetics, with an elimination T1/2 of ∼24 h after single and multiple doses.Citation50,Citation51 Steady-state levels were achieved within four days with repeated oral dosing.Citation51 Pharmacokinetic assays in healthy adult smokers indicated that varenicline did not undergo significant hepatic metabolism. Varenicline is <20% plasma protein bound. Its clearance is predominantly renal, with >90% excreted unchanged in the urine. Elimination of varenicline by the kidney primarily involves glomerular filtration and active tubular secretion via the renal organic cation transporter hOCT2.Citation51,Citation52
Therapeutic efficacy in humans
Following promising results in preclinical studies, together with a strong theoretical foundation for its use, testing of varenicline began in clinical safety and efficacy trials. summarizes the results of the ten clinical trials with varenicline since it was approved by the US FDA in 2006. These trials were conducted in Australia, Canada, Europe, Japan, South Korea, China, Thailand, Singapore, and the US, and enrolled both male and female subjects (age range, 18–75 years) with no major comorbidities in the past year. The primary end point in most of the studies was efficacy, which was assessed primarily in terms of the continuous abstinence rate (CAR) or continuous quit rate (CQR) based on subjective reporting and confirmation by exhaled carbon monoxide (CO) measurement (≤10 ppm). The second end points included the urge to smoke, withdrawal symptoms, and the reinforcing effects of nicotine. In addition, odds ratio (OR) meta-analysis was also used to measure the comparative efficacy and abstinence rates for various smoking cessation medications in some of those clinical trials.
Table 3 Clinical efficacy (CARs) of varenicline in human clinical trials
One of the trials reported follow-up data to 24 weeks,Citation53 and the others reported data to 52 weeks.Citation54–Citation62 During treatment with oral varenicline titrated to 1 mg twice per day (bid), CO-confirmed CQRs or CARs at week 12 ranged from 28.8% to 65.4%, at week-24 from 20.8% to 70.5%, and at week-52 from 14.4% to 43.6%. In all these trials, varenicline 1 mg bid was associated with significantly higher CARs or CQRs compared with placebo at either week 12, week 24, or week 52 when compared with placebo. Three trials reported significantly higher CARs or CQRs with varenicline 1 mg bid compared to bupropion,Citation55,Citation57,Citation58 and one trial reported significantly higher CARs with varenicline compared with NRT ().Citation62 In a relapse-prevention study, CARs were significantly improved at 24 weeks with varenicline relative to placebo (70.5% vs 49.6%).Citation59
Nides et alCitation63 conducted a pooled data analysis from the Phase III trials by Gonzales et alCitation57 and Jorenby et alCitation58 to explore the relative efficacy of varenicline, bupropion, and placebo for smoking cessation. Pooled CARs for weeks 9 through 12 were significantly greater for varenicline compared with bupropion and placebo (44.0%, 29.7%, and 17.7%, respectively; both comparisons P < 0.001).
West et alCitation64 conducted a similar analysis of pooled data from the same two Phase III trialsCitation57,Citation58 to evaluate the effects of varenicline, bupropion, and placebo on craving and withdrawal symptoms among smokers. They used the Minnesota Nicotine Withdrawal Scale (MNWS) to score craving and withdrawal symptoms in abstinent smokers (n = 612) and the Modified Cigarette Evaluation Questionnaire (mCEQ) to score the reinforcing effects of smoking in nonabstinent smokers (n = 1,115). They found that among all participants, cravings (urge to smoke) were significantly reduced with varenicline or bupropion compared with placebo (both P < 0.001) and with varenicline compared with bupropion (P = 0.008). Overall, varenicline or bupropion significantly inhibited negative withdrawal syndromes (depression, irritability, anxiety, difficulty concentrating, and insomnia) compared with placebo. In addition, they also found that varenicline-treated patients had significantly lower pleasurable effects of smoking compared with those treated with bupropion and placebo, as assessed by mCEQ scores for smoking satisfaction, psychological reward and enjoyment of respiratory tract sensations.
Cahill et alCitation65 conducted a systemic review and meta-analysis of the efficacy and tolerability of varenicline for smoking cessation in seven placebo-controlled trials, one relapse-prevention trial, and one open-label trial comparing varenicline with NRT. The nine trials covered 7,267 participants, 4,744 of whom used varenicline. The pooled ORs for CAR for varenicline versus placebo at six months or longer was 2.33 (95% confidence interval [CI]: 1.95–2.80), for varenicline versus bupropion at one year was 1.52 (95% CI: 1.22–1.88), and for varenicline versus NRT at one year was 1.31 (95% CI: 1.01–1.71). These data suggest that varenicline is even more effective than bupropion or NRT.
Mills et alCitation66 conducted large-scale pooled data analysis from nine trials with varenicline (n = 5,192), 101 clinical trials with NRT (n = 31,321), and 31 trials with bupropion (n = 11,118) in order to compare treatment effects across interventions. They found that the pooled ORs for smoking cessation at four weeks post-target quit data with varenicline, NRT, and bupropion were 3.16, 2.25, and 2.05, respectively (P < 0.001, compared to placebo). Two trials evaluated head to head comparisons of varenicline and bupropion, and found a pooled OR 1.86 (P < 0.001). Indirect comparison between varenicline and NRT was OR 1.56 (P < 0.001), and between varenicline and bupropion OR 1.40 (P = 0.01).
Taken together, all these clinical data suggest that varenicline is superior to placebo, NRT, and bupropion for achieving abstinence from smoking in the short-term. Varenicline not only significantly attenuates the craving and withdrawal symptoms that occur during abstinence from smoking, but also significantly reduces the rewarding effects of nicotine and delay smoking relapse. Thus, varenicline, as the newest agent approved for smoking-cessation, offers a new therapeutic option for the treatment of nicotine addiction.
Tolerability
Varenicline is generally well tolerated, with the most commonly reported adverse effects being nausea (28.8%, 9.9%, and 9.1%), insomnia (14.2%, 21.5%, and 12.6), and headache (14.2%, 11.1%, and 12.4) when compared to bupropion or placebo.Citation54
Nausea
Mild to moderate nausea was the most frequently reported adverse effect (overall incidence, 24.4%–52.0%) that occurred at a higher rate in varenicline group than in placebo groups. Most episodes of nausea began in the first week of treatment and lasted for a median duration of ≤12 days. Dose titration appeared to reduce the overall incidence of nausea.Citation56 There was a low incidence of nausea (13.4%) in varenicline-treated patients in the self-regulated flexible dosing study.Citation61 In clinical trials, rates of treatment discontinuation due to nausea were generally <5% in varenicline-treated patients.Citation54
Insomnia
Insomnia was another commonly reported adverse effect (14.0%–37.2%) associated with varenicline in the clinical trials.Citation5,Citation54 In general, insomnia occurred during the first four weeks of treatment with varenicline and became less common as treatment continued. In one extended treatment study,Citation67 the incidence of insomnia was 19.1% with varenicline and 9.5% with placebo, suggesting that insomnia may be a common symptom of nicotine withdrawal during smoking-cessation attempts.
Headache
Other common adverse effects include headache, abnormal dreams, sleep disturbance, dizziness, dry mouth, increased appetite, weight gain, and constipation, which generally occurred at rates twice those with placebo.Citation55–Citation67 These adverse events were mild-to-moderate and transient, occurring predominantly during the first four weeks of therapy. The rates of discontinuation of varenicline treatment due to these adverse effects were <2% of participants.
Utility in high risk people
Since the approval of varenicline in May 2006, post-marketing surveillance suggests an association between varenicline and increased risk of erratic behavior, agitation, suicidal attempt, depression, psychosis, and severe injuries.Citation68 While some of the behavioral and mood changes may be associated with nicotine withdrawal, some occurred in people who continued smoking while on the medication. The Institute for Safe Medication Practices (ISMP), an independent safety group, analyzed all adverse effects since the approval for marketing and found that varenicline accounted for more reports of serious adverse effects than any other drug in the US.Citation69,Citation70 Accordingly, the following people are thought to be high-risk to the use of varenicline.
Patients with mental illnesses
In the fourth quarter report of 2007,Citation71 the FDA reported that among the total 988 serious injuries related to varenicline from 2006 to December 2007, there were 227 reports of suicidal attempt or behavior, 397 cases of possible psychosis, and 525 reports of hostility or aggression within days to weeks of initiating varenicline therapy for smoking cessation. Based on these reports, in November 2007, the FDA issued an early alert about the safety of varenicline, emphasizing the need for screening for pre-existing psychiatric illness before using varenicline and the importance of monitoring/reporting of mood or behavior changes.Citation71 In May 2008, the FDA updated the previous Public Health Advisory and required that all patients should be observed and report to their physicians immediately for any mood or behavior changes, or worsening of preexisting psychiatric illness, during or upon discontinuation of varenicline therapy.Citation72 This safety concern in such high-risk patients was further emphasized in more recent clinical reports.Citation73–Citation76 For example, about 5% patients (from the total 2,682 patients since December 2006) in the UK reported psychiatric effects during treatment with varenicline, including sleep disorder (43, 1.6%), anxiety (33, 1.2%), depression (29, 1.0%), abnormal dreams (26, 1.0%), mood change (17, 0.6%), and suicidal events (n = 5).Citation77
Commercial vehicle drivers and heavy machinery operators
In addition to those psychiatric effects described above, in the fourth quarter report of 2007,Citation71 the FDA also reported 372 movement disorders, 173 serious accidental injuries (including 28 traffic accidents and 77 falls), at least 148 reports of visual disturbances, 224 reports of potential cardiac rhythm disturbances, 338 moderate to severe skin reactions, and numerous reports of drowsiness that may affect patients’ ability to drive or operate machinery. Based on these reports, the ISMP issued immediate safety concerns related to varenicline use among operators of vehicles and heavy machinery as well as in any setting in which alertness and motor control are required to avoid serious injury. In May 2008, the Federal Motor Carrier Safety Administration and Federal Aviation Administration announced that pilots, air-traffic controllers, and truck and bus drivers are barred from taking smoking-cessation drug.Citation78,Citation79
Conclusions
Varenicline (Chantix®; Pfizer, New York, NY), an α4β2 nAChR partial agonist, is the first in a new class of agents for smoking cessation. In the updated clinical practice guideline from the US Public Health Service, varenicline is recommended as a well-tolerated and effective first-line treatment option for smoking cessation. We should note that the majority of published clinical trials of the efficacy and tolerability of varenicline have generally excluded smokers with comorbid conditions (ie, psychiatric disorders, cardiovascular diseases), obese patients, adolescents, pregnant women, and light smokers (<10 cigarettes/d), which may reduce the generalization of the results to the broad population of smokers. To date, almost all clinical trials have been sponsored by the manufactures of varenicline, suggesting that potential clinician bias may also affect the results even when double-blind procedures are used. Thus, more clinical-trials and postmarketing data are needed to confirm its efficacy, safety, and tolerability. Given the growing evidence suggesting a possible association between varenicline and increased psychiatric symptoms and other severe injuries potentially relating to unconsciousness, the FDA has issued special warning for the use of varenicline in patients with pre-existing psychiatric illnesses, and the Federal Motor Carrier Safety Administration and Federal Aviation Administration have banned the use of varenicline in pilots, air-traffic controllers, and truck and bus drivers.
Acknowledgements
This work was supported by the Intramural Research Program of the National Institute on Drug Abuse (NIDA) and National Institutes of Health (NIH), USA.
Disclosure
The author reports no conflicts of interest in this work.
References
- Cigarette smoking among adults, United States 2006MMWR Morb Mortal Wkly Rep2007561157116117989644
- 2008 PHS Guideline Update Panel, Liaisons, and StaffTreating tobacco use and dependence: 2008 update US Public Health Service Clinical Practice Guideline executive summaryRespir Care2008531217122218807274
- Smoking-attributable mortality, years of potential life lost, and productivity losses, United States 2000–2004Morb Mortal Wkly Rep20085712261228
- EtterJFCytisine for smoking cessation: a literature review and a meta-analysisArch Intern Med20061661553155916908787
- HaysJTEbbertJOSoodAEfficacy and safety of varenicline for smoking cessationAm J Med20081214 Suppl 1S32S4218342165
- GarrisonGDDuganSEVarenicline: a first-line treatment option for smoking cessationClin Ther20093146349119393839
- GoldbergSRSpealmanRDGoldbergDMPersistent behavior at high rates maintained by intravenous self-administration of nicotineScience19812145735757291998
- JonesSSudweeksSYakelJLNicotinic receptors in the brain: correlating physiology with functionTrends Neurosci19992255556110542436
- DaniJABiasiMDCellular mechanisms of nicotine addictionPharmacol Biochem Behav20017043944611796143
- Le NovèreNCorringerPJChangeuxJPThe diversity of subunit composition in nAChRs: evolutionary origins, physiologic, and pharmacologic consequencesJ Neurobiol20025344745612436412
- McGeheeDSRoleLWPhysiological diversity of nicotinic acetylcholine receptors expressed by vertebrate neuronsAnnu Rev Physiol1995575215467778876
- WonnacottSPresynaptic nicotinic ACh receptorsTrends Neurosci19972092989023878
- ClarkePBPertAAutoradiographic evidence for nicotine receptors on nigrostriatal and mesolimbic dopaminergic neuronsBrain Res19853483553584075093
- ZhouFMWilsonCDaniJAMuscarinic and nicotinic cholinergic mechanisms in the mesostriatal dopamine systemsNeuroscientist20039233612580337
- WiseRADopamine, learning, and motivationNat Rev Neurosci2004548349415152198
- WatkinsSSEpping-JordanMPKoobGFBlockade of nicotine self-administration with nicotinic antagonists in ratsPharmacol Biochem Behav19996274375110208381
- PicciottoMRZoliMRimondiniRAcetylcholine receptors containing the beta2 subunit are involved in the reinforcing properties of nicotineNature19983911731779428762
- MarubioLMGardierAMDurierSEffects of nicotine in the dopaminergic system of mice lacking the alpha4 subunit of neuronal nicotinic acetylcholine receptorsEur J Neurosci2003171329133712713636
- WooltortonJRPidoplichkoVIBroideRSDifferential desensitization and distribution of nicotinic acetylcholine receptor subtypes in midbrain dopamine areasJ Neurosci2003233176318512716925
- PicciottoMRZoliMLénaCAbnormal avoidance learning in mice lacking functional high-affinity nicotine receptor in the brainNature199537465677870173
- XiZXSpillerKGardnerELMechanism-based medication development for the treatment of nicotine dependenceActa Pharmacol Sin20093072373919434058
- CarrozziLPistelliFViegiGPharmacotherapy for smoking cessationTher Adv Respir Dis2008230131719124379
- SilagyCLancasterTSteadLNicotine replacement therapy for smoking cessationCochrane Database Syst Rev20043CD00014615266423
- LancasterTSteadLFMecamylamine (a nicotine antagonist) for smoking cessationCochrane Database Syst Rev20002CD00100910796584
- RoseJELevinEDConcurrent agonist-antagonist administration for the analysis and treatment of drug dependencePharmacol Biochem Behav1992412192261539072
- RoseJEBehmFMWestmanECMecamylamine combined with nicotine skin patch facilitates smoking cessation beyond nicotine patch treatment aloneClin Pharmacol Ther19945686998033499
- ChildressARO’BrienCPDopamine receptor partial agonists could address the duality of cocaine cravingTrends Pharmacol Sci2000216910637646
- CoeJWBrooksPRWirtzMC3, 5-Bicyclic aryl piperidines: a novel class of alpha4beta2 neuronal nicotinic receptor partial agonists for smoking cessationBioorg Med Chem Lett2005154889489716171993
- BarlowRBMcLeodLJSome studies on cytisine and its methylated derivativesBr J Pharmacol1969351611744387392
- BenndorfSScharfenbergGKempeGSmoking withdrawal treatment with Cytisine (Tabex). Results of a semi-annual survey of former smokers after 4 weeks of therapyDtsch Gesundheitsw1970247747765524300
- ScharfenbergGBenndorfSKempeGCytisine (Tabex) as a pharmaceutical aid in stopping smokingDtsch Gesundheitsw1971264634654930772
- EtterJFLukasRJBenowitzNLCytisine for smoking cessation: a research agendaDrug Alcohol Depend2008923817825502
- PapkeRLHeinemannSFPartial agonist properties of cytisine on neuronal nicotinic receptors containing the β2 subunitMol Pharmacol1994451421498302273
- StolermanIPGarchaHSMirzaNRDissociations between the locomotor stimulant and depressant effects of nicotinic agonists in ratsPsychopharmacology (Berl)19951174304377604144
- ReavillCWaltherBStolermanIPBehavioral andpharmacokinetic studies on nicotine, cytisine, and lobelineNeuropharmacology1990296196242385332
- MuseoEWiseRAPlace preference conditioning with ventral tegmental injections of cytisineLife Sci199455117911867934614
- ChandlerCJStolermanIPDiscriminative stimulus properties of the nicotinic agonist cytisinePsychopharmacology (Berl)19971292572649084064
- RasmussenTSwedbergMDReinforcing effects of nicotinic compounds: intravenous self-administration in drug-naive micePharmacol Biochem Behav1998605675739632242
- RollemaHChambersLKCoeJWPharmacological profile of the alpha4beta2 nicotinic acetylcholine receptor partial agonist varenicline, an effective smoking cessation aidNeuropharmacology20075298599417157884
- RollemaHCoeJWChambersLKRationale, pharmacology, and clinical efficacy of partial agonists of alpha4beta2 nACh receptors for smoking cessationTrends Pharmacol Sci20072831632517573127
- CarrollFIYokotaYMaWSynthesis, nicotinic acetylcholine receptor binding, and pharmacological properties of 3′-(substituted phenyl) deschloroepibatidine analogsBioorg Med Chem20081674675417964169
- SpillerKXiZXLiXVarenicline attenuates nicotine-enhanced brain-stimulation reward by activation of alpha4beta2 nicotinic receptors in ratsNeuropharmacology200957606619393252
- O’ConnorECParkerDRollemaHThe alpha4beta2 nicotinic acetylcholine-receptor partial agonist varenicline inhibits both nicotine self-administration following repeated dosing and reinstatement of nicotine seeking in ratsPsychopharmacology2009125 [Epub ahead of print]
- SmithJWMoggATafiELigands selective for alpha4beta2 but not alpha3beta4 or alpha7 nicotinic receptors generalize to the nicotine discriminative stimulus in the ratPsychopharmacology200719015717017115136
- ZaniewskaMMcCrearyACStefan ′skiREffect of varenicline on the acute and repeated locomotor responses to nicotine in ratsSynapse20086293593918798299
- MihalakKBCarrollFILuetjeCWVarenicline is a partial agonist at alpha4beta2 and a full agonist at alpha7 neuronal nicotinic receptorsMol Pharmacol20067080180516766716
- BrioniJDKimDJBO’NeillABNicotine cue: lack of effect of the alpha7 nicotinic receptor antagonist methyllycaconitineEur J Pharmacol1996301158773440
- GommansJStolermanIPShoaibMAntagonism of the discriminative and aversive stimulus properties of nicotine in C57BL/6J miceNeuropharmacology2000392840284711044754
- StolermanIPChamberlainSBizarroLThe role of nicotinic receptor alpha7 subunits in nicotine discriminationNeuropharmacology20044636337114975691
- FaesselHMSmithBJGibbsMASingle-dose pharmacokinetics of varenicline, a selective nicotinic receptor partial agonist, in healthy smokers and nonsmokersJ Clin Pharmacol20064699199816920893
- FaesselHMGibbsMAClarkDJMultiple-dose pharmacokinetics of the selective nicotine receptor partial agonist, varenicline, in healthy smokersJ Clin Pharmacol2006461439144817101743
- FengBObachRSBursteinAHEffect of human renal cationic transporter inhibition on the pharmacokinetics of varenicline, a new therapy for smoking cessation: An in vitro-in vivo studyClin Pharmacol Ther20088356757617971819
- TsaiSTChoHJChengHSA randomized, placebo-controlled trial of varenicline, a selective alpha4beta2 nicotinic acetylcholine receptor partial agonist, as a new therapy for smoking cessation in Asian smokersClin Ther2007291027103917692719
- GarrisonGDDuganSEVarenicline: a first-line treatment option for smoking cessationClin Ther20093146349119393839
- NidesMOnckenCGonzalesDSmoking cessation with varenicline, a selective alpha4beta2 nicotinic receptor partial agonist: results from a 7-week, randomized, placebo-, and bupropion-controlledtrialwith1-yearfollow-upArchInternMed200616615611568
- OnckenCGonzalesDNidesMEfficacy and safety of the novel selective nicotinic acetylcholine receptor partial agonist, varenicline, for smoking cessationArch Intern Med20061661571157716908789
- GonzalesDRennardSINidesMVarenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trialJAMA2006296475516820546
- JorenbyDEHaysJTRigottiNAEfficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trialJAMA2006296566316820547
- TonstadSTønnesenPHajekPEffect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trialJAMA2006296647116820548
- NakamuraMOshimaAFujimotoYEfficacy and tolerability of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, in a 12-week, randomized, placebo-controlled, dose-response study with 40-week follow-up for smoking cessation in Japanese smokersClin Ther2007291040105617692720
- NiauraRHaysJTJorenbyDEThe efficacy and safety of varenicline for smoking cessation using a flexible dosing strategy in adult smokers: a randomized controlled trialCurr Med Res Opin2008241931194118513462
- AubinHJBobakABrittonJRVarenicline versus transdermal nicotine patch for smoking cessation: results from a randomized openlabel trialThorax20086371772418263663
- NidesMGloverEDReusVIVarenicline versus bupropion SR or placebo for smoking cessation: a pooled analysisAm J Health Behav20083266467518442345
- WestRBakerCLCappelleriJCEffect of varenicline and bupropion SR on craving, nicotine withdrawal symptoms, and rewarding effects of smoking during a quit attemptPsychopharmacology (Berl)200819737137718084743
- CahillKSteadLFLancasterTNicotine receptor partial agonists for smoking cessationCochrane Database Syst Rev200816CD00610318646137
- MillsEJWuPSpurdenDEfficacy of pharmacotherapies for short-term smoking abstinance: a systematic review and meta-analysisHarm Reduct J200962519761618
- WangCXiaoDChanKPPothiratCGarzaDDaviesSVarenicline for smoking cessation: a placebo-controlled, randomized studyRespirology20091438439219192221
- WilliamsKEReevesKRBillingCBJrA double-blind study evaluating the long-term safety of varenicline for smoking cessationCurr Med Res Opin20072379380117407636
- MooreTJCohenMRFurbergCDInstitute for Safe Medication PracticesStrong safety signal seen for new varenicline risks2008521 Available from: http://www.ismp.org/docs/vareniclinestudy.asp. Accessed 2008 May 29.
- Institute for Safe Medication Practices Quarter Watch (3rd Quarter 2008): Safety concerns with generics, Chantix aggressive behavior, and more. 2009 May 7. Available from: http://www.ismp.org/Newsletters/acutecare/articles/20090507.asp. Accessed 2010 March 29.
- US Food and Drug Administration Safety alerts for human medical products: Chantix (varenicline). 2007 November 20. Available from: http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm152098.htm. Accessed 2007 November 23.
- US Food and Drug Administration Public health advisory: important information on Chantix (varenicline). May 16, 2008. Available from: http://www.fda.gov/cder/drug/advisory/varenicline.htm. Accessed 2008 May 29.
- LyonGJPossible varenicline-induced paranoia and irritability in a patient with major depressive disorder, borderline personality disorder, and methamphetamine abuse in remissionJ Clin Psychopharmacol20082872072119011454
- KintzPEvansJVillainMSmoking cessation with varenicline: a suicidal fatalityJ Anal Toxicol20093311812019239738
- KutscherECStanleyMOehlkeKChantix-induced mental status changes in a young healthy femaleS D Med20096219319519489343
- PurvisTLMambourgSEBalvanzTMSafety and effectiveness of varenicline in a veteran population with a high prevalence of mental illnessAnn Pharmacother20094386286719383936
- KasliwalRWiltonLVShakirSASafety and drug utilization profile of varenicline as used in general practice in England: interim results from a prescription-event monitoring studyDrug Saf20093249950719459717
- US Dept of Transportation, Federal Motor Carrier Safety Administration Statement from administrator. 2008 May 23. Available from: http://www.fmcsa.dot.gov/statement-5-23-08.htm. Accessed 2008 May 28.
- Federal Aviation Administration Anti-smoking medicine Chantix banned. 2008 May 23. Available from: http://www.faa.gov/news/updates/index.cfm?newsld=56363. Accessed 2008 May 28.