
Abstract
Background
Diabetes is one of the most prevalent noncommunicable diseases worldwide. Children’s lipid accumulation product (CLAP) is a novel indicator to show children’s lipid accumulation and is effectively associated with metabolic syndrome among children and adolescents. The aim of the present study was to explore an association between CLAP and impaired fasting glucose (IFG) in Chinese children and adolescents.
Methods
A total of 683 children and adolescents aged 8–15 years were recruited using the stratified cluster sampling method in this cross-sectional study and were measured for body height, weight, waist circumference (WC), abdominal skinfold thickness (AST), triglycerides (TG), fasting plasma glucose, dietary behaviors and physical activities. A logistic regression model and receiver operating characteristic (ROC) curve were used to compare the effects of CLAP for predicting IFG.
Results
The prevalence of IFG in children and adolescents was 13.8%: 16.9% in boys and 10.1% in girls (P<0.05). The CLAP, height, weight, WC, AST, waist-to-height ratio (WHtR), and TG among boys with IFG were significantly higher than those among boys without IFG (P<0.05). The area under the ROC curve of CLAP for predicting IFG (0.637 (0.562–0.712)) was higher than those of WC, WHtR, AST, and TG. The cutoff point of P75 CLAP was the optimal value to predict IFG among boys, and the OR (95% CI) was 2.48 (1.40–4.42) and area under the ROC curve was 0.595 (0.513–0.676).
Conclusion
The CLAP was a novel indicator associated with IFG in Chinese boys, and it performed better than WC, WHtR, AST and TG.
Introduction
Diabetes is one of the most prevalent noncommunicable diseases worldwide, especially in developing countries.Citation1 The International Diabetes Federation reported approximately 86,000 new cases of T1DM in children per year worldwide.Citation2 A study showed that the prevalence of T2DM among adolescents and children increased by 30.5% in the United States from 2001 to 2009.Citation3 In addition, there was a high prevalence of impaired fasting glucose (IFG) in children.Citation4 A study from Chahkandi et al showed a prevalence of 10.6% for impaired fasting glucose in boys.Citation5 The individuals with impaired fasting glucose might progress to become diabetes patients.Citation6 The United States Preventive Services Task Force (USPSTF) recommended that screening for impaired fasting plasma glucose was important for preventing diabetes and identifying potential treatment for patients with undiagnosed diabetes.Citation7,Citation8
Previous studies reported that obesity and abdominal obesity were not only risk factors for insulin resistance syndrome but also related to abnormal glucose metabolism.Citation9 The BMI, waist circumference (WC), abdominal skinfold thickness (AST), and waist-to-height ratio (WHtR) are generally used to define obesity.Citation9–Citation12 BMI has been considered as an effective indicator for identifying diabetes.Citation13 However, a recent study showed that half of obese people based on body fat percentage (BFP) were classified as normal weight by BMI. In addition, the study showed that 33% of people with normal weight according to BMI were diagnosed with prediabetes or had undiagnosed diabetes.Citation14 Ford et alCitation15 reported that WC was a better predictor of diabetes than BMI. Schulze et alCitation16 reported that WC and WHtR are equivalently stronger predictors of diabetes than BMI among women, and WHtR improved the predictive power of diabetes compared with WC among men. However, WC and WHtR did not show the excess body fat present in circulating blood.Citation17 Scholars have suggested that diabetes might be related to the accumulation of ectopic or liver fat.Citation18 The excess lipid fuel appeared eventually as an enlarged abdomen or as elevated circulating triglycerides (TG).Citation12
Lipid accumulation product (LAP) was proposed to show the total lipid accumulation in adults: LAP for men= [WC (cm)-65]×TG (mmol/L); LAP for women=[WC (cm)-58]×TG (mmol/L).Citation19 In the formula above, the values 65 and 58 are the minimum WC for men and women, respectively. A growing number of studies have shown that LAP is a powerful marker for predicting fasting plasma glucose in adults. The study showed that LAP explained a greater variability in fasting plasma glucose (FPG) levels than WHtR and better predicted diabetes than BMI among young people.Citation18 The study from Kahn et alCitation19 showed that LAP was more effective in predicting diabetes than the waist-to-hip ratio (WHR) and WHtR. Zhang et alCitation20 developed children’s lipid accumulation product (CLAP) that was calculated using the formula of WC (cm) × TG (mmol/L) × AST (mm)/100, and reported that CLAP was significantly associated with metabolic syndrome (MS), and was better than BMI and WHtR for predicting MS.
Although the LAP is an important index for predicting diabetes in adults, however, LAP cannot be directly applied to show lipid accumulation in children and adolescents. CLAP is a novel indicator to show children’s lipid accumulation, however, it is not clear whether CLAP was associated with impaired fasting plasma glucose in children and adolescents. The purpose of this study was to explore a novel indicator of children’s lipid accumulation product (CLAP) associated with impaired fasting plasma glucose.
Materials and Methods
Subjects
In this study, 683 students, including 366 boys (53.6%) and 317 girls (46.4%), aged 8–15 years were effectively recruited from two nine-year-system schools using a stratified cluster sampling method. The present study was approved by the Medical Ethics Committee of Bengbu Medical College (2015 No.003), and conducted in accordance with the Declaration of Helsinki. The participants’ guardians signed informed consents before medical measurements.
Measurements of Anthropometric Indexes
The medical staff received standardized training to measure participants’ body height, weight, WC and AST. The participants were required to have an empty stomach, be barefoot, stand straight, and wear light clothes for the measurements. Body height was measured using a mechanical height gauge with an accuracy of 0.1 cm. Weight was measured using an electronic weight scale with an accuracy of 0.1 kg. The WC that was the perimeter of the WC at 1 cm above the belly button was measured using nylon tape with an accuracy of 0.1 cm. The abdominal skinfold thickness (AST), which was the skinfold thickness at the junction of the right collarbone midline and belly button horizontal line, was measured using a skinfold thickness gauge with an accuracy of 0.1 mm.
Calculation of Derivative Indicators
BMI = weight (kg)/[height (m)]2; WHtR = WC (cm)/height (cm); Children’s lipid accumulation product (CLAP) = WC (cm) × TG (mmol/L) × AST (mm)/100.Citation20
Survey of Behavioral Indexes
In this study, we surveyed the frequency of dietary behaviors, including the consumption of fresh vegetables, breakfast, fruits, eggs, milk, nuts, carbonated drinks, outside meals, Western fast food, fried foods, and high-energy snacks. Each dietary behavior score was assigned 0 points for never, 0.25 points for 1 time per month, 0.5 points for 2 times per month, 2 points for 1–3 times per week, 5 points for 4–6 times per week, and 7 points for 1 time per day. The total scores of healthy dietary behaviors (including fresh vegetables, breakfast, fruits, eggs, milk, and nuts) and risky dietary behaviors (including carbonated drinks, outside meals, Western fast food, fried foods, and high-energy snacks) were calculated.Citation21 According to the 75th percentile (P75) of healthy and risky dietary behaviors total scores, the children were divided into two groups, ≥ P75 and <P75, respectively. Physical activity was investigated through the Children’s Leisure Activity Study Survey (CLASS) questionnaire.Citation22 The moderate to vigorous physical activity time was divided into ≥60 min and <60 min grades.Citation23 The sedentary activity time was divided into ≥120 min and <120 min grades.Citation24
Measurement of Fasting Plasma Glucose and Triglyceride
Three milliliters of fasting venous blood was collected. Fasting plasma glucose and TG were detected using an automatic biochemical analyzer. A fasting plasma glucose value ≥5.6 mmol/L was defined as impaired fasting glucose (IFG).Citation25,Citation26
Statistical Analysis
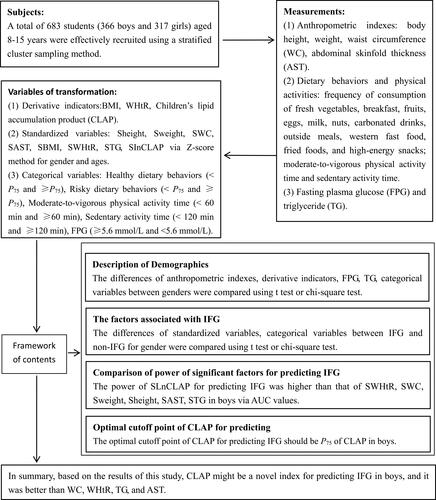
Statistical analysis was performed using SPSS23.0. The mean ± standard deviation and proportion (%) were used to describe the measurement and enumeration data, respectively. The logarithmic CLAP (LnCLAP), weight, height, BMI, WC, WHtR, AST and TG were standardized for sex and age using a normal deviation method. The t-test and chi-square test were used to compare the differences in the factors above between children with and without IFG. In addition, the receiver operating characteristic (ROC) was determined to analyze the predictive capabilities of the standardized variables above for IFG. A logistic regression model was used to explore optimal cutoff point of CLAP for predicting IFG. P< 0.05 was considered significant. The framework was showed in .
Figure 1 The framework figure of this study.
Results
Demographics
A total of 683 children, including 366 boys and 317 girls, aged 8–15 years were effectively recruited in this study. As shown in , the prevalence of impaired fasting glucose was 13.8%: 16.9% in boys and 10.1% in girls (P<0.05). The LnCLAP, TG and AST among girls were significantly higher than those among boys (P<0.05); however, the WHtR and fasting plasma glucose among girls were significantly lower than those among boys (P <0.05). The proportions of risky dietary behavior ≥P75, moderate to vigorous physical activity time ≥60 min and sedentary activity time <120 min among girls were significantly higher than those among boys (P<0.05).
Table 1 The Comparisons of Demographic Characteristics, Physical Activity Time and Dietary Behaviors Between Different Sexes (Mean±(m) or n (%))
The Factors Associated with IFG
As shown in , the Sheight, Sweight, SWC, SAST, SWHtR, STG and SLnCLAP among boys with IFG were significantly higher than those among boys without IFG, respectively (P<0.05). However, there were no significant differences in the above variables between girls with and without IFG.
Table 2 The Comparisons of Anthropometric Indexes, Dietary Behaviors and Physical Activity Time Between Children with and Without IFG (Mean±(m) or n (%))
The Comparison of Power for Predicting IFG Among Boys
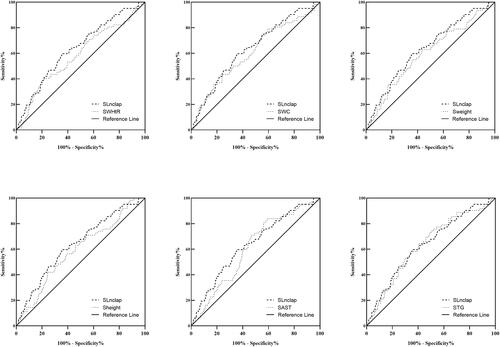
As shown in and , the receiver operator characteristic curve showed that the areas under the curve of SWHtR, SWC, Sweight, Sheight, SAST, STG and SLnCLAP for predicting IFG were 0.584 (95% CI 0.504–0.665), 0.606 (95% CI 0.526–0.686), 0.598 (95% CI 0.520–0.677), 0.590 (95% CI 0.513–0.667), 0.608 (95% CI 0.536–0.680), 0.635 (95% CI 0.560–0.709), and 0.637 (95% CI 0.562–0.712), respectively.
Table 3 The Areas Under ROC Curves of SlnCLAP, Sheight, Sweight, SWC, SWHtR, SAST, and STG for Predicting IFG Among Boys
Figure 2 The respective receiver operating characteristic curves of SWHtR, SWC, Sweight, Sheight, SAST, STG and SLnCLAP for predicting IFG.
Abbreviations: Sheight, Sweight, SWC, SAST, SWHtR, STG, and SLnCLAP are the standardized height, weight, WC, AST, WHtR, TG and LnCLAP by sex-age using the normal deviation method, respectively; IFG, impaired fasting glucose.
An Optimal Cutoff Point of CLAP for Predicting IFG
As shown in , the results showed that OR (95% CI) of P75, P85, P90, and P95 of CLAP for predicting IFG were 2.48 (1.40–4.42), 2.24 (1.19–4.20), 2.34 (1.14–4.78), and 2.45 (0.96–6.29), respectively. The optimal cutoff point of CLAP for predicting IFG should be P75 of CLAP. In addition, the prevalence of IFG was increased with P75, P85, P90, and P95 of CLAP.
Table 4 The Associations Between Anthropometric Indexes and IFG Using Logistic Regressions Among Boys
Discussion
With the prevalence of obesity or overweight, unhealthy eating habits and sedentary lifestyles, impaired fasting glucose among children and adolescents is increasingly common, and it is an important public health issue.Citation27,Citation28 The results of this study showed that the prevalence of IFG in children was 13.8%: 16.9% in boys and 10.1% in girls. Chahkandi et alCitation5 reported that the prevalence of IFG was 10.6% in boys and 4.8% in girls. A study from Wang et alCitation29 showed that the prevalence of impaired fasting glucose (IFG) was 2.80% in boys and 1.1% in girls. A study from Fu et alCitation30 showed that the prevalence of type 2 diabetes in boys aged 0–18 years was significantly higher than that in girls. A Danish study of fasting glucose in children and adolescents found that the impaired rate of fasting glucose was 11.2% in boys and 8.5% in girls. The impaired rate of fasting glucose increased with the increase in BMI (obesity, overweight and normal weight) in boys and girls, and fasting glucose may be associated with lipids.Citation31 Forbes et alCitation32 reported that the glycemic load (GL) in boys was higher than that in girls. One reason might be the differences in physical activity between sexes. In the present study, the rates of moderate to vigorous physical activity time ≥60 min and sedentary activity time <120 min among girls were significantly higher than those among boys, respectively. Anish et alCitation33 also found that women decreased their risk of diabetes by increasing their levels of physical activity. In addition, the present study showed that the AST and TG in girls were significantly higher than those in boys, and the WHtR in girls was significantly lower than that in boys. Comparing children in southern India, WHtR and TG in boys were significantly higher than those in girls, and AST in boys was significantly lower than that in girls.Citation34 In a study of Korean adolescents by Kim et al, TG in girls was significantly higher than that in boys.Citation35 Girls had a higher WHtR than boys compared with children in Amargosa.Citation36
In the present study, we found that the height, weight, WC, AST, WHtR, and TG among boys with IFG were significantly higher than those among boys without IFG; however, the differences in the above variables between IFG and non-IFG were not found in girls. Liu et alCitation37 reported that WC and TG were significantly related to fasting plasma glucose among adolescents. A study by West et al found a significant correlation between waist circumference and type 2 diabetes in boys.Citation38 Misra et al shown that a high prevalence of insulin resistance in postpubertal urban Asian Indian children was associated with abdominal adiposity.Citation39 Studies showed that WHtR was a better obesity index for predicting diabetes than BMI.Citation11,Citation40 In addition, we found that body height in boys with IFG was higher than that in boys without IFG. The study also showed that body height was related to diabetes.Citation40 However, the results of this study showed that BMI did not correlate with fasting plasma glucose, which was consistent with the findings from Sayeed et al.Citation40
The previous and present studies showed that WHtR, WC, TG and AST are significantly related to diabetes. The excess lipid fuel appeared eventually as an elevated circulating TG level or accumulation of fat. WHtR and WC were a better obesity index than BMI, but they were limited in indicating lipid accumulation in circulating blood.Citation41,Citation42 TG was limited in showing the accumulation of adipose tissue. AST is the skinfold thickness at the junction of naval horizontal line and the right clavicle midline, and it is used to show the accumulation point of abdominal fat. Based on waist circumference and fasting triglycerides, researchers developed LAP to identify diabetes in adults. The study showed that LAP was better than BMI in predicting glucose metabolism variables and far superior in identifying adults with diabetes.Citation19,Citation43 In the present study, WC, AST, and TG were used to calculate CLAP to show lipid accumulation in this study. The results showed that the AUC of CLAP (0.637) for predicting IFG in boys was higher than that of WC, AST, WHtR, and TG, indicating that CLAP had more power for predicting IFG compared with a single indicator. In addition, the optimal cutoff point of CLAP for predicting IFG was P75 of CLAP, with an OR (95% CI) value of 2.48 (1.40–4.42). Clearly, CLAP was a stronger risk factor for IFG compared with WC, WHtR, TG and AST. In summary, based on the results of this study, CLAP might be a novel index for predicting IFG in boys, and it was better than WC, WHtR, TG, and AST.
There were some limitations in this study. This study was a cross-sectional study, which limits inferring causality between CLAP and IFG. In addition, dietary behaviors and physical activity might be adopted before or after suffering from impaired fasting plasma glucose.
Acknowledgments
This project was supported by grants from the National Natural Science Foundation of China (No. 81502823), Sciences Foundation of Ministry of Education of China (No. 15YJAZH085), Outstanding Young Talent Key program of College and University in Anhui Province (No. gxyqZD2017063) and University Natural Science Foundation of Anhui Province (No. KJ2019A0298). The authors would like to thank the students who participated in the current study and thank Weige Jiang and Yu Liu for assisting in recruiting students.
Disclosure
Yongting Yuan and Hong Xie are co-first authors. All authors gave final approval of the submitted manuscript versions and declare no conflicts of interest in this work.
References
- Khorrami Z, Yarahmadi S, Etemad K, Khodakarim S, Kameli ME, Hazaveh ARM. Urban-rural differences in the prevalence of self-reported diabetes and its risk factors: the WHO STEPS Iranian noncommunicable disease risk factor surveillance in 2011. Iran J Med Sci. 2017;42(5):481–487.
- Group IDFDA. Update of mortality attributable to diabetes for the IDF Diabetes Atlas: estimates for the year 2013. Diabetes Res Clin Pract. 2015;109(3):461–465. doi:10.1016/j.diabres.2015.05.037
- Dabelea D, Mayer-Davis EJ, Saydah S, et al. Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA. 2014;311(17):1778–1786. doi:10.1001/jama.2014.3201
- Lee J, Gebremariam A, Wu E, LaRose J, Gurney J. Evaluation of nonfasting tests to screen for childhood and adolescent dysglycemia. Diabetes Care. 2011;34(12):2597–2602. doi:10.2337/dc11-0827
- Chahkandi T, Taheri F, Bijari B, Kazemi T, Namakin K, Zardast M. Prevalence of high normal FBS and prediabetes among adolescents in Birjand, East of Iran, 2012. J Educ Health Promot. 2015;4(1):68. doi:10.4103/2277-9531.162389
- Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
- Selph S, Dana T, Blazina I, Bougatsos C, Patel H, Chou R. Screening for type 2 diabetes mellitus: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2015;162(11):765–776. doi:10.7326/M14-2221
- Association AD. Standards of medical care in diabetes-2016 abridged for primary care providers. Clin Diabetes. 2016;34(1):3–21. doi:10.2337/diaclin.34.1.3
- Wang W, Wang K, Li T, et al. A discussion on utility and purposed value of obesity and abdomen obesity when body mass index, waist circumference, waist to hip ratio used as indexes predicting hypertension and hyper-blood glucose. Chin J Epidemiol. 2002;23(1):21–24.
- Yoon YS, Oh SW. Optimal waist circumference cutoff values for the diagnosis of abdominal obesity in Korean adults. Endocrinol Metab (Seoul). 2014;29(4):418–426. doi:10.3803/EnM.2014.29.4.418
- Weili Y, He B, Yao H, et al. Waist-to-height ratio is an accurate and easier index for evaluating obesity in children and adolescents. Obesity (Silver Spring). 2007;15(3):748–752. doi:10.1038/oby.2007.601
- Kahn HS. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison. BMC Cardiovasc Disord. 2005;5(1):26. doi:10.1186/1471-2261-5-26
- Hadaegh F, Shafiee G, Azizi F. Anthropometric predictors of incident type 2 diabetes mellitus in Iranian women. Ann Saudi Med. 2009;29(3):194–200. doi:10.5144/0256-4947.51788
- Jo A, Mainous AG 3rd. Informational value of percent body fat with body mass index for the risk of abnormal blood glucose: a nationally representative cross-sectional study. BMJ Open. 2018;8(4):e019200. doi:10.1136/bmjopen-2017-019200
- Ford ES, Maynard LM, Li C. Trends in mean waist circumference and abdominal obesity among US adults, 1999–2012. JAMA. 2014;312(11):1151–1153. doi:10.1001/jama.2014.8362
- Schulze MB, Heidemann C, Schienkiewitz A, Bergmann MM, Hoffmann K, Boeing H. Comparison of anthropometric characteristics in predicting the incidence of type 2 diabetes in the EPIC-Potsdam study. Diabetes Care. 2006;29(8):1921–1923. doi:10.2337/dc06-0895
- Ejike CECC. Lipid accumulation product and waist-to-height ratio are predictors of the metabolic syndrome in a Nigerian male geriatric population. J Rural Trop Public Health. 2011;10(1):101–105.
- Bozorgmanesh M, Hadaegh F, Azizi F. Diabetes prediction, lipid accumulation product, and adiposity measures; 6-year follow-up: tehran lipid and glucose study. Lipids Health Dis. 2010;9(1):45. doi:10.1186/1476-511X-9-45
- Kahn HS. The lipid accumulation product is better than BMI for identifying diabetes: a population-based comparison. Diabetes Care. 2006;29(1):151–153. doi:10.2337/diacare.29.01.06.dc05-1805
- Zhang YF, Hu JY, Li ZQ, et al. A novel indicator of lipid accumulation product associated with metabolic syndrome in Chinese children and adolescents. Diabetes Metab Syndr Obes. 2019;12:2075–2083. doi:10.2147/DMSO.S221786
- Yuexin Y, Huanmei Z. Dietary guidelines for Chinese residents. Acta Nutrimenta Sinica. 2016;38(3):209–217.
- Huang YJ, Wong SHS, Salmon J. Reliability and validity of the modified Chinese version of the Children’s Leisure Activities Study Survey (CLASS) questionnaire in assessing physical activity among Hong Kong children. Pediatr Exerc Sci. 2009;21(3):339–353. doi:10.1123/pes.21.3.339
- Australian Government Department of Health. Australian 24-hour movement guidelines for children (5-12 years) and young people (13-17 years): an integration of physical activity, sedentary behaviour, and sleep. EB/OL. Commonwealth of Australia. 2019. Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/ti-5-17years. Accessed May 11, 2020.
- Pérez SV, Novalbos-Ruiz JP, Rodríguez-Martín A, Martínez-Nieto JM, Lechuga-Sancho AM. Implications of family socioeconomic level on risk behaviors in child-youth obesity. Nutr Hosp. 2013;28(6):1951–1960.
- Siu AL, O’Malley PG. Screening for abnormal blood glucose and type 2 diabetes mellitus: U.S. Preventive services task force recommendation statement. Ann Intern Med. 2015;163(11):291–297. doi:10.7326/M15-0840
- Association AD. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2010;33(Suppl 1):S62–69. doi:10.2337/dc10-S062
- Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383(9911):69–82. doi:10.1016/S0140-6736(13)60591-7
- Aguiree F, Brown A, Cho NH, et al. IDF Diabetes Atlas. 6th ed. 2013.
- Wang Z, Zou Z, Wang H, et al. Prevalence and risk factors of impaired fasting glucose and diabetes among Chinese children and adolescents: a national observational study. Br J Nutr. 2018;120(7):813–819. doi:10.1017/S0007114518002040
- Fu JF, Liang L, Gong CX, et al. Status and trends of diabetes in Chinese children: analysis of data from 14 medical centers. World J Pediatr. 2013;9(2):127–134.
- Kloppenborg JT, Fonvig CE, Nielsen TRH, et al. Impaired fasting glucose and the metabolic profile in Danish children and adolescents with normal weight, overweight, or obesity. Pediatr Diabetes. 2018;19(3):356–365. doi:10.1111/pedi.12604
- Forbes LE, Storey KE, Fraser SN, et al. Dietary patterns associated with glycemic index and glycemic load among Alberta adolescents. Appl Physiol Nutr Metab. 2009;34(4):648–658. doi:10.1139/H09-051
- Anish TS, Shahulhameed S, Vijayakumar K, Joy TM, Sreelakshmi PR, Kuriakose A. Gender difference in blood pressure, blood sugar, and cholesterol in young adults with comparable routine physical exertion. J Family Med Prim Care. 2013;2(2):200–203. doi:10.4103/2249-4863.117424
- Vasan SK, Thomas N, Christopher S, Geethanjali FS, Paul TV, Sanjeevi CB. Anthropometric measurements for the prediction of the metabolic syndrome: a cross-sectional study on adolescents and young adults from southern india. Heart Asia. 2011;3(1):2–7. doi:10.1136/ha.2009.001735
- Kim S, So WY. Prevalence of metabolic syndrome among Korean adolescents according to the National Cholesterol Education Program, Adult Treatment Panel III and International Diabetes Federation. Nutrients. 2016;8(10):588. doi:10.3390/nu8100588
- Quadros TMB, Gordia AP, Andaki ACR, Mendes EL, Mota J, Silva LR. High blood pressure screening in children and adolescents from Amargosa, Bahia: usefulness of anthropometric indices of obesity. Rev Bras Epidemiol. 2019;22:e190017. doi:10.1590/1980-549720190017
- Liu J, Joshi D, Sempos CT. Non-high-density-lipoprotein cholesterol and cardiovascular risk factors among adolescents with and without impaired fasting glucose. Appl Physiol Nutr Metab. 2009;34(2):136–142. doi:10.1139/H08-149
- West NA, Hamman RF, Mayer-Davis EJ, et al. Cardiovascular risk factors among youth with and without type 2 diabetes: differences and possible mechanisms. Diabetes Care. 2009;32(1):175–180. doi:10.2337/dc08-1442
- Misra A, Vikram NK, Arya S, et al. High prevalence of insulin resistance in postpubertal Asian Indian children is associated with adverse truncal body fat patterning, abdominal adiposity and excess body fat. Int J Obes Relat Metab Disord. 2004;28(10):1217–1226. doi:10.1038/sj.ijo.0802704
- Sayeed MA, Mahtab H, Latif ZA, et al. Waist-to-height ratio is a better obesity index than body mass index and waist-to-hip ratio for predicting diabetes, hypertension and lipidemia. Bangladesh Med Res Counc Bull. 2003;29(1):1–10.
- McCarthy HD, Ellis SM, Cole TJ. Central overweight and obesity in British youth aged 11–16 years: cross sectional surveys of waist circumference. BMJ. 2003;326(7390):624. doi:10.1136/bmj.326.7390.624
- Weber DR, Leonard MB, Shults J, Zemel BS. A comparison of fat and lean body mass index to BMI for the identification of metabolic syndrome in children and adolescents. J Clin Endocrinol Metab. 2014;99(9):3208–3216. doi:10.1210/jc.2014-1684
- Cao BY, Mi J, Gong CX, et al. Blood glucose profile in children and adolescents in Beijing area. Zhonghua Er Ke Za Zhi. 2008;46(4):297–300.