
Abstract
Background
Elevation and health-related lifestyles have been associated with the development of metabolic syndrome (MetS). However, such associations have not been investigated extensively in a global context. The present study aimed to determine the associations among elevation of residence, health-related lifestyles, and the risk of MetS in an Ecuadorian adult population.
Subjects and Methods
This cross-sectional study was conducted utilizing secondary data from the 2012 Ecuador National Health and Nutrition Survey (ENSANUT-ECU). A total of 6024 adults (1964 men and 4060 women) 20 to 60 years old were included in the study. Elevation was obtained by georeferencing techniques and categorized into low (0–2000 masl) and high (>2001 masl). Dietary intake was measured using a 24-hour recall and health-related lifestyle via risk and physical activity standardized questionnaire. MetS was defined on the basis of the National Cholesterol Education Program Adult Treatment Panel III and the Latin American Diabetes Association criteria. Multiple logistic regression analyses were used to examine whether elevation of residence and health-related lifestyles can increase the risk of MetS.
Results
Residing at low elevation increased prevalence of MetS in men (1.37; 95% CI, 1.05–1.76) and elevated fasting glucose in both men (1.80; 95% CI, 1.32–2.46) and women (1.55; 95% CI, 1.24–1.93) after adjusting for confounders. Additionally, a lack of physical activity was identified as an important factor that raises the risk of increased waist circumference in both men (2.05; 95% CI, 1.22–3.45) and women (1.38; 95% CI, 1.05–1.83) living at low elevation.
Conclusion
Our findings suggest that low elevation of residence and physical inactivity are associated with a higher prevalence of MetS in Ecuadorian adults.
Introduction
Metabolic syndrome (MetS) is a multidimensional, progressive, and complex disorder characterized by the sum of elevated fasting glucose, hypertension, elevated serum triglycerides and low serum high-density lipoprotein (HDL) levels, and abdominal obesity.Citation1 The worldwide prevalence of MetS is estimated to be between 10% and 84% depending on the age, gender, and ethnicity of the population.Citation2 Additionally, 20% of adults in the Western world were found to have MetS.Citation3 Latin America exhibits a high prevalence of abdominal obesity and MetS, similar to or even higher than developed countries.Citation4 MetS culminates in adverse outcomes, including cardiovascular disease (CVD) and type 2 diabetes mellitus (DM2).Citation5 The specific causes that trigger MetS are still unknown, although genetics, lifestyle, and environmental factors have been identified.Citation6,Citation7 In Ecuador, Ecuador National Health and Nutrition Survey (ENSANUT-ECU) presented data on cardiometabolic risk factors nationwide for 2012, reporting a 27% prevalence of MetS nationally, which was higher in women than in men (29.2% and 25.2%, respectively).Citation8 For 2013, DM2 was the first cause of mortality, corresponding to 4695 deaths (7.44% of the annual total).Citation9
Several biological and behavioral factors, including age (ie, >40 yr), sex (female), smoking, unhealthy dietary habits, and sedentary behaviors have been recognized to contribute to the development of MetS. Moreover, the environment has been suggested to potentially influence the development of metabolic diseases.Citation10,Citation11 All of these factors have contributed to the design of health policies in urban environments.Citation12 As such, elevation, defined as the distance above sea level, has been proposed to increase pulmonary and cardiovascular functions.Citation13,Citation14 Many studies have reported that populations living at high elevation have lower serum low-density lipoprotein (LDL) cholesterol, higher HDL cholesterol, and lower fasting glucose levels as well as reduced obesity rates.Citation11,Citation15 It is also reported to increase glucose uptake and its tolerance, which reduces blood glucose levels.Citation16–Citation18 Furthermore, living at high elevation is associated with severe hypoxia and a reduction in peripheral oxygen saturation leading to a decrease in insulin sensitivity, whereas mild hypoxia may improve insulin sensitivity.Citation17,Citation19,Citation20 Some studies have described an inverse association between elevation and lower obesity prevalence and incidence,Citation21–Citation24 as well as lower diabetesCitation3,Citation25 and hypertension proportions.Citation14,Citation26 One Spanish study utilizing a university student cohort found that living at a high elevation was associated with a lower risk of MetS than living at a low elevation after a median follow-up period of 10 years.Citation27 Another Ecuadorian study also reported that residence at high elevation (2758–2787 meters above sea level (masl)) was associated with a lower prevalence of MetS, hypercholesterolemia, and hyperglycemia than residence at sea level (4–6 masl).Citation28
However, the association between elevation of residence and MetS development has not been extensively investigated. Furthermore, socioeconomic characteristics, dietary patterns, smoking, alcohol consumption, and physical activity patterns may also explain these associations.Citation2,Citation27 Therefore, effects of elevation of residence and lifestyle on populations living in the highest regions of the world should be further investigated. In this context, we examined the associations among elevation of residence, health-related lifestyles, and prevalence of MetS in the Ecuadorian population using national survey data from the Ecuadorian National Health and Nutrition Survey (ENSANUT-ECU).
Subjects and Methods
Study Design and Subjects
This study used data from the 2012 ENSANUT-ECU, which is a cross-sectional study with a complex, multistage, probability sampling design. The survey was conducted by the Ministry of Public Health of Ecuador (MSP). Detailed explanations of the ENSANUT-ECU are available elsewhere.Citation8
The initial samples were 20 years old or older with complete 24-hour dietary recall, anthropometric data, and biochemical variables related to metabolic syndrome; the initial data consisted of 11,044 participants. Among the eligible participants, we excluded those with missing physical activity information (n = 4166, rural residents), incomplete risk factor data (n = 493), and participants taking medication for hypertension (n = 361). Therefore, the final sample consisted of 6024 Ecuadorians (1964 men and 4060 women) over 20 years old. The study was approved by the MSP and the Institutional Review Board of Seoul National University (code: SNU 19–04-003). Written informed consent was obtained from all participants.
Measurement and Definition of Metabolic Syndrome
Anthropometric data including height, weight, and waist circumference were measured at people’s houses by trained health technicians using calibrated equipment. Body mass index (BMI) was calculated from weight and height data (kg/m2). Blood pressure was measured at three consecutive times according to standardized procedures of anthropometry and a determination of blood pressure manual;Citation29 the mean of the readings was used in this study. For measurement of levels of fasting blood glucose, serum total cholesterol, HDL cholesterol, and triglycerides, blood samples were collected from participants who fasted for at least 8 hours and stored at −80°C until analysis. An enzymatic colorimetric method was utilized to measure the concentrations of glucose, total cholesterol, HDL-C, and triglycerides using an automated auto-analyzer (Modular Evo-800, Roche Diagnostics, Mannheim, Germany). Details of laboratory procedures have been described in the ENSANUT-ECU 2012 report.Citation29 LDL-cholesterol was calculated according to Friedewald’s formula: [LDL-cholesterol] = [total cholesterol] – [triglycerides/5]. However, this calculation was valid when the triglycerides level was ≤400 mg/dL.Citation30 The definition of metabolic syndrome was based on the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) criteria for Latin America and the Metabolic Syndrome Diagnosis Criteria established by the Latin America Association of Diabetes. MetS was diagnosed when three or more of the following components existed: waist circumference ≥94 cm for men and ≥88 cm for women, systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg, HDL cholesterol <40 mg/dL for men and <50 mg/dL for women, triglycerides ≥150 mg/dL, and fasting blood glucose ≥100 mg/dL.
Measurement of Sociodemographic Variables and Health-Related Lifestyles
General- and socio-demographic variables including age, ethnicity, family economic status, and education level were collected. Data for ethnicity were obtained from the housing information standardized questionnaire; according to ENSANUT-ECU, the five main ethnic groups were categorized as mestizo and the rest of population (indigenous, montubio, afro-descendent and white). For family economic status, the population was divided into quintiles based on the Wealth Index Q1 (poor), Q2, Q3 (intermediate), Q4 and Q5 (rich). Education level was categorized into primary school (≤7th grade), secondary school (>8th grade <12th grade), and college or higher (college or associates degree or college graduate or above). Additionally, the questionnaire included the elevation of residence, which was obtained through georeferencing methods; elevation was classified as high elevation if the participant’s residence was located over 2001 masl and low elevation if the participant’s residence was under 2000 masl.Citation31,Citation32
Health-related lifestyles included current alcohol consumption, current smoking, and physical activity; data were obtained using risks and physical activity standardized questionnaires.Citation33,Citation34 Current alcohol consumption was defined by the number of alcoholic beverages consumed per day in the past 30 days and categorized as “Yes” or “No” according to the United States National Survey on Drug Use and Health (NSDUH). Current smoking status was defined as current tobacco consumption (“Yes” or “No”) for those who had smoked in the last 30 days according to the WHO-Ecuador, 2007 and based on the NSDUH.Citation33
Physical activity was defined according to the U.S. Department of Health and Human Services as “Yes” for those who participated in vigorous-intensity activities for at least 75 min, moderate-intensity activity for at least 150 min, or an equivalent combination of moderate and vigorous-intensity activity during the last 7 days and “No” for activities performed in less than 75 min in the past seven days.Citation34
Assessment of Dietary Intake
Dietary intake was measured by a single 24-hour dietary recall method administered by a trained technician at each participant’s residence. The recall data included all kinds of food and beverages consumed by subjects within a 24-hour period. Energy intake was estimated with dietary intakes and the food composition table in the Ecuadorian Food Dietary Guideline (GABA).Citation35 To evaluate the adequacy of energy intake, percentage (%) of estimated energy requirements (EER), based on the age-, sex-, and physical activity level-specific equations published in Dietary Reference Intakes, was calculated.Citation36,Citation37
Statistical Analyses
All statistical analyses were performed using SAS version 9.4 software.Citation38 The complex sampling design parameters including strata, cluster, and weight were applied to PROC SURVEY procedures. All p-values were two-sided (α=0.05).
All analyses were stratified by sex and geographical elevation. All variables are expressed as means ± standard error for continuous variables and as percentages (%) for categorical variables. For continuous variables, p-values were obtained from t-tests and χ2-tests for categorical variables to test the difference between sex and elevation; if more than 50% of the cells had expected counts less than 5, the T Fisher Exact Test was used.
Geographical elevation was categorized into two groups, including low elevation (0–2000 masl) and high elevation (above 2001 masl). Multiple logistic regression analysis was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for MetS across the elevation groups. In the multiple logistic regression model, the confounders of ethnicity, socio-economic status, education level, BMI (except for the model of waist circumference), physical activity, current alcohol consumption, current smoking, and total energy intake were adjusted when comparing both groups.
Results
Six thousand twenty-four participants (4060 females and 1964 males) were included in the study. The general characteristics of the study participants by sex and elevation are shown in . The mean age of the Ecuadorian participants was 34.7 ± 0.46 (SE) years old at low elevation and 34.4 ± 0.54 at high elevation for men and 35.1 ± 0.35 years old at low elevation and 35.3 ± 0.35- at high elevation for women. Ethnicity, family economic status, physical activity, and current smoking of study subjects were significantly different between living at high and low elevation in both sexes (p < 0.05). However, education level and alcohol consumption were significantly different between high and low elevation in men only (p = 0.0151, p = 0.0387, respectively).
Table 1 Demographic and Health-Related Lifestyle Characteristics of Study Subjects According to Their Elevation of Residence
shows the anthropometric and biochemical measurements of the MetS components and energy intake of the study participants. While blood pressure, total cholesterol level, triglyceride level, and energy intake were higher in men than women, BMI and EER (%) were higher in women than in men. A higher BMI was observed in both women and men living at low elevation than that in residents living at high elevation; however, a significant difference was only observed in women living at low elevation (p = 0.044). Fasting glucose levels of both men and women living at low elevation were significantly higher than those of residents living at high elevation (p = 0.0002 for men, p < 0.0001 for women). Both energy intake and EER (%) increased significantly as elevation decreased for both sexes (p < 0.0001).
Table 2 Anthropometric and Biochemical Measurements of MetS and Macronutrient Intake Among Study Subjects According to Their Elevation of Residence
The prevalence and ORs for MetS in Ecuadorian adults according to elevation are shown in . Living at low elevation significantly increased ORs of MetS in men (1.37; 95% CI, 1.05–1.76) and elevated fasting glucose levels in both men (1.80; 95% CI, 1.32–2.46) and women (OR=1.55; 95% CI,1.24–1.93) after adjusting for ethnicity, family economic status, education level, BMI, physical activity, current alcohol and smoking status, and total energy intake. We further analyzed the data according to quartiles of residential elevation, and found that ORs of MetS in men and ORs in elevated fasting glucose levels in both sexes were negatively elevation-dependent (Data not shown; ptrend < 0.0001 for all).
Table 3 Prevalence and Odds Ratio for MetS Among Study Subjects According to Their Elevation of Residence
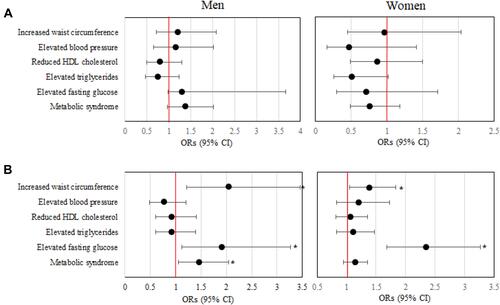
As shown in Supplementary Table 1, health-related lifestyle factors including current alcohol consumption, current smoking status, and physical activity individually increased ORs of MetS and/or elevated fasting glucose levels in residents at lower elevation over that in those living at high elevation; these are concordant to results shown in . However, interestingly, non-smoking or non-alcohol drinking women living at low elevation showed higher ORs of increased waist circumference, and men with low energy intake and living at low elevation had higher ORs of elevated fasting glucose levels. Furthermore, a lack of physical activity was also significantly associated with elevated fasting glucose levels in men (2.05; 95% CI,1.22–3.45) and women (1.38; 95% CI,1.05–1.83) living at low elevation, in addition to MetS and elevated fasting glucose levels (). The obtained data suggest that low elevation of residence and physical inactivity may play important roles in the development of MetS.
Figure 1 Odds ratios for MetS among low elevation residents according to physical activity. (A) Physically active and (B) physically inactive subjects. ORs were calculated based on high elevation residents (reference). All values were obtained from a multivariable logistic regression model applying appropriate sampling weight after adjusting for ethnicity, family economic status, education level, BMI (except for the model of waist circumference), current alcohol consumption, current smoking and total energy intake. *p < 0.05.
Discussion
Nationally representative data from the ENSANUT-ECU were utilized to determine whether living at low elevation (0–2000 masl) is associated with development of MetS in adult men and women. In our study, elevation over 2000 masl is classified as high elevation since it has shown to be associated with physiological changes at rest and marked changes in exercise. Opposed to it, living at low elevation (1–2000 masl) has no physiological effects at rest and presents a decrease in physical performance.Citation31,Citation32 Our study showed a higher prevalence of MetS in men and elevated fasting glucose levels in both men and women living at a lower elevation than in those living at a higher elevation. To our knowledge, this is the first study to report an association between residing elevation and prevalence of MetS utilizing a large number of Ecuadorian adults.
Two studies using a university student cohort reported that young adults living at high elevation show a lower prevalence of MetS.Citation27,Citation28 Several studies have also shown an inverse association between high elevation and MetS development. One study including 285,196 adults from the United States showed a lower prevalence of diabetes in men living above 1500 masl.Citation39 A Peruvian study also reported lower serum triglycerides and blood pressure in people living at higher elevation, while no significant differences in prevalence of MetS were observed between those living at sea level and those living at a higher elevation.Citation40 Another study performed in an Andean population reported a lower waist circumference at a higher elevation; an adjusted inverse association between geographical elevation and obesity that varied by sex was also found.Citation21 Furthermore, lower fasting glucose and better glucose tolerance were associated with a high elevation,Citation33,Citation41–Citation43 and lower prevalenceCitation22,Citation44 and incidenceCitation23,Citation24,Citation45 of overweight or obesity were also found in residents at high elevation.
Some causes of mortality were also associated with elevation; specifically, living at high elevation was associated with a lower mortality rate from coronary heart disease and ischemia, whereas a higher mortality from chronic obstructive pulmonary disease was observed.Citation14 People living at high elevation, above 2500 masl, display a fall in arterial oxygen saturation and present physiological adaptations to this environmental pressure.Citation16,Citation31 These two responses produce an increase in hemoglobin concentrations, enlarged lung volume and increased ventilatory response.Citation15,Citation33 In this case, the highest regions of the world demonstrate the biological human adaptation to low oxygen concentrations (hypoxia), including the Ethiopian Siemen Mountains, the Tibetan Himalayan valleys, and the Andean Altiplano in South America.Citation13 Genetic and physiological adaptations, principally to hypoxia, that affect glucose metabolism and trigger appetite suppression and reduced caloric consumptionCitation34 might explain the inverse association between elevation, diabetes, and cardiovascular diseases.
Furthermore, at sea level, the partial pressure of oxygen is approximately 160 mmHg, which represents 21% oxygen respired compared to 15% O2 at ~3000 masl at high‐elevation. This fact leads to a condition of moderate hypoxia for ten sequential nights, which increases whole‐body insulin sensitivity in obese men.Citation46,Citation47 Even though evidence suggests that exposure to lower levels of oxygen may enhance body metabolic homeostasis, intervention studies in humans are needed for further research.
In this study, we analyzed sex and elevation separately and found that men had a higher prevalence of MetS when living at low elevation than at high elevation; currently available data suggest that sex-specific pathophysiological differences in MetS may be associated with different effects of sex hormones on adipose tissue, genetic factors between men and women, or a combination of all.Citation48–Citation50 Diagnostic criteria for MetS vary for the cutoff points and definition of its components in a gender-specific manner. Glucose and lipid metabolism are directly modulated by estrogen and testosterone, with a lack of estrogen or a relative increase in testosterone inducing insulin resistance and an increase in the lipid profile.
Health-related lifestyle factors, physical activity patterns in particular, are inversely associated with development of MetS.Citation51 Our results are also consistent with those from other studies. Moderate exercise has been shown to have a positive impact on lipid profile (cholesterol and triglycerides), while a lack of physical activity has been associated with increased abdominal circumference.Citation51,Citation52 In addition, physical inactivity has been associated with a higher risk of type 2 diabetes, regardless of age, sex, ethnicity, or BMI.Citation53 Evidence shows that the prevalence of MetS, diabetes and dyslipidemias is higher in obese, overweight, and physically inactive individuals, and physical inactivity is independently related to an increased risk of each of these diseases.Citation54 Although an extensive literature exists on physical-related health benefits, measuring physical activity at a population level is difficult because of the existence of a variety of measurement methods. In the present study, the participants’ oxygen consumption levels were not available, which may have resulted in an over-estimation of physical activity level for some individuals from a physiological perspective; thus, this should be considered when interpreting our result and merits caution.
Other health-related lifestyle factors, including alcohol consumption and current smoking, were related to MetS and/or elevated fasting glucose levels in men living at a low elevation. These findings agree with previous studies where heavy alcohol consumption was associated with increased risk of MetS, while very light alcohol consumption had an inverse association.Citation55 Another study showed that several alcohol-drinking patterns were positively correlated with the prevalence of MetS in men.Citation56 Moreover, our study showed that men in the “No” current alcohol consumption group had a lower risk of elevated fasting glucose levels in comparison to the “Yes” group; these findings agree with some studies where drinking alcohol showed a less favorable alteration on glucose metabolism, blood pressure, hypertriglyceridemia, and central obesity.Citation57,Citation58 In addition, adult smokers have lower levels of plasma apolipoprotein A1, the main protein component of HDL, which is related to an increased risk of MetS and DM2.Citation59–Citation62 One hypothesis is that nicotine itself may lead to fat accumulation, attributable to its effect on insulin resistance.Citation63,Citation64 A meta-analysis of 13 prospective studies using long-term observation of the development of MetS revealed smoking to be a contributing factor for MetS depending on the amount of nicotine accumulation in the body,Citation65 which may explain our finding of a high risk of MetS in men. Interestingly, our data also showed that non-smoking or non-alcohol drinking women living at low elevation had a higher risk of increased waist circumference. Thus, elevation may influence waist circumference or obesity more than health-related lifestyles in women; however, further investigations are needed to confirm these associations.
Self-reported energy intake significantly differed by elevation in men and women (p < 0.0001); this inverse-adjusted association suggested a regulatory role for appetite in contracting MetS. However, our results are independent of energy intake, which was used as a confounder in the multiple logistic regression analysis. Previous studies reported that exposure to hypoxia under resting conditions increases energy expenditure and lipid metabolism and reduces appetite and food intake.Citation6 Acute exposure to hypoxia tends to stimulate the neuroendocrine system, triggering a strong endocrine response that improves oxygen delivery via cardiorespiratory and hemopoietic adaptations.Citation33 In this context, leptin and norepinephrine could increase sympathetic nerve activity, causing changes in energy expenditure and food intake at high elevation.Citation67 It is notable that high EER was associated with elevated fasting glucose in women at low elevation; in contrast, men with a low EER showed increased fasting glucose. This result suggests that EER influences insulin sensitivity. Several physiologic mechanisms may help to explain this finding.Citation68,Citation69 Our study has several limitations. Among initial participants (n = 11,044), physical activity data from a rural population were not collected for the ENSANUT-ECU; thus, we analyzed only 6024 participants residing in urban areas after excluding rural residents (n =4166) and others (n = 854). Consequently, we cannot exclude the possibility of residual bias, and our results should be interpreted with caution. One should consider reverse causality, attributable to a cross-sectional study design. Also, energy intake data from a single 24-hour recall method, which were used in this study due to data availability, could not represent individual’s usual energy intake. In addition, both the elevation exposure and the outcome are categorized as low or high and presence or absence, respectively; however, continuous variables would give more information regarding dose–response association. Despite these limitations, our study has some strengths. This is the first study on the association of residential elevation with MetS, which includes a large number of Ecuadorians selected from a nationally representative population. The analyses are adjusted for socio-economic and lifestyle factors to avoid any potential bias. Additionally, all data were collected by trained technicians, reducing data inaccuracy and preventing recall and response biases.
Conclusions
In conclusion, living at low elevation (0–2000 masl) is associated with a higher prevalence of MetS in men and an elevated fasting glucose level in both sexes. Additionally, a lack of physical activity was identified as an important factor that increases ORs of increased waist circumference in both men and women living at low elevation. Our findings suggest that low elevation of residence and physical inactivity may play important roles in development of MetS in Ecuadorian adults.
Disclosure
All authors declare no conflict of interest. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- IDF. The IDF consensus worldwide definition of the metabolic syndrome. Int Diab Federation. 2006;4–7.
- Kaur JA. Comprehensive review on metabolic syndrome. Cardiol Res Pract. 2014;2014:943162. doi:10.1155/2014/943162
- Pal S, Ellis V. The chronic effects of whey proteins on blood pressure, vascular function, and inflammatory markers in overweight individuals. Obesity. 2010;18:1354–1359. doi:10.1038/oby.2009.397
- Ferrari GLM, Kovalskys I, Fisberg M. et al. Socio-demographic patterning of objectively measured physical activity and sedentary behaviours in eight Latin American countries: findings from the ELANS study. Eur J Sport Sci;2019. 1–26. doi:10.1080/17461391.2019.1678671
- Kassi E, Pervanidou P, Kaltsas G, G C. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9:48. doi:10.1186/1741-7015-9-48
- Gosadi IM. Assessment of the environmental and genetic factors influencing prevalence of metabolic syndrome in Saudi Arabia. Saudi Med J. 2016;37(1):12–20. doi:10.15537/smj.2016.1.12675
- Werneck AO, Baldew SS, Miranda JJ, et al. The South American Physical Activity and Sedentary Behavior Network (SAPASEN). Glob Health Promot. 2019;1757975919859577.
- Freire WB, Belmont P, Lopez-Cevallos DF, Waters WF. Ecuador’s national health and nutrition survey: objectives, design, and methods. Ann Epidemiol. 2015;25(11):877–878. doi:10.1016/j.annepidem.2015.08.009
- National Institute of Statistics and Censuses. Yearbook of Vital Statistics Births and Deaths 2013. Quito, Ecuador: National Institute of Statistics and Censuses; 2013. https://www.ecuadorencifras.gob.ec/documentos/webinec/Poblacion_y_Demografia/Nacimientos_Defunciones/Publicaciones/Anuario_Nacimientos_y_Defunciones_2013.pdf. Accessed Aug 05, 2019.
- Burtscher M. Effects of living at higher altitudes on mortality: a narrative review. Aging Dis. 2014;5(4):274–280. doi:10.14336/AD.2014.0500274
- Burtscher M, Gatterer H, Burtscher J. Does growing up at high altitude pose a risk factor for type 2 diabetes? AIMS Public Health. 2019;6(1):96–98. doi:10.3934/publichealth.2019.1.96
- Pico SM, Bergonzoli G, Contreras A. Risk factors associated with the metabolic syndrome in Cali, Colombia (2013): a case-control study. Biomédica. 2019;39:46–54. doi:10.7705/biomedica.v39i1.3935
- Julian CG, Moore LG. Human genetic adaptation to high altitude: evidence from the andes. Genes. 2019;10:2. doi:10.3390/genes10020150
- Anderson JD, Honigman B. The effect of altitude‐induced hypoxia on heart disease: do acute, intermittent, and chronic exposures provide cardioprotection? High Alt Med Biol. 2011;12(1):45‐55. doi:10.1089/ham.2010.1021
- Hirschler V. Cardiometabolic risk factors in native populations living at high altitudes. Int J Clin Pract. 2016;70(2):113–118. doi:10.1111/ijcp.12756
- Lempesis IG, van Meijel RLJ, Manolopoulos KN, Goossens GH. Oxygenation of adipose tissue: a human perspective. Acta Physiol. 2019;e13298.
- Woolcott OO, Ader M, Bergman RN. Glucose homeostasis during short-term and prolonged exposure to high altitudes. Endocr Rev. 2015;36:149–173. doi:10.1210/er.2014-1063
- Horscroft JA, Kotwica AO, Laner V, et al. Metabolic basis to Sherpa altitude adaptation. Proc Natl Acad Sci USA. 2017;114:6382–6387. doi:10.1073/pnas.1700527114
- Louis M, Punjabi NM. Effects of acute intermittent hypoxia on glucose metabolism in awake healthy volunteers. J Appl Physiol. 2009;106:1538–1544. doi:10.1152/japplphysiol.91523.2008
- Oltmanns KM, Gehring H, Rudolf S, et al. Hypoxia causes glucose intolerance in humans. Am J Respir Crit Care Med. 2004;169:1231–1237. doi:10.1164/rccm.200308-1200OC
- Woolcott OO, Gutierrez C, Castillo OA, Elashoff RM, Stefanovski D, Bergman RN. Inverse association between altitude and obesity: a prevalence study among andean and low-altitude adult individuals of Peru. Obesity. 2016;24(4):929–937. doi:10.1002/oby.21401
- Voss JD, Masuoka P, Webber BJ, Scher AI, Atkinson RL. Association of elevation, urbanization and ambient temperature with obesity prevalence in the United States. Int J Obes. 2013;37(10):1407–1412. doi:10.1038/ijo.2013.5
- Voss JD, Allison DB, Webber BJ, Otto JL, Clark LL. Lower obesity rate during residence at high altitude among a military population with frequent migration: a quasi-experimental model for investigating spatial causation. PLoS One. 2014;9(4):e93493. doi:10.1371/journal.pone.0093493
- Hoke MK, Leatherman TL. Secular trends in growth in the high-altitude district of Nunoa, Peru 1964–2015. Am J Phys Anthropol. 2019;168(1):200–208. doi:10.1002/ajpa.23736
- Santos JL, Pérez‐Bravo F, Carrasco E, Calvillán M, Albala C. Low prevalence of type 2 diabetes despite a high average body mass index in the Aymara natives from Chile. Nutrition. 2001;17(4):305‐9. doi:10.1016/S0899-9007(00)00551-7
- Norboo T, Stobdan T, Tsering N, et al. Prevalence of hypertension at high altitude: cross-sectional survey in Ladakh, Northern India 2007–2011. BMJ Open. 2015;5(4):e007026. doi:10.1136/bmjopen-2014-007026
- Lopez-Pascual A, Bes-Rastrollo M, Sayon-Orea C, et al. Living at a geographically higher elevation is associated with lower risk of metabolic syndrome: prospective analysis of the SUN Cohort. Front Physiol. 2016;7:658. doi:10.3389/fphys.2016.00658
- Lopez-Pascual A, Arevalo J, Martinez JA, Gonzalez-Muniesa P. Inverse association between metabolic syndrome and altitude: a cross-sectional study in an adult population of Ecuador. Front Endocrinol. 2018;9:658. doi:10.3389/fendo.2018.00658
- Freire WB, Ramírez-Luzuriaga MJ, Belmont P, et al. Encuesta Nacional de Salud y Nutrición de la población ecuatoriana de cero a 59 años. ENSANUT-ECU. 2012;2014:1.
- Eblen-Zajjur A, Eblen-Zajjur M. Cálculo de la concentración de colesterol de la lipoproteína de baja densidad: análisis de regresión versus fórmula de Friedewald. Revista médica de Chile. 2001;129:1263–1270. doi:10.4067/S0034-98872001001100005
- Terrados-Cepeda N. Fisiología del ejercicio en altitud. In: Gonzales-Gallego J, editor. Fisiología de la actividad física y del deporte. Spain: Inter-americana; 1992:287–298.
- McLean B, Buttifant D, Gore C, White K, Liess C, Kemp J. Physiological and performance responses to a preseason altitude-training camp in elite team-sport athletes. Int J Sports Physiol Performance. 2013;8(4):391–399. doi:10.1123/ijspp.8.4.391
- Ryan H, Trosclair A, Gfroerer J. Adult current smoking: differences in definitions and prevalence estimates–NHIS and NSDUH, 2008. J Environ Public Health. 2012;2012:918368. doi:10.1155/2012/918368
- US Department of Health and Human Services. Physical Activity Guidelines for Americans. Hyattsville, MD: US Department of Health and Human Services; 2008; 2008. Available at: http://www.health.gov/paguidelines. Accessed June 9, 2020.
- Ministerio de Salud Pública del Ecuador y Organización de las Naciones Unidas para la Alimentación y la Agricultura. Documento Técnico de las Guías Alimentarias Basadas en Alimentos (GABA) del Ecuador. GABA-ECU. 2018.
- Trumbo P, Schlicker S, Yates AA, Poos M. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J Am Diet Assoc. 2002;102(11):1621–1630. doi:10.1016/S0002-8223(02)90346-9
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. Washington, DC: National Academy Press; 2005.
- SAS Institute Inc. Version 9.4. Cary, NC: SAS Institute Inc; 2014.
- Lindgärde F, Ercilla MB, Correa LR, Ahrén B. Body adiposity, insulin, and leptin in subgroups of Peruvian Amerindians. High Alt Med Biol. 2004;5:27–31. doi:10.1089/152702904322963663
- Woolcott OO, Castillo OA, Gutierrez C, Elashoff RM, Stefanovski D, Bergman RN. Inverse association between diabetes and altitude: a cross-sectional study in the adult population of the United States. Obesity. 2014;22(9):2080–2090. doi:10.1002/oby.20800
- Baracco R, Mohanna S, Seclen S. A comparison of the prevalence of metabolic syndrome and its components in high and low altitude populations in Peru. Metab Syndr Relat Disord. 2007;5(1):55–62. doi:10.1089/met.2006.0019
- Castillo O, Woolcott OO, Gonzales E, et al. Residents at high altitude show a lower glucose. High Alt Med Biol. 2007;8:307–311. doi:10.1089/ham.2007.8407
- Hill NE, Deighton K, Matu J, et al. Continuous glucose monitoring at high altitude-effects on glucose homeostasis. Med Sci Sports Exerc. 2018;50(8):1679–1686. doi:10.1249/MSS.0000000000001624
- Sherpa LY, Deji SH, Chongsuvivatwong V, Thelle DS, Bjertness E. Obesity in Tibetans aged 30–70 living at different altitudes under the north and south faces of Mt. Everest Int J Environ Res Public Health. 2010;7(4):1670–1680. doi:10.3390/ijerph7041670
- Díaz-Gutiérrez J, Martínez-González MÁ, Pons IJJ, González-Muniesa P, Martínez JA, Bes-Rastrollo M. Living at higher altitude and incidence of overweight/obesity: prospective analysis of the sun cohort. PLoS One. 11(11):e0164483. doi:10.1371/journal.pone.0164483. 2016
- Vogel M, Blaak E, Goossens G. Moderate hypoxia exposure: a novel strategy to improve glucose metabolism in humans. EMJ Diabet. 2015;3(1):73‐79.
- Lecoultre V, Peterson CM, Covington JD, et al. Ten nights of moderate hypoxia improves insulin sensitivity in obese humans. Diabetes Care. 2013;36(12):e197–8. doi:10.2337/dc13-1350
- Pradhan AD. Sex differences in the metabolic syndrome: implications for cardiovascular health in women. Clin Chem. 2014;60(1):44–52. doi:10.1373/clinchem.2013.202549
- Karastergiou K, Smith SR, Greenberg AS, Fried SK. Sex differences in human adipose tissues – the biology of pear shape. Biol Sex Differ. 2012;3(1):13. doi:10.1186/2042-6410-3-13
- Heid IM, Jackson AU, Randall JC, et al. Meta-analysis identifies 13 new loci associated with waist-hip ratio and reveals sexual dimorphism in the genetic basis of fat distribution. Nat Genet. 2010;42(11):949–960. doi:10.1038/ng.685
- Rennie KL, McCarthy N, Yazdgerdi S, Marmot M, Brunner E. Association of the metabolic syndrome with both vigorous and moderate physical activity. Int J Epidemiol. 2003;32:600–606. doi:10.1093/ije/dyg179
- Slentz CA, Aiken LB, Houmard JA, et al. Inactivity, exercise, and visceral fat. STRRIDE: a randomized, controlled study of exercise intensity and amount. J Appl Physiol. 1985;2005(99):1613–1618.
- González K, Fuentes J, Márquez JL. Physical inactivity, sedentary behavior and chronic diseases. Korean J Fam Med. 2017;38(3):111–115. doi:10.4082/kjfm.2017.38.3.111
- Admiraal WM, van Valkengoed IG, L de Munter JS, Stronks K, Hoekstra JB, Holleman F. The association of physical inactivity with type 2 diabetes among different ethnic groups. Diabet Med. 2011;28:668–672.4. doi:10.1111/j.1464-5491.2011.03248.x
- Sullivan PW, Morrato EH, Ghushchyan V, Wyatt HR, Hill JO. Obesity, inactivity, and the prevalence of diabetes and diabetes-related cardiovascular comorbidities in the U.S., 2000–2002. Diab Care. 2005;28:1599–1603. doi:10.2337/diacare.28.7.1599
- Sun K, Ren M, Liu D, Wang C, Yang C, Yan L. Alcohol consumption and risk of metabolic syndrome: a meta-analysis of prospective studies. Clin Nutr. 2014;33(4):596–602.
- Sun K, Liu J, Ning G. Active smoking and risk of metabolic syndrome: a meta-analysis of prospective studies. PLoS One. 2012;7(10):e47791. doi:10.1371/journal.pone.0047791
- Carlsson S, Hammar N, Grill V. Alcohol consumption and type 2 diabetes meta-analysis of epidemiological studies indicates a U-shaped relationship. Diabetologia. 2005;48(6):1051–1054. doi:10.1007/s00125-005-1768-5
- Corrao G, Bagnardi V, Zambon A, La Vecchia C. A meta-analysis of alcohol consumption and the risk of 15 diseases. Prev Med. 2004;38(5):613–619. doi:10.1016/j.ypmed.2003.11.027
- Slagter SN, Vliet-Ostaptchouk J, Vonk JM, et al. Associations between smoking, components of metabolic syndrome and lipoprotein particle size. BMC Med. 2013;11:195. doi:10.1186/1741-7015-11-195
- Walldius G,IJ, Apolipoprotein B and apolipoprotein A-I: risk indicators of coronary heart disease and targets for lipid-modifying therapy. J Intern Med. 2004;255:188–205. doi:10.1046/j.1365-2796.2003.01276.x
- Arsenault BJ, Lemieux I, Despres JP, et al. HDL particle size and the risk of coronary heart disease in apparently healthy men and women: the EPIC-Norfolk prospective population study. Atherosclerosis. 2009;206(1):276–281. doi:10.1016/j.atherosclerosis.2009.01.044
- Fujiyoshi A, Miura K, Kadowaki S, et al. Lifetime cigarette smoking is associated with abdominal obesity in a community-based sample of Japanese men: the Shiga Epidemiological Study of Subclinical Atherosclerosis (SESSA). Prev Med Rep. 2016;4:225–232. doi:10.1016/j.pmedr.2016.06.013
- Keith RJ, Al Rifai M, Carruba C, et al. Tobacco use, insulin resistance, and risk of type 2 diabetes: results from the multi-ethnic study of atherosclerosis. PLoS One. 2016;11(6):e0157592. doi:10.1371/journal.pone.0157592
- Cheng E, Burrows R, Correa P, Guichapani CG, Blanco E, Gahagan S. Apolipoprotein B and apolipoprotein A-I: risk indicators of coronary heart disease and targets for lipid-modifying therapy. Acta Diabetol. 2004;255(2):188–205. doi:10.1007/s00592-018-1264-2
- Lee KW, Park BJ, Kang HT, Lee YJ. Alcohol-drinking patterns and metabolic syndrome risk: the 2007 Korean National Health and Nutrition Examination Survey. Alcohol. 2011;45(5):499–505.
- Workman C, FA B. Post‐metabolic response to passive normobaric hypoxic exposure in sedendary overweight males: a pilot study. Nutr Metab. 2012;9(1):103. doi:10.1186/1743-7075-9-103
- Palmer BF, Clegg DJ. Ascent to altitude as a weight loss method: the good and bad of hypoxia inducible factor activation. Obesity. 2014;22(2):311–317. doi:10.1002/oby.20499
- Hagobian TA, Braun B. Interactions between energy surplus and short-term exercise on glucose and insulin responses in healthy people with induced, mild insulin insensitivity. Metabolism. 2006;55(3):402–408. doi:10.1016/j.metabol.2005.09.017