Abstract
Objectives
Diabetic foot ulcer (DFU) has been linked to high mortality and morbidity in diabetic patients. In spite of the increasing prevalence of diabetes and its complications, this issue has not been adequately studied in Iran.
Materials and methods
In this cross-sectional study we attempt to describe the prevalence of diabetic foot amputation in patients admitted to our training hospitals in Urmia, Iran, and also to determine the associated demographic, behavioral, and clinical factors.
Results
Of 94 patients with DFU, 34 (32%) had amputation. Those with amputation were significantly older and were also less educated than those without amputation, had longer duration of diabetes (hence were more likely to suffer from complications), and had high-risk wounds plus a poor glycemic control. On logistic regression analysis two variables were associated with amputation: Wagner classification ≥3 and HbA1c. On a receiver operating characteristics curve, the HbA1c cutoff point of 9.7% significantly discriminated to predict increasing risk of amputation.
Conclusion
Both glycemic control and promoting the knowledge of patients and health care professionals in order to diagnose DFU in the early stages and to prevent development of the high-grade wounds would be a significant step in reducing the burden of DFU and its effect on quality of life in Iran.
Keywords:
Introduction
Foot ulceration is one of the most serious and disabling complications of diabetes mellitus. It is the most common cause of nontraumatic foot amputation worldwide. Diabetic patients are 15 to 20 times more likely to require amputation than those without the disease.Citation1 The prevalence of diabetic foot ulcer (DFU) ranges from 4% to 10% in hospitalized patients. The risk of developing a foot ulcer in diabetic patients could be as high as 25% in their lifetime.Citation2 Nearly 14%–24% of patients with DFU require amputation, which means that every 30 seconds a lower limb is lost because of diabetes. Citation1 The Global Lower Extremity Amputation Study Group estimated that 25%–90% of all amputations were associated with diabetes.Citation3 Diabetic foot amputation tends to be concomitant with a rise in mortality rates over time. The concomitant mortality is believed to be 13%–40% at 1 year, 35%–65% after 3 years, and 39%–80% after 5 years.Citation1 Treatment of DFU results in increased healthcare expenditures, prolonged hospital length of stay, and risk for amputation.Citation1 In developed countries, more than 5% of diabetic patients have DFU, the care for which consumes up to 20% of the total healthcare resources available for diabetes.Citation4 In developing countries, not only does the prevalence of DFU exceed that in developed countries but also DFU care devours as much as 40% of the available resources.Citation4
Currently, the prevalence of diabetes in Iran is 7.7%, which is equivalent to 3 million cases when extrapolated to the Iranian population aged 25–64 years, with the prevalence of DFU estimated at 3%.Citation1,Citation5 This figure is expected to rise considerably by 2025.Citation6
Several risk factors for amputation among patients with DFU have been cited in the literature, including age; sex (male); comorbidities or complications of diabetes such as hypertension, nephropathy, and retinopathy; having a previous history of DFU; and duration of diabetes.Citation1,Citation2,Citation7–Citation10
However, the validity of these findings in different cultures and communities remains to be shown. Prediction of the outcome in patients with DFU might be helpful for clinicians in optimizing management strategy. Thus, we developed a cross-sectional study to describe the prevalence of amputation and to determine the associated demographic, clinical, and behavioral factors with amputation in hospitalized DFU patients in medical training settings. Clarifying these factors would lead to appropriate care and aid in preventing amputation.
Material and methods
This prospective cross-sectional study was conducted from September 2009 to December 2010. All diabetic patients with DFU admitted to two medical training hospitals (Taleghani and Imam) in Urmia, Iran, were enrolled into the study. The method of data collection was simple random sampling. The aim of the study was explained to all participants, and informed written consent was obtained from all. The Urmia University of Medical Sciences review board and ethics committee approved the study.
A questionnaire was used to collect data about clinical status, such as type of diabetes, duration of diabetes, treatment category (insulin therapy, oral agents, and diet), presence of complications of diabetes according to medical records (including retinopathy, nephropathy, presence of comorbidity such as hypertension, ischemic heart disease, dyslipidemia), previous history of DFU, the length of hospitalization, baseline laboratory data (including HbA1c and blood sugar), grade of foot ulcer, and behavioral factors, including current smoking (daily and occasional smokers) and body mass index (BMI). Please note: foot ulcer was graded according to Wagner’s classification: Grade 0, high- risk foot; Grade 1, superficial ulcer; Grade 2, deep ulcer penetrating to tendon, bone, or joint; Grade 3, deep ulcer with abscess or osteomyelitis; Grade 4, localized gangrene; and Grade 5, extensive gangrene requiring a major amputation. BMI was divided into two categories: normal <25 or overweight ≥25. Wounds were classified into two groups; Wegner grade ≤2 were classified as low risk and grade ≥3 were classified as high risk.
Data regarding age, sex, educational level, and marital status (married, single, divorced, widowed) were also collected in the same questionnaire.
Amputation was defined as the complete loss of the transverse anatomical plan of any part of the lower limb.
Statistical analysis
Patients were divided into two groups: those who underwent major or minor amputation and those without amputation. All statistical analysis was performed using SPSS (version 12, SPSS, Inc, Chicago, IL). We used simple percentage to calculate the prevalence of amputation. We used the χ2 test for categorical variables and independent Student’s t-test for continuous variables. A P-value of less than 0.05 was considered significant. Logistic regression analysis was constructed to model the odds of amputation versus nonamputation. All variables were examined for the association with amputation, including sociodemographic factors (age, sex, education, marital status), behavioral factors (BMI and smoking), and clinical factors (duration of diabetes, treatment intensity, number of complications, and Wagner classification). We calculated odds ratios (OR) and 95% confidence intervals (CI) for all variables in the models.
A receiver operating characteristics curve was generated to determine the predictability of HbA1c and blood sugar levels at admission time for amputation. Sensitivity and specificity of cutoff point for blood sugar and HbA1c were also calculated.
Results
Of the 94 patients, 63.8% were men and the mean age was 60.24 ± 11.5 years. More than half (57.4%) of the participants had a low education level (below high school). The mean BMI was 26.95 ± 3.3 and 60.6% of participants were overweight (BMI ≥ 25 kg/m2).
Most of the participants had diabetes type 2 (96.8%). Treatment category showed that 86.2% of participants were managed with an oral agent plus diet, and only 13.8% were on insulin alone or a combination of insulin and diet. Mean length of admission was 9.51 ± 5.3 days.
Eighty-four percent of patients reported having at least one complication of diabetes, eg, cardiovascular disease, nephropathy, or retinopathy. A total of 20.2% of patients were on antilipid therapy. There was a high frequency of hypertension (46.8%) and retinopathy (38.2%) when compared with other complications. Almost three-quarters (71.3%) of participants had a previous history of DFU. A total of 83% of patient wounds were classified as high risk (grade ≥3).
Prevalence of amputation and its associated factors
Of the 94 patients, 32 (34%) met the clinical criteria for amputation. Compared with the group without amputation, those with amputation were significantly older (68.15 ± 8.36 years vs 56.16 ± 10.88 years) (P-value = 0.000). Patients who were aged ≥50 years had a significantly higher risk of amputation than those aged ≤50 years (OR = 4.65, 95% CI: 1.22–5.51) (P-value = 0.007). The prevalence of amputation was the same in the males and females statistically.
Patients managed with amputation were less educated than those in the nonamputated group (25/32, 78.1% vs 29/62, 46.8%, P-value = 0.009). There was a significant difference regarding marital status; a higher proportion of patients with amputation were not married (46.9%) compared with those in the nonamputation group (16.1%) (P-value = 0.01). represents demographic, behavioral, and clinical characteristics in the amputation and nonamputation groups.
Table 1 Demographic, behavioral, and clinical features of diabetic foot ulcer (DFU) patients with and without amputation
Clinical factors associated with amputation were duration of diabetes, having at least one complication, having a previous history of DFU, and BMI < 25. The mean duration of diabetes was 9.21 ± 6.03 years in the amputation group and 5.34 ± 3.21 years in the nonamputation group (P-value = 0.008). The average number of previous DFU was 3.46 ± 1.81 and 1.5 ± 1.04 times in the amputation and nonamputation groups, respectively (P-value = 0.000). Patients without amputation were more likely to be overweight (OR = 2.7, 95% CI: 2.01–4.97) ().
Other clinical and behavioral factors such as treatment category, smoking, dyslipidemia, and ischemic heart disease had the same distribution in the amputation and nonamputation groups. Distribution of patients by Wagner ulcer classification showed grade ≥3 in 93.8% patients who underwent amputation, which was significantly different from the other group.
Comparison of diabetic complications revealed that retinopathy, nephropathy, and hypertension were more frequent among patients with amputation ().
Table 2 Comparison of diabetic complications and comorbidities between groups with and without amputation
Baseline laboratory data, including HbA1c and blood sugar at admission time, were significantly higher among patients who had amputation ().
Using logistic regression analysis and by excluding all confounders in the model, HbA1c ≥ 8% (OR = 4.2, 95% CI: 2.11–7.27) and high-risk wounds (OR = 6.4, 95% CI: 3.08–9.32) remained statistically significant regarding amputation.
Receiver operating characteristic curves were generated to determine the predictability of the levels of HbA1c and blood sugar at admission time for amputation ().
Figure 1 Receiver operating characteristics (ROC) curve showing HbA1c and blood sugar (BS) in predicting overall amputation.
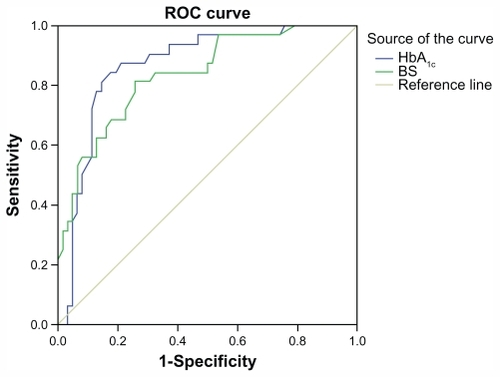
A cutoff point of 9.75% for HbA1c and 305 g/dL showed 75.2% specificity and 81.5% sensitivity for amputation. Area under the curve showed a value of 0.86 and 0.83 for HbA1c and blood sugar, respectively (P-value = 0.05).
Discussion
Management of the DFU by early education of the associated risk factors still remains a challenge in order to decrease the rate of amputation among DFU patients.
The overall prevalence of amputation in our setting was 34%. However, frequency of amputation was reported in a wide range in several studies. Larijani et alCitation11 reported that the rate of amputation dropped from 40% in 1995 to 14% in 2001 and to less than 12% in 2007 with a mean length of hospitalization stay of 4 weeks. Another study in Iran in 2008 noted an amputation rate of 28.8% among DFU patients. The overall amputation rate was found to be 52.4% in Japan, 27.2% in Singapore, and 21.8% in China.Citation3 Richard et alCitation12 reported that 35% of the patients with DFU underwent lower limb amputation in France during hospitalization. High amputation rates might be due to the prevalence of disease in different settings, late presentation, inadequate resources, and a local approach by surgeons.Citation13
Older patients are found to be less cooperative both physically and psychologically and to have a greater number of diabetic complications.Citation6 In our study, amputation was more frequent in those patients with a lower educational level, who are unmarried, and of older age, which suggests an association with social and financial factors.
The effect of gender on the frequency of DFU and amputation has been documented by many studies.Citation1,Citation14 The rate of amputation according to sex was about the same in our study.
Several studies showed that the duration of diabetes was correlated with higher risk of amputation,Citation10,Citation15,Citation16 which is the same as in our study and in contrast with the report by Li et al,Citation3 which found no relation between the duration of diabetes and the risk of amputation.
Meanwhile, insulin use was independently related to higher DFU occurrence and amputation.Citation15,Citation17,Citation18 The category of treatment had no effect on amputation in our study.
Patients with at least one complication of diabetes and a previous history of DFU also had a higher risk of amputation in our study. There is also a large discrepancy between rate of amputation, comorbidities, and chronic complications of diabetes. Yesil et alCitation10 have reported that the frequency of nephropathy was lower in patients who underwent amputation. However, the frequency of hypertension,Citation17 nephropathy, and retinopathy was higher with increasing risk of amputation.Citation3,Citation7–Citation9 Lipsky et alCitation19 reported that there was a high association between lower extremity amputation and its risk factors.
Some of the previous studies have reported that the Wagner classification has a strong predictive factor for amputation,Citation13,Citation17,Citation20 which was also concluded by the results of our study.
Sohn et alCitation21 reported a significant J-shaped association between BMI and DFU. As a matter of fact, obesity was a significant risk factor for developing microvascular complications. Citation22 A survey of the effectiveness of foot care education in diabetic patients in Iran has concluded that obese patients referring to diabetic clinics need much more attention and better care programs.Citation23 A BMI < 25 was significantly associated with amputation in our study, which is the same as previously reported by Yesil et al.Citation10 The energy consumption of the wound is higher during healing, due both to inflammatory cells and to the fibroblast production of collagen and matrix.Citation24 This can explain malnutrition in patients with BMI < 25 and a consequent delay in healing of the wound or an increased risk of amputation.
Alcohol consumption and cigarette smoking are reported to be behavioral risk factors of amputation.Citation2,Citation10,Citation15 There was no statistically significant difference between the number of smokers in amputation and nonamputation patients in our study, which was also reported by Li et al.Citation3
The prevalence of diabetic microvascular complications and diabetic neuropathy is also reported to be higher in patients with poor glycemic control,Citation22,Citation25 whereas little research has demonstrated no correlation between HbA1c and risk of amputation.Citation3,Citation16 It is strongly shown that HbA1c was a significant risk factor for overall amputation in previous studies.Citation7,Citation9,Citation26 According to our study, HbA1c is a predictive factor for risk of amputation, and the cutoff point for the risk is 9.2 (specificity 81% and sensitivity 87.5%).
One of the limitations of our study is that we evaluated the level of education and duration of diabetes based on self- reporting. Another limitation was to use medical records and drug history for verifying diabetic complications instead of clinical examination. These data came only from hospitalized patients, so outpatients with DFU who did not need amputation were not included in our study.
Conclusion
In summary, the fact that diabetes is a prevalent disease with an increasing incidence in Iran means that the rate of its complications such as DFU can be expected to soar in the future. Glycemic control and early diagnosis of DFU can be improved by increasing the knowledge of the patients and healthcare professionals to prevent the development of high-grade wounds, which would be a significant step in the collective effort to ease the burden of DFU in Iran.
Acknowledgment
Thanks to Urmia University of Medical Sciences for approval of the study and thanks to all the patients, nurses, and hospitals for their help and cooperation in this study.
Disclosure
All authors declare that they have no conflict of interest.
References
- Tabatabaei Malazy O Mohajeri-Tehrani MR Pajouhi M Iranian diabetic foot research network Adv Skin Wound Care 2010 23 450 454 20859075
- Marston WA Risk factors associated with healing chronic diabetic foot ulcers: the importance of hyperglycemia Ostomy Wound Manage 2006 52 26 28 30, 32 passim 16567857
- Li X Xiao T Wang Y Incidence, risk factors for amputation among patients with diabetic foot ulcer in a Chinese tertiary hospital Diabetes Res Clin Pract 2011 93 26 30 21466901
- Bakker K The year of the diabetic foot Diabetes Voice 2005 50 4 11
- Yekta Z Pourali R Aghassi MR Assessment of self-care practice and its associated factors among diabetic patients in urban area of Urmia, northwest of Iran Journal of Research in Health Sciences 2011 11
- Yekta Z Pourali R Yavarian R Behavioural and clinical factors associated with depression among individuals with diabetes Eastern Mediterranean Health Journal 2010 16
- Hennis AJ Fraser HS Jonnalagadda R Explanations for the high risk of diabetes-related amputation in a Caribbean population of Black African descent and potential for prevention Diabetes Care 2004 27 2636 2641 15504998
- Nather A Bee CS Huak CY Epidemiology of diabetic foot problems and predictive factors for limb loss J Diabetes Complications 2008 22 77 82 18280436
- Resnick HE Carter EA Sosenko JM Incidence of lower-extremity amputation in American Indians: the Strong Heart Study Diabetes Care 2004 27 1885 1891 15277412
- Yesil S Akinci B Yener S Predictors of amputation in diabetics with foot ulcer: single center experience in a large Turkish cohort Hormones (Athens) 2009 8 286 295 20045802
- Larijani B Afshari M Bastan Hagh MH Lower limb umputation in patients with diabetic foot ulcer: a 22-year review MJIRC 2006 8 4 21
- Richard JL Lavigne JP Got I Management of patients hospitalized for diabetic foot infection: results of the French OPIDIA study Diabetes Metab 2011 37 208 215 21169044
- Barberan J Granizo JJ Aguilar L Predictive model of short-term amputation during hospitalization of patients due to acute diabetic foot infections Enferm Infecc Microbiol Clin 2010 28 680 684 20570020
- Altindas M Kilic A Cinar C The epidemiology of foot wounds in patients with diabetes: a description of 600 consecutive patients in Turkey J Foot Ankle Surg 2011 50 146 152 21353997
- Jbour AS Jarrah NS Radaideh AM Prevalence and predictors of diabetic foot syndrome in type 2 diabetes mellitus in Jordan Saudi Med J 2003 24 761 764 12883610
- Mehmood K Akhtar ST Talib A Clinical profile and management outcome of diabetic foot ulcers in a tertiary care hospital J Coll Physicians Surg Pak 2008 18 408 412 18760063
- Al-Tawfiq JA Johndrow JA Presentation and outcome of diabetic foot ulcers in Saudi Arabian patients Adv Skin Wound Care 2009 22 119 121 19247012
- Boyko EJ Ahroni JH Stensel V A prospective study of risk factors for diabetic foot ulcer. The Seattle Diabetic Foot Study Diabetes Care 1999 22 1036 1042 10388963
- Lipsky BA Weigelt JA Sun X Developing and validating a risk score for lower-extremity amputation in patients hospitalized for a diabetic foot infection Diabetes Care 2011 34 1695 1700 21680728
- Winkley K Stahl D Chalder T Risk factors associated with adverse outcomes in a population-based prospective cohort study of people with their first diabetic foot ulcer J Diabetes Complications 2007 21 341 349 17967704
- Sohn MW Budiman-Mak E Lee TA Significant J-shaped association between body mass index (BMI) and diabetic foot ulcers Diabetes Metab Res Rev 2011 27 402 409 21360633
- Shera AS Jawad F Maqsood A Prevalence of chronic complications and associated factors in type 2 diabetes J Pak Med Assoc 2004 54 54 59 15134204
- Vatankhah N Khamseh ME Noudeh YJ The effectiveness of foot care education on people with type 2 diabetes in Tehran, Iran Prim Care Diabetes 2009 3 73 77 19524494
- Mary DL Nutrition issues in the patient with diabetes and foot ulcers Levin and O’Neals the Diabetic Foot 7th ed Philadelphia, PA Mosby Elsevier 2008
- Martin Borge V Herranz de la Morena L Castro Dufourny I Diabetic foot and risk factors An Med Interna 2007 24 263 266 17907895
- Miyajima S Shirai A Yamamoto S Risk factors for major limb amputations in diabetic foot gangrene patients Diabetes Res Clin Pract 2006 71 272 279 16139385