
Abstract
Background
Epicardial adipose tissue thickness (EATT) measured by echocardiography is a reliable indicator of visceral adipose tissue in the body and metabolic syndrome. The objective of this work was to study the effect of 12-week aerobic exercise training on echocardiographic epicardial adipose tissue thickness (EEATT), body composition and other metabolic parameters in asymptomatic overweight adults.
Methods
A total of 170 overweight and mild obese individuals were randomly allocated to 12-week aerobic exercise program (intervention group) or no supervised exercise (control group). The body fat percentage and visceral fat levels were measured by bioelectric impedance analyzer, and blood tests were conducted to measure lipids, fasting blood sugar (FBS) and high-sensitivity C-reactive protein (Hs-CRP). The participants also underwent transthoracic echocardiography to measure EATT. All the outcomes were measured after 12 weeks. Repeated measures were analyzed using ANOVA and Mann–Whitney U-test were used to analyze the data.
Results
EEATT values significantly reduced by −16.24% (3.12±1.18 to 2.70±1.04, p<0.05) following 12 weeks of aerobic exercise along with a reduction in weight by 2.96% (80.66±12.12 to 78.27±12.31, p<0.05), body mass index by 3.11% (29.20±2.71 to 28.29±2.81, p<0.05) and waist circumference by 2.29% (94.82±7.23 to 92.64±7.33, p<0.05) and improved Hs-CRP values.
Conclusion
The 12-week aerobic exercise was found to be effective in reducing EEATT in overweight and mild obese individuals. There was significant improvement in body composition, blood lipids, FBS, Hs-CRP and exercise capacity in intervention group compared to control group.
Introduction
The knowledge on adverse effects of increased visceral adipose tissue (VAT) has created new research interest in primary and secondary prevention of diseases. The overweight and obese individuals are more prone to cardiovascular disorders due to pathogenic profile of excess VAT.Citation1 VAT is more pro-inflammatory and metabolically active compared to the subcutaneous adipose tissue (SAT) and associated with cardiovascular diseases even in nonobese population.Citation2,Citation3 Recently, the adipose tissue within the thoracic cavity has been found to play a greater role in development and progression of diseases.Citation4
Epicardial adipose tissue (EAT), the fat on the surface of the myocardium and beneath the epicardium, is a known risk factor for cardiometabolic diseases in obese population.Citation5 There is also evidence on its pathogenic profile and clinical implications of increased epicardial adipose tissue thickness (EATT).Citation6 EATT is increased in coronary artery disease (CAD) patients compared to those without CAD. The role of EAT in CAD is explained by its presence in abundance closer to coronary arteries, its ability to store excess lipids and its active role in producing inflammatory substances like C-reactive protein.Citation7,Citation8 EATT is increased in healthy and asymptomatic individuals with increased body mass index (BMI) across different ages, and also in lean individuals with CAD.Citation9,Citation10 The literature on EAT and its relationship with metabolic syndrome is mostly limited to European and Caucasian population.Citation11 Studies on EAT in other ethnic populations, focusing on prevention of obesity-related diseases, are limited.
As the prevalence of obesity and its related complications is increasing in developing countries like India, the prevention and management of this global epidemic has gained importance recently.Citation12 The reduction of excess body fat and visceral fat with exercise as mainstay of treatment has been demonstrated in several studies earlier.Citation13,Citation14 Anthropometric parameters are still widely used to monitor the effects of weight loss interventions, but the accuracy of these parameters in monitoring the changes in VAT is not good.Citation15 The quantification of VAT using computed tomography and magnetic resonance imaging (MRI) provides accurate measurements, helping in risk stratification of obese individuals and also to monitor the effect of therapeutic interventions in primary prevention of cardiovascular diseases.Citation16,Citation17 It was observed that VAT or intra-abdominal fat estimated by MRI had good correlation with EATT in earlier studies.Citation18 EATT measurement using echocardiography has been proposed to be an easy and inexpensive method for quantifying the VAT in overweight and obese population.Citation19 The interrater and intrarater reliability of EATT measurement is found to be good, and the method has been validated with MRI.Citation20
Echocardiographic epicardial adipose tissue thickness (EEATT) is proposed as a therapeutic target in obesity management.Citation21 The reduction of EATT with low-calorie diet, bariatric surgery and anti-dyslipidemia drugs has been demonstrated in the previous studies.Citation22–Citation24 Although the reduction of VAT with aerobic and resistance exercises has been demonstrated earlier, there is scarcity of literature on the effect of exercise on EAT.Citation25 Aerobic exercise has been found to be effective in reducing the EEATT along with a reduction in VAT in a study conducted by Kim et al in asymptomatic obese men.Citation26 This study did not include non-exercise control group. A study conducted by Wilund et al in patients undergoing hemodialysis confirmed the role of aerobic exercise in reducing EEATT.Citation27 The reduction in EAT was associated with an improvement in the left ventricular regional myocardial function in patients with metabolic syndrome.Citation28 Even though there is some evidence, the magnitude of effect of aerobic exercise on EEATT has not been well characterized in a large sample-based study so far. The objective of our study was to determine the effect of aerobic exercise program on the EEATT, body weight, BMI, waist circumference (WC), blood lipids and high-sensitivity C-reactive protein (Hs-CRP) in overweight and obese individuals.
Methods
A total of 170 overweight and mild obese Asian-Indian individuals (BMI 25.00–34.9) of age between 20 and 45 years were randomized to study group or control group after thorough screening as part of a randomized controlled trial. Institutional ethical committee approval (Manipal Academy of Higher Education, India; approval number: UEC/55/2009) was obtained prior to commencement of the study. A written informed consent was obtained from all the participants. The sample size was estimated. To detect a minimal clinically important difference of 0.8 mm and SD of 1.4 mm at 5% level of significance and 90% power for a two-tailed test, the sample size required in each group was 64. But considering the high attrition rate, 85 participants were included in each group. The participants included were primary prevention population with no known diseases and those who expressed willingness to participate in the study. All the participants were recruited by verbal advertisement, mainly by conducting awareness programs in the institutions and during disease prevention camps.
Randomization
Ninety females and 80 males were allocated to one of the two groups using Sequentially Numbered Opaque Sealed Envelopes method and block randomization method. The sequence generation was not known to the primary investigator, and the treatment allocation was not known to the sonologist and medical lab technician who interpreted the blood test results.
Initial screening
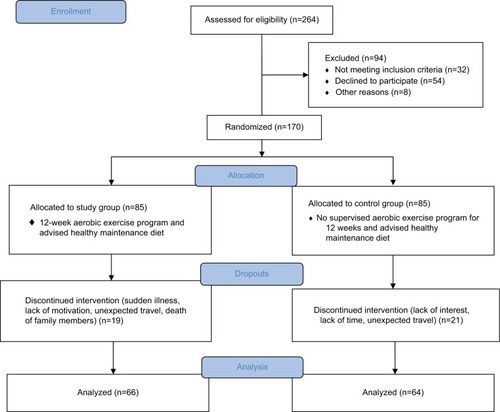
A brief questionnaire was administered to know the physical activity status, and dietary and other lifestyle habits of the participants. A short version of Physical Activity Readiness Questionnaire was administered as part of the screening, and participants with known history of medical conditions were not included.Citation29 Resting blood pressure was measured, and participants with consistent high readings were advised to go for further medical examination and were not included in the study. Participants who were on medications known to affect carbohydrate or lipid metabolism, or anti-inflammatory drugs, or had psychiatric disorders were excluded from the study. The exclusion criteria also included diagnosis of musculoskeletal or neurological conditions and any major nutritional deficiency disorders contraindicating the exercise test and prescription. Chronic smokers and alcoholics were also not included in the study. The eligible participants were invited for an orientation session where the explanation and clarifications about the study were given. After the randomization process, the participants were given advice on healthy weight maintenance diet, but no calorie restriction was advised. The participants who agreed to sign the informed consent were assigned to one of the two groups and underwent anthropometric assessment, body composition assessment, exercise testing, echocardiography and blood tests. The sequence of assessment and the outcome measurements are mentioned in the flowchart shown in .
Figure 1 Flow diagram showing the procedure according to CONSORT guidelines.
Anthropometrics
Height was measured at baseline using a wall tape calibrated to 0.1 cm with shoes off. Body weight was measured using an electronic weighing scale (model DS-215 series; Essae-Teraoka Limited) in light clothing without shoes to the nearest 0.1 kg. BMI was calculated as body weight divided by height squared in kg/m2. WC was measured in centimeters between the lower rib margin and the iliac crest at the end of normal expiration using a snug inch tape while the participants were standing with their heels together. The National Institutes of Health guidelines for measurement of WC and ethnic-specific risk categorization recommended for south Asians were used for interpretation. All measurements were performed after an overnight fast.
Body fat measurement
Four-electrode bioelectric impedance analyzer (HBF-362 Omron Karada Scan) was used to measure the total body fat percentage and visceral fat levels. It was ensured that the participants did not consume food or water for at least 1 hour prior to the measurement. Test–retest reliability examined in the present study for total body fat percentage and visceral fat levels was found to be excellent with standard measurement errors ranging from 0.8% to 2% and 0.5% to 1.5%, respectively.
Blood tests
The participants were asked to go for a blood test after overnight fasting for 10–12 hours and were also asked to refrain from consuming alcohol and exercise for 24 hours prior. Total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood sugar (FBS) levels and Hs-CRP (immunoturbidimetric method) were measured. The blood lipid values were interpreted according to the 2002 National Cholesterol Education Program – ATP III guidelines.Citation30
EEATT measurement
All the participants underwent transthoracic two-dimensional M-mode echocardiography (General Electric Company [GE] Vivid E echo machine). The measurements were taken in standard parasternal view in the left lateral decubitus position by an experienced sonologist, and the mean values between long- and short-axis views were recorded. The EAT was identified as the echo-free space between the outer wall of the myocardium and the visceral layer of the pericardium. The thickness was measured perpendicularly on the free wall of the right ventricle at end systole in three to ten cardiac cycles as described by Iacobellis et al.Citation31 The images were stored in the device for accurate measurement. All the measurements were taken by a single tester, and the tester was blinded about the treatment allocation. The interobserver and intraobserver agreement (intraclass correlation coefficient 0.98 and 0.96, respectively) for EEATT measurement was found to be excellent in a sample of 40 overweight and obese individuals participated in the present study.
Assessment of physical activity and cardiorespiratory fitness
The cardiorespiratory endurance test was conducted using treadmill testing protocol.Citation32 A polar heart monitor (Polar FT1; Polar Electro Oy, Kempele, Finland) was used to monitor the heart rate response to the incremental exercise. The termination of the test was done as soon as the client reached the age-predicted maximum heart rate or once he/she achieved more than 17 on Borg’s rate of perceived exertion scale. The duration of total exercise before the participant stopped the exercise test was recorded, and peak VO2 values were estimated.
Treatment for the study group
The American College of Sports Medicine (ACSM) guidelines were followed for the exercise prescription for the intervention group. Moderate-intensity (40%–60% of heart rate reserve) aerobic exercise program on treadmill was assigned to the intervention group participants.Citation33 The continuous aerobic exercise was preceded by 5–15 minutes of warm-up session and followed by 5–10 minutes of cool-down session. Stretching exercises and low-intensity treadmill exercises were mainly the part of warm-up and cool-down sessions. The frequency of exercise was set as a minimum of three sessions in a week to all seven sessions, and each session lasted for 40–60 minutes including the warm-up and cool-down sessions. The prescribed heart rate range was maintained by adjusting the speed and inclination in the treadmill. A logbook was maintained to track the duration, intensity and frequency of the exercise sessions done by each participant. The adherence to the exercise program was calculated for each participant, and average for all participants was calculated. The investigators also conducted several counseling sessions to motivate the participants and improve the adherence to the exercise program. The total exercise minutes and energy expenditure in terms of MET minutes per week were calculated.
Attrition
The participants who missed more than three follow-up appointments or were not exercising for a minimum of three sessions in a week were contacted via telephone. Thorough attempts were made by the investigators to contact the participants and to improve adherence to the prescribed exercise program. The participants who missed more than four exercise sessions in a week and who did not complete a minimum of 30 sessions in 12-week duration were considered as dropouts. The participants in the control group who did not respond to the phone calls made to monitor physical activity levels and who did not appear for assessment and investigations after 12 weeks were considered as dropouts. The number of dropouts in both the groups was 40, and a total of 130 participants (71 females and 59 males) were included for the data analysis. The overall compliance to the exercise prescription was ~86% in this study.
Treatment for participants in control group
Participants in the control group were asked to maintain their current level of activity during the 12-week study period. The activity logs were given to all the participants and were monitored every week either by telephone or personal contact.
Statistical analysis
The descriptive statistics were used for calculating the mean/median of demographics of the participants in both the groups. Independent t-test was used to compare the baseline parameters between the intervention and control groups. Shapiro–Wilk test was conducted to examine whether data met assumptions of normality of distribution, and Mauchly’s test was used to examine assumptions of sphericity for repeated measures. The data met assumptions of normality and sphericity, and thus, a repeated measures ANOVA was used to compare the changes in EATT, anthropometrics and FBS and lipid levels at the baseline and after 12 weeks between the two groups. Post hoc pairwise comparisons with a Bonferroni correction were used for significant effects by “time”, “group” or “group × time”. The data did not meet assumptions of normality of distribution, and thus, a Mann–Whitney U-test was used to compare the changes in Hs-CRP values at baseline and after 12 weeks of intervention between the intervention and control group. The mean percentage change from baseline to 12 weeks and Cohen’s “d” effect sizes were used to summarize the strength of association in study and control groups. The effect size was considered as small if d was >0.2 and <0.5, medium if d was >0.5 and <0.8 and large if d was >0.8. The statistical analysis was performed using SPSS Statistics version 15 (SPSS Inc.), and p<0.05 was set as the limit for statistical significance.
Results
A total of 85 overweight and obese individuals in intervention group and 85 overweight and mild obese individuals in control group participated in the study. The mean age of the participants in the study was 30.99. The attrition rate was 23.52% in both the groups, but the required sample size was achieved. The anthropometric parameters, blood lipids, fasting blood glucose and peak VO2 values were all comparable at the baseline between the intervention and control groups ().
Table 1 Comparison of baseline parameters between study group and control group
Table 2 Comparison of anthropometrics, EEATT and aerobic capacity at baseline and 12 weeks between intervention group (n=66) and control group (n=64)
Table 3 Comparison of the outcomes between intervention and control group at baseline and 12 weeks in females
Table 4 Comparison of the outcomes between intervention and control group at baseline and 12 weeks in males
Table 5 Comparison of FBS and lipids at baseline and 12 weeks between intervention group (n=66) and control group (n=64)
Change of EEATT, anthropometrics, lipid profile, FBS levels and peak VO2 values from baseline to post-intervention in study and control groups
EEATT values significantly reduced by −16.24% following 12 weeks of aerobic exercise along with a reduction in weight by 2.96%, BMI by 3.11% and WC by 2.29%. The study group also showed significant improvement in lipids and VO2 max (), whereas there were no significant changes seen in the control group. There was significant reduction of Hs-CRP values in study group as compared to control group in the present study. The median values of Hs-CRP reduced from 2.95 (1.80, 4.97) to 2.70 (1.55, 4.02) in the study group compared to a change of 2.90 (1.80, 4.80) to 2.95 (1.60, 5.00) in the control group after 12 weeks of study period.
Discussion
EATT measured by echocardiography was found to be reduced with moderate-intensity aerobic exercise program in the present study. Similar findings were shown in several pharmacological and non-pharmacological interventional studies conducted on EATT measured by echocardiography.Citation23 It was observed from the present study that EEATT values in Asian-Indian overweight and obese population are comparatively less than other ethnic populations.Citation34 However, the cutoff values for EEATT as an indicator of metabolic syndrome in Asian-Indian population are not known. As the reasons for lower EEATT values are not known, there is still uncertainty about the role of EEATT in CAD and metabolic syndrome in Indian population. Studies on exercise-induced changes in EEATT in obese Indian individuals would help in learning its clinical applicability in obesity management. It was found in the previous studies that the exercise-induced EEATT reduction was higher in magnitude compared to reduction in SAT and was similar to the amount of reduction in VAT. Most of the earlier studies were conducted in moderate-to-severe obese individuals of high-risk category. Our study was the first to investigate the exercise-induced changes in EEATT in primary prevention population.
The VAT measurement using precise and reliable methods has become an important part of interventional studies in obesity management as there is evidence on its unfavorable risk profile. The use of expensive imaging methods is limited to only few research studies and may not be practically feasible for routine clinical use. The predictive ability of VAT with EEATT measurement was found to be better than WC in an earlier study.Citation35 Although the sensitivity and specificity of EEATT are not known, it was observed that the changes of VAT and EEATT were almost similar in magnitude in one study.
In the present study, EEATT values were reduced by 16.24% with respect to change in BMI by 3.11% and reduction in WC by 2.29% (). The mean EEATT was reduced by 0.42 mm with respect to reduction of mean weight by 2.39 kg, BMI by 0.91 and WC by 2.18 cm after 12 weeks of exercise. A reduction of 2–3 cm of WC with significant reduction in the weight was associated with the reduction in EATT in the present study. EEATT values were reduced by 8.61% along with a reduction in BMI by 4.3% and WC by 4.2% in response to 12-week aerobic exercise in a study conducted by Kim et al.Citation26 The non-exercise control group and female participants were not included in this study. EEATT values were reduced by 11% after lower-intensity aerobic exercise in patients undergoing hemodialysis in a study conducted by Kenneth et al.Citation27 The magnitude of effect on EEATT was found to be higher in our study compared to the previous study conducted by Kim et al.Citation26 This could be due to participation of younger overweight and obese individuals in our study compared to the other studies. It can be well said that EEATT reduction occurs with aerobic exercise at a higher magnitude with minimal weight loss and minimal reduction in WC. EEATT reduction of 32% was achieved with a BMI reduction of 19% and WC reduction of 23% in response to 6-month low-calorie diet in a study conducted by Iacobellis et al.Citation22 It indicates that more weight loss is associated with higher amount of EEATT reduction. The reduction of EEATT values was observed in both females (0.37 mm) and males (0.55 mm) after 12 weeks of aerobic exercise, although the magnitude of effect was higher in males compared to males ( and ). The influence of gender on cardiovascular disease risk associated with the higher values of EEATT and the effect of exercise on this important risk factor are presently not known.
Although there is evidence on the effect of aerobic exercise on body fat and more specifically the VAT, the mechanism of its effect on regional adipose tissues such as EAT is not well known. The mechanisms related to visceral fat reduction in subjects with metabolic-related diseases were found to be different from subjects without metabolic-related diseases. There is limited understanding about the clinical implications of VAT reduction, and the significance of reduction in quantity of VAT translating to improvement in cardiovascular disease risk. The results in our study also support the fact that VAT is used more quickly as an energy resource than subcutaneous fat during aerobic exercise-induced weight loss. Ross and Janssen suggested that physical activity with or without weight loss was associated with a reduction in VAT.Citation36 Although there is insufficient evidence to understand the reasons for preferential VAT reduction with aerobic exercise in obese individuals, some of the probable mechanisms explained for VAT reduction include secretion of lipolytic hormones, facilitating greater post-exercise energy expenditure and fat oxidation favoring a greater negative energy balance.Citation37 As the EAT is an indicator of VAT, we presume that the same mechanisms could have caused the EEATT reduction in the present study.
EEATT values were found to be higher in obese population with dyslipidemia in various ethnic groups. Twelve-week aerobic exercise was effective in improving the metabolic parameters associated with or without significant loss in the present study. We found a significant improvement in all the metabolic parameters along with a reduction in the body fat percentage. The reduction in blood sugar levels and improvement in dyslipidemia () were associated with a reduction in EEATT values. It implies that exercise causes physiological changes in the body leading to visceral fat reduction and further improving the cardiometabolic risk profile. The evaluation of body fat and visceral fat levels with bio impedance analysis is a more reliable method to assess body composition compared to other anthropometric measures.Citation38 There was a significant improvement in visceral fat levels and body fat percentage after 12 weeks of aerobic exercise in the present study. The changes in Hs-CRP values were not statistically significant in intervention group compared to the control group. These findings agreed with the previous findings that only longer-duration exercise (more than 6 months) causes significant reduction in Hs-CRP values.
The relationship between EATT and aerobic capacity was first studied by Kim et al. The obese individuals with higher EEATT values were found to have lower aerobic capacity tested by a bicycle ergometer.Citation39 The mechanism by which EEATT influences the aerobic capacity is not known. The moderate-intensity exercise of minimum 12 weeks causes physiological changes in the body leading to an improvement in the aerobic capacity.Citation40,Citation41 We also found that there is a significant improvement in aerobic capacity which is associated with reduced EEATT values and improvement in metabolic parameters.
To the best of our knowledge, this was the first randomized controlled trial to study the efficacy of aerobic exercise on EEATT in both men and women, also in Asian-Indian population. The limitation of the study is that the normal-weight individuals with increased values of EATT were not included in the study. Future studies may focus on determining the effect of aerobic exercise on EATT in normal-weight individuals. The dose–response relation between aerobic exercise and EEATT can be further studied. The nutraceuticals are also known to influence the blood cholesterol levels and thus reduce the burden of atherosclerosis.Citation42 In the present study, the food intake during the study period was not monitored which can be considered as a confounding factor. High-volume training and high-intensity resistance training induced faster visceral loss in a study conducted by Dutheil et al.Citation43 The effect of resistance exercises and in combination with aerobic exercises with varying volumes can be studied in future. Future research should focus on studying the sensitivity and specificity of EEATT measurements in visceral fat monitoring.
Conclusion
The 12-week aerobic exercise is effective in reducing EATT measured by echocardiography. The reduction in EEATT is associated with an improvement in anthropometrics, aerobic capacity, lipid profile and Hs-CRP.
Acknowledgments
The authors acknowledge the contribution of lab assistants during the study period. The abstract of this paper was presented at the Twenty-Third Annual Scientific Congress, organized by Hong Kong College of Cardiology, held on 29–31 May 2015 in Hong Kong, and was published in the Journal of the Hong Kong College of Cardiology.
Disclosure
The authors report no conflicts of interest in this work.
References
- Baker AR Silva NF Quinn DW Human epicardial adipose tissue expresses a pathogenic profile of adipocytokines in patients with cardiovascular disease Cardiovasc Diabetol 2006 5 1 1 16412224
- Wajchenberg BL Subcutaneous and visceral adipose tissue: their relation to the metabolic syndrome Endocr Rev 2000 21 6 697 738 11133069
- Nakamura T Tokunaga K Shimomura I Contribution of visceral fat accumulation to the development of coronary artery disease in non-obese men Atherosclerosis 1994 107 2 239 246 7980698
- Matsuzawa Y Nakamura T Shimomura I Kotani K Visceral fat accumulation and cardiovascular disease Obes Res 1995 3 S5 645S 647S 8653544
- Yerramasu A Dey D Venuraju S Increased volume of epicardial fat is an independent risk factor for accelerated progression of sub-clinical coronary atherosclerosis Atherosclerosis 2012 220 1 223 230 22015177
- Iacobellis G Willens HJ Echocardiographic epicardial fat: a review of research and clinical applications J Am Soc Echocardiogr 2009 22 12 1311 1319 19944955
- Eroglu S Sade LE Yildirir A Epicardial adipose tissue thickness by echocardiography is a marker for the presence and severity of coronary artery disease Nutr Metab Cardiovasc Dis 2009 19 3 211 217 18718744
- Ahn SG Lim HS Joe DY Relationship of epicardial adipose tissue by echocardiography to coronary artery disease Heart 2008 94 3 e7 17923467
- Rabkin SW Epicardial fat: properties, function and relationship to obesity Obes Rev 2007 8 3 253 261 17444966
- Silaghi A Piercecchi-Marti MD Grino M Epicardial adipose tissue extent: relationship with age, body fat distribution, and coronaropathy Obesity (Silver Spring) 2008 16 11 2424 2430 18719675
- Willens HJ Gómez-Marín O Chirinos JA Goldberg R Lowery MH Iacobellis G Comparison of epicardial and pericardial fat thickness assessed by echocardiography in African American and non-Hispanic White men: a pilot study Ethn Dis 2008 18 2 311 316 18785445
- Misra A Pandey RM Devi JR Sharma R Vikram NK Khanna N High prevalence of diabetes, obesity and dyslipidaemia in urban slum population in northern India Int J Obes Relat Metab Disord 2001 25 11 1722 1729 11753596
- Slentz CA Aiken LB Houmard JA Inactivity, exercise, and visceral fat. STRRIDE: a randomized, controlled study of exercise intensity and amount J Appl Physiol (1985) 2005 99 4 1613 1618 16002776
- Ohkawara K Tanaka S Miyachi M Ishikawa-Takata K Tabata I A dose–response relation between aerobic exercise and visceral fat reduction: systematic review of clinical trials Int J Obes (Lond) 2007 31 12 1786 1797 17637702
- Rankinen T Kim SY Pérusse L Després JP Bouchard C The prediction of abdominal visceral fat level from body composition and anthropometry: ROC analysis Int J Obes Relat Metab Disord 1999 23 8 801 809 10490780
- Kaul S Rothney MP Peters DM Dual-energy X-ray absorptiometry for quantification of visceral fat Obesity (Silver Spring) 2012 20 6 1313 1318 22282048
- Seidell JC Bakker CJ van der Kooy K Imaging techniques for measuring adipose-tissue distribution—a comparison between computed tomography and 1.5-T magnetic resonance Am J Clin Nutr 1990 51 6 953 957 2349931
- Iacobellis G Assael F Ribaudo MC Epicardial fat from echocardiography: a new method for visceral adipose tissue prediction Obes Res 2003 11 2 304 310 12582228
- Iacobellis G Imaging of visceral adipose tissue: an emerging diagnostic tool and therapeutic target Curr Drug Targets Cardiovasc Hematol Disord 2005 5 4 345 353
- Iacobellis G Willens HJ Barbaro G Sharma AM Threshold values of high-risk echocardiographic epicardial fat thickness Obesity (Silver Spring) 2008 16 4 887 892 18379565
- Iacobellis G Sharma AM Epicardial adipose tissue as new cardiometabolic risk marker and potential therapeutic target in the metabolic syndrome Curr Pharm Des 2007 13 21 2180 2184 17627550
- Iacobellis G Singh N Wharton S Sharma AM Substantial changes in epicardial fat thickness after weight loss in severely obese subjects Obesity (Silver Spring) 2008 16 7 1693 1697 18451775
- Willens HJ Byers P Chirinos JA Labrador E Hare JM de Marchena E Effects of weight loss after bariatric surgery on epicardial fat measured using echocardiography Am J Cardiol 2007 99 9 1242 1245 17478151
- Park JH Park YS Kim YJ Effects of statins on the epicardial fat thickness in patients with coronary artery stenosis underwent percutaneous coronary intervention: comparison of atorvastatin with simvastatin/ezetimibe J Cardiovasc Ultrasound 2010 18 4 121 126 21253360
- Ismail I Keating SE Baker MK Johnson NA A systematic review and meta-analysis of the effect of aerobic vs. resistance exercise training on visceral fat Obes Rev 2012 13 1 68 91 21951360
- Kim MK Tomita T Kim MJ Sasai H Maeda S Tanaka K Aerobic exercise training reduces epicardial fat in obese men J Appl Physiol (1985) 2009 106 1 5 11 18927266
- Wilund KR Tomayko EJ Wu PT Intradialytic exercise training reduces oxidative stress and epicardial fat: a pilot study Nephrol Dial Transplant 2010 25 8 2695 2701 20190243
- Serrano-Ferrer J Crendal E Walther G Effects of lifestyle intervention on left ventricular regional myocardial function in metabolic syndrome patients from the RESOLVE randomized trial Metabolism-Clinical and Experimental 2016 65 9 1350 1360 27506742
- Warburton DE Jamnik VK Bredin SSD Gledhill N PAR-Q+ Research Collaboration The Physical Activity Readiness Questionnaire for Everyone (PAR-Q+) and electronic Physical Activity Readiness Medical Examination (ePARmed-X+) Health Fitness J Can 2011 4 2 3 17
- Heng D Ma S Lee JJ Modification of the NCEP ATP III definitions of the metabolic syndrome for use in Asians identifies individuals at risk of ischemic heart disease Atherosclerosis 2006 186 2 367 373 16112123
- Iacobellis G Willens HJ Echocardiographic epicardial fat: a review of research and clinical applications Journal of the American Society of Echocardiography 2009 22 12 1311 1319 19944955
- Rowland TW Aerobic exercise testing protocols Rowland TW Pediatric Laboratory Exercise Testing: Clinical Guidelines Champaign, IL Human Kinetics 1993 19 41
- American College of Sports Medicine ACSM’s Guidelines for Exercise Testing and Prescription Baltimore, MD Lippincott Williams & Wilkins 2013
- Xu Y Cheng X Hong K Huang C Wan L How to interpret epicardial adipose tissue as a cause of coronary artery disease: a meta-analysis Coron Artery Dis 2012 23 4 227 233 22361934
- Natale F Tedesco MA Mocerino R Visceral adiposity and arterial stiffness: echocardiographic epicardial fat thickness reflects, better than waist circumference, carotid arterial stiffness in a large population of hypertensives Eur J Echocardiogr 2009 10 4 549 555 19211568
- Ross R Janssen I Physical activity, total and regional obesity: dose-response considerations Med Sci Sports Exerc 2001 33 6 Suppl S521 S527 discussion S528–S529 11427779
- Park HS Lee K Greater beneficial effects of visceral fat reduction compared with subcutaneous fat reduction on parameters of the metabolic syndrome: a study of weight reduction programmes in subjects with visceral and subcutaneous obesity Diabet Med 2005 22 3 266 272 15717873
- Meleleo D Bartolomeo N Cassano L Evaluation of body composition with bioimpedence. A comparison between athletic and non-athletic children Eur J Sport Sci 2017 17 6 710 719 28319679
- Kim MK Tanaka K Kim MJ Epicardial fat tissue: relationship with cardiorespiratory fitness in men Med Sci Sports Exerc 2010 42 3 463 469 19952810
- Gaesser GA Rich RG Effects of high- and low-intensity exercise training on aerobic capacity and blood lipids Med Sci Sports Exerc 1984 16 3 269 274 6748925
- Wong PC Chia MY Tsou IY Effects of a 12-week exercise training programme on aerobic fitness, body composition, blood lipids and C-reactive protein in adolescents with obesity Ann Acad Med Singapore 2008 37 4 286 293 18461212
- Scicchitano P Cameli M Maiello M Nutraceuticals and dyslipidaemia: beyond the common therapeutics J Funct Foods 2014 6 11 32
- Dutheil F Lac G Lesourd B Different modalities of exercise to reduce visceral fat mass and cardiovascular risk in metabolic syndrome: the RESOLVE randomized trial Int J Cardiol 2013 168 4 3634 3642 23714599