
Abstract
Background
Although the frequency of surgical weight loss interventions has increased in Saudi Arabia, literature describing the clinical outcomes of bariatric surgery in Saudi Arabia is limited. This study aimed to assess whether weight loss intervention improves hemoglobin A1c (HbA1c) in obese patients and to identify its associated factors.
Patients and methods
A retrospective study was carried out on 318 patients with obesity class 1 or higher (body mass index [BMI] ≥ 30 kg/m2) who underwent laparoscopic sleeve gastrectomy or Roux-en-Y gastric bypass at King Abdulaziz Medical City in Riyadh, Saudi Arabia, between January 1, 2001 and March 31, 2017. Preoperatively and 12 months postoperatively, characteristics of patients were collected. BMI reduction was calculated, based on which patients were divided into three groups (0–9, 10–14, and >14 kg/m2).
Results
The postoperative HbA1c was 5.83±0.9, while the baseline level was 6.74±2.1 (P=0.001). Fifty-eight of the 318 patients had diabetes. We observed significantly higher HbA1c in diabetic than in non-diabetic patients preoperatively, whereas an insignificantly different HbA1c was observed postoperatively. Among those who had minimal reduction in BMI (0–9 kg/m2), we observed significantly higher HbA1c in diabetic than in non-diabetic patients, whereas among those who had large reduction in BMI (10–14 kg/m2) and (>14 kg/m2), we observed insignificant differences in HbA1c in diabetic than in non-diabetic patients.
Conclusion
Being a diabetic patient was related to a significant reduction in HbA1c levels postoperatively. The study suggests that the reduction in HbA1c levels could be modified by BMI, wherein greater reduction in BMI leads to greater reduction in HbA1c levels.
Introduction
Obesity is a major public health challenge in Saudi Arabia because it can pose serious health-related issues.Citation1,Citation2 In fact, its high prevalence has been projected as 41% in males and 78% in females by 2022.Citation3 It has been associated with a number of noncommunicable diseases,Citation4 which are responsible for increasing the rate of mortality in the Saudi population.Citation5 With the increased obesity prevalence in Saudi Arabia, weight loss or bariatric surgeries are becoming the most popular and effective surgical interventions in patients with obesity.
In addition to investigating substantial weight loss, several international studies have explored the associations between weight loss results from the surgical interventions and long-term health benefits such as reduction of underlying medical conditions among morbidly obese patients.Citation6–Citation19 For instance, earlier reports investigated the effectiveness of weight loss after bariatric surgery in achieving optimal glycemic control.Citation9–Citation19 According to these studies, bariatric procedures could be effective therapeutic interventions in morbidly obese patients with diabetes. However, a few other studies reported bariatric surgery may not necessarily correlate with optimal glycemic control.Citation20,Citation21
The health benefits of bariatric procedures in diabetes patients are well documented in several international studies. It has been reported that laparoscopic sleeve gastrectomy (LSG) in diabetic patients with obesity may be effective in achieving optimal glycemic control.Citation14–Citation19 Other studies reported that LSG and Roux-en-Y gastric bypass (RYGB) lead to similar improvements in plasma glucose homeostasis, insulin sensitivity, and beta-cell function in non-diabetic obese people.Citation12,Citation13
Despite the fact that bariatric surgery confirmed improved patient clinical outcome by reducing the risk of potential weight-related health problems, our understanding of the health benefits of bariatric surgery in Saudi Arabia has not yet been documented, specifically in diabetic patients. Two studies in Saudi Arabia focused only on weight reduction and one on a surgical option, which is sleeve gastrectomy.Citation22,Citation23 Another study compared weight reduction, complications, and quality of life in patients who underwent one of three surgical procedures – LSG, RYGB, and laparoscopic adjustable gastric banding.Citation24 No evidence is available on the impact of the bariatric surgery on glycemic control status (i.e., hemoglobin A1c [HbA1c]) in the Saudi population.
Recently, Ahmed et al, in a study conducted at King Abdulaziz Medical City in Riyadh, reported a hospital readmission rate of 8% and an emergency department visit rate of 14% in obese Saudi patients who underwent bariatric surgery.Citation25 According to this study, LSG was associated with fewer hospital readmissions or emergency department visits as compared to RYGB.
To date, the effectiveness of bariatric surgery has not been assessed in Saudi Arabia to obtain optimal glycemic control. Such studies on the Saudi Arabian population would be of international interest. The hypotheses of the study are the following: there is a statistically significant reduction in the HbA1c over a 1-year period after surgery among patients with diabetes. The study aimed to 1) assess whether bariatric surgery improves HbA1c in obese patients and 2) identify its associated factors in Saudi Arabia.
Patients and methods
The authors retrospectively studied 318 patients with obesity class 1 or higher BMI (≥30 kg/m2), who underwent either bariatric surgery LSG or RYGB at King Abdulaziz Medical City in Riyadh, Saudi Arabia, between January 1, 2001 and March 31, 2017. The study was approved by the Institutional Review Board at King Abdullah International Medical Research Center, Riyadh, Saudi Arabia (RC17/138/R). Patient consent to review their medical records was not required by the Institutional Review Board at King Abdullah International Medical Research Center. This study involves the use of existing information with no patient-related care responsibilities. No identifier was used, and the privacy and confidentiality of patients were completely protected.
Data for this study were retrieved from the collected medical records. The baseline and clinical characteristics included information such as age, sex, BMI (kg/m2), diabetes (Yes/No), asthma (Yes/No), obstructive sleep apnea (Yes/No), and procedure type (LSG/RYGB). The authors evaluated surgery outcomes in the study population. Available BMI and/or HbA1c readings were reviewed for patients who had visited our center and these measurements were only considered if they occurred within a period of 12 months after the surgery. In the case of multiple readings, the most recent reading was selected and recorded. Differences between the preoperative visit and postoperative visit were calculated for each reading of BMI, and HbA1c. Percent reduction was calculated for BMI and HbA1c using the formula (postoperative − preoperative)/preoperative × 100%. Also, for the purpose of the analysis, BMI reduction was classified into three groups: reduction of 9 kg/m2 or less, reduction between 10 and 14 kg/m2, and reduction of >14 kg/m2. As per the criteria of the American Diabetes Association, the authors used HbA1c ≤6.5% as the definition of achieving optimal HbA1c.
Statistical analyses
Statistical analyses were performed using SAS V 9.4 (SAS Institute, Cary, NC, USA). Categorical patient characteristics were expressed as frequency and percent, while continual patient characteristics were expressed as mean and SD. Paired sample t-tests were used to test differences in HbA1c in the whole sample (N=318). Furthermore, paired sample t-tests were used to assess the differences in HbA1c before and after the surgery, separately, and in the diabetic group and non-diabetic group. The effects of visit (pre- and postoperative) on HbA1c were also assessed. We assessed the impact of diabetes, BMI reduction, and visit on lowering HbA1c after the surgery, controlling the patient characteristics. A multivariate mixed-effects model was used to identify the interaction terms that were associated with lowering HbA1c. The following interaction terms were examined: (diabetes × visit), (diabetes × BMI reduction), and (procedure type × visit). Moreover, multiple comparisons were performed using the Tukey for significant interactions terms.
Results
The sample included 318 obese subjects who underwent surgical weight loss intervention (LSG or RYGB) during the study period. The baseline characteristics of the sample with obesity are shown in . The mean age was 34.7 years with an SD of 11.7 years, and the age ranged between 13 and 64 years. The mean of baseline BMI was 46.8 kg/m2 with an SD of 7.7 kg/m2, and the BMI ranged between 32.7 and 83 kg/m2. The mean HbA1c at baseline was 6.7 with an SD of 2.1, and HbA1c ranged between 2.5 and 14. The majority of patients (67.6%) were females, and 88.4% underwent LSG. Of the sample, 18.4% had diabetes, 13.9% had asthma, and 7.9% had obstructive sleep apnea.
Table 1 Patient characteristics (N=318)
Paired sample t-test showed significant reduction in HbA1c in the whole sample (N=318) from pre- to postoperative (6.74±2.1 preoperative vs. 5.83±0.9 postoperative, P=0.001). This analysis was stratified further by the diabetic status: we noted significantly greater reduction in HbA1c from pre- to postoperative (8.5±2.4 preoperative vs. 6.3±1.0 postoperative, P=0.001) in the diabetes group and slight but significant reduction in HbA1c (5.7±0.7 preoperative vs. 5.4±0.5 postoperative, P=0.001) in the non-diabetic group. This resulted in a reduction of 25.9% in the diabetic group and 5.3% in non-diabetic group. The individual changes in HbA1c after surgery can be found in . The waterfall plot shows that the procedure was associated with greater HbA1c reduction in patients with diabetes than in those without diabetes. Postoperatively, the HbA1c target of 6.5% or below was met in 62.5% of the diabetic group and 97.1% of the non-diabetic group.
Figure 1 Changes in HbA1c by visit, diabetes status, body mass index (kg/m2) reduction, and procedure type after bariatric surgery.
Abbreviations: BMI, body mass index; HbA1c, hemoglobin A1c; LS-means, least squares-means.
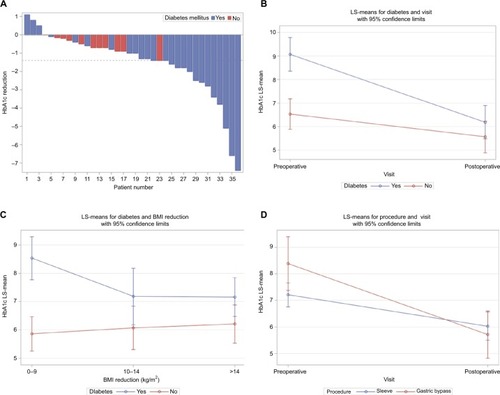
Analysis with the multivariate mixed model showed that there were insignificant differences in HbA1c by demographic characteristics: age and sex. The model demonstrated significant diabetes by visits interaction effects (P=0.001). According to Tukey multiple comparisons, diabetic patients had significantly higher HbA1c than non-diabetic patients at the baseline, whereas diabetic patients had insignificantly higher HbA1c than non-diabetic patients following the surgical procedure ().
We found significant interaction effects between diabetes by BMI reduction (10–14 kg/m2 [P=0.012] and >14 kg/m2 [P=0.003]) on HbA1c. In those who had minimal reduction in BMI (0–9 kg/m2), we observed significantly higher HbA1c levels in diabetic patients than in non-diabetic patients. In those who had greater reduction in BMI (10–14 and >14 kg/m2), we observed insignificant differences in HbA1c levels in diabetic patients than in non-diabetic patients ().
Results of the mixed-effects model analysis presented in indicate significant interaction effects between procedure type-by-visit (P=0.018) on HbA1c. There was significant difference in HbA1c within the LSG and RYGB groups between baseline and following the surgical procedure, while there was insignificant difference between the LSG and RYGB groups in the HbA1c preoperatively and postoperatively ().
Table 2 Factors associated with the change in HbA1c using mixed-effects model
Discussion
The literature describing the clinical outcomes of surgical weight loss interventions in Saudi Arabia is limited, particularly regarding the HbA1c parameter. In this study, we retrospectively gathered data on patients with obesity class I or higher (BMI ≥ 30 kg/m2) who underwent LSG and RYGB at King Abdulaziz Medical City in Riyadh, Saudi Arabia, between January 1, 2001 and March 31, 2017. The surgical weight loss interventions appear to have had a large effect on the HbA1c parameter within a short term, that is, a period of 12 months after the surgery.
In a period of 12 months postoperatively, the HbA1c target of 6.5% or below was met in 62.5% of the diabetic patients and 97.1% of the non-diabetic patients. This can be compared with patients who were on HbA1c target of 6.5% or below at baseline or prior to the procedure: 25.71% of the diabetic patients and 91.8% of the non-diabetic patients. Similar findings are found in reports from various international regions and with different follow-up periods, where they have shown rapid improvement in glycemic control after bariatric surgery.Citation9–Citation19 Thus, our data provide strong evidence for the effectiveness of bariatric surgery in improving HbA1c in a Saudi sample of patients in whom optimal HbA1c has not been investigated. Future research studies are needed to assess the effectiveness of weight reduction in treating obese patients with other comorbidities.
The uniqueness of the current study is that we were able to link the reduction in HbA1c to the diabetic status and to the reduction in BMI. For instance, at baseline, we noted significantly higher HbA1c in diabetic patients than in non-diabetic patients, whereas postoperatively, insignificant differences were noted between diabetes patients and non-diabetes patients. The reduction in HbA1c levels in our study can be explained by diabetes and the greater reduction in BMI. Among those who had minimal reduction in BMI (0–9 kg/m2), we observed significantly higher HbA1c levels in diabetic patients than in non-diabetic patients, whereas among those who had a large reduction in BMI (10–14 kg/m2) and (>14 kg/m2), we observed insignificant differences in HbA1c levels in diabetic patients than in non-diabetic patients. These findings were similar to a number of previous international reports,Citation26–Citation29 in which weight reduction led to a significant improvement of glycemic control in diabetic patients who underwent bariatric surgery.
Although we noted significant reduction in HbA1c within the LSG and RYGB groups between preoperative and postoperative periods, in agreement with our analysis results,Citation30,Citation31 both LSG and RYGB had a similar effect on the reduction of HbA1c levels postoperatively. LSG seems to be a promising weight loss procedure in our center, as 88.4% of our patients underwent this procedure. A long-term longitudinal study is needed to compare and evaluate the effectiveness of these procedures in achieving early optimal glycemic control after surgery.
The current study was limited by its nature, that is, retrospective chart review, as not all data were available during the 12-month period after surgery. We did not retrieve data on the types and dose of insulin prescribed to diabetes patients. Data were collected only preoperatively and postoperatively, rather than by using multiple records: baseline, 3, 6, and 12 months. Despite these limitations, the study findings represent preliminary highlights of the clinical outcomes of bariatric surgery on achieving optimal glycemic control in Saudi Arabia, as none of the studies have evaluated metabolic comorbidities in this population.
Conclusion
A significant reduction in HbA1c levels at postoperative was noted in diabetic patients. The study suggests that reduction in HbA1c levels could be modified by BMI, wherein greater reduction in BMI leads to greater reduction in HbA1c levels. Large longitudinal studies on the long-term clinical outcomes of the surgical weight loss interventions are warranted, specifically assessing remission of other comorbidities that are related to obesity.
Acknowledgments
We would like to thank King Abdullah International Medical Research Center, Riyadh, Saudi Arabia, for approving the study.
Disclosure
The authors report no conflicts of interest in this work.
References
- Baslaim G Bashore J Alhoroub K Impact of obesity on early outcomes after cardiac surgery: experience in a Saudi Arabian center Ann Thorac Cardiovasc Surg 2008 14 6 369 375 19131923
- Al-Hazzaa HM Prevalence and trends in obesity among school boys in Central Saudi Arabia between 1988 and 2005 Saudi Med J 2007 28 10 1569 1574 17914521
- Al-Quwaidhi AJ Pearce MS Critchley JA Sobngwi E O’Flaherty M Trends and future projections of the prevalence of adult obesity in Saudi Arabia, 1992–2022/Tendances et projections de la prévalence de l’obésité chez l’adulte en Arabie saoudite, 1992–2022 East Mediterr Health J 2014 20 10 589 595 25356689
- Al-Daghri NM Alkharfy KM Al-Attas OS Association between type 2 diabetes mellitus-related SNP variants and obesity traits in a Saudi population Mol Biol Rep 2014 41 3 1731 1740 24435973
- Aldawood A Arabi Y Dabbagh O Association of obesity with increased mortality in the critically ill patient Anaesth Intensive Care 2006 34 5 629 633 17061639
- Sudan R Nguyen NT Hutter MM Brethauer SA Ponce J Morton JM Morbidity, mortality, and weight loss outcomes after reoperative bariatric surgery in the USA J Gastrointest Surg 201519 1 171 179
- Herman KM Carver TE Christou NV Andersen RE Keeping the weight off: physical activity, sitting time, and weight loss maintenance in bariatric surgery patients 2 to 16 years postsurgery Obes Surg 2014 24 7 1064 1072 24682779
- Douglas IJ Bhaskaran K Batterham RL Smeeth L Bariatric surgery in the United Kingdom: a cohort study of weight loss and clinical outcomes in routine clinical care PLoS Med 2015 12 12 e1001925 26694640
- le Roux CW Aylwin SJ Batterham RL Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters Ann Surg 2006 243 1 108 114 16371744
- Caballero MA Jiménez JM Castro MJ Solórzano JO Arango A Outcomes in weight loss, fasting blood glucose and glycosylated hemoglobin in a sample of 415 obese patients, included in the database of the European accreditation council for excellence centers for bariatric surgery with laparoscopic one anastomosis gastric bypass Nutrición hospitalaria: Organo oficial de la Sociedad española de nutrición parenteral y enteral 2014 30 5 1032 1038
- Abegg K Corteville C Docherty NG Effect of bariatric surgery combined with medical therapy versus intensive medical therapy or calorie restriction and weight loss on glycemic control in Zucker diabetic fatty rats Am J Physiol Regul Integr Comp Physiol 2015 308 4 R321 R329 25540099
- Bradley D Magkos F Eagon JC Matched weight loss induced by sleeve gastrectomy or gastric bypass similarly improves metabolic function in obese subjects Obesity 2014 22 9 2026 2031 24891156
- Woelnerhanssen B Peterli R Steinert RE Peters T Borbély Y Beglinger C Effects of postbariatric surgery weight loss on adipokines and metabolic parameters: comparison of laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy—a prospective randomized trial Surg Obes Relat Dis 2011 7 5 561 568 21429816
- Chondronikola M Harris LL Klein S Bariatric surgery and type 2 diabetes: are there weight loss-independent therapeutic effects of upper gastrointestinal bypass? J Intern Med 2016 280 5 476 486 27739136
- Faucher P Poitou C Carette C Bariatric surgery in obese patients with type 1 diabetes: effects on weight loss and metabolic control Obes Surg 2016 26 10 2370 2378 26886929
- Leung M Xie M Durmush E Leung DY Wong VW Weight loss with sleeve gastrectomy in obese type 2 diabetes mellitus: impact on cardiac function Obes Surg 2016 26 2 321 326 26091811
- Liu SY Wong SK Lam CC Yung MY Kong AP Ng EK Long-term results on weight loss and diabetes remission after laparoscopic sleeve gastrectomy for a morbidly obese Chinese population Obes Surg 2015 25 10 1901 1908 25761944
- Hoogerboord M Wiebe S Klassen D Ransom T Ellsmere J Laparoscopic sleeve gastrectomy: perioperative outcomes, weight loss and impact on type 2 diabetes mellitus over 2 years Can J Surg 2014 57 2 101 24666447
- Reis CE Alvarez-Leite JI Bressan J Alfenas RC Role of bariatric-metabolic surgery in the treatment of obese type 2 diabetes with body mass index <35 kg/m2: a literature review Diabetes Technol Ther 2012 14 4 365 372 22176155
- Chuang J Zeller MH Inge T Crimmins N Bariatric surgery for severe obesity in two adolescents with type 1 diabetes Pediatrics 2013 132 4 e1031 e1034 24062368
- To VT Hüttl TP Lang R Piotrowski K Parhofer KG Changes in body weight, glucose homeostasis, lipid profiles, and metabolic syndrome after restrictive bariatric surgery Exp Clin Endocrinol Diabetes 2012 120 09 547 552 23070831
- Bawahab MA Assiri AS Maksoud WA Effects of weight reduction after sleeve gastrectomy on metabolic variables in Saudi obese subjects in Aseer Province of Kingdom of Saudi Arabia Obes Surg 2017 27 8 2005 2014 28224472
- Aldaqal SM Sehlo MG Self-esteem and quality of life in adolescents with extreme obesity in Saudi Arabia: the effect of weight loss after laparoscopic sleeve gastrectomy Gen Hosp Psychiatry 2013 35 3 259 264 23466348
- Al Kadi A Siddiqui ZR Malik AM Al Naami M Comparison of the efficacy of standard bariatric surgical procedures on Saudi population using the bariatric analysis and reporting outcome system Saudi Med J 2017 38 3 251 256 28251219
- Ahmed A AlBuraikan D ALMuqbil B AlJohi W Alanazi W AlRasheed B Readmissions and emergency department visits after bariatric surgery at Saudi Arabian Hospital: the rates, reasons, and risk factors Obes Facts 2017 10 5 432 443 28988235
- Cheng V Kashyap SR Schauer PR Kirwan JP McCrae KR Restoration of glycemic control in patients with type 2 diabetes mellitus after bariatric surgery is associated with reduction in microparticles Surg Obes Relat Dis 2013 9 2 207 212 22093380
- Buchwald H Estok R Fahrbach K Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis Am J Med 2009 122 3 248 256 19272486
- Dorman RB Serrot FJ Miller CJ Case-matched outcomes in bariatric surgery for treatment of type 2 diabetes in the morbidly obese patient Ann Surg 2012 255 2 287 293 21975321
- Diniz MD Diniz MT Sanches SR Glycemic control in diabetic patients after bariatric surgery Obes Surg 2004 14 8 1051 1055 15479592
- Tang Q Sun Z Zhang N Xu G Song P Xu L Tang W Cost-effectiveness of bariatric surgery for type 2 diabetes mellitus: a randomized controlled trial in China Medicine (Baltimore) 2016 95 20 e3522 27196454
- Cutolo PP Nosso G Vitolo G Brancato V Capaldo B Angrisani L Clinical efficacy of laparoscopic sleeve gastrectomy vs laparoscopic gastric bypass in obese type 2 diabetic patients: a retrospective comparison Obes Surg 2012 22 10 1535 1539 22960950