
Abstract
Background
Diabetes mellitus (DM) is a metabolic disorder characterized by chronic hyperglycemia due to either insulin deficiency or resistance or both. Hyperglycemia induces tissue damage through mitochondrial superoxide production, affecting retina, glomerulus, and neurons. It requires continuing medical care and ongoing self-care management to prevent and delay acute and long-term complications. Therefore, our study was designed to assess glycemic control and diabetes complications among diabetes patients attending at University of Gondar Hospital.
Materials and methods
A cross-sectional study was conducted among DM patients attending at University of Gondar Hospital diabetes follow-up clinic during February–March 2017. Five milliliters of blood was collected using aseptic technique. Levels of fasting blood sugar (FBS), triglycerides, and cholesterol were measured using MINDRAY BS-200E machine. FBS ≥152 mg/dL was taken as poor glycemic control. Binary and multivariable logistic regression models were used to evaluate associated risk factors for the outcome variable. A P-value of <0.05 was considered as statistically significant.
Result
Three hundred sixty-seven diabetes patients were included in this study. About 222 (60.5%) of them had poor glycemic control (FBS ≥152 mg/dL). The proportion of poor glycemic control was slightly higher among type 1 DM patients (61.4%) than type 2 DM patients (59.8%). Age ≥65 years (adjusted odds ratio [AOR]: 0.070; 95% CI: 0.016–0.308), being divorced (AOR: 0.226; 95% CI: 0.064–0.8000), and increased waist circumference (AOR: 0.361: 95% CI: 0.181–0.720) were factors that significantly reduce poor glycemic control. Diabetes complications were slightly higher in insulin- and tablet-only users, 72.5% and 64.5%, respectively. DM complications were also higher in patients who had poor glycemic control (61/222) and type 2 diabetes (78 [37.3%]).
Conclusion
Prevalence of poor glycemic control and DM complications was high, which indicate that appropriate intervention is required to improve glycemic control and prevent or control complications among DM patients.
Introduction
Diabetes mellitus (DM) is a group of metabolic disorders characterized by hyperglycemia due to failure in secretion, action, or both of insulin.Citation1 Chronic noncommunicable diseases are becoming considerable 21st century global epidemic and have already become the leading causes of death and disability worldwide.Citation2 A total of 415 million adults were estimated to live with diabetes in 2015 and the number is expected to reach 640 million by the year 2040 worldwide. In seven International Diabetes Federation regions, the highest regional unadjusted prevalence was seen in the North America and Caribbean (11.5%), and Africa has the lowest (3.8%) prevalence. However, Africa is projected to have the largest proportional increase by 2040, with 147% increment. In Ethiopia, the prevalence of diabetes is expected to be 5.1% in 2035 from 4.4% in 2013.Citation3
Chronic hyperglycemia of diabetes is associated with long-term damage, dysfunction, and failure of different organs.Citation1
Based on the pathophysiology, DM complications are classified as microvascular (small blood vessels damage) and macrovascular (arterial damage) complications.Citation1,Citation4 Thus, diabetes is the leading cause of blindness, end-stage renal disease, and stroke, which are common among diabetic patients.Citation5
Hyperglycemia is a biochemical parameter seen in all types of diabetes patients, which induces tissue damage through mitochondrial superoxide production.Citation4,Citation6 Capillary endothelial cells in the retina, mesangial cells in the renal glomerulus, and neurons and Schwann cells in peripheral nerves are cells commonly damaged due to hyperglycemia. These cells are particularly at high risk for damage because they are unable to regulate uptake of glucose during hyperglycemia.Citation7,Citation8 Diabetic polyneuropathy develops in the case of prolonged hyperglycemia, which is associated with metabolic imbalances, accumulation of advanced glycation end products, oxidative stress, and lipid alterations.Citation9
Diabetes management targets on maintenance of optimum glucose level and prevention and early diagnosis of complications.Citation10 According to the American Diabetes Association (ADA) Standards of Medical Care in Diabetes 2017, fasting blood sugar (FBS) measurement can be used for glycemic control assessment and individuals having FBS ≥152 mg/dL are said to have poor glycemic control.Citation11
Chronic diabetes complications like retinopathy, nephropathy, neuropathy, self-reported chest pain, vision decrement, painful paresthesias, and psychiatric events result in decrement of health-related quality of life.Citation12 Appropriate glycemic control and management is fundamental to prevent and delay DM complications. Poor glycemic control is highly correlated with high burden of diabetes complications. However, data are scanty in Ethiopia, particularly in Gondar, regarding factors for poor glycemic control and the relationship between glycemic control and DM complications. Hence, this study will be used as a baseline data for further researches regarding factors associated with poor glycemic control and DM complications among diabetes patients. Therefore, the aim of this study was to assess glycemic control and DM complications among DM patients attending at University of Gondar Hospital, Northwest Ethiopia.
Materials and methods
Study area
The study was conducted at University of Gondar Hospital, which is a teaching and referral hospital located 738 km away from Addis Ababa in northwest Ethiopia. The city is a well-known tourist site with its collection of Royal castles and very ancient churches. The hospital gives a referral service with >400 beds and serving for >5 million people in northwest Ethiopia. The hospital has chronic illness follow-up clinic providing service for >8,000 diabetes patients.
Study design and subjects
Institution-based cross-sectional study was conducted from February 1 to March 30, 2017 to assess glycemic control and diabetes complications among diabetes patients attending at University of Gondar Hospital. All DM patients who visited chronic illness follow-up clinic during the study period were included until the required sample size was attained. Severely ill patients were excluded because they were unable to answer questions.
Sample size and sampling technique
The required sample size was calculated via Open Epi software using single population proportion formula by considering the following assumptions: prevalence of poor glycemic control in Gondar, Ethiopia (P=64.7%),Citation13 95% confidence level, and 5% margin of error. Therefore, the total calculated sample size was 351. DM patients who had at least 12 months follow-up in the hospital during the study period were included in this study.
Data collection and laboratory analysis
Sociodemographic data were collected by trained nurses working in the diabetes clinic of University of Gondar Hospital using a pretested semi-structured questionnaire. All study subjects were approached during their respective appointment schedule for follow-up. After interview and detailed review of their medical records, the study subjects were sent to laboratory where blood was collected for determination of FBS, total cholesterol (TC), and triglycerides (TG). Five milliliters of blood was collected using anticoagulant-free and clot-activated test tube for biochemical parameters determination. Those biochemical parameters were determined using MINDRAY BS-200E (Shenzhen Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) using its MINDRAY reagents. The manufacturer instructions were followed for each parameter.Citation14 Glucose, TG, and TC were determined using glucose oxidase, glycerokinase peroxidase, and cholesterol oxidase peroxidase methods, respectively. Glycemic control level was categorized as poor if FBS was >152 mg/dL, which is comparable with 7% HbA1C according to ADA Standards of Medical Care in Diabetes.Citation11
Anthropometric measurements
All measurements were taken using standardized techniques and calibrated equipment. Weight was measured by balance with light indoor clothing and bare foot. Height was measured using a stadiometer. Body mass index (BMI) was calculated as weight/height.Citation2 It was classified as underweight (BMI <18.5), normal (18.5≤ BMI ≤25.0), overweight (25.0≤ BMI ≤30.0), and obese (BMI ≥30).
Waist circumference (WC) was measured by placing a plastic tape to the nearest 0.5 cm horizontally, midway between the 12th rib and the iliac crest on the mid axillary line. WHO recommended three health risk categories: low risk (men, WC ≤93.9 cm; women, WC ≤79.9 cm); increased risk (men, WC =94.0–101.9 cm; women, WC =80.0–87.9 cm); and high risk (men, WC ≥102.0 cm; women, WC ≥88.0 cm or more) for DM patients.Citation15 Blood pressure (BP) was measured using calibrated automated sphygmomanometer. Cutoff point for BP was taken as >135 mmHg for systolic blood pressure and >85 mmHg for diastolic blood pressure.
Data analysis and interpretation
Data were entered into Epi Info™ version 7 software and then exported to Microsoft Excel 2013 to check its completeness and cleanness. Finally, the data were exported to SPSS version 20 software for analysis. Frequency distributions of sociodemographic, clinical, and behavioral characteristics of study subjects were explored. Continuous variables were expressed as mean ± SD and categorical variables were expressed as percentage. Binary and multivariable logistic regression models were fitted to evaluate associated risk factors for the outcome variable. All variables with a P-value of ≤0.2 were entered into a multivariable model to control the possible effect of confounders. A P-value of <0.05 was considered as statistically significant.
Ethical consideration
Ethical clearance was obtained from School of Biomedical and Laboratory Sciences Research and Ethics committee and the study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the study participants before the commencement of data collection. There was no financial compensation or provision for the study participants. To ensure confidentiality of data, the study participants were identified using codes, and unauthorized persons had no access to the collected data. Furthermore, all findings were utilized for proper management of the patients.
Results
Sociodemographic characteristics
A total of 367 individuals participated in this study. The majority of the T2DM patients were within 45–64 years old (59.8%) having a mean age of 48.6±16.6. Among the T2DM patients, majority were females (124 [59.3%]). Majority of the study participants were urban residents (269 [73.3%]), married (213 [58.0%]), orthodox Christians (325 [88.6%]), and unable to read and write (157 [42.8%]) ().
Table 1 Sociodemographic characteristics of DM patients attending at University of Gondar Hospital, northwest Ethiopia, 2017 (N=367)
Prevalence of poor glycemic control
The mean FBS level of study participants was 174.25±57.14 mg/dL. The overall prevalence of poor glycemic control was 60.5% (222/367) (95% CI: 55.6–65.7). The proportion of poor glycemic control was 61.4% among type 1 and 59.8% among type 2 DM patients. Poor glycemic control was predominant among 45–64 years age group (99 [60.7%]), in females (116 [59.8%]), in urban dwellers (157 [58.4%]), in self-employed individuals (101 [57.1%]), and among participants who cannot read and write (99 [63.1%]) ().
Table 2 Prevalence of poor glycemic control among DM patients attending at University of Gondar Hospital, northwest Ethiopia, 2017 (N=367)
Clinical and anthropometric measurements
Higher prevalence of poor glycemic control was reported among study participants with DM duration <7 years (152 [62.8%]), non-glucometer users (188 [60.6%]), and insulin-(113 [62.1%]) and tablet-only users (90 [58.1%]) ().
Table 3 Clinical and anthropometric measurements of DM patients attending at University of Gondar Hospital, northwest Ethiopia, 2017 (N=367)
Factors associated with poor glycemic control
In multivariable logistic regression model, age ≥65 years (adjusted odds ratio [AOR]: 0.070; 95% CI: 0.016–0.308), divorce (AOR: 0.226; 95% CI: 0.064–0.800), and increased WC (AOR: 0.361; 95% CI: 0.181–0.720) were factors significantly associated with poor glycemic control ().
Table 4 Multivariable logistic regression analysis of factors associated with poor glycemic control among DM patients attending at University of Gondar Hospital, northwest Ethiopia, 2017 (N=367)
Diabetes complications
Diabetes complications were found in 115 (31.33%) of study participants. The prevalence of DM complications was higher in DM patients with >7 years DM duration (39.2%), overweight (38.9%), high-risk WC (39.7%), and TG level ≤150 mg/dL (30.8%) ().
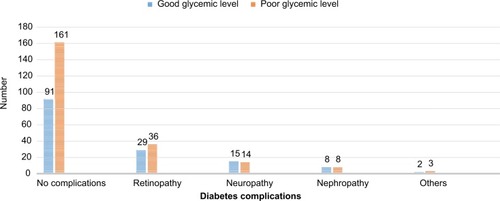
DM complications by their type account as follows: retinopathy (65 [17.7%]), neuropathy (29 [7.9%]), nephropathy (16 [4.4%]), and others (5 [1.4%]). The prevalence of diabetes complications was higher in diabetic patients having poor glycemic control (61/222) than those with good glycemic control ().
Figure 1 Diabetes complications based on glycemic level of diabetic mellitus patients attending at University of Hospital, northwest Ethiopia, 2017.
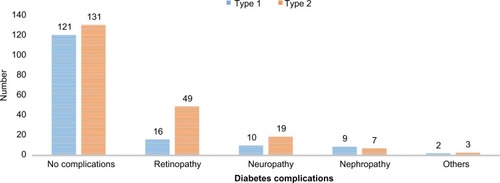
Diabetes complications were higher among T2DM patients (78 [37.32%]) than T1DM study participants (37 [23.42%]) ().
Figure 2 Diabetes complications based on the type of DM among DM patients attending at University of Gondar Hospital, northwest Ethiopia, 2017.
Discussion
The main target in the management of DM is to maintain good glycemic control, which is very important for controlling diabetes and preventing and delaying diabetes complications.Citation16 Glucose measurement is the main tool for assessing glycemic control. In this study, glucose level >152 mg/dL was taken as poor glycemic control level according to ADA Standards of Medical Care in Diabetes 2017.Citation11
In this study, the mean FBS level was 174.25±57.14 mg/dL. Similar study from Jimma, Ethiopia found an average FBS of 163±45 mg/dL.Citation17 The overall prevalence of poor glycemic control was 60.5% (95% CI: 55.6–65.7) in the current study. This finding is similar to the previous studies conducted in Gondar (64.7%), Kenya (60.5%), and Jordan (65.1%).Citation18–Citation20
Prevalence of poor glycemic control (60.5%) is lower compared to the studies conducted in Jimma, Ethiopia (81.7%), Venezuela (76%), and Hawaii (68.5%).Citation17,Citation21,Citation22 This variation would have happened due to the difference in the method of glucose measurement, cutoff points, socioeconomic status, culture, genetics, environmental factors, urbanization, and lifestyle, which predispose individuals to different risk factors of poor glycemic control among the study participants.
The prevalence of poor glycemic control was slightly higher among type 1 DM patients (61.4%) than among type 2 DM patients (59.8%). This is similar to the studies done in Gondar and Venezuela.Citation13,Citation21 This may be related to the fact that type 1 DM patients are commonly treated by insulin or combination therapy in more severe cases that require more aggressive treatment to control their disease, while type 2 DM patients with milder disease are more easily controlled by diet or oral hypoglycemic agents.
The result of our study revealed that age ≥65 years, divorced marital status, and increased WC have significant negative association with poor glycemic control. Possible reason of poorer glycemic control in younger populations compared to elders can be associated with the fact that the young people may not adhere to their treatments as elders.
In the current study, poor glycemic control was predominant among 25- to -year-old study subjects with 63% prevalence (AOR: 0.151; 95% CI: 0.041–0.555), which is consistent with a similar study in Gondar,Citation18 which showed higher prevalence among younger DM patients. Diabetic patients aged ≥65 years are less likely to have poor glycemic control (AOR: 0.070; 95% CI: 0.016–0.308) compared to other age groups similar to another study done here in GondarCitation13 and in USA, which indicated that elderly people had better diabetes control.Citation22 Exposure to stressful conditions associated with puberty may aid to the poor glycemic control through stimulation of the autonomic nervous system to induce hyperglycemia.Citation23 Several studies have demonstrated that insulin sensitivity decreases early in puberty, which returns to normal once somatic growth and sexual maturation are completed.Citation24 However, the result contradicts to a study in Kenya,Citation19 in which patients aged >40 years were at risk for poor glycemic control (COR: 1.08; 95% CI: 0.60–1.95). Variation in age group cut point may be the possible reason for the discrepancy.
Study participants who were single showed higher (64.6%; AOR: 0.966; 95% CI: 0.486–1.924) poor glycemic control compared to other groups. Divorced DM patients were less likely to have poor glycemic control (AOR: 0.226; 95% CI: 0.064–0.800) compared to married DM patients. Poor glycemic control was also higher in unemployed individuals (65.4%; AOR: 1.100; 95% CI: 0.547–2.213) compared to employed DM patients. Unemployed DM patients may not be economically good to buy DM medications. Work type had no significant association according to a study in Kenya.Citation19
In our study, individuals having high-risk WC are less likely to have poor glycemic control (AOR: 0.361; 95% CI: 0.181–0.720) compared to individuals having low-risk WC (≤93.9 cm for males and ≤79.9 cm for females). Most of the low-risk WC participants were type 1 DM patients treated mostly with insulin; therefore, if they have strict adherence to insulin, it may increase body weight and WC.Citation25
Even if it was not significant, ≤7 years diabetes duration was protective for poor glycemic level (AOR: 0.854; 95% CI: 0.528–1.381) compared to ≥7 years diabetes duration. Besides, studies in Venezuela, Jordan, and HawaiiCitation20–Citation22 showed that poor glycemic control was more likely associated with long duration of the disease. The association between poor glycemic control and long diabetes duration may be due to progressive impairment of insulin secretion through time because of β cell failure and the difficulty for the patients to continue monitoring the blood glucose level and adjust with the regimen of treatment, diet, and exercise.Citation26
Diabetic complications were high in diabetic patients having poor glycemic control (61 [53.0%]) than their counterparts (54 [47.0%]). A study in Arbaminch, EthiopiaCitation27 also found higher level of glucose (177±35.45 mg/dL) among DM patients with foot ulcer. Similarly, diabetic retinopathy was predominant among poor glycemic control level DM patients according to a case–control study in Brazil.Citation28 The relationship between the level of glucose and diabetic retinopathy was also showed by a follow-up study in USA, that is, regulating glucose level using intensive treatment resulted in delayed slow progression of diabetic retinopathy.Citation29 Increased level of HbA1c also showed significant association with urinary tract infection in women with type 1 DM.Citation30 The main limitations of our study were the use of FBS instead of HbA1c to determine the glycemic status, unable to measure the role of inflammatory cytokines on DM complications, and the cross-sectional nature of the study, which does not show cause–effect relationship of the independent variables to the outcome variable.
Conclusion
The prevalence of poor glycemic control and DM complications is considerably high among diabetes patients. Poor glycemic control showed significant and negative association with study participants aged ≥65 years old, increased WC, and divorced diabetes patients. DM complications are found to be higher among patients with poor glycemic control and type 2 DM.
Data sharing statement
The data sets used and analyzed during the current study are available from the corresponding author on a reasonable request.
Author contributions
AF designed and implemented the study, collected data, undertook statistical analysis, performed data interpretation, and drafted the manuscript. AF, MA and BB participated in data analysis and data interpretation and reviewed the manuscript. All authors contributed toward data analysis, drafting, and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
Our deepest gratitude goes to all study participants, and nurses working at University of Gondar Hospital Chronic Illness Clinic. We would also like to extend our appreciation to University of Gondar, School of Biomedical and Laboratory Sciences, Department of Clinical Chemistry for their multidimensional support. No funding is received from any funding organization for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- American Diabetes Association Diagnosis and classification of diabetes mellitus Diabetes Care 2014 37 Suppl 1 S81 S90 24357215
- Gizaw M Harries AD Ade S Diabetes mellitus in Addis Ababa, Ethiopia: admissions, complications and outcomes in a large referral hospital Public Health Action 2015 5 1 74 78 26400605
- Ogurtsova K da Rocha Fernandes JD Huang Y IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040 Diabetes Res Clin Pract 2017 128 40 50 28437734
- Forbes JM Cooper ME Mechanisms of diabetic complications Physiol Rev 2013 93 1 137 188 23303908
- Feleke Y Enquselassie F An assessment of the health care system for diabetes in Addis Ababa, Ethiopia Ethiop J Health Dev 2005 19 3 203 210
- Brownlee M The pathobiology of diabetic complications: a unifying mechanism Diabetes 2005 54 6 1615 1625 15919781
- Heilig C Concepcion L Riser B Freytag S Zhu M Cortes P Over-expression of glucose transporters in rat mesangial cells cultured in a normal glucose milieu mimics the diabetic phenotype J Clin Invest 1995 96 4 1802 7560072
- Kaiser N Sasson S Feener EP Toronto Diabetic Neuropathy Expert Group Differential regulation of glucose transport and transporters by glucose in vascular endothelial and smooth muscle cells Diabetes 1993 42 1 80 89 7678404
- Tesfaye S Boulton AJ Dyck PJ Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments Diabetes Care 2010 33 10 2285 2293 20876709
- Diabetes Control and Complications Trial Research Group Nathan DM Genuth S Lachin J The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus N Engl J Med 1993 329 14 977 986 8366922
- American Diabetes Association Standards of medical care in diabetes-2017: summary of revisions Diabetes Care 2017 40 Suppl 1 S4 S5 27979887
- Jacobson AM Braffett BH Cleary PA Gubitosi-Klug RA Larkin ME DCCT/EDIC Research Group The long-term effects of type 1 diabetes treatment and complications on health-related quality of life Diabetes Care 2013 36 10 3131 3138 23835693
- Abebe SM Berhane Y Worku A Alemu S Mesfin N Level of sustained glycemic control and associated factors among patients with diabetes mellitus in Ethiopia: a hospital-based cross-sectional study Diabetes Metab Syndr Obes 2015 8 65 25657591
- Biochemistry Handbook for Mindray BS-200E-Operation-Manual-V4-0-En.pdf. Available from: https://www.scribd.com/document/341537236/BS-200E-Operation-Manual-V4-0-En-pdf Accessed January 10, 2017
- Patry-Parisien J Shields M Bryan S Comparison of waist circumference using the World Health Organization and National Institutes of Health protocols Health Rep 2012 23 3 53 60 23061265
- UK Prospective Diabetes Study Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group Lancet 1998 352 9131 837 853 9742976
- Angamo MT Melese BH Ayen WY Determinants of glycemic control among insulin treated diabetic patients in Southwest Ethiopia: hospital based cross sectional study PLoS One 2013 8 4 e61759 23620789
- Abebe SM Berhane Y Worku A Alemu S Mesfin N Level of sustained glycemic control and associated factors among patients with diabetes mellitus in Ethiopia: a hospital-based cross-sectional study Diabetes Metab Syndr Obes 2015 8 65 71 25657591
- Otieno CF Kariuki M Ng’ang’a L Quality of glycaemic control in ambulatory diabetics at the out-patient clinic of Kenyatta National Hospital, Nairobi East Afr Med J 2003 80 8 406 410 14601781
- Khattab M Khader YS Al-Khawaldeh A Ajlouni K Factors associated with poor glycemic control among patients with type 2 diabetes J Diabetes Complications 2010 24 2 84 89 19282203
- Moreira ED Neves RC Nunes ZO Venezuelan Diabetes Investigators’ Group Glycemic control and its correlates in patients with diabetes in Venezuela: results from a nationwide survey Diabetes Res Clin Pract 2010 87 3 407 414 20060190
- Juarez DT Sentell T Tokumaru S Factors associated with poor glycemic control or wide glycemic variability among diabetes patients in Hawaii, 2006-2009 Prev Chronic Dis 2012 9 120065 23017247
- Moussa MA Alsaeid M Abdella N Refai TM Al-Sheikh N Gomez JE Social and psychological characteristics of Kuwaiti children and adolescents with type 1 diabetes Soc Sci Med 2005 60 8 1835 1844 15686813
- Goran MI Gower BA Longitudinal study on pubertal insulin resistance Diabetes 2001 50 11 2444 2450 11679420
- Castaneda C Janssen I Castaneda C Janssen I Ethnic comparisons of sarcopenia and obesity in diabetes Ethn Dis 2005 15 4 664 670 16259491
- Mohammad HA Farghaly HS Metwalley KA Monazea EM Abd El-Hafeez HA Predictors of glycemic control in children with Type 1 diabetes mellitus in Assiut-Egypt Indian J Endocrinol Metab 2012 16 5 796 23087867
- Deribe B Woldemichael K Nemera G Prevalence and factors influencing diabetic foot ulcer among diabetic patients attending Arbaminch Hospital, South Ethiopia J Diabetes Metab 2014 05 01 1 7
- Lima VC Cavalieri GC Lima MC Nazario NO Lima GC Risk factors for diabetic retinopathy: a case-control study Int J Retina Vitreous 2016 2 1 21 27847639
- Aiello LP DCCT/EDIC Research Group Diabetic retinopathy and other ocular findings in the diabetes control and complications trial/epidemiology of diabetes interventions and complications study Diabetes Care 2014 37 1 17 23 24356593
- Lenherr SM Clemens JQ Braffett BH DCCT/EDIC Research Group Glycemic control and urinary tract infections in women with type 1 diabetes: results from the DCCT/EDIC J Urol 2016 196 4 1129 1135 27131462