
Abstract
Purpose
The high prevalence of metabolic syndrome (MetS), prediabetes, and increased risk of cardiovascular diseases linked with prolonged sitting has created a need to identify options to limit sedentary behaviors. A potentially simple approach to achieve this goal in the university setting is to provide students the option to stand during courses rather than sit. The purpose of the present study was to examine the effects of standing in the college classroom setting on cardiometabolic risk factors in a cohort of college students.
Patients and methods
Healthy college students (n=21) who attended at least two courses per week (a minimum of 5 hours) in a specified university building with standing desks participated in a 7-week intervention that was divided into three phases: 3 weeks of standing, 1 week of washout (sitting), and 3 weeks of sitting. The participants (mean ± SD: age, height, weight, body mass index, and waist-to-hip ratio were 22.7±6.4 years, 174.3±10.0 cm, 70.6±14.3 kg, 23.0±3.0 kg/m2, and 0.76±0.05, respectively) were randomly assigned to the phase of intervention of which they should start (sitting or standing), and all participants engaged in sitting during the washout phase. Cardiometabolic risk factors and metabolic equivalents (METs) were measured at baseline and weekly throughout the intervention.
Results
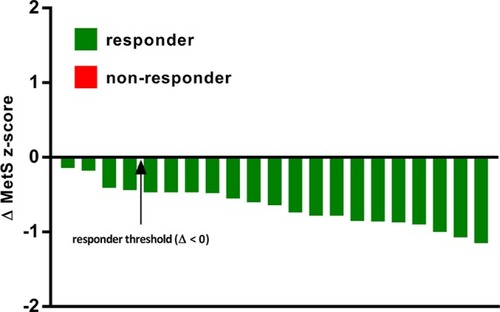
Paired t-tests revealed significant differences (P<0.05) in all cardiometabolic risk factors between the 3 weeks of sitting and 3 weeks of standing time blocks. Moreover, MetS z-score was significantly improved (P<0.05) during the 3 weeks of standing (–5.91±2.70) vs 3 weeks of sitting (–5.25±2.69). The METs were significantly higher (P<0.05) during standing (1.47±0.09) than during sitting (1.02±0.07). Although there was considerable interindividual variability in the ∆ MetS z-score response, there was a 100% (21/21) incidence of a favorable change (ie, responders) in MetS z-score response.
Conclusion
A standing desk in the classroom paradigm was found to significantly improve cardiometabolic health throughout a short 3 weeks time span. Increasing standing time in the classroom, and therefore lessening weekly sedentary behavior, could be a potential wide-scale, effective strategy for primordial prevention of cardiometabolic diseases.
Introduction
Cardiovascular disease (CVD) is widespread in the US, but it is largely preventable with changes in lifestyle. The most prominent risk factors for CVD are dyslipidemia, physical inactivity, and obesity.Citation1 Within a university setting, college students are a population perceived to be relatively healthy and have low risk for such diseases due to their younger age and being relatively active, but this may be a misconception. Unfortunately, many students are unaware of the presence of these risk factors because of infrequent testing and appearing to have a healthier lifestyle; however, much of their time is spent sitting during courses, studying, and exhibiting sedentary behaviors as a whole due to them being students. For example, Dalleck and KjellandCitation2 found that 6.8% of college students had metabolic syndrome (MetS), 13.0% had two risk factors for MetS, and 42.5% of the sample exhibited one risk factor for MetS. For an average adult, the recommended guideline for physical activity (PA) is 2.5 hours of moderate-intensity aerobics per week. Individuals can meet the recommended PA guidelines, but still live a less-than-ideal lifestyle. Sedentary individuals who follow the weekly recommendations for PA, but are sedentary for great lengths throughout the day, are at a higher risk for cardiometabolic diseases relative to their less sedentary counterparts who exercise the same amount.Citation3 Unfortunately, meeting the PA guidelines alone cannot overcome the negative effects of high amounts of daily sedentary behavior.
With the high prevalence of MetS, dyslipidemia, and pre-diabetes and an increase in the risk of CVD due to prolonged sedentary behavior, there is a need to include options to limit these sedentary behaviors, especially in a university setting. A simple approach to achieve this goal is to provide students the option to stand during courses rather than sit. A recent publication on the feasibility of standing desks in a university-based classroom found that 95% of students preferred the option to stand.Citation4 Therefore, standing desk could be a simple way to lessen the negative cardiometabolic effects of increased sedentary behavior. To our knowledge, there have been no prior studies investigating the effectiveness of standing desks in the university setting. The purpose of the present study was to assess the effectiveness of a standing desk university classroom model for attenuating cardiometabolic risk in a cohort of college students. It was hypothesized that incorporating standing desks into the university classroom setting will improve the cardiometabolic risk factor profile of college students.
Materials and methods
Participants
Participants (n=21) were recruited through poster advertisement, word-of-mouth, and email between November 2017 and January 2018. The characteristics of participants who completed the study (n=21) are shown in . Each participant was asked to read and sign an informed consent form outlining the study procedures and goals of the study, and agreeing that her/his participation was voluntary. Additionally, each participant was informed verbally and in writing that the consent could be withdrawn at any time without any consequence. Inclusion criteria were: 1) ≥18 years old and 2) a college student at Western State Colorado University with at least two classes in a single, specified building on campus. Exclusion criteria were: 1) pregnancy and 2) an injury/medical condition that would prevent standing for an extended period of time. This study was approved by the Human Research Committee of Western State Colorado University (HRC2017-02-02R03).
Table 1 Participant characteristics (values are mean ± SD and %)
Experimental design
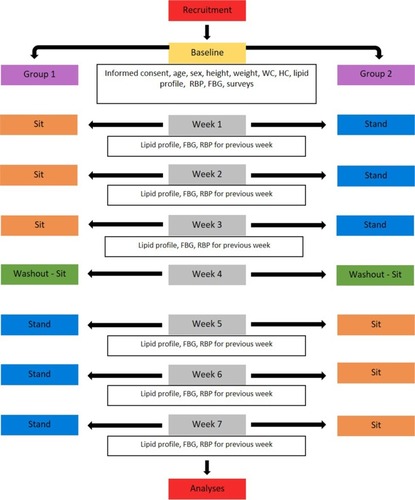
This randomized, crossover trial was designed to evaluate the effects of increased standing time on various cardiometabolic markers, including fasting blood glucose, high-density lipoprotein (HDL) cholesterol, triglycerides, and SBP/DBP. Data were collected from January to March 2018. All participants were part of the intervention and served as their own controls. The intervention trial required standing during at least two different class periods per week, utilizing standing desks; this totaled to a minimum of 5 hours per week of standing for 3 weeks. The control trial required sitting in the same two classes for 3 weeks. The control and intervention trials were separated by a one-week washout period in which all participants were required to sit. The participants were randomized to the trial which they would start with first.
At baseline, measures were obtained for the following variables: age, height, weight, waist circumference, hip circumference, resting blood pressure, and fasting lipids/blood glucose. Additionally, each participant also filled two survey questionnaires regarding PA and sedentary behavior: International Physical Activity Questionnaire and Sedentary Behavior Questionnaire. Each week throughout the study, with the exception of the washout week, fasting blood glucose and lipid profiles and resting blood pressure were measured. Further, on one occasion in the intervention, a metabolic cart was used to measure gas exchange data between standing and sitting for each participant to establish metabolic demands of the activities. A flow diagram of the experimental design outlining the timing of measurements throughout the duration of the study is presented in .
Figure 1 Experimental flowchart.
Procedures
Anthropometric measurements
All anthropometric measurements were obtained using standardized guidelines.Citation5 The participants were weighed to the nearest 0.1 kg on a medical-grade scale and measured for height to the nearest 0.5 cm using a stadiometer. Waist and hip circumference measurements were obtained using a cloth tape measure with a spring-loaded handle (Creative Health Products, Ann Arbor, MI, USA). For waist circumference, a horizontal measurement was taken at the narrowest point of the torso (below the xiphoid process and above the umbilicus). Hip circumference measures were obtained at the point where the buttocks extended the maximum when viewed from the side. Measurements of each site (ie, waist and hip) were taken three times before averages were calculated and recorded. Waist-to-hip ratios were calculated using the averages.
Fasting blood lipid and blood glucose measurement
A fasting blood sample was collected and analyzed for the measurement of blood lipid profile and glucose. Participants’ hands were washed with soap and rinsed thoroughly with water, then cleaned with alcohol swabs, and allowed to dry. Skin was punctured using lancets, and a fingerstick sample was collected into heparin-coated 40 µL capillary tube. Blood was allowed to flow freely from the fingerstick into the capillary tube without milking of the finger. The samples were then dispensed immediately onto commercially available test cassettes for analysis in the Cholestech LDX System (Alere Inc., Waltham, MA, USA) according to strict standardized operating procedures. The Cholestech LDX system measured total cholesterol, HDL cholesterol, low-density lipoprotein cholesterol, triglycerides, and blood glucose in the fingerstick blood. A daily optics check was performed on the Cholestech LDX analyzer.
Resting blood pressure measurement
The procedures for measuring resting blood pressure outlined elsewhere were followed.Citation5 Briefly, the participants were seated quietly for 5 minutes in a chair with a back support with feet on the floor and arm supported at the heart level. The left arm brachial artery blood pressure was measured using a sphygmomanometer in duplicate at 1-minute interval. The mean of the two measurements was reported for baseline and weekly values.
MetS z-score
A continuous risk score assessment scale (MetS z-score) was used previously to identify changes in MetS risk factors following an exercise intervention.Citation6 The MetS severity was presented as sex-specific MetS z-score calculated using the following equations:Citation7 1) MetS z-scoremen =[(40−HDL-C)/8.9]+[(TG −150/69)]+[(FG −100)/17.8]+[(WC −102)/11.5]+[(MAP −100)/10.1]; 2) MetS z-scorewomen =[(50−HDL-C)/14.5]+[(TG −150/69)]+[(FG −100)/17.8]+[(WC −88)/12.5]+[(MAP −100)/10.1], where FG = fasting glucose, HDL-C = high-density lipoprotein cholesterol, MAP = mean arterial pressure, TG = triglycerides, and WC = waist circumference.
Standing desk protocol
The standing desks were located within the Department of Recreation, Exercise, and Sport Science at the local university. All participants used the standing desks for 3 weeks in two of their classes, totaling to a minimum of 5 hours per week. The participants were instructed not to lean on the desks or other stationary items while using the desk to avoid contamination of results during data collection. They were also encouraged not to stand outside of their requirements for this study nor did they keep a log. The participants were asked each week at the lipid profile test regarding whether they attended their classes, stood in their classes, and left early from class; total hours of standing per week were recorded.
Measurement of the metabolic equivalents (METs) of sitting and standing
The participants were required to attend a 1-hour metabolic testing session to measure the METs of sitting and standing. Because numerous factors affect the true resting metabolic rate, the participants were required to refrain from eating for 2–4 hours before the test, from consuming caffeine for at least 4 hours before the test, and from exercising. The test was rescheduled if the participant felt ill. The sessions occurred in this order: 1) seated at a desk for 20 minutes and 2) standing at a standing desk for 20 minutes with a 5-minute break between each session. During each 20-minute session, the participant was asked not to talk or laugh. The participants could read, write, text, or watch videos if the activity was relaxing. At the start of each 20-minute session, the participants were instructed to wear a mask apparatus with a breathing valve to collect expired gases. Expired gases were collected using the Parvo Medics TrueOne 2400 Metabolic Measurement System (Sandy, UT, USA). For analyses, the METs of the last 5 minutes of each sitting and standing session were averaged and recorded. A visual depiction of the protocol for the measurement of standing METs is shown in .
Figure 2 A study participant with the attached Parvo Medics metabolic analyzer during the measurement of standing METs.

Statistical analysis
All analyses were performed using SPSS Version 25.0 (IBM Corporation, Armonk, NY, USA). All variables were initially checked for normality using the Kolmogorov– Smirnov test. Measures of centrality and spread are presented as mean ± SD. Mean cardiometabolic measures representative of the 3 weeks of sitting and 3 weeks of standing were calculated using the data collected from the weekly assessments. Next, MetS z-scores representative of the 3-week blocks of sitting and standing were determined. Differences in cardiometabolic factors and MetS z-scores between standing and sitting were analyzed with paired t-tests. Likewise, the difference in METs between standing and sitting was analyzed with a paired t-test. Lastly, the mean difference in MetS z-score between sitting and standing was calculated. To determine individual MetS z-score responsiveness to standing, delta values (Δ) were calculated (standing minus sitting) to establish the change (Δ) in MetS z-score. Subsequently, the participants were categorized as a “responder” if Δ was <0 or “nonresponder” if Δ was >0. The alpha level of statistical significance was set at P<0.05 for all analyses.
Results
All analyses and data presented in the results are for those participants (n=21) who completed the intervention. One participant dropped out of the study because of a medical leave of absence from school not associated with the study. All participants acted as their own control in this crossover-design study. The participants were randomly assigned to sit or stand for 3 weeks followed by a 1-week (sitting) washout and 3 weeks of the opposite condition to the first 3 weeks. Both phases were well tolerated by all participants.
Lifestyle
As illustrated in , the sample on average exercised greater than the minimum recommendations by the American College of Sports Medicine.Citation5
Table 2 Physical activity and sedentary behavior (mean ± SD) based on the International Physical Activity Questionnaire and Sedentary Behavior Questionnaire
Cardiometabolic risk factors and METs
The mean measurements for cardiometabolic risk factors for 3 weeks of sitting and 3 weeks of standing along with METs are presented in . Paired t-tests revealed significant differences (P<0.05) in all cardiometabolic risk factors between the 3 weeks of sitting and 3 weeks of standing time blocks. Moreover, MetS z-score was significantly improved (P<0.05) during the 3 weeks of standing vs 3 weeks of sitting. The METs were significantly higher (P<0.05) during standing than during sitting.
Table 3 Cardiometabolic and metabolic variables for sitting and standing (mean ± SD) and mean differences (95% CI) between postures
Interindividual variability in MetS z-score responses to standing
The incidence of MetS z-score responders and nonresponders to standing in the classroom when compared to sitting is presented in . Although there was considerable interindividual variability in the ∆ MetS z-score response, there was a 100% (21/21) incidence of a favorable change (ie, responders) in MetS z-score response.
Figure 3 Interindividual variability in Δ MetS z-score responses to standing when compared to sitting.
Discussion
The main finding of the present study was that a standing desk in the classroom paradigm significantly improved cardiometabolic health in a cohort of university students throughout a short 3 weeks time span. Overall, the intervention was well tolerated and therefore may be a promising modality to improve the cardiometabolic health profile of students who engage in high levels of sedentary behavior. Increasing standing time in the classroom, and therefore lessening weekly sedentary behavior, could be a potential, wide-scale, effective strategy for primordial prevention of cardiometabolic diseases.
The active couch potato lifestyle
In recent years, the term “active couch potato” has been used to describe people who meet PA recommendations yet spend the remainder of their waking hours engaged in primarily sedentary behaviors. Indeed, indicates that the participants in the present study likely could be categorized as “active couch potatoes”. It has been demonstrated that a negative dose–response relationship exists between sedentary behavior and waist circumference, blood pressure, and blood glucose levels, further emphasizing that sedentary behavior is a risk factor independent from physical inactivity.Citation8 Moreover, the amount of time spent in sedentary behaviors is positively correlated with all-cause mortality, type 2 diabetes, cancer, high body mass index, CVD, and MetS.Citation9 Therefore, for participants in the current sample and others in the population who spend the majority of their waking hours sedentary, exercising for an hour may not be enough to stave off the deleterious cardiometabolic effects from prolonged sitting.
Cardiometabolic risk factors
The relationship between sedentary behavior and cardio-metabolic disease risk is well established.Citation8,Citation10,Citation11 From the findings of the present study and those of other studies, adjusting the physical environment of schools and offices can have a major impact with regard to health outcomes in students and workers alike. As more and more time per day is dedicated to low MET activities (≤1.5 METs), in the name of productivity and/or entertainment, increasing standing time may be a simple, yet effective way to decrease the negative cumulative health consequences of prolonged sitting. To date, the present study is the first to assess the effects of increasing standing time on cardiometabolic risk factors in college students. Other studies on college students in this topic have focused on cognitionCitation12 and energy expenditureCitation13 while at active workstations. As these studies differ in methodology and intention, it is difficult to relate them to the present study. However, on the basis of previous research on office workers, together with the present study, we can extrapolate and derive some conclusions on the efficacy of incorporating standing desks into the school/work environment. In this study, the participants were relatively healthy (), and yet, they experienced widespread subtle improvements in cardiometabolic health with reduced sitting. It may be surmised that the changes seen in a less healthy cohort would be greater. Indeed, several authors have reported that a standing intervention elicits improvements in various cardiometabolic risk factors such as HDL cholesterol,Citation14 total cholesterol, and DBP.Citation15 With regard to energy expenditure and substrate utilization, Gao et alCitation10 found a significant increase in muscle activity (49.4%), energy expenditure (9.2%), and fat oxidation (fat usage increased from 39.4% to 48.3% and carbohydrate usage decreased from 60.6% to 51.7%) when standing compared to that when sitting in 18 Finnish, female, middle-aged office workers (49.4±7.9 years). The increase in fat oxidation is vital as it may lead to improved insulin sensitivity over time, which is a primary goal when targeting reduced cardiometabolic disease risk. Additionally, increasing muscle activity and energy expenditure with each day, week, and year may result in gradual and sustained long-term improvements in one’s lifetime cardiometabolic profile.
Primordial prevention
To take a step in the other direction, with regard to primordial prevention, as mentioned previously, the present study group was reasonably healthy and they still saw a positive change. This raises the question – are we too late in looking at college students? What would the cardiometabolic profiles of college students look like had they been standing in class since kindergarten? The current trend in primary education is to provide different “workstation” options for children, where they can choose to sit or stand. As children progress, however, through secondary school and then into college, the norm is to keep people in their seats. Therefore, by the time one enters the workplace, these habits are well formed and the road to poor health has been set in motion. The good news is that, on the basis of the modest yet significant changes seen in this study with 3 weeks of standing in the classroom, regardless of when sitting behavior changes during the lifespan, cardiometabolic risk factors may be reduced, reversed, or even prevented all together.
Cardiometabolic outcomes: standing vs exercise training
Interestingly, positive modifications in the cardiometabolic profile observed in the present study that occurred over the course of 3 weeks of classroom standing () are comparable to modifications reported in the literature with regular aerobic exercise training. For example, the chronic benefits from aerobic exercise training in terms of blood pressure reduction are a decrease of 3 and 2 mmHg in SBP and DBP, respectively, after anywhere between 1 and 6 months of training.Citation16 Although these changes appear rather unassuming, it has been demonstrated that a blood pressure decrease of as little as 2 mmHg is associated with a 6% decrease in stroke mortality and a 4% decrease in coronary artery disease.Citation17 Three months of aerobic exercise training has been linked to increase in HDL cholesterol of 2–8 mg/dL.Citation18 This positive modification of the lipid profile yields important overall health benefits as it has been estimated that for every 1 mg/dL increase in HDL cholesterol, the risk of a coronary heart disease event is reduced by 2%–3%.Citation19 Triglycerides can also be attenuated following several months of regular exercise training with typical reductions between 5 and 38 mg/dL.Citation18
Methodological considerations
Thus far, the research design of studies on increasing standing time in office and other settings has been inconsistent in controlling for standing time as well as length of intervention. Despite methodological differences across studies, an emerging theme is that decreasing sitting time (and concomitantly increasing standing time) appears to be beneficial in improving cardiometabolic risk factors and increasing energy expenditure. To fully understand the impact of changing the work environment to include more standing time, it is imperative to have consistency with regard to the number of hours per day spent standing. Additionally, understanding the time component, with regard to weeks of standing, to elicit positive change in the cardiometabolic profile of sedentary adults is also needed.
Conclusion
The relationship between sedentary behavior and cardiometabolic disease risk is well established. As such, the results of the current study provide encouraging preliminary evidence that subtly adjusting the classroom environment to promote increased standing time and decreased sitting time can help improve cardiometabolic health of students in the university setting. A standing desk in the classroom paradigm could be a potential, wide-scale, effective strategy for primordial prevention of cardiometabolic diseases.
Acknowledgments
This study was supported by a grant from the American Council on Exercise.
Disclosure
The authors report no conflicts of interest in this work.
References
- Schilter JM Dalleck LC Fitness and fatness: indicators of metabolic syndrome and cardiovascular disease risk factors in college students? J Exerc Physiol Online 2010 13 29 39
- Dalleck LC Kjelland EM The prevalence of metabolic syndrome and metabolic syndrome risk factors in college-aged students Am J Health Promot 2012 27 1 37 42 22950924
- Yates T Wilmot EG Khunti K Biddle S Gorely T Davies MJ Stand up for your health: Is it time to rethink the physical activity paradigm? Diabetes Res Clin Pract 2011 93 2 292 294 21507499
- Benzo RM Gremaud AL Jerome M Carr LJ Learning to stand: the acceptability and feasibility of introducing standing desks into college classrooms Int J Environ Res Public Health 2016 13 8 823
- Riebe D Ehrman JK Liguori G Magal M ACSM’s Guidelines for Exercise Testing and Prescription 10th ed Baltimore, MD Lippincott Williams & Wilkins 2018
- Ramos JS Dalleck LC Borrani F Low-volume high-intensity interval training is sufficient to ameliorate the severity of metabolic syndrome Metab Syndr Relat Disord 2017 15 7 319 328 28846513
- Malin SK Nightingale J Choi SE Chipkin SR Braun B Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults Obesity (Silver Spring) 2013 21 1 93 100 23505172
- Maddison R Jiang Y Foley L Scragg R Direito A Olds T The association between the activity profile and cardiovascular risk J Sci Med Sport 2016 19 8 605 610 26320386
- Lee PH Wong FK The association between time spent in sedentary behaviors and blood pressure: a systematic review and meta-analysis Sports Med 2015 45 6 867 880 25749843
- Gao Y Silvennoinen M Pesola AJ Kainulainen H Cronin NJ Finni T Acute metabolic response, energy expenditure, and EMG activity in sitting and standing Med Sci Sports Exerc 2017 49 9 1927 1934 28463899
- Macewen BT Saunders TJ Macdonald DJ Burr JF Sit-stand desks to reduce workplace sitting time in office workers with abdominal obesity: a randomized controlled trial J Phys Act Health 2017 14 9 710 715 28513245
- Bantoft C Summers MJ Tranent PJ Palmer MA Cooley PD Pedersen SJ Effect of Standing or Walking at a Workstation on Cognitive Function: A Randomized Counterbalanced Trial Hum Factors 2016 58 1 140 149 26408647
- Fountaine CJ Johann J Skalko C Liguori GA Metabolic and energy cost of sitting, standing, and a novel sitting/stepping protocol in recreationally active college students Int J Exerc Sci 2016 9 2 223 229 27182423
- Alkhajah TA Reeves MM Eakin EG Winkler EA Owen N Healy GN Sit-stand workstations: a pilot intervention to reduce office sitting time Am J Prev Med 2012 43 3 298 303 22898123
- Graves LEF Murphy RC Shepherd SO Cabot J Hopkins ND Evaluation of sit-stand workstations in an office setting: a randomised controlled trial BMC Public Health 2015 15 1145 26584856
- Fagard RH Exercise is good for your blood pressure: effects of endurance training and resistance training Clin Exp Pharmacol Physiol 2006 33 9 853 856 16922820
- Chobanian AV Bakris GL Black HR National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report JAMA 2003 289 19 2560 2572 12748199
- Durstine JL Grandjean PW Davis PG Ferguson MA Alderson NL Dubose KD Blood lipid and lipoprotein adaptations to exercise: a quantitative analysis Sports Med 2001 31 15 1033 1062 11735685
- Pasternak RC Grundy SM Levy D Task force 3: Spectrum of risk factors for CHD J Am Coll Cardiol 1990 27 964 1047