
Abstract
Purpose
Free insulin-like growth factor-1 (IGF-1) ratio (the ratio of IGF-1/insulin-like growth factor binding protein-3 [IGFBP-3]) was shown to be negatively correlated with metabolic syndrome (MetS) in adults, but it was unknown in Chinese adolescents.
Patients and methods
The cross-sectional study enrolled 701 healthy school students (aged 12–16 years, 46.1% females) and 93 of them (18–22 years old, 46.2% females) were followed after 5 years.
Results
In the cross-sectional study, the IGF-1/IGFBP-3 ratios were found correlated with low-density lipoprotein cholesterol (LDL-C; r= −0.071, P<0.05) and diastolic blood pressure (r= −0.077, P=0.034). A lower IGF-1/IGFBP-3 ratio was an independent risk factor for MetS (OR =2.348, 95% CI: 1.040–5.303), hypertension (OR=1.729, 95% CI: 1.040–5.303), and increased LDL-C (OR=1.841, 95% CI: 1.230–2.755). In the follow-up study, all the participants were >18 years old. We found a lower baseline ratio of IGF-1/IGFBP-3 in adolescence was an independent risk factor for MetS in adulthood (OR=10.724, 95% CI: 1.032–11.403) and also indicated a higher body mass index (β=−1.361, 95% CI: −2.513 to −0.208) after 5 years.
Conclusion
The lower IGF-1/IGFBP-3 ratio was an independent risk factor for MetS, hypertension, and high LDL-C in adolescents of northeast China and was also a predictive marker for MetS and increased body mass index in the adulthood.
Keywords:
Introduction
In recent years, along with China’s economic development and improvements in living standards, the incidence of metabolic syndrome (MetS) has increased not only in adults but also in adolescents.Citation1,Citation2 However, the adolescent population who are in the growth and development period must be different from adults in terms of metabolic characteristics.Citation3 Identification of serum-specific markers that are closely related to adolescent MetS is significant in the prevention of MetS disease and determination of pathogenesis. Insulin-like growth factor-1 (IGF-1) is a polypeptide hormone possessing structural and functional homology with proinsulin and is widely involved in inflammation, glucose and lipid metabolism.Citation4 Ninety-nine percent of circulating IGF-1 exists in the form that binds to insulin-like growth factor binding proteins (IGFBPs), of which at least 75% of IGF-1 constitutes a stable trimer structure with insulin-like growth factor binding protein-3 (IGFBP-3) and an acid-labile subunit to extend the half-life of IGF-1 and regulate transport of IGF-1 between intravascular and extravascular spaces.Citation5–Citation8 It is widely accepted that the IGF-I/IGFBP-3 ratio can be used as a marker for the accurate assessment of free IGF-1 levels.Citation9 Studies in adults have found that free IGF-1 levels are negatively correlated with MetS;Citation10 however, a correlation between free IGF-1 levels in the adolescent population and MetS has not yet been reported.Citation11 In this study, adolescents aged 12–16 years in Liaoyang, a city in northeast China, were selected and observed for 5 years to analyze the correlations between adolescent levels of IGF-1, MetS, and its components as well as other cardiovascular disease risk factors. This will contribute not only to a deeper understanding of the pathophysiological function of IGF-1/IGFBP-3 but also to knowledge on serum-specific markers of MetS in adolescents, thereby providing data to establish control strategies for the disease.
Materials and methods
Study population
From December 2010 to January 2011, junior and senior high school students in Liaoyang, a city with a medium-sized economic development level in northeast China, were selected using the stratified cluster sampling method. Questionnaires were assigned to 947 students with informed consent signed by their guardian. In addition, fasting blood samples were collected and the levels of IGF-1, IGFBP-3, fasting plasma glucose (FPG), fasting insulin (FINS), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), and serum uric acid were determined. In total, 701 students (12–16 years old, 46.1% females) with complete data were included in the statistical analysis. These subjects had no history of anemia, diabetes, and hypertension or drug therapy. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Shengjing Hospital, China Medical University.
Height, weight, waist circumference (WC), hip circumference, and blood pressure (systolic blood pressure [SBP] and diastolic blood pressure [DBP]) were measured by a trained physician before blood sample collection. The subjects then sat quietly for more than 10 minutes, and blood pressure was measured twice in the sitting position using a desktop mercury sphygmomanometer with a 2-minute interval between measurements. The average systolic and DBP was recorded. All subjects fasted for≥10 hours at night and fasting venous blood was obtained at 07:00–09:00 the next morning. All blood samples were immediately transported to the laboratory in Liaoyang Diabetes Hospital and centrifuged (within 1 hour). FPG (Glucose Oxidase method, Olympus 400; Olympus Optical Company, Tokyo, Japan) was determined within 2 hours after centrifugation. Serum LDL-C, HDL-C, TG, and uric acid were determined by routine enzymatic methods. Some of the plasma was stored at −80°C and FINS was measured by radioimmunoassay (China Institute of Atomic Energy, Beijing, P.R. China). Serum total IGF-1 and IGFBP-3 were measured by enzyme-linked immunosorbent assay. Body mass index (BMI) was calculated by body weight/height2 (kg/m2). Steady-state model homeostasis model assessment of insulin resistance (HOMA-IR) was calculated using the following formula: HOMA-IR= fasting blood glucose (mmol/L) × FINS (μU/mL) /22.5.
The subjects were followed-up 5 years later (July 2016). As most of the students went to universities in various cities, only 93 subjects (18–22 years old, 46.2% females) were recruited in the follow-up. Methods of investigation and personnel, as well as the clinical and biochemical parameters measured, were the same as in the baseline study. None of the 93 subjects had new chronic diseases or long-term medication use during the previous 5 years.
Diagnostic criteria and definition
Metabolic syndrome for adolescents
MetS was defined according to 2007 guidelines provided by International Diabetes Federation (IDF).Citation12 These guidelines state that for an adolescent to be diagnosed as MetS, the individual must have central obesity as defined by ethnic-, gender-, and age-specific values (≥90th percentile, criteria proposed by the Capital Institute of Pediatrics),Citation13 plus any two of the following four components: hypertriglyceridemia (TG ≥1.7 mmol/L), low HDL-C (<1.03 mmol/L for individuals 10–15 years of age and boys ≥16 years of age or <1.29 mmol/L for girls ≥16 years of age), hypertension (SBP ≥130 or DBP ≥85 mmHg), and fasting hyperglycemia (FPG ≥5.6 mmol/L).
Metabolic syndrome for adults
After the 5-year follow-up, the 93 subjects were all >18 years old. The IDF definition of MetS in adult was applied to this cohortCitation14 as follows. The IDF defines MetS as having an increased WC, with ethnic-specific WC cut points (for our study population, the IDF indicates the cut points for South-Asian populations, which are ≥90 cm in men and ≥80 cm in women), plus any two of the following: 1) TG >150 mg/dL or specific treatment for this lipid abnormality; 2) HDL-C <40 mg/dL in men, <50 mg/dL in women, or specific treatment for this lipid abnormality; 3) SBP ≥130 mmHg, DBP ≥85 mmHg, or treatment for previously diagnosed hypertension; 4) FPG ≥100 mg/dL, or previously diagnosed type 2 diabetes.
Overweight/Obesity
We adopted the age- and gender-specific criteria for obesity and overweight proposed by the Group of China Obesity Task ForceCitation15 in which obesity and overweight were defined as BMI ≥95th and ≥85th percentiles, respectively.
High LDL-C hyperlipidemia
There were no diagnostic criteria for high LDL-C developed for children and adolescents in China yet. In this study, we defined LDL-C ≥95th percentile as high LDL-C.
Statistical analysis
All analyses were carried out using the statistical program SPSS for Windows (version 22.0; SPSS, Inc., Chicago, IL, USA). A normal distribution was evaluated with the Kolmogorov–Smirnov test. Nonnormally distributed variables were ln-transformed to normality before analysis. Normally distributed continuous variables are presented as mean ± standard error and nonnormally distributed variables as the median (interquartile range). Categorical data are shown as numbers (percentage) and were analyzed using a chi-square test. The between-group differences in means were tested using Kruskal–Wallis H test or ANOVA. Comparisons were conducted after adjusting for confounding factors using one-way generalized linear models. Correlations of IGF-1/ IGFBP-3 levels with MetS and other cardiovascular disease (CVD)-related risk factors were evaluated after adjusting for confounding factors with partial correlation analysis. Logistic multivariate regression analysis was used to assess associations of IGF-1/IGFBP-3 levels with MetS and risk factors of CVD. The linear regression analysis was used to analyze the relationship between different IGF-1/IGFBP-3 levels and the BMI levels after 5 years. P<0.05 was considered significant for each of these analyses.
Results
The cross-sectional study
All the subjects in this study were of Han nationality. The IGF-1 (495.39±17.42 ng/mL) and IGFBP-3 (6,489.94±334.37 ng/mL) levels were well correlated (r=0.449, P<0.01). The ratios of IGF-1/IGFBP-3 in men and women were 0.147 (95% CI: 0.127–0.168) and 0.156 (95% CI: 0.133–0.178), respectively, without significant difference (). The baseline men had a higher level of SBP than the women (). As shown in , the subjects were divided into three groups according to the tertile range values of IGF-1/IGFBP-3 ratios from low to high (group T1, T2, and T3 with age 12–16 years in each group), the IGF-1/IGFBP-3 ratio being highest in group T3. shows that the adolescents in group T3 were older than the other two groups. After adjusting for sex and age, the levels of LDL-C decreased significantly (P<0.05) with increased IGF-1/IGFBP-3 ratios. The FPG level was lowest in group T3 (P<0.05).
Figure 1 Serum IGF-1/IGFBP-3 levels in men (A) and women (B).
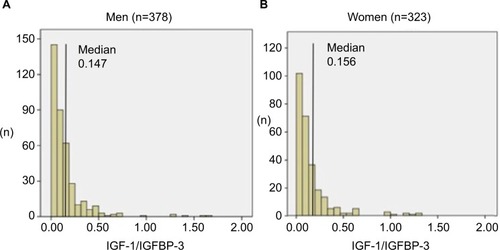
Table 1 Clinical characteristics of the subjects in baseline study and the follow-up study
Table 2 Clinical characteristics of the subjects in the groups with different levels of IGF-1/IGFBP-3
Partial correlation analysis, after age and sex were adjusted, showed that IGF-1/IGFBP-3 ratios were significantly negatively correlated with LDL-C and DBP (the correlation coefficient r was −0.071 and −0.077, respectively, all P<0.05; ).
Table 3 Partial correlation between IGF-1/IGFBP-3 ratio level and CVD risk factors
Logistic regression analysis was performed with group T3 with highest IGF-1/IGFBP-3 ratio as the reference (). The risk of MetS clearly increased with a decrease in IGF-1/IGFBP-3 ratios (P<0.05). This higher risk still existed statistically after all other factors such as age, sex, family history, high-sensitivity C-reactive protein (hs-CRP), alanine transaminase, and adiponectin were corrected, and the risk of MetS in the lowest IGF-1/IGFBP-3 group was 2.348 times that in the reference group (95% CI: 1.040–5.303). Of all the MetS components, hypertension was most closely related to the decrease in IGF-1/IGFBP-3 ratios, and the risk of hypertension in the lowest IGF-1/IGFBP-3 group was 1.729 times (95% CI: 1.040–5.303) that in the reference group. For cardiovascular disease risk factors other than MetS components, we analyzed the associations of different IGF-1/IGFBP-3 ratios with LDL-C elevation and overweight/obesity, and found that the reduction of IGF-1/ IGFBP-3 ratios was closely associated with increased LDL-C levels (odds ratio [OR]=1.841, 95% CI: 1.230–2.755), but not overweight/obesity.
Table 4 The association of IGF-1/IGFBP-3 with MetS, MetS components, and CVD risk factors
The follow-up study
There were no significant differences in basic clinical characteristics and baseline serum biochemical markers between the subjects who participated in the follow-up (n=93) and the subjects who did not participate in the follow-up survey (n=701; ), suggesting that the follow-up subjects were representative of the overall baseline population. WC, SBP, and HDL-C were significantly higher in the follow-up men than in women (). Adult MetS diagnostic criteria were used in these subjects, which was completely different from the MetS diagnostic criteria for adolescents used 5 years previously.
It was observed that BMI levels in the three groups statistically decreased with increased IGF-1/IGFBP-3 ratios (). Correlation analysis showed that the baseline IGF-1/IGFBP-3 ratios in adolescents were not correlated with any cardiovascular risk factors after 5 years in adulthood (all P>0.05; ). Logistic multivariate regression analysis showed that the risk of MetS in the baseline lowest IGF-1/IGFBP-3 group was 10.724 times (OR =10.724, CI: 1.032–11.403) that in the baseline highest IGF-1/IGFBP-3 group after 5 years, and there were no statistically significant differences between the three groups in terms of any single MetS component (). We used BMI after 5 years as the dependent variable and the three IGF-1/IGFBP-3 ratio groups as the independent variables in the linear regression analysis and found that a lower ratio of IGF-1/IGFBP-3 in adolescence indicated a significantly higher BMI in adulthood (β=−1.361, 95% CI: −2.513 to −0.208, P=0.021).
Table 5 Clinical characteristics of subjects from the three baseline groups after 5 years
Table 6 The association of IGF-1/IGFBP-3 levels with MetS and MetS components after 5 years follow-up
Discussion
Both the cross-sectional and the longitudinal data in the present study showed that IGF-1/IGFBP-3 ratios in Han adolescents in Liaoyang China were independently associated with the risk of MetS, and lower baseline IGF-1/IGFBP-3 ratios predicted a significantly higher risk of MetS when the subjects became adults 5 years later. We also found that the ratios of IGF-1/IGFBP-3 were negatively correlated with DBP and LDL-C, although this correlation was not observed 5 years later. In addition, a negative association between the baseline ratios of IGF-1/IGFBP-3 in adolescence with BMI 5 years later was revealed.
The IGF system includes three ligands (IGF-1, IGF-2, and insulin), their surface receptors, six binding proteins (IGFBP-1–6) and their proteases (eg, PAPP-A). IGF-1 enhances insulin sensitivity, promotes glucose uptake, improves lipid metabolism, and has anti-inflammatory activity.Citation16–Citation20 The IGFBP family in serum functions to regulate the endocrine actions of IGF-1 by regulating the amount of bioavailable IGF-1, and the major binding protein (>75%) for IGF-1 is IGFBP-3. A study of IGF-1 and IGFBP-3 in children and adolescents showed that the trend in IGF-1 and IGF-1/ IGFBP-3 ratio changes was the same.Citation21 Furthermore, the IGF-1/IGFBP-3 ratio had a stronger association with all of the MetS components than either IGF-1 or IGFBP-3 alone, also represents a balance between cardiac and metabolic risk.Citation22 Thus, in this study, the ratio was used to determine the correlations between IGF-1, MetS, and cardiovascular disease risk factors.
In terms of whether IGF-1/IGFBP-3 ratios are associated with the risk of MetS, in recent years, studies of different populations have not been consistent. A low ratio of IGF-1/ IGFBP-3 was associated with an increased prevalence of MetS, according to a cross-sectional study of the German adult population by Friedrich et al.Citation23 In contrast, Yeap et al found that the IGF-1/IGFBP-3 ratio was independent of MetS based on the data obtained from 3,980 males >70 years old in Australia.Citation24 These studies suggest that the relationship between the IGF-1/IGFBP-3 ratio and MetS may be different due to age or race. Numerous epidemiological and clinical studies have shown that MetS is a complex phenotype, and abnormal glucose and lipid metabolism, insulin resistance, central obesity, and the inflammatory reaction are leading factors in the development of MetS.Citation25,Citation26 Thus, in addition to IGF-1, population-specific factors, diet, physical activity environment affect the onset of MetS, which explain the contradicting results in the literature.
In this study, the correlation between IGF-1/IGFBP-3 ratio and MetS in the adolescent population in northeastern China was determined, and a 5-year follow-up study was performed to further investigate whether this correlation changed with age. In the cross-sectional investigation, we found that there was a clear association between the IGF-1/ IGFBP-3 ratios and the high risk of MetS, and this association was driven by hypertension, which was shown to be the most closely correlated component. In the follow-up study, we also found a strong correlation between baseline IGF-1/ IGFBP-3 ratios in adolescents and the presence of MetS in early adulthood, although different diagnostic criteria were used at different stages, while no correlation between baseline IGF-1/IGFBP-3 ratio and any MetS components in the adult period was found. As to this inconsistency, we speculated that the effects from various MetS components showed the same trend; thus, the accumulated effects led to the significant correlation between baseline IGF-1/IGFBP-3 ratios and overall risk of MetS after 5 years. Our present study was the first longitudinal one to reveal the prospective effects of IGF-1/ IGFBP-3 for MetS. Also, it was a novel finding that despite changes in growth and development from adolescence to adulthood, adolescent IGF-1/IGFBP-3 ratios were still indicative of adult metabolic diseases.
In addition to MetS components, LDL-C was also considered as an important cardiovascular risk factor. We found a significant negative correlation between IGF-1/IGFBP-3 and LDL-C levels, and a decrease in IGF-1/IGFBP-3 ratio was an independent risk factor for high LDL-C. In contrast, TG and HDL-C, which are closely related to MetS, did not show any independent association with IGF-1/IGFBP-3 in this study. Malík et al also demonstrated this difference in their study, as the IGF-1/IGFBP-3 ratio was reduced in patients with hypercholesterolemia alone, but elevated in the mixed hyperlipidemia group.Citation27 Therefore, the relationship between IGF-1 or IGFBP-3 and various lipid metabolism components may not be the same. As the evaluation of obesity, BMI was not associated with IGF-1/IGFBP-3 ratio in the adolescent cross-sectional data. However, in the follow-up study, when the 93 adolescents became adults, the group with the lowest ratio of IGF-1/IGFBP-3 in adolescence showed the highest level of BMI in adulthood, which was consistent with the increased risk of MetS. It was reported that the association of IGF-1 with MetS was affected by adiponectin, hs-CRP, and abnormal liver function,Citation10,Citation24,Citation28 and that is why we adjusted these potentially confounding factors in the analysis to show an independent relationship. Some national and international studies showed that the IGF-1/IGFBP-3 ratio was negatively correlated with the number of MetS components,Citation12,Citation21,Citation29 which was not found in this study (results not shown).
The results of our cross-sectional and prospective studies were not completely the same, and this was presumably due to the following reasons. First, the subjects experienced adolescence and adulthood, and definitions of cardiovascular disease risk factors such as MetS components and overweight/ obesity in the two periods were very different; thus, even in the same disease state, the degree of consistency of diagnosis for subjects before and after was significantly reduced due to different criteria. Second, the correlation between IGF-1/IGFBP-3 ratio and metabolic diseases was affected by factors such as age, growth, and development, which could partly explain why the results of published studies in different age groups were often contradictory. For example, a study of young people aged 11–18 years in the United States showed a clear correlation between IGF-1/IGFBP-3 ratio and adolescent blood pressure,Citation30 while another study carried out in young people aged 20–34 years failed to find this correlation.Citation31 Third, as most of the subjects had gone to universities in different cities, the follow-up sample size in the present study was small, which was an obvious flaw of this study. Therefore, expanding the follow-up sample size and prolonging the follow-up period would help to further elucidate the causal relationships between IGF-1/IGFBP-3 ratio, adolescent MetS, and various cardiovascular disease risk factors.
Conclusion
Using cross-sectional and prospective methods, we determined the ratios of IGF-1/IGFBP-3 in Han adolescents aged 12–16 years residing in Liaoyang, northeastern China, and showed that a decrease in IGF-1/IGFBP-3 ratios in adolescents had a predictive effect on the high risk of MetS in adulthood. The prevalence of obesity, type 2 diabetes, and other metabolic diseases in Chinese adolescents is increasing.Citation32 The IGF-1/IGFBP-3 ratio would be useful for epidemiological screening as a simple and effective serum marker of MetS, especially its predictive ability for future MetS and higher BMI in adulthood, which is of great practical value.
Acknowledgments
The authors are grateful to all children and their parents for participating in this study. This work was supported by Fund for young scientists of the National Natural Science Foundation of China (grant number 81600644).
Supplementary Materials
Table S1 Comparison of clinical characteristics between the follow-up group and the non-follow-up group
Table S2 Partial correlation between IGF-1/IGFBP-3 ratio level and risk factors for cardiovascular disease in follow-up group
Disclosure
The authors report no conflicts of interest in this work.
References
- Xi B He D Hu Y Zhou D Prevalence of metabolic syndrome and its influencing factors among the Chinese adults: the China health and Nutrition Survey in 2009 Prev Med 2013 57 6 867 871 24103567
- Ye P Yan Y Ding W 中国儿童青少年代谢综合征患病率Meta 分析 [Prevalence of metabolic syndrome in Chinese children and adolescents: a meta-analysis] Zhonghua Liu Xing Bing Xue Za Zhi 2015 36 8 884 888 Chinese 26714549
- Agirbasli M Tanrikulu AM Berenson GS Metabolic syndrome: bridging the gap from childhood to adulthood Cardiovasc Ther 2016 34 1 30 36 26588351
- Clemmons DR Metabolic actions of insulin-like growth factor-I in normal physiology and diabetes Endocrinol Metab Clin North Am 2012 41 2 425 443 22682639
- Mohan S Baylink DJ IGF-binding proteins are multifunctional and act via IGF-dependent and -independent mechanisms J Endocrinol 2002 175 1 19 31 12379487
- Clemmons DR Role of IGF binding proteins in regulating metabolism Trends Endocrinol Metab 2016 27 6 375 391 27117513
- Rajpathak SN Gunter MJ Wylie-Rosett J The role of insulin-like growth factor-I and its binding proteins in glucose homeostasis and type 2 diabetes Diabetes Metab Res Rev 2009 25 1 3 12 19145587
- Rosenfeld RG Hwa V Wilson E Plymate SR Oh Y The insulin-like growth factor-binding protein superfamily Growth Horm IGF Res 2000 10 Suppl A S16 S17 10984276
- Juul A Dalgaard P Blum WF Serum levels of insulin-like growth factor (IGF)-binding protein-3 (IGFBP-3) in healthy infants, children, and adolescents: the relation to IGF-I, IGF-II, IGFBP-1, IGFBP-2, age, sex, body mass index, and pubertal maturation J Clin Endocrinol Metab 1995 80 8 2534 2542 7543116
- Koegelenberg AS Schutte R Smith W Schutte AE Bioavailable IGF-1 and its relation to the metabolic syndrome in a bi-ethnic population of men and women Horm Metab Res 2016 48 2 130 136 26348017
- Liang S Hu Y Liu C Qi J Li G Low insulin-like growth factor 1 is associated with low high-density lipoprotein cholesterol and metabolic syndrome in Chinese nondiabetic obese children and adolescents: a cross-sectional study Lipids Health Dis 2016 15 1 112 27343122
- Zimmet P Alberti G Kaufman F The metabolic syndrome in children and adolescents Lancet 2007 369 9579 2059 2061 17586288
- Guansheng MA Chengye Ji Jun MA Waist circumference reference values for screening cardiovascular risk factors in Chinese children and adolescents aged 7-18 years Chin J Epidemiol 2010 31 609 615
- Herrera-Enriquez K Narvaez-Guerra O Discordance of metabolic syndrome and abdominal obesity prevalence according to different criteria in Andean highlanders: a community-based study Diabetes Metab Syndr 2017 11 Suppl 1 S359 S364 28284909
- Group of China Obesity Task Force The classification standard of body mass index for overweight and obesity in Chinese school-age children and adolescents Chin J Epidemiol 2004 25 97 102
- Knacke H Pietzner M Do KT Metabolic fingerprints of circulating IGF-1 and the IGF-1/IGFBP-3 ratio: a multifluid metabolomics study J Clin Endocrinol Metab 2016 101 12 4730 4742 27710242
- Conti E Andreotti F Sestito A Reduced levels of insulin-like growth factor-1 in patients with angina pectoris, positive exercise stress test, and angiographically normal epicardial coronary arteries Am J Cardiol 2002 89 8 973 975 11950439
- Dimmeler S Zeiher AM Exercise and cardiovascular health: get active to “AKTivate” your endothelial nitric oxide synthase Circulation 2003 107 25 3118 3120 12835404
- Malik J Stulc T Ceska R Unraveling Reaven’s syndrome X: serum insulin-like growth factor-I and cardiovascular disease Circulation 2003 107 20 190 192
- Spies M Nesic O Barrow RE Perez-Polo JR Herndon DN Liposomal IGF-1 gene transfer modulates pro- and anti-inflammatory cytokine mRNA expression in the burn wound Gene Ther 2001 8 18 1409 1415 11571581
- Kong APS Wong GWK Choi K-C Reference values for serum levels of insulin-like growth factor (IGF-1) and IGF-binding protein 3 (IGFBP-3) and their ratio in Chinese adolescents Clin Biochem 2007 40 15 1093 1099 17673197
- Sierra-Johnson J Romero-Corral A Somers VK IGF-I/IGFBP-3 ratio: a mechanistic insight into the metabolic syndrome Clin Sci 2009 116 6 507 512 18816247
- Friedrich N Nauck M Schipf S Cross-sectional and longitudinal associations between insulin-like growth factor I and metabolic syndrome: a general population study in German adults Diabetes Metab Res Rev 2013 29 6 452 462 23576494
- Yeap BB Chubb SA Ho KK IGF1 and its binding proteins 3 and 1 are differentially associated with metabolic syndrome in older men Eur J Endocrinol 2010 162 2 249 257 19917654
- Cornier MA Dabelea D Hernandez TL The metabolic syndrome Endocr Rev 2008 29 7 777 822 18971485
- Leroith D Pathophysiology of the metabolic syndrome: implications for the cardiometabolic risks associated with type 2 diabetes Am J Med Sci 2012 343 1 13 16 22205060
- Malík J Stulc T Wichterle D Hyperlipidemia is associated with altered levels of insulin-like growth factor-I Physiol Res 2008 57 6 919 925 18052685
- Oh J Kim JY Park S The relationship between insulin-like growth factor-1 and metabolic syndrome, independent of adiponectin Clinica Chimica Acta 2012 413 3–4 506 510
- Parekh N Roberts CB Vadiveloo M Lifestyle, anthropometric, and obesity-related physiologic determinants of insulin-like growth factor-1 in the third National Health and Nutrition Examination Survey (1988–1994) Ann Epidemiol 2010 20 3 182 193 20159489
- Jiang X Srinivasan SR Dalferes ER Berenson GS Plasma insulin- like growth factor 1 distribution and its relation to blood pressure in adolescents: the Bogalusa heart study Am J Hypertens 1997 10 7Pt 1 714 719 9234824
- Colangelo LA Liu K Gapstur SM CARDIA Male Hormone Study Insulin-like growth factor-1, insulin-like growth factor binding protein-3, and cardiovascular disease risk factors in young black men and white men: the CARDIA Male Hormone Study Am J Epidemiol 2004 160 8 750 757 15466497
- Viner R White B Christie D Type 2 diabetes in adolescents: a severe phenotype posing major clinical challenges and public health burden Lancet 2017 389 10085 2252 2260 28589895