Abstract
Objective
This study aimed to compare the glucose-lowering effect and glycemic variability of insulin glargine with those of insulin detemir.
Material and methods
This was an open-label, single-center, randomized, two-way crossover study in patients with diabetes on basal-bolus insulin therapy, with neutral protamine Hagedorn (NPH) insulin as basal insulin. Patients switched from NPH insulin to a course either of insulin glargine followed by insulin detemir, or insulin detemir followed by insulin glargine, continuing the same dose of the prior bolus of insulin. To evaluate the glucose-lowering effect, daily glycemic profiles were recorded for 72 hours by continuous glucose monitoring (CGM) in an outpatient setting. The mean amplitude of glycemic excursions, standard deviation (SD), and the mean of daily difference (MODD) were used to assess intraday and day-to-day glycemic variability.
Results
Eleven patients were enrolled and nine completed the study. Mean blood glucose calculated from CGM values was significantly lower with insulin glargine compared with insulin detemir (9.6 ± 2.4 mmol/L versus 10.4 ± 2.8 mmol/L, P = 0.038). The SD was significantly lower with insulin glargine versus insulin detemir (2.5 ± 0.9 mmol/L vs 3.5 ± 1.6 mmol/L, P = 0.011). The MODD value was significantly lower with insulin glargine than with insulin detemir (2.2 ± 1.1 mmol/L vs 3.6 ± 1.7 mmol/L, P = 0.011). There was no significant difference between the two insulin analogs in terms of hypoglycemia.
Conclusion
This study suggests that insulin glargine leads to more effective and more stable glycemic control than the same dose of insulin detemir.
Introduction
The Diabetes Control and Complications TrialCitation1 and the Kumamoto StudyCitation2 have shown that intensive insulin therapy and the resulting improvements in glycemic control reduce the incidence and delay the progression of microvascular complications. However, neutral protamine Hagedorn (NPH) insulin, which was used as basal insulin in these studies, has several limitations. Of note, its duration of action is only 8–12 hours, with a peak in action occurring within 4–6 hours after subcutaneous administration, thus increasing the risk of hypoglycemia.Citation3–Citation7 Indeed, some patients complain of hypoglycemia before dawn, necessitating a reduction in the NPH insulin dose at bedtime. However, reducing the NPH insulin dose at bedtime increases the blood glucose level in the morning. Additionally, NPH insulin is a suspension, which must be thoroughly resuspended before injection, and inadequate resuspension results in a very large day-to-day glycemic variability of action.Citation8,Citation9 Therefore, to achieve tight glycemic control without increasing the risk of hypoglycemia, insulin preparations with a long duration of action and low day-to-day glycemic variability in terms of glucose-lowering action are needed.
Insulin glargineCitation4,Citation6,Citation10 and insulin detemirCitation5,Citation7,Citation11,Citation12 are basal insulin analogs of the dissolution type that have flatter profiles and longer duration of action compared with NPH insulin. However, there is controversy over which insulin analog has the longer and more stable action. Therefore, in this study, the aim was to compare the glucose-lowering effect and glycemic stability of insulin glargine with those of insulin detemir using continuous glucose monitoring (CGM).
Material and methods
Patients
Diabetic patients who were prescribed basal-bolus insulin therapy with NPH insulin as basal insulin at bedtime for 1 year or more were enrolled in the study. Patients who injected NPH insulin two or more times per day, with proteinuria >1.0 g/day, serum creatinine >132 μmol/L (men) or 106 μmol/L (women), abnormal aspartate aminotransferase/ alanine aminotransferase elevation (>3 ×the upper limit of normal), myocardial infarction or stroke within 6 months prior to study entry, or HbA1c > 10.0% or <5.8%, were excluded from this study.
All patients received an explanation of the procedures and possible disadvantages of participating in the study and gave written informed consent prior to entry. This study was approved by the Institutional Review Board of Kitasato Institute Hospital and was performed in accordance with the Declaration of Helsinki.
Design of the study
Patients were randomized using a computer to either Sequence A (NPH insulin was first switched to insulin glargine, then to insulin detemir) or Sequence B (insulin detemir followed by insulin glargine). The patient’s prior NPH insulin was discontinued and replaced with the allocated long-acting insulin analog (insulin glargine or insulin detemir). Patients were asked to continue their other antihyperglycemic medications and to not change their dosage throughout the study. To compare insulin glargine with insulin detemir under the same conditions, the dose of the long-acting insulin analogs was the same as that of NPH, and the doses of bolus insulin (insulin lispro or insulin aspart) were not changed. The study drugs were injected at bedtime. The CGM examination, of 72 hours in duration from 12 pm on day 1 to 12 pm on day 4, was carried out at least 5 days after switching insulin. The study drugs were crossed over on the day when the first CGM examination ended.
The CGM sensor (CGMS® System Gold; Medtronic, Northridge, CA) was applied to the abdominal area by a certified diabetologist. Patients were instructed to measure their capillary blood glucose using finger sticks, at least four times per day (at mealtimes and at bedtime). Glucose meters were calibrated immediately before starting CGM. All patients used the CGM in outpatient settings.
Glycemic control
The outcomes of this study included determining the effectiveness of each type of insulin on glycemic control and glycemic variability. Glycemic control was estimated as the mean blood glucose (MBG), the area under the glucose curve above 7.8 or 10.0 mmol/L (area under the curve [AUC]>7.8,10), and the percentage of time above 7.8 or 10.0mmol/L (t>7.8,10). The AUC was calculated using the trapezoidal method.
Glycemic variability
Intraday glycemic variability was assessed as the standard deviation (SD) and the mean amplitude of glycemic excursions (MAGE). The SD around the mean glucose values is considered the “gold standard” assessment of intraday glycemic variability.Citation13 MAGE, described by Service et al,Citation14 is probably more appropriate for selecting the major glucose swings that are calculated as the arithmetic mean of differences between consecutive peaks and nadirs, provided that the differences are greater than the SD around the mean values.Citation13
Day-to-day glycemic variability was assessed as the mean of daily difference (MODD). MODD, described by Molnar et al,Citation15 is the mean of the absolute difference between glucose values taken on 2 consecutive days at the same time.
Hypoglycemia
Hypoglycemia, which was defined as a sensor value of ≤3.9 mmol/L, was also calculated as a total time at ≤3.9 mmol/L. Severe hypoglycemia was defined as a sensor value of ≤2.8 mmol/L.
Statistical analysis
All values are shown as means with SD. The differences between two insulin analogs were analyzed using the Wilcoxon rank-sum test. A P value of <0.05 was considered statistically significant. SPSS software 14.0J (SPSS Japan Inc, Tokyo, Japan) was used for all statistical analyses.
Results
Patient characteristics
A total of eleven Japanese patients, six with type 1 and five with type 2 diabetes, were enrolled between May 2008 and June 2009. Because of an alert for insulin glargine issued by the European Association for the Study of Diabetes,Citation16 this study was discontinued and the available data was analyzed. Two patients were excluded from analysis because of protocol violation (misuse of NPH). Therefore, nine patients (five in Sequence A and four in Sequence B) completed the study. The demographic and baseline characteristics of these patients are shown in .
Table 1 Patient demographics and baseline characteristics
Glycemic control
MBG, as calculated from CGM values, was significantly lower with insulin glargine than with insulin detemir (9.6 ± 2.4 mmol/L versus 10.4 ± 2.8 mmol/L, P = 0.038) (type 1: 11.0 ± 2.5 mmol/L versus 12.2 ± 2.7 mmol/L; type 2: 8.4 ± 1.8 mmol/L versus 9.0 ± 2.2 mmol/L). shows the mean daily profiles of day 2 and day 3. This difference between the two insulin analogs was particularly evident at nighttime. In addition, AUC>10 and AUC>7.8 were significantly lower with insulin glargine versus insulin detemir ().
Figure 1 24-hour glucose profiles of day 2 and day 3. Each point represents the mean± standard deviation of nine patients treated with insulin glargine (○) or detemir (▪).
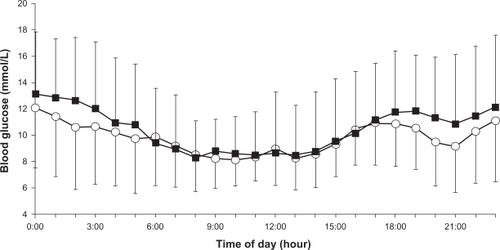
Table 2 Comparison of glargine CGM data with detemir CGM data
Glycemic variability
The SD was significantly lower with insulin glargine than with insulin detemir. However, the MAGE value was not significantly different between the two insulin analogs (). The MODD value was significantly lower with insulin glargine than with insulin detemir (2.2 ± 1.1 mmol/L vs 3.6 ± 1.7 mmol/L, P = 0.011; ) (type 1: 2.7 ± 1.2 mmol/L vs 4.7 ± 1.8 mmol/L; type 2: 1.8 ± 0.9 mmol/L vs 2.7 ± 0.9 mmol/L).
Figure 2 Comparison of the mean of daily difference (MODD) in nine patients treated with insulin glargine or detemir. The MODD value was significantly lower with insulin glargine than with insulin detemir.
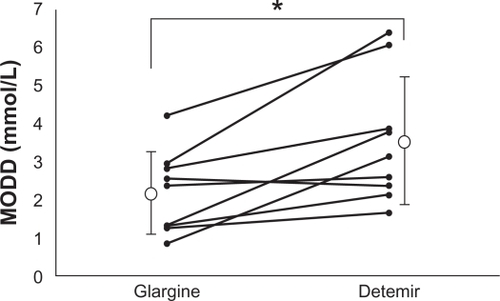
Table 3 Comparison of the intraday glycemic variability of glargine with that of detemir
Hypoglycemia
There was no difference between the two insulin analogs in terms of the total hypoglycemic time. This lack of a difference remained even after separating the results according to daytime and nighttime values. Severe hypoglycemic time was also similar for both insulin analogs ().
Discussion
In this study, the glucose-lowering effect and glucose stability of insulin glargine was compared with those of insulin detemir using CGM. Glycemic control parameters, such as MBG, AUC>10, and AUC>7.8, were better with insulin glargine than with insulin detemir. The present study suggests that insulin glargine has a greater glucose-lowering effect than insulin detemir at the same dose. The difference in glucose-lowering effect can be compensated for by increasing the insulin dose but there might be a difference in the cost-effectiveness and hypoglycemic episode. Because the same tendency was found in both type 1 and type 2 diabetes (MBG in type 1: insulin glargine, 11.0 ± 2.5 mmol/L versus insulin detemir, 12.2 ± 2.7 mmol/L; type 2: 8.4 ± 1.8 mmol/L versus 9.0 ± 2.2 mmol/L), to maintain statistical power, the two types of diabetes were not distinguished.
However, the hypoglycemic time was comparable for both of the two insulin analogs. These findings suggest that, if higher doses of insulin detemir are administered to achieve equivalent glycemic control to insulin glargine, the hypoglycemic time might increase.
Furthermore, the intraday and day-to-day glycemic variability of insulin glargine was compared with those of insulin detemir. The results of CGM revealed that SD and MODD were lower with insulin glargine than with insulin detemir. These findings suggest that insulin glargine might have better glycemic variability compared with insulin detemir. It is expected that the risk of hypoglycemia is lower with insulin glargine than with insulin detemir, if the aim of treatment is near-normal glycemia.
Several previous studies have compared insulin glargine with insulin detemir.Citation17–Citation29 Three studies using insulin-clamp tests yielded very conflicting results.Citation17–Citation19 Heise et al reported that the same doses (0.4 U/kg) of insulin glargine and insulin detemir are very similar in terms of the mean shape of their pharmacodynamic profiles and duration of action in patients with type 1 diabetes.Citation17 They also reported that the day-to-day glycemic variability is lower with insulin detemir. Klein et al reported a similar duration of action and lower day-to-day glycemic variability with insulin detemir versus insulin glargine in patients with type 2 diabetes (0.8–1.6 U/kg).Citation18 By contrast, Porcellati et al reported that 0.35 U/kg of insulin detemir has similar effects to the same dose of insulin glargine during the first 12 hours, and that the metabolic effects of insulin detemir are lower at 12–24 hours.Citation19
Six clinical studies have compared insulin glargine with insulin detemir. In five studies, in which all patients or more than half of the patients were injected with insulin detemir twice daily, glycemic control was similar to that of once-daily insulin glargine.Citation20–Citation24 The other study, in which the majority (87.4%) of patients were injected with insulin detemir once a day, suggested inferiority of glycemic control for insulin detemir versus once-daily insulin glargine.Citation25
These clinical studies clearly showed that, at similar daily doses, insulin detemir has a shorter action time and weaker action than insulin glargine. These findings are consistent with the results of the present study and with the results of a clamp study reported by Porcellati et al.Citation19
Tone et al compared the day-to-day glycemic variability of insulin glargine with that of insulin detemir.Citation26 However, CGM was not used and the study evaluated only fasting plasma glucose; therefore, the study was inconclusive. However, King et al and Wiesli et al have reported comparisons of insulin glargine with insulin detemir using CGM. Although these studies concluded that once-daily insulin detemir provided 24-hour glycemic control similar to that of insulin glargine in patients with type 2 diabetes, did glycemic variability was not reported.Citation27–Citation29 To the best of the present authors’ knowledge, the present study is the first to show that insulin glargine has better glycemic variability than insulin detemir based on CGM.
There are several limitations to this study. First, because of the alert for insulin glargine, it was deemed inappropriate to continue enrolling patients to receive insulin glargine. Therefore, the number of subjects enrolled was too small to reach a definitive conclusion and patients with type 1 and type 2 diabetes were combined. However, as shown in , most of the patients had lower MODD values with insulin glargine than with insulin detemir. In fact, our finding of lower MODD was consistent after stratification for the type of diabetes (insulin glargine versus insulin detemir, type 1: 2.7 ± 1.2 mmol/L versus 4.7 ± 1.8 mmol/L; type 2: 1.8 ± 0.9 mmol/L versus 2.7 ± 0.9 mmol/L). Therefore, the authors’ believe this conclusion may be robust. Second, the doses of basal insulin used in the present study were different from those used in the earlier clinical studies. The average basal insulin dose was 0.24 U/kg/day in this study (type 1: 0.22 U/kg/day; type 2: 0.26 U/kg/day), which was much lower than in earlier clinical studies (insulin glargine: 0.33Citation21–0.75Citation25 U/kg/day; insulin detemir: 0.40Citation21–0.82Citation23 U/kg/day). However, these studies were performed in European countries or in the USA. The doses of basal insulin used in our study are similar to those used in the Japanese national phase III program for insulin glargine for Japanese patients with type 1 diabetes (mean: 0.21 U/kg/day)Citation30 and insulin detemir for Japanese patients with type 1 or type 2 diabetes (mean: 0.27 U/kg/day).Citation31 Therefore, the insulin dose in the present study appears to be appropriate for Japanese patients.
Conclusion
The results of the present study suggest that insulin glargine provides more effective and more stable glycemic control than insulin detemir. Because this study was too small to make a final conclusion, however, large-scale studies are required to confirm these findings.
Disclosure
The authors report no conflicts of interest in this work.
References
- Diabetes Control and Complications Trial (DCCT) Research Group The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus N Engl J Med 2003 329 977 986
- Ohkubo Y Kishikawa H Araki E Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus Diabetes Res Clin Pract 1995 28 103 117 7587918
- Hirsch IB Insulin analogues N Engl J Med 2005 352 174 183 15647580
- Lepore M Pampanelli S Fanelli C Pharmacokinetics and pharmacodynamics of subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente human insulin and continuous subcutaneous infusion of insulin lispro Diabetes 2000 49 2142 2148 11118018
- Plank J Bodenlenz M Sinner F A double-blind, randomized, dose-response study investigating the pharmacodynamic and pharmacokinetic properties of the long-acting insulin analog detemir Diabetes Care 2005 28 1107 1112 15855574
- Heinemann L Linkeschova R Rave K Hompesch B Sedlak M Heise T Time-action profile of the long-acting insulin analog insulin glargine (HOE901) in comparison with those of NPH insulin and placebo Diabetes Care 2000 23 644 649 10834424
- Fanelli GC Pampanelli S Porcellati F Rossetti P Brunetti P Bolli GB Administration of neutral protamine Hagedorn insulin at bedtime versus dinner in type 1 diabetes mellitus to avoid nocturnal hypoglycemia and improve control. A randomized, controlled trial Ann Intern Med 2002 136 504 514 11926785
- Jehle PM Micheler C Jehle DR Breitig D Boehm BO Inadequate suspension of neutral protamine Hagedorn (NPH) insulin in pens Lancet 1999 354 1604 1607 10560676
- Kølendorf K Bojsen J Deckert T Clinical factors influencing the absorption of 125I-NPH insulin in diabetic patients Horm Metab Res 1983 15 274 278 6409773
- Wang F Carabino JM Vergara CM Insulin glargine: a systematic review of a long-acting insulin analogue Clin Ther 2003 25 1541 1577 12860485
- Kurtzhals P Havelund S Jonassen I Albumin binding of insulins acylated with fatty acids: characterization of the ligand-protein interaction and correlation between binding affinity and timing of the insulin effect in vivo Biochem J 1995 312 725 731 8554512
- Havelund S Plum A Ribel U The mechanism of protraction of insulin detemir, a long-acting, acylated analog of human insulin Pharm Res 2004 21 1498 1504 15359587
- Monnier L Colette C Owens DR Glycemic variability: the third component of the dysglycemia in diabetes. Is it important? How to measure it? J Diabetes Sci Technol 2008 2 1094 1100 19885298
- Service FJ Molnar GD Rosevear JW Ackerman E Gatewood LC Taylor WF Mean amplitude of glycaemic excursions, a measure of diabetic instability Diabetes 1970 19 644 655 5469118
- Molnar GD Taylor WF Ho MM Day-to-day variation of continuously monitored glycaemia: a further measure of diabetic instability Diabetologia 1972 8 342 348 4641791
- Hemkens LG Grouven U Bender R Risk of malignancies in patients with diabetes treated with human insulin or insulin analogues: a cohort study Diabetologia 2009 52 1732 1744 19565214
- Heise T Nosek L Ronn BB Lower within-subject variability of insulin detemir in comparison to NPH insulin and insulin glargine in people with type 1 diabetes Diabetes 2004 53 1614 1620 15161770
- Klein O Lynge J Endahl L Damholt B Nosek L Heise T Albumin-bound basal insulin analogues (insulin detemir and NN344): comparable time-action profiles but less variability than insulin glargine in type 2 diabetes Diabetes Obes Metab 2007 9 290 299 17391154
- Porcellati F Rossetti P Busciantella NR Comparison of pharmacokinetics and dynamics of the long-acting insulin analogs glargine and detemir at steady state in type 1 diabetes: a double-blind, randomized, crossover study Diabetes Care 2007 30 2447 2452 17623819
- Rosenstock J Davies M Home PD Larsen J Koenen C Schernthaner G A randomized, 52 week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naïve people with type 2 diabetes Diabetologia 2008 51 408 416 18204830
- Heller S Koenen C Bode B Comparison of insulin detemir and insulin glargine in a basal-bolus regimen, with insulin aspart as the mealtime insulin, in patients with type 1 diabetes: a 52-week, multinational, randomized, open-label, parallel-group, treat-to-target noninferiority trial Clin Ther 2009 31 2086 2097 19922879
- Pieber TR Treichel HC Hompesch B Comparison of insulin detemir and insulin glargine in subjects with Type 1 diabetes using intensive insulin therapy Diabet Med 2007 24 635 642 17381500
- Hollander P Cooper J Bregnhøj J Pedersen CB A 52-week, multinational, open-label, parallel-group, noninferiority, treat-to-target trial comparing insulin detemir with insulin glargine in a basal-bolus regimen with mealtime insulin aspart in patients with type 2 diabetes Clin Ther 2008 30 1976 1987 19108786
- Swinnen SG Dain MP Aronson R A 24-week, randomized, treat-to-target trial comparing initiation of insulin glargine once-daily with insulin detemir twice-daily in patients with type 2 diabetes inadequately controlled on oral glucose-lowering drugs Diabetes Care 2010 33 1176 1178 20200301
- Raskin P Gylvin T Weng W Chaykin L Comparison of insulin detemir and insulin glargine using a basal-bolus regimen in a randomized, controlled clinical study in patients with type 2 diabetes Diabetes Metab Res Rev 2009 25 542 548 19565569
- Tone A Iseda I Higuchi C Comparison of insulin detemir and insulin glargine on glycemic variability in patients with type 1 and type 2 diabetes Exp Clin Endocrinol Diabetes 2010 118 320 324 20072962
- King AB Once-daily insulin detemir is comparable to once-daily insulin glargine in providing glycaemic control over 24 h in patients with type 2 diabetes: a double-blind, randomized, crossover study Diabetes Obes Metab 2009 11 69 71 19120433
- King AB No higher dose requirements with insulin detemir than glargine in type 2 diabetes: a crossover, double-blind, and randomized study using continuous glucose monitoring J Diabetes Sci Technol 2010 4 151 154 20167179
- Wiesli P Krayenbuhl P Uthoff H Seifert B Schmid C Omitting breakfast and lunch after injection of different long-acting insulin preparations at bedtime: a prospective study in patients with type 2 diabetes Diabetologia 2009 52 1816 1819 19565212
- Kawamori R Iwamoto Y Kadowaki T Iwasaki M Comparison of efficacy between insulin glargine and NPH human insulin in type 1 diabetes patients undergoing intensive insulin treatment – phase II/III clinical studies in Japan [in Japanese] Rinsho Iyaku 2003 19 423 440
- Kobayashi M Iwamoto Y Kaku K Kawamori R Tajima N 48-week randomized multicenter open-label parallel group phase 3 trial to compare insulin detemir and NPH insulin efficacy and safety in subjects with insulin requiring diabetes mellitus in a basal-bolus regimen [in Japanese] J Japan Diab Soc 2007 50 649 663