
Abstract
Type 1 diabetes (T1D) is associated with an increased fracture risk, which is present at young and old age. Reductions in bone mineral density do not explain the increased fracture risk. Novel scanning modalities suggest that structural deficits may contribute to the increased fracture risk. Furthermore, T1D may due to insulinopenia be a state of low bone turnover. However, diabetes complications and comorbidities may influence fracture risk. Patients with T1D are fearful of falls. The diabetes related complications, hypoglycemic events, and antihypertensive treatment may all lead to falls. Thus, the increased fracture risk in T1D seems to be multifactorial, and earlier intervention with antiosteoporotic medication and focus on fall prevention is needed. This systematic review addresses the epidemiology of fractures and osteoporosis in patients with T1D and the factors that influence fracture risk.
Introduction
Type 1 diabetes (T1D) is a condition with insulinopenia and well-known complications such as retinopathy, neuropathy, and nephropathy. During recent years, T1D has been linked to a new complication: Bone fragility. Osteoporosis is a condition related to an increased fracture risk. Based on estimates from the United States, the prevalence of T1D is 0.5 % and more common in young adults compared to type 2 diabetes (T2D),Citation1 whereas the prevalence of osteoporosis is 10.3% and most common in the elderly.Citation2 Based on prevalences,a small overlap between T1D and osteoporosis would be expected, however, recent research reports high fracture rates in patients with T1D compared to non-diabetes individuals, thus fracture rates may not be explained by classical osteoporosis. This review addresses the epidemiology of fractures and bone fragility in patients with T1D and elucidates the factors that may influence fracture risk.
Methods
A systematic literature search was performed on the 17th of June 2019 using the database Medline at Pubmed. The search terms were “type 1 diabetes and fracture” and “type 1 diabetes and osteoporosis” leading to 624 hits. Furthermore, the reference list of systematic reviews and meta-analysis were examined. In total, 63 studies were included in the systematic review which all investigated bone fragility or mechanisms of bone fragility in patients with type 1 diabetes.
Epidemiology of Fractures in Type 1 Diabetes
Meta-analyses of observational studies have linked T1D to an increased risk of fractures compared with non-diabetes individuals. In the meta-analysis by Vestergaard,Citation3 the risk of a hip fracture was 7 fold increased in T1D compared to individuals without diabetes. This estimate is similar to the findings of Janghorbani et al,Citation4 where a 6 fold increased risk of hip fracture was found. In the meta-analyses, the age of the participants ranged from mean ages of 20 to 60 years. In a more recent cohort study using The Health Improvement Network (THIN) database, Weber et al reported increased risks of any fracture with HRs of 2.03 and 2.18 for women and men with T1D compared to individuals without diabetes, respectively.Citation5 Furthermore, in this studyCitation6 the risk of hip fracture was increased in women at all ages and in men from age 30 and older. Shah et al evaluated 14 observational studies in a meta-analysis and reported that the risk of any fracture is 3 fold increased in patients with T1D compared to individuals without diabetes, but only 1.8 fold increased in men and 4.1 fold increased in women.Citation7 A more recent meta-analysis restricted the analysis to relatively young patients with T1D aged 18–50 years and reported a 1.9 fold increased risk of any fracture and a 4.4 fold increased risk of hip fracture in patients with T1D compared to individuals without diabetes.Citation8 Results from the previously mentioned meta-analyses are supported by more recent cohort studies: Hamilton et al reported a 7.11 increased hip fracture risk for patients with T1D compared with individuals without diabetes, but a 5 fold increased fracture risk when comparing patients with T1D with patients with T2D.Citation9 Notably, the study is limited by a low number of included patients with T1D (n=121), however, the study has a relatively long follow up of 14.5 years.Citation9 A cohort study using the Danish National Patient Registry provided more modest fracture risk estimates, with a 2.4 fold increased hip fracture risk and 2 fold increased upper extremity fracture risk.Citation10 Also, a cohort study using the Scottish national registries reported a 3.5 fold and a 3.3 fold increased risk of hip fracture in women and men with T1D compared to the general population, respectively.Citation11
Less is known about vertebral fractures in patients with T1D, however a study evaluated 82 patients with T1D and 82 controls by vertebral fracture assessment (VFA) with subsequent confirmation by x-ray, and reported a prevalence of vertebral fractures of 24% and 6%, respectively.Citation12 Another study by Jensen et al reported a 2.2 fold increased risk of spinal fractures in T1D compared with patients without diabetes, however this study is based solely on registry data where subclinical vertebral fractures are susceptible to non-registration.Citation10 Based on the evidence available, patients with T1D have an increased risk of fracture during their entire life. The relative risk seems to be constant throughout life, although in absolute numbers most fractures occur at older age where the total fracture burden in the general population is greatest.
Bone Mineral Density in Type 1 Diabetes
One explanation of the increased bone fragility in patients with T1D is a decreased BMD and thereby classical osteoporosis. The meta-analysis by Vestergaard reported decreased BMD at the lumbar spine (ls) and hip in patients with T1D compared to individuals without diabetes, corresponding to Z-scores of −0.22 and −0.38, respectively.Citation3 A more recent meta-analysis by Shah et al including 16 studies reported no differences in BMD at the ls in patients with T1D compared to individuals without diabetes.Citation13 In this meta-analysis, however, the femoral neck (fn) BMD was decreased by 0.055 g/cm2, which corresponds to a Z-score of −0.55 assuming the standard deviation is 0.1. The decreased BMD is apparent in both male and female patients with T1D.Citation14 Patients with T1D have lower BMD compared with patients with T2D,Citation15 hence, the reduced BMD is a unique feature of T1D and is not due to any shared risk factors with T2D. Furthermore, BMD seems to be relatively stable in T1D irrespective of disease progression: A recent study reported reduced levels of fn BMD in patients with T1D duration of more than 50 years, whereas ls BMD was increased.Citation16 Likewise, Hamilton et al followed 48 patients with T1D for 10 years and found that BMD at the spine, fn, and forearm remained stable when adjusted for body mass index (BMI).Citation17 Hence, changes may occur early in T1D as children with T1D have decreased fn BMD with a Z-score of −0.57, similar to previously described meta-analysis.Citation13,Citation18,Citation19 In addition, children with T1D and glycated hemoglobin A1c (HbA1c) ≥7.5% have lower bone mass accrual during twelve monthsCitation18 and adolescents with T1D and HbA1c ≥8.0% have lower total body BMD compared to those with better glycemic control.Citation20 The early onset of low BMD in T1D may be due to calcium loss, as 25% of young women with T1D had greater urinary calcium excretion and less calcium retention in a study that used a dual stable calcium isotope to evaluate calcium intake and excretion.Citation21 Furthermore, insulinopenia in T1D may impact bone accrual (see the section Bone turnover in Type 1 diabetes for details). Thus, BMD changes seem to occur early in life in T1D.
However, the reduced BMD does not fully explain the increased risk of fracture in patients with T1D.Citation3 In T1D, the association between low BMD and fracture incidence has not been investigated, thus it is uncertain to which extent the small reduction in BMD influence fracture risk. Furthermore, the fracture risk assessment (FRAX) tool, which uses BMD among other risk factors to determine a 10-year fracture risk, has not been validated in cohorts of patients with T1D. However, a review by Hough et al provided insights of similar expected fracture rates in patients with and without T1D when applying the FRAX tool.Citation22 Thus, current fracture predictors underestimate the burden of fractures for patients with T1D, as illustrated by . Development of fracture prediction strategies is needed in T1D.
Bone Turnover in Type 1 Diabetes
Another mechanism underlying bone fragility may be an altered bone turnover. Diabetes is characterized by a state of low bone turnover.Citation23,Citation24 This characterization is mainly based on measurements of bone turnover markers in plasma or serum. In a meta-analysis, we found that levels of the bone resorption marker C-terminal cross-link of collagen (CTX) and the bone formation marker osteocalcin were decreased in T1D compared to individuals without diabetes.Citation23 Interestingly, levels of tartrate resistant acid phosphatase (TRAP) and of procollagen type 1 amino terminal propeptide (P1NP) were similar in patients with T1D compared with non-diabetes individuals but lower in patients with T2D compared to individuals without diabetes. However this may be due to a relatively low number of included studies that report on T1D (n=3 for TRAP and n=2 for P1NP).Citation23 Further, Vitamin D levels were reduced in patients with T1D compared with non-diabetes individuals.Citation24 A meta-analysis on levels of circulating bone turnover markers in children and adolescents with T1D also reported decreased levels of osteocalcin compared to individuals without diabetes whereas data were inconclusive for CTX and P1NP,Citation25 although, levels of P1NP tended towards being lower and levels of CTX towards being higher in T1D compared to individuals without diabetes.Citation25 A more recent study reported lower levels of bone specific alkaline phosphatase and CTX in children with T1D compared to healthy children.Citation26 In the 10-year follow up study by Hamilton et al, reported that men with T1D had lower levels of P1NP and osteocalcin after 10 years compared with baseline,Citation17 however this drop in bone formation markers is more likely to be an age-related phenomenon than due effects of T1D.Citation27 In a study of the diurnal variations in bone turnover markers, levels of P1NP and osteocalcin were significantly lower in patients with T2D compared to individuals without diabetes, whereas results were non-significant for T1D.Citation28 Similarly, in a cross-sectional study comparing patients with T1D and T2D, levels of P1NP and osteocalcin were lower in T2D compared with T1D.Citation29 However, in the diurnal study, the bone formation markers tended to being lower in T1D compared with individuals without diabetes, and the lack of significance for the results may be due to low study power (participant n=5 in each group).Citation28
Levels of CTX, osteocalcin, and P1NP are stable during addition of glucose to blood samples,Citation24 thus, analytical factors do not explain the measured low levels of bone turnover markers. In our meta-analysis, the levels of circulating sclerostin were increased in patients with T1D compared with non-diabetes controls, and this may explain the lower bone turnover. Further, the levels of circulating osteoprotegerin and Receptor activator of nuclear factor kappa-B ligand (RANKL) were similar in T1D and individuals without diabetes.Citation23 A low bone turnover should optimally be confirmed by bone tissue biopsies. However, available data from bone tissue biopsies is sparse for patients with T1D. Based on the largest published study, T1D is a state of normal bone turnover. However the interpretation of the study is limited by very few biopsies (n=18), and that the participants had a well-controlled glycemic status.Citation30 Only one other bone biopsy study with T1D patients is available, however it reports diabetes patients as a whole with few patients with T1D compared to T2D (one out of six).Citation31 Thus, based on current evidence mainly based on cross-sectional studies where studies using bone turnover markers are more abundant; T1D is a state of low bone turnover.
A possible mechanism of low bone turnover may be hyperglycemia.Citation29 However, neither fluctuations in glucose during 24 hoursCitation28 nor clamps with hypoglycemia and hyperglycemiaCitation32 alter the levels of CTX or P1NP in patients with T1D. During a meal or an oral glucose tolerance test, levels of bone turnover markers decrease in healthy individuals and in patients with T2D.Citation33,Citation34 The influence of meals on bone turnover was similar between T1D, T2D and controls based on the diurnal study.Citation28 Insulin does not alter the levels of CTX or P1NP in T1D,Citation32 which has been confirmed by Basu et al.Citation35 However, insulinopenia in T1D may contribute to a low bone formation as insulin is a bone anabolic agent,Citation36 and bone turnover was decreased in a mouse model of insulinopenia but restored by insulin treatment.Citation37 Another mouse model of insulinopenia reported decreased levels of osteocalcin and RUNX2 with concomitant low insulin levels.Citation38 The low bone turnover caused by insulin deficiency possibly occurs over time and may not be detected in studies with acute changes in insulin levels as described above.Citation32,Citation35
As meals influence bone turnover, gastro-intestinal hormones may influence bone turnover in patients with T1D. A GIP infusion decreased the levels of CTX but not P1NP in patients with T1D.Citation32 The evidence of the incretin response in T1D is conflicting, but both GLP-1 and −2 have been suggested to impact bone turnover.Citation39 The diurnal study showed lower levels of GLP-2 in patients with T1D compared with T2D, and levels of GIP also tended to being lower in patients with T1DCitation28 compared with T2D. In T1D, both bone formation and bone resorption seems to be reduced but GLP-2 is mainly related to a decreased bone resorption and GLP-2 does not seem to impact bone formation.Citation40 Although insulinopenia and gastrointestinal hormones may influence bone turnover in T1D, the etiology of a reduced bone turnover remains unknown.
Bone Structure in Type 1 Diabetes
Microarchitectural changes may also impact the bone fragility in patients with T1D and recently more sophisticated scanning techniques have been developed. High Resolution peripheral Quantitative Computed Tomography (HRpQCT) is a technique that allows for in vivo measurement of bone microarchitecture in the tibia and radius. Few studies have evaluated this technique in T1D. A study by Shanbhogue et al compared 55 patients with T1D with 55 individuals without diabetes and found decreased trabecular thickness, increased trabecular separation, and decreased trabecular bone volume at the tibia and decreased trabecular thickness, and decreased trabecular bone volume, trabecular thickness and cortical thickness at the radius in patients with T1D and microvascular complications compared to individuals without diabetes. However, the findings were not present in patients with T1D without microvascular complications.Citation41 A study by our group compared 52 patients with T1D with 67 patients with T2DCitation15 and found similar characteristics of the trabecular compartment in patients with T1D and T2D when using HRpQCT. However, tissue stiffness at the tibia was lower in T1D compared with T2D. Notably, in contrast to the study by Shanbhogue et al, no association was present between microvascular complications and bone microarchitecture.Citation15 A study applying magnetic resonance imaging (MRI) showed increased trabecular separation and decreased trabecular number and trabecular bone volume at the tibia in 30 patients with T1D compared to 28 healthy individuals. The reduction in trabecular bone volume was most pronounced in individuals with retinopathy.Citation42 Taken together, these studies suggest alterations of the trabecular compartment. This is consistent with another study evaluating trabecular bone score (TBS) in T1D that reported lower TBS in patients with T1D compared to individuals without.Citation43 Another study reported borderline significantly (p=0.075) decreased TBS in patients with T1D compared to controls, but patients with T1D with prevalent fractures had lower TBS compared to patients with T1D without fracture.Citation44 Finally, a single study reported low cortical BMD measured by quantitative CT (QCT) at the ls in children and adolescents with T1D compared to healthy age-matched individuals.Citation45 These studies with advanced techniques are suggestive of structural changes beside what is explained by BMD in patients with T1D. However, only few studies with relatively small sample sizes are available. Whether structural changes depend on microvascular complications in T1D is unknown. The hip primarily consists of cortical bone and is most prone to fracture in T1D therefore it is notable that the structural deficits primarily are from the trabecular compartment. HRpQCT, QCT, MRI, and TBS are all novel technologies but with limited evidence both in the general population and especially in type 1 diabetes. Further research is warranted to evaluate whether the structural changes that can be detected by these techniques may explain the increased fracture risk in patients with T1D.
Impact of Hyperglycemia and AGEs on Bone Strength and Fracture Risk
Hyperglycemia may contribute to the bone fragility in T1D. Long-term hyperglycemia and oxidative stress may negatively impact bone strength by the production of advanced glycation endproducts (AGEs). It has been hypothesized that non-enzymatic cross-links are built into the collagen structure of the bone, thereby creating immature bone that is more fragile than normal bone.Citation46 Furthermore, the accumulation of AGEs seems to decrease bone formation in a rat model.Citation47 In a T1D mice model, microspectroscopy showed that AGEs accumulate in the bone and that bone strength is decreased.Citation48 In bone tissue biopsies from five patients with T1D and fracture, five patients with T1D and no fracture, and five healthy individuals, the levels of the AGE, pentosidine, were increased in patients with T1D and fracture compared to the other two groups.Citation49 Furthermore, patients with T1D and fracture had increased mineralization.Citation49 Thus in T1D, accumulations of AGEs may promote fractures, whereas the evidence for hyperglycemia as a fracture predictor is weaker. High levels of circulating pentosidine and HbA1c are associated with prevalent fractures,Citation50 where each percentage increase in HbA1c increases the OR for any fracture by 1.9. High levels of HbA1c is also associated with fragility fractures with an OR of 4.19 (for each percentage increase) and associated with multiple fractures in patients with T1D.Citation16,Citation51 A cohort study by Thayakaran et al reported an increased fracture risk with increasing HbA1c, although with a more modest risk increase of 1.01 per mmol/mol increase.Citation52 Although it is tempting to conclude that hyperglycemia may explain the increased fracture risk, other studies report no association between HbA1c and fracture,Citation53,Citation54 and the available data for patients with T1D is limited. The hypothesis of bone fragility due to hyperglycemia and development of AGEs is based on limited evidence and needs to be confirmed in both mechanistic studies and cohort studies.
Influence of Complications and Comorbidities on Fracture Risk
Diabetes-related complications may influence fracture risk, as neuropathy may lead to falls,Citation55,Citation56 retinopathy to decreased vision and falls,Citation57,Citation58 and nephropathy to renal osteodystrophy.Citation59 In T1D, the association is uncertain between diabetes-related complications and fracture risk. Some studies report increased fracture risk in patients with neuropathy,Citation51 retinopathy,Citation51 and nephropathy,Citation60 whereas others report no increased risk in patients with neuropathy,Citation9,Citation52,Citation53,Citation60 retinopathyCitation9,Citation52,Citation53,Citation60 and nephropathy.Citation9 One study reported increased fracture risk in patients with T1D and no complications.Citation60 Although the association between diabetes complications and fracture risk remains controversial, a study reported that 41% of patients with T1D are fearful of falls, and that the main contributors to falls are neuropathy and hypoglycemia.Citation61 A severe limitation to the studies assessing diabetes complications, falls, and fracture risk is that the data is mainly collected through registries and questionnaires, and therefore patients may be misclassified by both diabetes diagnosis (e.g. type 2 instead of type 1), falls (underestimation of actual number of falls), and fracture (date and site of fracture) in these studies.
Besides diabetes-related complications, T1D is linked to several other diseases. As a disease with an autoimmune component, other autoimmune diseases are more common in patients with T1D. T1D is associated with thyroid disease and celiac disease.Citation62 Both hypothyroidism and hyperthyroidism are associated with an increased fracture riskCitation63 and celiac disease is associated with an increased fracture risk in patients with T1D.Citation54 A study by Dhaliwal et al reported data on 756 patients with T1D and found a borderline significant association between fractures and celiac disease (p=0.06).Citation53 T1D is also linked to other autoimmune conditions such as rheumatoid arthritis, which is also associated with an increased fracture risk.Citation64,Citation65 Pancreatitis may cause endocrine dysfunction of the pancreas, potentially resulting in diabetes.Citation66 This pancreas insufficiency-related diabetes, type 3c diabetes, is insulin-dependent and may be misclassified as T1D.Citation67 Pancreatitis and fractures share alcohol abuse as a risk factor,Citation66 and pancreatitis is strongly linked to fracture risk (3.5 fold increased risk of a hip fracture).Citation68 The increased risk of fracture in patients with T1D may thus be partly explained by misclassification, comorbidities, and complications. However, current evidence neither confirm nor reject that comorbidities and complications in T1D may contribute to the observed fracture risk. Further large-scale cohort studies should investigate the influence of these conditions on fracture risk.
Impact of Medications on Fracture Risk
The medications used to treat T1D may influence fracture risk. Treatment of patients with T1D is based mainly on insulin, and a recent registry-based study found no effect of insulin dose on fracture risk in patients with T1D.Citation10 However, in that study, hypoglycemic events increased fracture risk by 1.58 fold.Citation10 Other studies have reported increased risk of fractures due to hypoglycemic events,Citation69,Citation70 whereas other studies found no association.Citation9,Citation52,Citation53 Although evidence on hypoglycemia and fracture is conflicting, hypoglycemia is associated with fallsCitation61 and hypoglycemia may be widely underdiagnosed in studies that mainly use registries and questionnaires. Thus, the true prevalence of fractures due to hypoglycemia is susceptible to be larger than what is presented in the literature.
Patients with T1D are frequent users of antihypertensives and lipid lowering drugs (e.g. statins).
Antihypertensives may induce orthostatic hypotension and thereby falls, which could increase fracture risk. Diuretics may also increase the loss of minerals (e.g. calcium and magnesium) by urinary excretion. In patients with diabetes, loop diuretics but not thiazides are associated with an increased risk of fracture.Citation71 A post-hoc prospective evaluation of the randomized controlled trial (RCT) “Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial” showed a decreased fracture rate in individuals treated with thiazide diuretics compared to angiotensin converting enzyme inhibitors (ACEi).Citation72 In meta-analyses of observational studies, loop diuretics and ACEi are associated with an increased fracture risk compared to non-users.Citation73,Citation74 Although these studies are not restricted to patients with diabetes; antihypertensives are linked to fractures and may especially induce fracture in patients with low BMD as in T1D. Although antihypertensives may have adverse effects on bone health, they should not be disregarded due to the large benefit in the prevention of cardiovascular disease in patients with T1D. The current evidence can neither reject nor confirm that drugs used for the treatment of T1D influence the observed fracture risk.
Perspectives
T1D is related to an increased risk of fracture, especially hip fracture. Vertebral fractures seem more common in T1D although the evidence is sparse. This is a societal health issue as vertebral fractures and hip fractures are associated with an increased mortality risk caused mainly by cardiovascular disease.Citation75,Citation76 BMD deficits are observed in T1D, however these do not fully explain the increased fracture risk in T1D. The International Osteoporosis Foundation has suggested a threshold for osteoporosis treatment at T-score <-2.0 for patients with diabetes aged 50 or with risk factors for fracture, whereas it is −2.5 for other individuals,Citation77 however there is no specific evidence that support early intervention with BMD improvement and prevention of osteoporosis and this recommendation is based on the observed fracture rates and BMD deficits. Based on current knowledge, antiosteoporotic drugs are as efficient in patients with T1D as in individuals without diabetes, although evidence is sparse and mainly from observational studies and post-hoc analyses of RCTs.Citation78 Vitamin D supplementation may be beneficial in T1D due to lower levels of vitamin D compared with individuals without diabetes. However, a systematic review reported that there is insufficient data on the effect of vitamin D intake, calcium intake, and physical activity on bone health in T1D.Citation79 Thus, vitamin D and calcium supplementation in T1D should follow national guidelines. Many patients with T1D are fearful of falls, and treatment with antihypertensives, hypoglycemia, and diabetes complications may lead to falls. displays efforts to detect increased fracture risk and prevent fractures in patients with T1D. Hypoglycemic events may be reduced by continuous glucose monitoring which is highlighted by the closed loop insulin delivery system that reduces hypoglycemic events compared to sensor-augmented pump.Citation80,Citation81 Although current evidence is conflicting, a fall prevention strategy may reduce fracture rates in T1D and implementation of such efforts should be at large scale to detect potential benefits.
Figure 1 Risk of fracture in patients with type 1 diabetes. The depicted fracture risks are based on epidemiological evidence and the expected fracture risk by BMD and FRAX (see text for details and references).
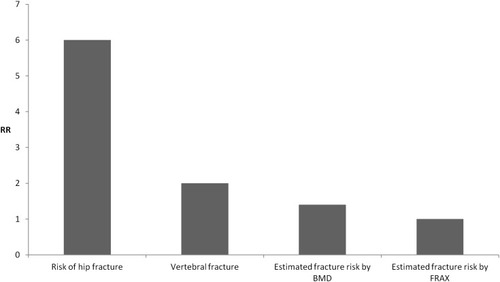
Table 1 Measures to Detect Increased Fracture Risk and Intervention to Prevent Fracture in Patients with T1D
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work. All authors have approved the final version of the manuscript.
Funding
The authors received no funding for the presented work.
Disclosure
JSL reports personal fees from Gilead Sciences Denmark outside the submitted work. BL has received research grants to institution from Amgen and Novo Nordisk and serves on the advisory boards and/or performs lectures for Amgen, UCB, and Eli Lilly. The authors report no other conflicts of interest in this work.
References
- Xu G , Liu B , Sun Y , et al. Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: population based study. BMJ . 2018;362:k1497. doi:10.1136/bmj.k1497 30181166
- Wright NC , Looker AC , Saag KG , et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Miner Res . 2014;29(11):2520–2526. doi:10.1002/jbmr.2269 24771492
- Vestergaard P . Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes–a meta-analysis. Osteoporos Int . 2007;18(4):427–444. doi:10.1007/s00198-006-0253-4 17068657
- Janghorbani M , Van Dam RM , Willett WC , Hu FB . Systematic review of type 1 and type 2 diabetes mellitus and risk of fracture. Am J Epidemiol . 2007;166(5):495–505. doi:10.1093/aje/kwm106 17575306
- Weber DR , Haynes K , Leonard MB , Willi SM , Denburg MR . Type 1 diabetes is associated with an increased risk of fracture across the life span: a population-based cohort study using The Health Improvement Network (THIN). Diabetes Care . 2015;38:1913–1920. doi:10.2337/dc15-0783 26216874
- Khosla S , Riggs BL . Pathophysiology of age-related bone loss and osteoporosis. Endocrinol Metab Clin North Am . 2005;34(4):1015–30, xi. doi:10.1016/j.ecl.2005.07.009 16310636
- Shah VN , Shah CS , Snell-Bergeon JK . Type 1 diabetes and risk of fracture: meta-analysis and review of the literature. Diabet Med . 2015;32(9):1134–1142. doi:10.1111/dme.12734 26096918
- Thong EP , Herath M , Weber DR , et al. Fracture risk in young and middle-aged adults with type 1 diabetes mellitus: a systematic review and meta-analysis. Clin Endocrinol (Oxf) . 2018;89(3):314–323. doi:10.1111/cen.13761 29876960
- Hamilton EJ , Davis WA , Bruce DG , Davis TME . Risk and associates of incident hip fracture in type 1 diabetes: The Fremantle Diabetes Study. Diabetes Res Clin Pract . 2017;134:153–160. doi:10.1016/j.diabres.2017.10.011 29054483
- Jensen MH , Vestergaard P . Hypoglycaemia and type 1 diabetes are associated with an increased risk of fractures. Osteoporos Int . 2019;30:1663–1670. doi:10.1007/s00198-019-05014-6 31129687
- Hothersall EJ , Livingstone SJ , Looker HC , et al. Contemporary risk of hip fracture in type 1 and type 2 diabetes: a national registry study from Scotland. J Bone Miner Res . 2014;29(5):1054–1060. doi:10.1002/jbmr.2118 24155126
- Zhukouskaya VV , Eller-Vainicher C , Vadzianava VV , et al. Prevalence of morphometric vertebral fractures in patients with type 1 diabetes. Diabetes Care . 2013;36(6):1635–1640. doi:10.2337/dc12-1355 23340886
- Shah VN , Harrall KK , Shah CS , et al. Bone mineral density at femoral neck and lumbar spine in adults with type 1 diabetes: a meta-analysis and review of the literature. Osteoporos Int . 2017;28(9):2601–2610. doi:10.1007/s00198-017-4097-x 28580510
- Pan H , Wu N , Yang T , He W . Association between bone mineral density and type 1 diabetes mellitus: a meta-analysis of cross-sectional studies. Diabetes Metab Res Rev . 2014;30(7):531–542. doi:10.1002/dmrr.2508 24376190
- Starup-Linde J , Lykkeboe S , Gregersen S , et al. Bone structure and predictors of fracture in type 1 and type 2 diabetes. J Clin Endocrinol Metab . 2016;101(3):928–936. doi:10.1210/jc.2015-3882 26756117
- Alhuzaim ON , Lewis EJH , Lovblom LE , et al. Bone mineral density in patients with longstanding type 1 diabetes: results from the Canadian Study of Longevity in Type 1 Diabetes. J Diabetes Complications . 2018;33(11):107324.31003922
- Hamilton EJ , Drinkwater JJ , Chubb SAP , et al. A 10-year prospective study of bone mineral density and bone turnover in males and females with type 1 diabetes. J Clin Endocrinol Metab . 2018;103(9):3531–3539. doi:10.1210/jc.2018-00850 30032248
- Weber DR , Gordon RJ , Kelley JC , et al. Poor glycemic control is associated with impaired bone accrual in the year following a diagnosis of type 1 diabetes. J Clin Endocrinol Metab . 2019;104:4511–4520. doi:10.1210/jc.2019-00035 31034056
- Gunczler P , Lanes R , Paz-Martinez V , et al. Decreased lumbar spine bone mass and low bone turnover in children and adolescents with insulin dependent diabetes mellitus followed longitudinally. J Pediatr Endocrinol Metab . 1998;11(3):413–419. doi:10.1515/JPEM.1998.11.3.413 11517957
- Wierzbicka E , Swiercz A , Pludowski P , Jaworski M , Szalecki M . Skeletal status, body composition, and glycaemic control in adolescents with type 1 diabetes mellitus. J Diabetes Res . 2018;2018:8121634. doi:10.1155/2018/8121634 30250851
- Weber DR , O’Brien KO , Schwartz GJ . Evidence of disordered calcium metabolism in adolescent girls with type 1 diabetes: an observational study using a dual-stable calcium isotope technique. Bone . 2017;105:184–190. doi:10.1016/j.bone.2017.09.001 28882565
- Hough FS , Pierroz DD , Cooper C , Ferrari SL , IOF CSA Bone and Diabetes Working Group. MECHANISMS IN ENDOCRINOLOGY: mechanisms and evaluation of bone fragility in type 1 diabetes mellitus. Eur J Endocrinol . 2016;174(4):R127–R138. doi:10.1530/EJE-15-0820 26537861
- Hygum K , Starup-Linde J , Harslof T , Vestergaard P , Langdahl BL . MECHANISMS IN ENDOCRINOLOGY: diabetes mellitus, a state of low bone turnover - a systematic review and meta-analysis. Eur J Endocrinol . 2017;176(3):R137–R157. doi:10.1530/EJE-16-0652 28049653
- Starup-Linde J , Eriksen SA , Lykkeboe S , Handberg A , Vestergaard P . Biochemical markers of bone turnover in diabetes patients–a meta-analysis, and a methodological study on the effects of glucose on bone markers. Osteoporos Int . 2014;25(6):1697–1708. doi:10.1007/s00198-014-2676-7 24676844
- Madsen JOB , Jorgensen NR , Pociot F , Johannesen J . Bone turnover markers in children and adolescents with type 1 diabetes-A systematic review. Pediatr Diabetes . 2019. doi:10.1111/pedi.12853
- Chen SC , Shepherd S , McMillan M , et al. Skeletal fragility & its clinical determinants in children with type 1 diabetes. J Clin Endocrinol Metab . 2019;104:3585–3594. doi:10.1210/jc.2019-00084 30848792
- Almeida M . Aging mechanisms in bone. Bonekey Rep . 2012;(1). doi:10.1038/bonekey.2012.102
- Hygum K , Starup-Linde JK , Harslof T , et al. The diurnal variation of bone formation is attenuated in adult patients with type 2 diabetes. Eur J Endocrinol . 2019;181:221–231. doi:10.1530/EJE-19-0309
- Starup-Linde J , Lykkeboe S , Gregersen S , et al. Differences in biochemical bone markers by diabetes type and the impact of glucose. Bone . 2015;83:149–155. doi:10.1016/j.bone.2015.11.004 26555635
- Armas LA , Akhter MP , Drincic A , Recker RR . Trabecular bone histomorphometry in humans with type 1 diabetes mellitus. Bone . 2012;50(1):91–96. doi:10.1016/j.bone.2011.09.055 22001578
- Krakauer JC , McKenna MJ , Buderer NF , Rao DS , Whitehouse FW , Parfitt AM . Bone loss and bone turnover in diabetes. Diabetes . 1995;44(7):775–782. doi:10.2337/diab.44.7.775 7789645
- Christensen MB , Lund A , Calanna S , et al. Glucose-Dependent Insulinotropic Polypeptide (GIP) inhibits bone resorption independently of insulin and glycemia. J Clin Endocrinol Metab . 2018;103(1):288–294. doi:10.1210/jc.2017-01949 29099978
- Clowes JA , Allen HC , Prentis DM , Eastell R , Blumsohn A . Octreotide abolishes the acute decrease in bone turnover in response to oral glucose. J Clin Endocrinol Metab . 2003;88(10):4867–4873. doi:10.1210/jc.2002-021447 14557467
- Lopes LSG , Schwartz RP , Ferraz-De-Souza B , Da SM , Corrêa PHS , Nery M . The role of enteric hormone GLP-2 in the response of bone markers to a mixed meal in postmenopausal women with type 2 diabetes mellitus. Diabetol Metab Syndr . 2015;7:1. doi:10.1186/s13098-015-0006-7 25810781
- Basu R , Peterson J , Rizza R , Khosla S . Effects of physiological variations in circulating insulin levels on bone turnover in humans. J Clin Endocrinol Metab . 2011;96(5):1450–1455. doi:10.1210/jc.2010-2877 21325461
- McCarty MF . Anabolic effects of insulin on bone suggest a role for chromium picolinate in preservation of bone density. Med Hypotheses . 1995;45(3):241–246. doi:10.1016/0306-9877(95)90112-4 8569546
- Thrailkill KM , Liu L , Wahl EC , et al. Bone formation is impaired in a model of type 1 diabetes. Diabetes . 2005;54(10):2875–2881. doi:10.2337/diabetes.54.10.2875 16186388
- Carvalho FR , Calado SM , Silva GA , et al. Altered bone microarchitecture in a type 1 diabetes mouse model Ins2(Akita). J Cell Physiol . 2019;234(6):9338–9350. doi:10.1002/jcp.27617 30317631
- Hygum K , Starup-Linde J , Langdahl BL . Diabetes and bone. Osteoporos Sarcopenia . 2019;5:29–37. doi:10.1016/j.afos.2019.05.001 31346556
- Henriksen DB , Alexandersen P , Hartmann B , et al. Four-month treatment with GLP-2 significantly increases hip BMD: a randomized, placebo-controlled, dose-ranging study in postmenopausal women with low BMD. Bone . 2009;45(5):833–842. doi:10.1016/j.bone.2009.07.008 19631303
- Shanbhogue VV , Hansen S , Frost M , et al. Bone geometry, volumetric density, microarchitecture, and estimated bone strength assessed by HR-pQCT in adult patients with type 1 diabetes mellitus. J Bone Miner Res . 2015;30(12):2188–2199.26096924
- Abdalrahaman N , McComb C , Foster JE , et al. Deficits in trabecular bone microarchitecture in young women with type 1 diabetes mellitus. J Bone Miner Res . 2015;30(8):1386–1393. doi:10.1002/jbmr.2465 25627460
- Shah VN , Sippl R , Joshee P , et al. Trabecular bone quality is lower in adults with type 1 diabetes and is negatively associated with insulin resistance. Osteoporos Int . 2018;29(3):733–739. doi:10.1007/s00198-017-4353-0 29290026
- Neumann T , Lodes S , Kastner B , et al. Trabecular bone score in type 1 diabetes–a cross-sectional study. Osteoporos Int . 2016;27(1):127–133. doi:10.1007/s00198-015-3222-y 26187124
- Roe TF , Mora S , Costin G , Kaufman F , Carlson ME , Gilsanz V . Vertebral bone density in insulin-dependent diabetic children. Metabolism . 1991;40(9):967–971. doi:10.1016/0026-0495(91)90074-7 1895962
- Saito M , Marumo K . Bone quality in diabetes. Front Endocrinol (Lausanne) . 2013;4:72. doi:10.3389/fendo.2013.00072 23785354
- Yang X , Mostafa AJ , Appleford M , Sun LW , Wang X . Bone formation is affected by matrix Advanced Glycation End Products (AGEs) in vivo. Calcif Tissue Int . 2016;99:373–383. doi:10.1007/s00223-016-0153-3 27240574
- Rubin MR , Paschalis EP , Poundarik A , et al. Advanced glycation endproducts and bone material properties in type 1 diabetic mice. PLoS One . 2016;11(5):e0154700. doi:10.1371/journal.pone.0154700 27140650
- Farlay D , Armas LA , Gineyts E , Akhter MP , Recker RR , Boivin G . Nonenzymatic glycation and degree of mineralization are higher in bone from fractured patients with type 1 diabetes mellitus. J Bone Miner Res . 2016;31(1):190–195. doi:10.1002/jbmr.2607 26234180
- Neumann T , Lodes S , Kästner B , et al. High serum pentosidine but not esRAGE is associated with prevalent fractures in type 1 diabetes independent of bone mineral density and glycaemic control. Osteoporosis Int . 2014;25(5):1527–1533. doi:10.1007/s00198-014-2631-7
- Leanza G , Maddaloni E , Pitocco D , et al. Risk factors for fragility fractures in type 1 diabetes. Bone . 2019;125:194–199. doi:10.1016/j.bone.2019.04.017 31059862
- Thayakaran R , Perrins M , Gokhale KM , et al. Impact of glycaemic control on fracture risk in 5368 people with newly diagnosed Type 1 diabetes: a time-dependent analysis. Diabet Med . 2019;36:1013–1019. doi:10.1111/dme.13945 30848519
- Dhaliwal R , Foster NC , Boyle C , et al. Determinants of fracture in adults with type 1 diabetes in the USA: results from the T1D exchange clinic registry. J Diabetes Complications . 2018;32(11):1006–1011. doi:10.1016/j.jdiacomp.2018.08.016 30220582
- Thong EP , Wong P , Dev A , Ebeling PR , Teede HJ , Milat F . Increased prevalence of fracture and hypoglycaemia in young adults with concomitant type 1 diabetes mellitus and coeliac disease. Clin Endocrinol (Oxf) . 2018;88(1):37–43. doi:10.1111/cen.13488 28960394
- Richardson JK , Hurvitz EA . Peripheral neuropathy: a true risk factor for falls. J Gerontol a Biol Sci Med Sci . 1995;50(4):M211–M215. doi:10.1093/gerona/50a.4.m211 7614243
- Timar B , Timar R , Gaita L , Oancea C , Levai C , Lungeanu D . The impact of diabetic neuropathy on balance and on the risk of falls in patients with type 2 diabetes mellitus: a cross-sectional study. PLoS One . 2016;11(4):e0154654. doi:10.1371/journal.pone.0154654 27119372
- Bamashmus MA , Gunaid AA , Khandekar RB . Diabetic retinopathy, visual impairment and ocular status among patients with diabetes mellitus in Yemen: a hospital-based study. Indian J Ophthalmol . 2009;57(4):293–298. doi:10.4103/0301-4738.53055 19574698
- Gupta P , Aravindhan A , Gand ATL , et al. Association between the severity of diabetic retinopathy and falls in an asian population with diabetes: the singapore epidemiology of eye diseases study. JAMA Ophthalmol . 2017;135(12):1410–1416. doi:10.1001/jamaophthalmol.2017.4983 29145583
- Moe SM . Renal osteodystrophy or kidney-induced osteoporosis? Curr Osteoporos Rep . 2017;15(3):194–197. doi:10.1007/s11914-017-0364-1 28497212
- Vestergaard P , Rejnmark L , Mosekilde L . Diabetes and its complications and their relationship with risk of fractures in type 1 and 2 diabetes. Calcif Tissue Int . 2009;84(1):45–55. doi:10.1007/s00223-008-9195-5 19067021
- Shah VN , Wu M , Foster N , Dhaliwal R , Al Mukaddam M . Severe hypoglycemia is associated with high risk for falls in adults with type 1 diabetes. Arch Osteoporos . 2018;13(1). doi:10.1007/s11657-018-0475-z
- Witek PR , Witek J , Pankowska E . Type 1 diabetes-associated autoimmune diseases: screening, diagnostic principles and management. Med Wieku Rozwoj . 2012;16(1):23–34.22516771
- Vestergaard P , Mosekilde L . Fractures in patients with hyperthyroidism and hypothyroidism: a nationwide follow-up study in 16,249 patients. Thyroid . 2002;12(5):411–419. doi:10.1089/105072502760043503 12097203
- Liao KP , Gunnarsson M , Kallberg H , et al. Specific association of type 1 diabetes mellitus with anti-cyclic citrullinated peptide-positive rheumatoid arthritis. Arthritis Rheum . 2009;60(3):653–660. doi:10.1002/art.24362 19248096
- Xue AL , Wu SY , Jiang L , Feng AM , Guo HF , Zhao P . Bone fracture risk in patients with rheumatoid arthritis: A meta-analysis. Medicine (Baltimore) . 2017;96(36):e6983. doi:10.1097/MD.0000000000006983 28885321
- Sarles H . Chronic pancreatitis and diabetes. Baillieres Clin Endocrinol Metab . 1992;6(4):745–775. doi:10.1016/S0950-351X(05)80164-8 1445167
- Hardt PD , Brendel MD , Kloer HU , Bretzel RG . Is pancreatic diabetes (type 3c diabetes) underdiagnosed and misdiagnosed? Diabetes Care . 2008;31(Suppl–2):S165–9. doi:10.2337/dc08-s244 18227480
- Munigala S , Agarwal B , Gelrud A , Conwell DL . Chronic pancreatitis and fracture: a retrospective, population-based veterans administration study. Pancreas . 2015. doi:10.1097/MPA.0000000000000381
- Vestergaard P , Rejnmark L , Mosekilde L . Relative fracture risk in patients with diabetes mellitus, and the impact of insulin and oral antidiabetic medication on relative fracture risk. Diabetologia . 2005;48(7):1292–1299. doi:10.1007/s00125-005-1786-3 15909154
- Majkowska L , Walilko E , Moleda P , Bohatyrewicz A . Thoracic spine fracture in the course of severe nocturnal hypoglycemia in young patients with type 1 diabetes mellitus–the role of low bone mineral density. Am J Emerg Med . 2014;32(7):816.e5–816.e7. doi:10.1016/j.ajem.2013.12.055
- Starup-Linde J , Gregersen S , Vestergaard P . Associations with fracture in patients with diabetes: a nested case-control study. BMJ Open . 2016;6(2):e009686-2015-009686. doi:10.1136/bmjopen-2015-009686
- Barzilay JI , Davis BR , Pressel SL , et al. The impact of antihypertensive medications on bone mineral density and fracture risk. Curr Cardiol Rep . 2017;19(9). doi:10.1007/s11886-017-0888-0
- Cheng YZ , Huang ZZ , Shen ZF , et al. ACE inhibitors and the risk of fractures: a meta-analysis of observational studies. Endocrine . 2017;55(3):732–740. doi:10.1007/s12020-016-1201-5 27995498
- Xiao F , Qu X , Zhai Z , et al. Association between loop diuretic use and fracture risk. Osteoporos Int . 2015;26(2):775–784. doi:10.1007/s00198-014-2979-8 25491766
- Hasserius R , Karlsson MK , Jonsson B , Redlund-Johnell I , Johnell O . Long-term morbidity and mortality after a clinically diagnosed vertebral fracture in the elderly–a 12- and 22-year follow-up of 257 patients. Calcif Tissue Int . 2005;76(4):235–242. doi:10.1007/s00223-004-2222-2 15812579
- Panula J , Pihlajamaki H , Mattila VM , et al. Mortality and cause of death in hip fracture patients aged 65 or older: a population-based study. BMC Musculoskelet Disord . 2011;12:105-2474-12-105. doi:10.1186/1471-2474-12-105
- Ferrari SL , Abrahamsen B , Napoli N , et al. Diagnosis and management of bone fragility in diabetes: an emerging challenge. Osteoporos Int . 2018;29(12):2585–2596. doi:10.1007/s00198-018-4650-2 30066131
- Anagnostis P , Paschou SA , Gkekas NN , et al. Efficacy of anti-osteoporotic medications in patients with type 1 and 2 diabetes mellitus: a systematic review. Endocrine . 2018;60(3):373–383. doi:10.1007/s12020-018-1548-x 29411304
- Gil-Diaz MC , Raynor J , O’Brien KO , Schwartz GJ , Weber DR . Systematic review: associations of calcium intake, vitamin D intake, and physical activity with skeletal outcomes in people with Type 1 diabetes mellitus. Acta Diabetol . 2019. doi:10.1007/s00592-019-01334-5
- Anderson SM , Buckingham BA , Breton MD , et al. Hybrid closed-loop control is safe and effective for people with type 1 diabetes who are at moderate to high risk for hypoglycemia. Diabetes Technol Ther . 2019;21(6):356–363. doi:10.1089/dia.2019.0018 31095423
- Hermanns N , Heinemann L , Freckmann G , Waldenmaier D , Ehrmann D . Impact of CGM on the management of hypoglycemia problems: overview and secondary analysis of the hypode study. J Diabetes Sci Technol . 2019;13(4):636–644. doi:10.1177/1932296819831695 30841740