
Abstract
Gestational diabetes mellitus (GDM) is a frequent medical complication during pregnancy. Screening and diagnostic practices for GDM are inconsistent across the world. This narrative review includes data from 87 observational studies and randomized controlled trials (RCTs), and aims to give an overview of the current evidence on screening strategies and diagnostic criteria for GDM. Screening in early pregnancy remains controversial and studies show conflicting results on the benefit of screening and treatment of GDM in early pregnancy. Implementing the one-step “International Association of Diabetes and Pregnancy Study Groups” (IADPSG) screening strategy at 24–28 weeks often leads to a substantial increase in the prevalence of GDM, without conclusive evidence regarding the benefits on pregnancy outcomes compared to a two-step screening strategy with a glucose challenge test (GCT). In addition, RCTs are needed to investigate the impact of treatment of GDM diagnosed with IADPSG criteria on long-term maternal and childhood outcomes. Selective screening using a risk-factor-based approach could be helpful in simplifying the screening algorithm but carries the risk of missing significant proportions of GDM cases. A two-step screening method with a 50g GCT and subsequently a 75g oral glucose tolerance test (OGTT) with IADPSG could be an alternative to reduce the need for an OGTT. However, to have an acceptable sensitivity to screen for GDM with the IADPSG criteria, the threshold of the GCT should be lowered from 7.8 to 7.2 mmol/L. A pragmatic approach to screen for GDM can be implemented during the COVID-19 pandemic, using fasting plasma glucose (FPG), HbA1c or even random plasma glucose (RPG) to reduce the number of OGTTs needed. However, usual guidelines and care should be resumed as soon as the COVID pandemic is controlled.
Introduction
Gestational diabetes mellitus (GDM) is defined as diabetes diagnosed in the second or third trimester of pregnancy provided that overt diabetes was excluded before pregnancy or at the latest in early pregnancy.Citation1 Most international guidelines such as the American Diabetes Association (ADA) and World Health Organization (WHO) recommend to screen for overt diabetes at first prenatal visit, since these women have (untreated) a very high risk for pregnancy complications and need treatment with insulin.Citation1,Citation2 The prevalence of GDM is rising globally and if left untreated, the condition is associated with an increased risk of fetal and maternal complications such as preeclampsia and large-for-gestational age (LGA) infants.Citation3,Citation4 Shortly after delivery, the glucose values generally normalize, but women with GDM and their offspring are at increased risk to develop type 2 diabetes (T2DM) later in life.Citation5–Citation7 Two large randomized controlled trials (RCTs) have confirmed that treatment of GDM between 24 and 28 weeks of pregnancy results in a lesser degree of perinatal complications, mainly in the frequency of LGA and preeclampsia.Citation3,Citation4 However, controversy exists regarding the optimal screening and diagnostic approach for GDM. These controversies are situated in various domains such as the use of different diagnostic criteria for GDM, selective screening based on risk factors versus universal screening, one-step screening or two-step screening, the use of alternate screening methods like fasting plasma glucose (FPG) or HbA1c, the potential benefit of screening for GDM in early pregnancy, screening for GDM in specific populations or circumstances, such as in women who underwent bariatric surgery or in the COVID-19 pandemic setting.
The initial diagnostic criteria of GDM were established by O’ Sullivan almost 60 years ago.Citation8 In the 1980s, Carpenter and Coustan modified these criteria and proposed a two-step screening method, consisting of a 50g glucose challenge test (GCT) and subsequent a 3h 100g oral glucose tolerance test (OGTT) if screening threshold of the GCT was exceeded.Citation9 However, these criteria were chosen to identify women at high risk for the development of diabetes after pregnancy and not necessarily to identify pregnancies with an increased risk for adverse perinatal outcomes.Citation10 In 1980, the 2h 75g OGTT was established as the diagnostic test for diabetes and glucose intolerance, and the WHO extended this recommendation to pregnant women. However, the ADA and many other medical associations continued to follow the National Diabetes Data Group (NDDG) recommendation to use the 3h 100g OGTT, because the 2h 75g OGTT had been little investigated during pregnancy. In 2010, the “International Association of Diabetes and Pregnancy Study Groups” (IADPSG) made an attempt to unify the guidelines for screening and diagnosis of GDM by recommending a universal one-step approach with a 75g OGTT and more stringent diagnostic criteria.Citation11 This recommendation was based on the results of the “Hyperglycemia and Adverse Pregnancy Outcomes” (HAPO) study, which demonstrated a continuous and graded relationship between maternal hyperglycemia and the risk for adverse perinatal outcomes.Citation12 However, the adoption of the IADPSG criteria remains controversial due to the significant increase in the number of women categorized and treated as GDM. Recently, a review on current screening guidelines for GDM assessed 16 different guidelines across the world and confirmed that there is an ongoing lack of consensus, with inconsistencies mainly focusing on the screening process (one-step vs two-step) and criteria for the OGTT.Citation13 In addition, a survey in 2015 on screening practices in Europe demonstrated that the majority of European societies still recommended risk-factor-based screening and about one-third recommended a universal one-step approach with a 75g OGTT and IADPSG criteria.Citation14 This lack of consensus creates problems in addressing and comparing prevalence, outcomes, efficacy of treatment, and follow-up of GDM.
This comprehensive review provides an update on screening strategies and diagnostic criteria for GDM in early and late pregnancy. In addition, evidence on pragmatic approaches to screen for GDM after bariatric surgery and in a pandemic setting such as COVID-19 are discussed.
Methods
A literature search was conducted on PubMed between January 2021 and March 2021. Cross-sectional studies, case–control studies, cohort studies, and RCTs were considered for this narrative review. The populations studied included pregnant women with or without GDM, in which we evaluated the effects of the implementation of different protocols, guidelines or programs for screening for GDM, compared with the absence of screening, or compared with other protocols, guidelines or programs for screening. Screening strategies included universal versus selective screening, one-step versus two-step screening, early versus late screening, screening after bariatric surgery, and screening in times of COVID-19. We excluded animal studies, descriptive designs (case series and case reports), studies with a low quality (no method section, no p-values mentioned), and articles written in a language other than English, French or Dutch. The search was not limited to a certain time period. The following search strategy was used in PubMed: ((“Screening”[Title/Abstract] OR “screening strateg*”[Title/Abstract]) AND (“diabetes, gestational”[MeSH Terms:noexp] OR “Gestational diabetes”[Title/Abstract] OR “Pregnancy-Induced Diabetes”[Title/Abstract] OR “gestational hyperglycemia”[Title/Abstract] OR “hyperglycemic pregnancy”[Title/Abstract] OR “Pregnancy-Induced Diabetes”[Title/Abstract] OR “gestational hyperglycemia”[Title/Abstract] OR “gestational glucose intolerance”[Title/Abstract])) AND (((“Universal”[Title/Abstract] OR “one-step”[Title/Abstract]) AND “Screening”[Title/Abstract]) OR (“risk factor”[Title/Abstract] AND “Screening”[Title/Abstract]) OR (“two-step”[Title/Abstract] AND “Screening”[Title/Abstract]) OR (“early screening”[Title/Abstract] OR “in early pregnancy”[Title/Abstract]) OR (“Bariatric Surgery”[MeSH Terms] OR “Gastric Bypass”[MeSH Terms] OR “Gastrectomy”[MeSH Terms] OR “Bariatric Surgery”[Title/Abstract] OR “Gastric Bypass”[Title/Abstract] OR “Gastrectomy”[Title/Abstract]) OR (“COVID-19”[MeSH Terms] OR “SARS-CoV-2”[MeSH Terms] OR “COVID-19”[Title/Abstract] OR “SARS-CoV-2”[Title/Abstract] OR “2019-nCoV”[Title/Abstract] OR “Coronavirus Disease-19”[Title/Abstract])).
In addition, the reference lists of all identified articles were examined to identify studies not captured by the electronic search. As this is not a systematic review of the literature, we reported our results in a descriptive manner.
Overview of the Included Publications
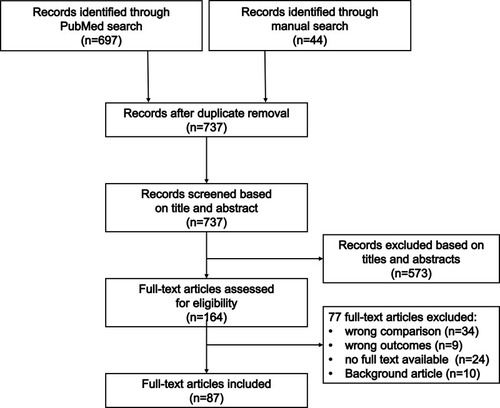
We identified 737 articles of which 164 were selected as possibly relevant. After examination of the full-text articles, 87 studies were included in this review ().
Figure 1 The literature search and selection process.
Screening in Early Pregnancy
The Impact of Screening in Early Pregnancy on Pregnancy Outcomes
The aim of early screening would be to identify women at low or high risk for GDM later in pregnancy. In addition, this might help to identify women who already have GDM to allow earlier treatment and potentially improve maternal and neonatal outcomes.
Early testing in pregnancy for diabetes will lead to the identification of hyperglycemia under the threshold of overt diabetes. These women could be labeled as early GDM. However, the IADPSG criteria have not been validated for use in early pregnancy. Observational studies show conflicting results as to whether screening for early-onset GDM can improve pregnancy outcomes (). Several studies reported an improvement in maternal and neonatal outcomes.Citation15–Citation18 A retrospective cohort study by Bartha et al found that early glucose intolerance screening with a GCT could avoid diabetes-related complications such as polyhydramnios, fetal anomalies and preterm birth in women diagnosed with GDM.Citation16 Ryan et al demonstrated that early screening improved the primary composite outcome [emergency caesarean section, neonatal hypoglycemia and macrosomia; 41.2% vs 30.3%, adjusted OR (aOR) 0.62, 95% CI 0.43–0.91] in high-risk pregnant women.Citation18 More recently, a large French study reported that women with early fasting hyperglycemia who received initial care versus those who did not, were more likely to be insulin-treated during pregnancy (58.0% vs 20.9%, respectively; p < 0.00001), gained less gestational weight (8.6 ± 5.4 kg vs 10.8 ± 6.1 kg, respectively; p < 0.00001), had a lower rate of preeclampsia [1.2% vs 2.6%, aOR 0.247 (0.082–0.759), p = 0.01], and similar rates of LGA infants and shoulder dystocia.Citation15 On the contrary, no beneficial effect of early diagnosing or treatment of GDM on maternal or neonatal outcomes was found in several other studies.Citation19–Citation22 These studies showed that early screening for GDM nearly doubled the prevalence of GDM and that women with an early GDM diagnosis were treated to a greater extent with pharmacotherapy. However, no differences were observed in neonatal outcomes such as small-for-gestational age (SGA) and LGA infants, cesarean sections and macrosomia.Citation19,Citation20 Hong et al reported that women who were screened prior to 20 weeks were more likely to receive insulin and to deliver preterm compared with routinely screened women.Citation21 They hypothesized that early screening and diagnosis of GDM could result in more aggressive management of the disease due to a presumption of pregestational diabetes. Another prospective cohort study showed that early-onset GDM was associated with an increased risk of Apgar score at 1 min <7, neonatal respiratory distress syndrome and neonatal intensive care unit (NICU) admission compared to the late-onset group.Citation22 In addition, the DALI (vitamin D And Lifestyle Intervention for GDM prevention) study in obese women showed that women with early GDM had a profile similar to the metabolic syndrome and that prepregnancy body mass index (BMI) was a strong predictor of early GDM.Citation23 These findings support the need for weight control before pregnancy to improve perinatal outcomes.
Table 1 Screening for GDM in Early Pregnancy
Few results are yet available from large RCTs comparing treatment of early-onset GDM with standard treatment of GDM between 24 and 28 weeks of pregnancy (). Several large RCTs are still ongoing, such as the “Prediabetes in pregnancy, can early intervention improve outcomes” (PINTO) study,Citation24 the “Treatment of Booking Gestational diabetes Mellitus” (ToBOGM) studyCitation25 and the “Effect of Early Screening and Intervention for Gestational Diabetes Mellitus on Pregnancy Outcomes” (TESGO) study (NCT03523143).Citation26 A small RCT demonstrated that early treatment of mild hyperglycemia (HbA1c of 5.7–6.4%) did not reduce the risk of GDM, except in non-obese women.Citation27 A pilot study of the ToBOGM trial showed that early GDM treatment was associated with a reduced LGA rate (0% vs 33% p = 0.030) but an increased NICU admission rate (36% vs 0% p = 0.043), largely driven by a higher rate of SGA infants.Citation28 SGA can be a consequence of overtreatment or insufficient gestational weight gain. Other smaller RCTs did not show benefits of early screening and treatment of GDM on pregnancy outcomes. The EGGO study, for instance, showed no effect of early screening for GDM on the composite perinatal outcome consisting of macrosomia, primary cesarean delivery, hypertensive disease of pregnancy, shoulder dystocia, neonatal hyperbilirubinemia, and neonatal hypoglycemia in obese women.Citation29 The LiP study evaluated the impact of lifestyle intervention vs standard care on metabolic and clinical outcomes in obese women with GDM in early pregnancy, classified according to the IADPSG criteria. They found no differences in obstetric or metabolic outcomes except for a higher rate of planned cesarean sections in the early treated group (22.2% vs 5.6%, p = 0.02).Citation30 In addition, an RCT in 200 women with hyperglycemia in early pregnancy showed that early treatment could not improve maternal or neonatal outcomes significantly.Citation31
Different methods have been suggested for the screening of GDM in early pregnancy: direct glycemic markers such as FPG, indirect methods like HbA1c, and more recently biochemical markers (). Riskin et al demonstrated that higher first-trimester FPG levels in the non-diabetic range increased the risk for adverse pregnancy outcomes, including cesarean sections, LGA infants and macrosomia.Citation32 Likewise, a multicentric Belgian prospective cohort study showed recently that women with a FPG of 5.1–5.5 mmol/L in early pregnancy had a significantly higher NICU admission rate compared to women with FPG < 5.1 mmol/L (20.4% vs 9.3%, p = 0.009).Citation33 On the contrary, several studies have shown that a FPG ≥ 5.1 mmol/L in early pregnancy was a poor predictor of GDM.Citation15,Citation33 A Belgian study demonstrated that only 37% of all women with an FPG ≥ 5.1–5.5 mmol/L in early pregnancy developed GDM based on the IADPSG criteria later in pregnancy.Citation33 A large Chinese study showed that in their population an FPG 6.1–7.0 mmol/L in early pregnancy was a much stronger predictor for GDM later in pregnancy compared to an FPG ≥ 5.1 mmol/L.Citation34 A French study recommended to use a threshold of 5.5 mmol/L for starting GDM treatment in early pregnancy, as they demonstrated improved pregnancy outcomes in these women.Citation15
Few studies evaluated the use of HbA1c in early pregnancy to diagnose GDM.Citation35–Citation39 It has been established that an early HbA1c ≥5.9% identified women at high risk of adverse pregnancy outcomes independently of GDM diagnosis later in pregnancy.Citation35,Citation39 HbA1c can be used to screen for overt diabetes, but most studies demonstrated that HbA1c in early pregnancy has insufficient sensitivity and specificity to use as a diagnostic test for GDM. However, it could still be useful in simplifying the algorithm for GDM screening.Citation36–Citation38 A retrospective cohort study showed that HbA1c at first prenatal visit allowed an early diagnosis of GDM in 25.8% of women; however, HbA1c could not replace routine testing for GDM later in pregnancy with an OGTT because of poor sensitivity.Citation37 HbA1c could be used as an adjunct to routine testing, identifying those with values between 5.9% and 6.4% at high risk of GDM early in pregnancy, allowing early intervention to potentially improve perinatal outcomes. However, RCTs are needed to prove that treatment of women with mildly elevated HbA1c in early pregnancy leads to better outcomes.
Prediction Models in Early Pregnancy
Improved prediction of GDM through identification of risk factors might increase the diagnostic accuracy of selective screening strategies and allow lifestyle interventions in early pregnancy to prevent the development of GDM and adverse pregnancy outcomes. Various risk factors for GDM have been identified, but it remains a struggle to accurately predict who is at increased risk to develop GDM. Several studies have proposed prediction models, such as the risk scores of van Leeuwen en TeedeCitation40,Citation41 (). More recently, Benhalima et al developed a prediction model for GDM based on the IADPSG criteria, using easy available clinical and biochemical risk factors in early pregnancy.Citation42 In this model, a history of a first degree relative with diabetes, a history of GDM, non-Caucasian origin, age, height, weight, FPG, triglycerides and HbA1c were independent predictors for GDM, with an area under the curve (AUC) of the model of 0.72 [95% confidence interval (CI) 0.66–0.78] after cross-validation, compared to an AUC of 0.67 (95% CI 0.63–0.71) using the van Leeuwen model and an AUC of 0.66 (95% CI 0.62–0.70) using the Teede model.Citation40–Citation42 In conclusion, prediction models based on variables in early pregnancy seem to have moderate accuracy to predict GDM.
Screening for GDM Between 24 and 28 Weeks of Pregnancy
Introduction of the IAPDSG Criteria: What is the Impact on Prevalence and Outcomes?
Since 2010, the IADPSG recommends a universal one-step approach with a 75g OGTT at 24–28 weeks of pregnancy for screening and diagnosis of GDM. The IADPSG criteria have been adopted by the WHO since 2013, and are therefore now commonly referred to as the 2013 WHO criteria for GDM.Citation2,Citation11 However, the IADPSG recommendation remains controversial due to the significant increase in GDM prevalence. Moreover, the implementation of the IADPSG screening strategy leads to an increased workload with the need for a fasting test, and this might lead to increased medicalization of care. An overview of the most commonly used guidelines for screening and diagnosis of GDM is shown in .
Table 2 Current Guidelines for Screening and Diagnosis of GDM
Many studies reported a substantial increase in the prevalence of GDM if the more stringent IADPSG criteria are adopted.Citation43–Citation49 However, conflicting evidence exists regarding the impact of introducing IADPSG criteria on maternal and neonatal outcomes. There are no RCTs that have compared treatment of GDM based on the IADPSG criteria with no treatment. Some observational studies reported no difference or even an increase in adverse perinatal outcomes,Citation46,Citation47,Citation50–Citation55 whereas others showed a significant improvement in perinatal outcomes associated with the use of the IADPSG criteriaCitation56–Citation58 ().
Table 3 One-Step Screening with IADPSG Criteria versus One- or Two-Step Screening with Other Criteria
A Spanish study reported that the prevalence of GDM doubled following the introduction of the IADPSG screening strategy compared to the previous use of the two-step screening strategy with the Carpenter and Coustan criteria (CC). The adoption of the IADPSG criteria improved pregnancy outcomes such as a reduction in the rate of gestational hypertension (4.1 to 3.5%; −14.6%, p < 0.021), cesarean section (25.4 to 19.7%; −23.9%, p < 0.002), LGA rate (4.6 to 3.7%; −20%, p < 0.004), SGA rate (7.7 to 7.1%; −6.5%, p < 0.042), and NICU admissions (8.2 to 6.2%; −24.4%, p < 0.001).Citation56 In contrast, an Australian study showed a 74% increase in annual incidence of GDM by changing from the “Australasian Diabetes in Pregnancy Society” (ADIPS) diagnostic criteria to the universal IADPSG strategy. This was not associated with improvements in primary health outcomes such as caesarean section rates, hypertensive disorder of pregnancy, LGA infant rates and preterm birth.Citation57 However, babies born to mothers with GDM diagnosed with the IADPSG criteria had lower rates of neonatal hypoglycemia and NICU admissions, suggesting a milder form of the disease.Citation57 A Belgian retrospective cohort study reported that GDM prevalence increased significantly from 3.4% to 16.2% comparing a two-step screening strategy with one-step IADPSG criteria, but no significant differences in maternal and neonatal complications were observed.Citation51 A pre-post comparison study in Australia also found that the introduction of the IADPSG criteria increased GDM prevalence from 8.7% to 11.9%, but that it was not associated with lower rates of gestational hypertension, cesarean birth, or LGA or SGA neonates.Citation47 A multicenter retrospective study demonstrated that introducing the IADPSG criteria resulted in an earlier GDM diagnosis, lower rates of insulin treatment and more spontaneous deliveries compared with a cohort diagnosed with the 1999 WHO criteria. However, no significant differences were found in adverse pregnancy outcomes.Citation55 Studies that evaluated perinatal outcomes of women diagnosed with GDM by the IADPSG criteria who would not have been identified with other criteria showed in general that these women had higher adverse outcome rates compared with GDM-negative controls.Citation48,Citation59,Citation60
These conflicting results highlight the need for long-term, adequately powered, prospective research to establish if applying the IADPSG one-step screening strategy decreases the frequency of adverse outcomes. An overview of the (ongoing) RCTs is given in . A small Iranian RCT compared pregnancy outcomes in women diagnosed with GDM by the IADPSG one-step screening versus two-step screening using the CC criteria. They demonstrated that the group diagnosed with the IADPSG criteria had only a decreased risk of neonatal hyperbilirubinemia (odds ratio (OR) 0.25, 95% CI 0.68–0.88).Citation61 Another RCT performed in 1000 pregnant women compared the incidence, maternal and fetal outcomes of GDM diagnosed using the one-step screening with IADPSG criteria versus two-step screening with GCT and diagnosis based on a 100g OGTT with CC criteria.Citation62 They found that the incidence of GDM using IADPSG criteria almost doubled (19.23% vs 11.81%, p=0.0001), and that maternal and neonatal outcomes were comparable in both groups except for lower rates of preterm delivery (11.6% vs 24.1%, relative risk (RR) 2.08, 95% CI 1.01–4.2, p = 0.046) and neonatal hypoglycemia (7.4% vs 29.31%, RR 3.98, 95% CI 1.75–9.01, p = 0.003) when using IADPSG criteria. Very recently, a large pragmatic RCT in about 23,000 pregnant women from the US evaluated the impact of a one-step screening strategy with IADPSG criteria compared with two-step screening with GCT and 100g OGTT using the CC criteria. They showed that despite a much higher rate of GDM diagnosis in the IADPSG group (16.5% vs 8.5%,), there were no significant differences in perinatal and maternal complications between both groups.Citation63 The Changing Diagnostic Criteria for Gestational diabetes (CDC4G) in Sweden study is an ongoing RCT (ISRCTN41918550) that also aims to evaluate whether treating women with GDM diagnosed by the IADPSG screening strategy will reduce the risks of adverse pregnancy outcomes.Citation64 Another ongoing RCT (NCT02309138) involves 921 women to compare diagnosis of GDM and pregnancy outcomes according to the CC criteria compared with the IADPSG criteria.Citation65
In conclusion, implementing the IADPSG screening strategy leads to a much higher prevalence of GDM without evidence of improvement pregnancy outcomes compared to a two-step screening strategy using the CC criteria for GDM. However, long-term follow-up studies are needed since women identified as GDM by the IADPSG screening strategy might be a higher risk population for diabetes and obesity postpartum. The HAPO Follow-up Study investigated whether GDM diagnosed with IADPSG criteria was associated with long-term risks for a disorder of glucose metabolism in mothers and greater adiposity in children.Citation66 They found that GDM diagnosed with IADPSG criteria was significantly associated with maternal development of prediabetes or T2DM (OR 3.44), but not with childhood overweight or obesity at a median follow-up of 11.4 years. However, additional analysis showed that the children of these mothers had increased measures of adiposity and a higher risk of impaired glucose tolerance compared with offspring of mothers without GDM.Citation67,Citation68 With the increasing prevalence of GDM and potential transgenerational impact on the offspring, adequately powered interventional trials are needed to investigate the effect of prevention and treatment of GDM diagnosed with IADPSG criteria on long-term maternal and childhood outcomes.
Screening Based on Risk Factors or Universal Screening for GDM
The debate on the best way to screen for GDM continues, with conflicting recommendations for universal and selective screening. Over the past years, different screening tools have been proposed to diminish the need for an OGTT, but large inconsistencies exist regarding the specific screening procedures and outcomes that should necessitate diagnostic testing. The ongoing discussion is also due to the lack of RCTs that have evaluated whether universal screening for GDM leads to better pregnancy outcomes than selective screening for GDM.
In several guidelines, the decision for a diagnostic test is often still based on maternal risk factor assessment,Citation69–Citation72 but there is no clear consensus on which risk factors should be included in the decision-making process and whether this is an adequate approach to screen for GDM. Comparing the accuracy of different European selective screening guidelines to detect GDM, Benhalima et al showed that about 50% of pregnant women would need an OGTT with the lowest number of missed cases (33%) by the Dutch guidelines.Citation73 Various studies have confirmed that a risk-factor-based approach misses 5–45% of GDM casesCitation74–Citation81 (). An argument for using a selective, risk-factor-based approach would be that women who are only detected as part of universal screening and not by risk-factor-based screening, have a milder form of GDM with similar pregnancy outcomes as the background pregnant population. A French retrospective cohort study found that selective screening based on risk factors would have missed one-sixth of GDM cases diagnosed with IADPSG criteria, but that these cases were milder, characterized by normal FPG, and that LGA was only associated with GDM in the presence of risk factors.Citation80 A more recent retrospective study in more than 12,000 women confirmed that women with GDM diagnosed according to the IADPSG criteria without risk factors had fewer obstetric and neonatal complications compared with those having risk factors.Citation82 In contrast, several studies showed that missed GDM cases without risk factors had worse pregnancy outcomes than women without GDM.Citation77,Citation78 For example, data from the Irish ATLANTIC-DIP study reported that selective screening based on risk factors in a Caucasian population missed 20% (using National Institute for Health and Care Excellence (NICE) criteria), 16% (following Irish guidelines), and 5% (with ADA guidelines) of women diagnosed with GDM using IADPSG criteria.Citation78 Moreover, outcomes in these pregnancies were worse compared with normal glucose tolerance (NGT) pregnancies, including hypertensive disorders, cesarean sections, polyhydramnios, congenital malformations and NICU admissions.Citation78 Often, the choice between universal and selective screening depends on the organization of prenatal care and the characteristics of the pregnant population, which differ widely internationally. In general, most guidelines such as the ADA, WHO and the International Federation of Gynecology and Obstetrics (FIGO) recommend universal screening in countries with enough resources, while alternative screening strategies can be used in low resource settings.Citation1,Citation2,Citation83
Table 4 Selective Screening Based on Risk-Factors versus Universal Screening
One-Step versus Two-Step Screening
Several professional associations such as the American College of Obstetricians and Gynecologists (ACOG), the National Institute of Health (NIH), German and Flemish guidelines recommend a universal two-step screening strategy, using a non-fasting 50g GCT to limit the number of OGTTs that are needed.Citation84–Citation87 The GCT has the advantage that it can be performed in the non-fasting state, it is better tolerated and takes less time than the OGTT, and can therefore be easily implemented in primary care. The GCT has been used in combination with the 100g OGTT or the 75g OGTT with various diagnostic criteria such as the CC criteria, the NDDG criteria, the 1999 WHO criteria, or the Canadian Diabetes Association criteria. A systematic review showed in 2013 that the sensitivity and specificity for the OGTT at a GCT threshold of 7.8 mmol/L after 1 hour were 70–88% and 69–89% respectively. At a threshold of 7.2 mmol/L after 1 hour, sensitivity varied between 88% and 99% and specificity between 66% and 77%.Citation88 More recently, the two-step screening strategy with diagnosis based on the 100g OGTT and CC criteria has been shown to lead to similar pregnancy outcomes compared to the one-step approach with IADPSG criteria, while it has the advantage that the number of OGTTs can be limited and that the prevalence of GDM is much lowerCitation63 (). A large Belgian multicentric prospective cohort study (BEDIP-N) has demonstrated that a GCT can also be used in a two-step screening strategy with the diagnosis of GDM based on a 75g OGTT with the IADPSG criteriaCitation89 (). However, to have an acceptable sensitivity to screen for GDM with the IADPSG criteria, the threshold of the GCT should be lowered from 7.8 to 7.2 mmol/L after 1 hour. In our center, a modified two-step screening strategy combining the GCT ≥7.2 mmol/L with clinical risk factors is applied.Citation87 Women with a BMI ≥30 kg/m2 and/or a previous history of GDM immediately receive a 75g OGTT with the use of IAPDSG criteria at 24 weeks since they are at high risk for GDM, while women without any of these risk factors would be screened with a 50g GCT. This strategy can reduce the workload and the need for an OGTT in nearly 60% of the women while reducing the number of women that would be missed with GDM.
Additional Screening Methods
An overview of studies investigating additional screening methods for GDM to limit the number of OGTTs needed is given in .
Table 5 Use of FPG, HbA1c or pGCD59 as a Screening Tool
An FPG at the time of screening for GDM between 24 and 26 weeks of pregnancy can be used to decide whether a full OGTT is needed for the diagnosis of GDM. When FPG is ≥ 5.1 mmol/L, GDM can be diagnosed according to the IADPSG criteria and an OGTT can be avoided.Citation2 Alternatively, an FPG threshold with a high negative predictive value for GDM could be applied (in low resource settings) to reduce the number of women requiring an OGTT and at the same time avoiding missed diagnoses. In 2010, a retrospective cohort study in a South Asian population suggested a rule-in/rule-out approach for the FPG to predict GDM, with a higher FPG threshold of ≥5.1 mmol/L ruling in GDM in 28.9% of women with 100% specificity and a lower FPG threshold of <4.4 mmol/L ruling out GDM in 21.7% women at an acceptable sensitivity of 95.4%.Citation45 This approach could eliminate half of the OGTTs needed to diagnose GDM, thereby providing relief to health-delivery systems in countries with high-risk populations. More recently, a prospective study in South-African women confirmed that universal screening using FPG ≥ 4.5 mmol/L had greater sensitivity and specificity in identifying GDM-affected women and required fewer women to undergo a resource-intensive diagnostic OGTT than risk-factor-based selective screening.Citation90 Likewise, a retrospective study found that risk factor screening for GDM alone or in combination with random capillary glucose was poorly predictive of GDM, but FPG 4.8–5.0 mmol/l showed good test characteristics and resulted in a low rate of OGTTs needed.Citation91 A study evaluating FPG as a screening tool to rule-out GDM in a low-risk population found that women with FPG ≤3.4 mmol/L were at low risk of developing GDM with a sensitivity of 91.3%, thereby avoiding a two-step screening in 10% of their population.Citation92
Some authors suggest that sensitivity and specificity for risk-factor based GDM screening could be considerably improved by using clinical risk prediction models that include combinations of several risk indicators in combination with FPG for improved prediction. For example, an estimation model developed by an Austrian research group (including history of GDM, glycosuria, family history of diabetes, age, preconception dyslipidemia and ethnic origin, in addition to FPG) showed that it was accurate for detecting GDM in participants with normal FPG. The ROC AUC of the screening algorithm was 0.90 (95% CI 0.88, 0.91) and a cut-off value of 0.20 was able to differentiate between low and intermediate risk for GDM with a high sensitivity.Citation93 More recent research is also focused on the use of risk models to connect hyperglycemia in pregnancy (HIP) with adverse pregnancy outcomes. A risk calculator developed by an Australian research group integrated the risks of hyperglycemia, maternal BMI and other basic demographic data available at the OGTT, and had a superior performance on ROC analysis for predicting an individual’s absolute risk of adverse pregnancy outcomes compared to the existing GDM diagnostic criteria.Citation94 The Prediction for Risk-Stratified care for women with GDM (PeRSonal GDM) study is still ongoing and will develop, validate and evaluate the clinical utility of a prediction model for adverse pregnancy outcomes in women with GDM.Citation95 These models show promise for use in clinical practice, but further research and development is necessary.
Several studies evaluated the usefulness of an HbA1c measurement for the diagnosis of GDM. In the large HAPO study cohort, associations were significantly stronger with glucose measures than with HbA1C for different adverse neonatal outcomes, suggesting that measurement of HbA1c is not a useful alternative to an OGTT for diagnosing GDM in pregnant women.Citation96 Later studies confirmed that even though HbA1c measurement does not have sufficient sensitivity and specificity to be used as the only diagnostic test for GDM, different HbA1c thresholds in combination with an OGTT could be useful in detecting GDMCitation49,Citation97–Citation100. In 2019, a systematic review bundled the results of eight studies that investigated the accuracy of HbA1c in the diagnosis of GDM.Citation101 The diagnostic accuracy of HbA1c was reported at different thresholds ranging from 5.4% to 6.0%, and the AUC was 0.825 (95% CI 0.751–0.899), indicating a good level of overall accuracy. They concluded that the HbA1c test presented high specificity but low sensitivity regardless of the threshold used to diagnose GDM. Therefore, HbA1c could be useful as a rule-in test in association with standard diagnostic tools such as an OGTT to diagnose GDM.
Globally, researchers are working to identify biomarkers that may have potential future application in diagnosing women with GDM. One such promising biomarker is plasma glycated CD59 (pGCD59), a cell membrane-anchored complement regulatory protein that protects “self” cells from complement-mediated damage. A case–control study evaluated levels of pGCD59 in plasma samples from 1000 women who underwent routine screening and diagnosis of GDM. It was the first study to demonstrate that a single measurement of pGCD59 at 24–28 weeks of gestation could identify women with GDM with high sensitivity and specificity, and that it could potentially identify the risk for LGA.Citation102 More recently, these findings were confirmed by Ma et al, showing that pGCD59 in pregnant women before 20 weeks of pregnancy accurately predicts the results of the OGTT and that pGCD59 levels were associated with a higher risk of delivering an LGA infant.Citation103 However, prospective studies are needed to confirm the clinical utility of pGCD59 as a biomarker for detection and diagnosis of GDM. An ongoing study aims to prospectively examine the validity of pGCD59 as a biomarker for the prediction, diagnosis, management and follow-up of women with GDM diagnosed using IADPSG criteria in a one-step approach in an unselected pregnant population.Citation104
Two recent systematic reviews elucidated the potential role of other first-trimester biochemical predictors such as inflammatory markers (C-reactive protein, tumor necrosis factor-alpha), insulin resistance markers (fasting insulin, sex hormone-binding globulin), adipocyte-derived markers (adiponectin, leptin) and placenta-derived markers (follistatin-like-3, placental growth factor, placental exosomes).Citation105,Citation106 However, to convert the findings from observational studies of these biomarkers to clinical practice, strategies that use first-trimester biomarkers to avoid additional screening for GDM should be examined for effects on outcomes and costs.
Screening After Bariatric Surgery
Bariatric surgery (BS) is an effective way to reduce the risk for GDM in obese women.Citation107 Nevertheless, women often remain overweight after BS and the risk to develop GDM is generally still higher compared to pregnant women with a normal weight. Therefore, screening for GDM is still required in women with a history of BS. However, the diagnosis of GDM after BS is challenging, since an OGTT can trigger dumping syndromes with serious adverse effects. In addition, wide variations in glucose excursions and reactive hypoglycemia on the OGTT have been reported in pregnant women with a history of BS.Citation108–Citation110 An OGTT is therefore not recommended to use in pregnant women with BS. Guidelines on screening for GDM in women with BS are lacking and there is no evidence that treatment of GDM diagnosed with an OGTT leads to improved pregnancy outcomes in this population.Citation109 A recent narrative reviewCitation111 summarized the results of studies that tested different screening strategies for GDM after BS, and concluded that capillary blood glucose measurements may currently be the most acceptable alternative to the OGTT for screening in pregnancy after BS. They suggested a pragmatic approach in which all pregnant women with a history of BS are screened at 24–28 weeks of pregnancy by recording capillary blood glucose daily before and after meals during 3–7 days. For the diagnostic and intervention glycemic targets, the same treatment targets as recommended by the ADA were proposed (FPG < 5.3 mmol/L, 1h after the meal <7.8 mmol/L or 2h after the meal <6.7 mmol/L). More research is needed to define optimal glycemic targets in this population. In addition, as an alternative to capillary blood glucose measurements, continuous glucose measurement (CGM) should be evaluated for the diagnosis of GDM. Large studies are needed to evaluate the association between glycemic metrics from the CGM with pregnancy outcomes in this population.
Screening in Times of COVID-19
Due to the COVID-19 pandemic, screening for GDM might lead to an increased risk for exposure to the virus. Temporary changes to diagnostic testing procedures for GDM have been recommended. Several large observational studies described how screening for GDM could be organized in a pragmatic way using blood tests and risk calculators ().
Table 6 Screening During the COVID-19 Pandemic
McIntyre et al described how altered diagnostic processes and criteria for GDM during COVID-19 in Australia, Canada and the United Kingdom (UK) would affect GDM frequency and adverse outcomes.Citation112,Citation113 They showed that the COVID-19 diagnostic approaches reduced GDM frequency by 81% in the UK, by 82% in Canada and by 25% in Australia. Missed GDM cases in Canada displayed similar rates of pregnancy complications to those with GDM, while using UK and Australian modifications, the missed GDM group was respectively at slightly and substantially lower risk. Meek et alCitation114 reported that women with hyperglycemia at risk of suboptimal pregnancy outcomes were identified with an RPG ≥ 8.5 mmol/L at 12 weeks, and an FPG ≥ 5.2–5.4 mmol/L or HbA1c ≥5.7% at 28 weeks of pregnancy. They recommended using these easy-to-perform laboratory tests when an OGTT is not possible. Thangaratinam et al suggested to undertake additional tests at booking to detect overt diabetes and identify those at highest risk for GDM.Citation115 At 24 weeks, they recommended to combine FPG with HbA1c to improve the detection rate, since evidence showed that using FPG alone will only pick up about half of all women with GDM, based on NICE or IADPSG criteria. Furthermore, they suggest that lower FPG thresholds consistent with the IADPSG criteria (FPG ≥ 5.1) could be considered if resources allow. In India, the use of a “single test procedure”, consisting of 2h plasma glucose ≥7.8 mmol/L with 75g oral glucose administered to a pregnant woman in the fasting or non-fasting state, without regard to the time of the last meal, is considered most appropriate for screening during the COVID-19 pandemic.Citation116 Italian guidelines recommended that screening for GDM based on risk factors and FPG forms an acceptable alternative if screening with an OGGT cannot be safely performed.Citation117 A French study retrospectively applied in more than 4000 women the seven proposals of the Australian-New Zealand Societies to limit the number of OGTTs during the COVID-19 pandemic.Citation118 In their cohort, the option in which OGTTs would be performed in women without history of HIP and with FPG 4.7–5.0 mmol/L between 22 and 30 weeks of pregnancy, applying universal screening, was preferred. This approach offered a good compromise because it reduced the rate of women undergoing OGTTs by more than 80%, while identifying around 70% of the women with HIP, especially those with the highest risk of adverse outcomes.
Temporarily modified guidelines for GDM screening to limit the number of OGTTs in the context of the COVID-19 pandemic will inevitably lead to underdiagnosing of GDM. A retrospective analysis in almost 2000 women diagnosed with GDM showed that 29% of them had a FPG <4.7 mmol/L and would have been missed applying the temporary ADIPS criteria.Citation119 Based on these data, the cut-off for the FPG required to identify at least 95% of GDM cases would be ≥4.0 mmol/L. Likewise, a retrospective Australian studyCitation120 showed that 25.3% of GDM cases would be missed using the COVID-19 guidelines. A study from the UK examined the differences in detection rate for GDM comparing the methodology recommended by NICE with the temporarily guidelines for screening during COVID-19 pandemic.Citation121 They found that the overall rate of women identified as having GDM decreased from 7.7% to 4.2% and that the COVID-19 regimen failed to detect 57% women identified as GDM.
Considerations
There is an ongoing lack of consensus regarding the screening and diagnostic approaches for GDM, with inconsistencies mainly focusing on the appropriate timing of screening, the screening process (one-step vs two-step), the use of a risk-factor-based approach and the different diagnostic criteria for the OGTT.
Up to date, screening for GDM in early pregnancy remains controversial. Observational studies have shown conflicting results on the effect of screening and treatment of GDM in early pregnancy. Smaller RCTs have also not shown conclusive evidence of the beneficial effect of early screening and treatment of GDM. Evidence from large RCTs is needed to evaluate whether early treatment has a positive effect on maternal and neonatal outcomes, without an increased risk for harm such as a higher rate of SGA infants. Awaiting the results of several large ongoing RCTs, screening and treatment of GDM before 24–28 weeks of gestation is currently not recommended in our center.Citation87 Instead, a pragmatic approach is proposed for women diagnosed with mild hyperglycemia (FPG 5.5–6.9 mmol/L) in early pregnancy. These women are not labeled as early GDM, but we advise a follow-up with a dietician early in pregnancy and provide screening for GDM with a 75g OGTT and IAPDSG criteria at 24 weeks of pregnancy.Citation87 Moreover, there is no clear consensus on which criteria should be used to define GDM in early pregnancy. Several studies have shown that FPG and HbA1c in early pregnancy are a poor predictor for GDM later in pregnancy because of low sensitivity. However, they could still be useful in simplifying the algorithm for GDM screening later in pregnancy.
The debate on the most appropriate screening strategy for GDM at 24–28 weeks of pregnancy is also ongoing. Implementing the one-step IADPSG screening strategy often leads to an important increase in the prevalence of GDM, without conclusive evidence regarding the benefits on pregnancy outcomes compared to a two-step screening strategy with GCT. Adequately powered RCTs are also needed to investigate the impact of prevention and treatment of GDM diagnosed with IADPSG criteria on long-term maternal and childhood outcomes. In several guidelines, selective screening for GDM is still applied, using a risk-factor-based approach or a two-step screening strategy with a GCT to limit the number of required OGTTs. However, most studies reported significant numbers of missed GDM cased when implementing a risk-factor-based approach, with conflicting results regarding the impact on pregnancy outcomes. Another potential selective screening approach is the two-step screening strategy with a GCT. This approach has the potential to reduce the need of an OGTT, but evidence has shown that the threshold of the GCT should be lowered to 7.2 mmol/L to reach an acceptable sensitivity when using the IADPSG criteria. Other additional screening methods such as FPG or HbA1c often lack sensitivity and/or specificity to be used as the only diagnostic test, but could be helpful as screening test in association with diagnostic tests. In conclusion, the choice between universal and selective screening often depends on the organization of prenatal care, the characteristics of the pregnant population, and the resources of the country, which differ widely internationally.
In pregnant women with bariatric surgery, capillary blood glucose measurements may currently be the most acceptable alternative to the OGTT for GDM screening. The lack of specific guidelines regarding the screening and management of GDM in women with bariatric surgery highlights the need for more research for a better understanding of how to define and treat dysglycemia in a pregnancy after bariatric surgery.
Since 2020, the COVID-19 pandemic is having a major impact on health care delivery, including the screening processes for GDM and overt diabetes in pregnancy. OGTTs could often not be performed since they involve high risk of exposure and an increased burden on health services. Several guidelines have proposed a pragmatic approach to screen for GDM with HbA1c, FPG or even RPG as an alternative during the COVID-19 pandemic. However, usual guidelines and care should be resumed as soon as the COVID pandemic is controlled.
We performed an extensive narrative review including data from 87 observational studies and RCTs on screening and diagnosing of GDM. We covered several controversial areas, including screening and diagnostic approaches for GDM in early and late pregnancy, after bariatric surgery and in pandemic times such as COVID-19. However, we did not perform a systematic review and could therefore not perform a meta-analysis. We could therefore also not assess the risk of bias of individual studies and did not contact the authors for obtaining missing and unpublished data.
Author Contributions
All authors in this paper made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Acknowledgments
CM has a PhD Fellowship Strategic Basic Research of the Research Foundation – Flanders (FWO). KB (Katrien Benhalima) is the recipient of “Fundamenteel Klinisch Navorserschap FWO Vlaanderen”.
Disclosure
The authors declare no conflict of interest.
Additional information
Funding
References
- American Diabetes Association. Standards of medical care in diabetes-2021. Diabetes Care . 2021;44(Suppl. 1):S1–S232. doi:10.2337/dc21-Sint 33298409
- World Health Organization (WHO). Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy . 2013.
- Crowther CA , Hiller JE , Moss JR , McPhee AJ , Jeffries WS , Robinson JS . Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N Engl J Med . 2005;352(24):2477–2486. doi:10.1056/NEJMoa042973 15951574
- Landon MB , Spong CY , Thom E , et al. A multicenter, randomized trial of treatment for mild gestational diabetes. N Engl J Med . 2009;361(14):1339–1348. doi:10.1056/NEJMoa0902430 19797280
- Benhalima K , Lens K , Bosteels J , Chantal M . The risk for glucose intolerance after gestational diabetes mellitus since the introduction of the IADPSG criteria: a systematic review and meta-analysis. J Clin Med . 2019;8(9):1431. doi:10.3390/jcm8091431
- Bellamy L , Casas JP , Hingorani AD , Williams D . Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet . 2009;373(9677):1773–1779. doi:10.1016/S0140-6736(09)60731-5 19465232
- Grunnet LG , Hansen S , Hjort L , et al. Adiposity, dysmetabolic traits, and earlier onset of female puberty in adolescent offspring of women with gestational diabetes mellitus: a clinical study within the Danish national birth cohort. Diabetes Care . 2017;40(12):1746–1755. doi:10.2337/dc17-0514 29038315
- O’sullivan JB , Mahan CM . Criteria for oral glucose tolerance test in pregnancy. Diabetes . 1964;13:278–285.14166677
- Carpenter MW , Coustan DR . Criteria for screening tests for gestational diabetes. Am J Obstet Gynecol . 1982;144(7):768–773. doi:10.1016/0002-9378(82)90349-0 7148898
- Metzger BE , Buchanan TA , Coustan DR , et al. Summary and recommendations of the fifth international workshop-conference on gestational diabetes mellitus. Diabetes Care . 2007;30(2):251–260. doi:10.2337/dc07-s225
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care . 2010;33(3):676–682. doi:10.2337/dc09-1848 20190296
- HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med . 2008;358(19):1991–2002. doi:10.1056/NEJMoa0707943 18463375
- Li-Zhen L , Yun X , Xiao-Dong Z , et al. Evaluation of guidelines on the screening and diagnosis of gestational diabetes mellitus: systematic review. BMJ Open . 2019;9::e023014. doi:10.1136/bmjopen-2018-023014
- Benhalima K , Mathieu C , Van Assche A , et al. Survey by the European Board and College of Obstetrics and Gynaecology on screening for gestational diabetes in Europe. Eur J Obstet Gynecol Reprod Biol . 2016;201:197–202. doi:10.1016/j.ejogrb.2016.04.003 27129745
- Cosson E , Vicaut E , Berkane N , et al. Prognosis associated with initial care of increased fasting glucose in early pregnancy: a retrospective study. Diabetes Metab . 2020.
- Bartha JL , Martinez-Del-Fresno P , Comino-Delgado R . Early diagnosis of gestational diabetes mellitus and prevention of diabetes-related complications. Eur J Obstet Gynecol Reprod Biol . 2002;109(1):41–44. doi:10.1016/S0301-2115(02)00480-3
- Liu B , Cai J , Xu Y , et al. Early diagnosed gestational diabetes mellitus is associated with adverse pregnancy outcomes: a prospective cohort study. J Clin Endocrinol Metab . 2020;105(12):e4264–e4274. doi:10.1210/clinem/dgaa633
- Ryan DK , Haddow L , Ramaesh A , et al. Early screening and treatment of gestational diabetes in high-risk women improves maternal and neonatal outcomes: a retrospective clinical audit. Diabetes Res Clin Pract . 2018;144:294–301. doi:10.1016/j.diabres.2018.09.013 30244050
- Bianchi C , de Gennaro G , Romano M , et al. Early vs. standard screening and treatment of gestational diabetes in high-risk women - an attempt to determine relative advantages and disadvantages. Nutr Metab Cardiovasc Dis . 2019;29(6):598–603. doi:10.1016/j.numecd.2019.02.007 30954416
- Alunni ML , Roeder HA , Moore TR , Ramos GA . First trimester gestational diabetes screening - change in incidence and pharmacotherapy need. Diabetes Res Clin Pract . 2015;109(1):135–140. doi:10.1016/j.diabres.2015.04.027 25958098
- Hong WY , Biggio JR , Tita A , Harper LM . Impact of early screening for gestational diabetes on perinatal outcomes in high-risk women. Am J Perinatol . 2016;33(8):758–764. doi:10.1055/s-0036-1571317 26890436
- Hosseini E , Janghorbani M , Shahshahan Z . Comparison of risk factors and pregnancy outcomes of gestational diabetes mellitus diagnosed during early and late pregnancy. Midwifery . 2018;66:64–69. doi:10.1016/j.midw.2018.07.017 30130677
- Harreiter J , Simmons D , Desoye G , et al. IADPSG and WHO 2013 gestational diabetes mellitus criteria identify obese women with marked insulin resistance in early pregnancy. Diabetes Care . 2016;39(7):e90–e92. doi:10.2337/dc16-0200 27208336
- Hughes RCE , Rowan J , Williman J , Ruth D , Hughes CE . Prediabetes in pregnancy, can early intervention improve outcomes? A feasibility study for a parallel randomised clinical trial. BMJ Open . 2018;8(3):18493. doi:10.1136/bmjopen-2017-018493
- Simmons D , Hague WM , Teede HJ , et al. Hyperglycaemia in early pregnancy: the treatment of booking gestational diabetes mellitus (TOBOGM) Study. A randomised controlled trial. Med J Aust . 2018;209(9):405–406. doi:10.5694/mja17.01129 29793404
- The effect of early screening and intervention for gestational diabetes mellitus on pregnancy outcomes. Available from: https://clinicaltrials.gov/ct2/show/NCT03523143. Accessed 3 30, 2021.
- Osmundson SS , Norton ME , El-Sayed YY , Carter S , Faig JC , Kitzmiller JL . Early screening and treatment of women with prediabetes: a randomized controlled trial. Am J Perinatol . 2016;33(2):172–179. doi:10.1055/s-0035-1563715 26344009
- Simmons D , Nema J , Parton C , et al. The treatment of booking gestational diabetes mellitus (TOBOGM) pilot randomised controlled trial. BMC Pregnancy Childbirth . 2018;18(1):151. doi:10.1186/s12884-018-1809-y 29747594
- Harper LM , Jauk V , Longo S , Biggio JR , Szychowski JM , Tita AT . Early gestational diabetes screening in obese women: a randomized controlled trial. Am J Obstet Gynecol . 2020;222(5):495.e1–495.e8. doi:10.1016/j.ajog.2019.12.021
- Vinter CA , Tanvig MH , Christensen MH , et al. Lifestyle intervention in Danish obese pregnant women with early gestational diabetes mellitus according to WHO 2013 criteria does not change pregnancy outcomes: results from the LiP (Lifestyle in Pregnancy) Study. Diabetes Care . 2018;41(10):2079–2085. doi:10.2337/dc18-0808 30061318
- Roeder HA , Moore TR , Wolfson MT , Gamst AC , Ramos GA . Treating hyperglycemia in early pregnancy: a randomized controlled trial. Am J Obstet Gynecol . 2019;1(1):33–41.
- Riskin-Mashiah S , Younes G , Damti A , Auslender R . First-trimester fasting hyperglycemia and adverse pregnancy outcomes. Diabetes Care . 2009;32(9):1639–1643. doi:10.2337/dc09-0688 19549728
- Benhalima K , Van Crombrugge P , Moyson C , et al. Women with mild fasting hyperglycemia in early pregnancy have more neonatal intensive care admissions. J Clin Endocrinol Metab . 2021;106(2):e836–e854. doi:10.1210/clinem/dgaa831 33180931
- Zhu WW , Yang HX , Wei YM , et al. Evaluation of the value of fasting plasma glucose in the first prenatal visit to diagnose gestational diabetes mellitus in china. Diabetes Care . 2013;36(3):586–590. doi:10.2337/dc12-1157 23193214
- Mañe L , Flores-le Roux JA , Benaiges D , et al. Role of first-trimester HbA1c as a predictor of adverse obstetric outcomes in a multiethnic cohort. J Clin Endocrinol Metab . 2017;102(2):390–397. doi:10.1210/jc.2016-2581 27880069
- Benaiges D , Flores-le Roux JA , Marcelo I , et al. Is first-trimester HbA1c useful in the diagnosis of gestational diabetes? Diabetes Res Clin Pract . 2017;133:85–91. doi:10.1016/j.diabres.2017.08.019 28918341
- Boe B , Barbour LA , Allshouse AA , Heyborne KD . Universal early pregnancy glycosylated hemoglobin A1c as an adjunct to Carpenter-Coustan screening: an Observational Cohort Study. Am J Obstet Gynecol . 2019;1(1):24–32.
- Punnose J , Malhotra RK , Sukhija K , Mathew A , Sharma A , Choudhary N . Glycated haemoglobin in the first trimester: a predictor of gestational diabetes mellitus in pregnant Asian Indian women. Diabetes Res Clin Pract . 2020;159:107953. doi:10.1016/j.diabres.2019.107953 31794807
- Sweeting AN , Ross GP , Hyett J , et al. Baseline HbA1c to identify high-risk gestational diabetes: utility in early vs standard gestational diabetes. J Clin Endocrinol Metab . 2017;102(1):150–156. doi:10.1210/jc.2016-2951 27797673
- van Leeuwen M , Opmeer B , Zweers E , et al. Estimating the risk of gestational diabetes mellitus: a clinical prediction model based on patient characteristics and medical history. BJOG an Int J Obstet Gynaecol . 2010;117(1):69–75. doi:10.1111/j.1471-0528.2009.02425.x
- Teede HJ , Harrison CL , Teh WT , Paul E , Allan CA . Gestational diabetes: development of an early risk prediction tool to facilitate opportunities for prevention. Aust N Z J Obstet Gynaecol . 2011;51(6):499–504. doi:10.1111/j.1479-828X.2011.01356.x 21951203
- Benhalima K , Van Crombrugge P , Moyson C , et al. Estimating the risk of gestational diabetes mellitus based on the 2013 WHO criteria: a prediction model based on clinical and biochemical variables in early pregnancy. Acta Diabetol . 2020;57(6):661–671. doi:10.1007/s00592-019-01469-5 31915927
- Huhn EA , Massaro N , Streckeisen S , et al. Fourfold increase in prevalence of gestational diabetes mellitus after adoption of the new international association of diabetes and pregnancy study groups (IADPSG) criteria. J Perinat Med . 2017;45(3):359–366. doi:10.1515/jpm-2016-0099 27508951
- Adam S , Rheeder P . Screening for gestational diabetes mellitus in a South African population: prevalence, comparison of diagnostic criteria and the role of risk factors. S Afr Med J . 2017;107(6):523–527. doi:10.7196/SAMJ.2017.v107i6.12043 28604326
- Agarwal MM , Dhatt GS , Shah SM . Gestational diabetes mellitus: simplifying the international association of diabetes and pregnancy diagnostic algorithm using fasting plasma glucose. Diabetes Care . 2010;33(9):2018–2020. doi:10.2337/dc10-0572 20519664
- Luewan S , Bootchaingam P , Tongsong T . Comparison of the screening tests for gestational diabetes mellitus between “one-step” and “two-step” methods among Thai pregnant women. Obstet Gynaecol Int . 2018;2018:1521794.
- Meloncelli NJL , Barnett AG , D’Emden M , De Jersey SJ . Effects of changing diagnostic criteria for gestational diabetes mellitus in Queensland, Australia. Obstet Gynaecol . 2020;135(5):1215–1221. doi:10.1097/AOG.0000000000003790
- Waters TP , Dyer AR , Scholtens DM , et al. Maternal and neonatal morbidity for women who would be added to the diagnosis of GDM using IADPSG criteria: a secondary analysis of the hyperglycemia and adverse pregnancy outcome study. Diabetes Care . 2016;39(12):2204–2210. doi:10.2337/dc16-1194 27634392
- Rajput R , Yadav Y, Rajput M , Nanda S . Utility of HbA 1c for diagnosis of gestational diabetes mellitus. Diabetes Res Clin Pract . 2012;98(1):104–107. doi:10.1016/j.diabres.2012.02.018 22456454
- Fuller KP , Borgida AF . Gestational diabetes mellitus screening using the one-step versus two-step method in a high-risk practice. Clin Diabetes . 2014;32(4):148–150. doi:10.2337/diaclin.32.4.148 25646939
- Costa E , Kirckpartick C , Gerday C , et al. Change in prevalence of gestational diabetes and obstetric complications when applying IADPSG screening criteria in a Belgian French speaking University Hospital. A Retrospective Cohort Study. BMC Pregnancy Childbirth . 2019;19(1):249. doi:10.1186/s12884-019-2406-4 31311547
- Feldman RK , Tieu RS , Yasumura L . Gestational diabetes screening: the international association of the diabetes and pregnancy study groups compared with Carpenter-Coustan screening. Obstet Gynaecol . 2016;127(1):10–17. doi:10.1097/AOG.0000000000001132
- March MI , Modest AM , Ralston SJ , Hacker MR , Gupta M , Brown FM . The effect of adopting the IADPSG screening guidelines on the risk profile and outcomes of the gestational diabetes population. J Matern Fetal Neonatal Med . 2016;29(7):1141–1145. doi:10.3109/14767058.2015.1038513 25958989
- Pocobelli G , Yu O , Fuller S , et al. One-step approach to identifying gestational diabetes mellitus: association with perinatal outcomes. Obstet Gynaecol . 2018;132(4):859–867. doi:10.1097/AOG.0000000000002780
- Goedegebure EAR , Koning SH , Hoogenberg K , et al. Pregnancy outcomes in women with gestational diabetes mellitus diagnosed according to the WHO-2013 and WHO-1999 diagnostic criteria: a multicentre retrospective cohort study. BMC Pregnancy Childbirth . 2018;18(1). doi:10.1186/s12884-018-1810-5
- Duran A , Śaenz S , Torrejon MJ , et al. Introduction of IADPSG criteria for the screening and diagnosis of gestational diabetes mellitus results in improved pregnancy outcomes at a lower cost in a large cohort of pregnant women: the St. Carlos Gestational Diabetes Study. Diabetes Care . 2014;37(9):2442–2450. doi:10.2337/dc14-0179 24947793
- Cade TJ , Polyakov A , Brennecke SP . Implications of the introduction of new criteria for the diagnosis of gestational diabetes: a health outcome and cost of care analysis. BMJ Open . 2019;9(1):e023293. doi:10.1136/bmjopen-2018-023293
- Hung TH , Hsieh TT . The effects of implementing the international association of diabetes and pregnancy study groups criteria for diagnosing gestational diabetes on maternal and neonatal outcomes. PLoS One . 2015;10(3):e0122261. doi:10.1371/journal.pone.0122261 25756838
- Benhalima K , Hanssens M , Devlieger R , Verhaeghe J , Mathieu C . Analysis of pregnancy outcomes using the new IADPSG recommendation compared with the Carpenter and Coustan criteria in an area with a low prevalence of gestational diabetes. Int J Endocrinol . 2013;2013:1–6. doi:10.1155/2013/248121
- Meek CL , Lewis HB , Patient C , Murphy HR , Simmons D . Diagnosis of gestational diabetes mellitus: falling through the net. Diabetologia . 2015;58(9):2003–2012. doi:10.1007/s00125-015-3647-z 26071759
- Mirzamoradi M , Bakhtiyari M , Kimiaee P , Hosseini-Najarkolaei A , Mansournia MA . Investigating the effects of treatment based on single high blood glucose in gestational diabetes screening on maternal and neonatal complications. Arch Gynecol Obstet . 2015;292(3):687–695. doi:10.1007/s00404-015-3670-9 25753159
- Satodiya M , Takkar N , Goel P , Kaur J . Comparison of one-step versus two-step screening for diagnosis of GDM in Indian population: a randomized controlled trial. J Obstet Gynaecol India . 2017;67(3):190–195. doi:10.1007/s13224-016-0955-2 28546666
- Hillier TA , Pedula KL , Ogasawara KK , et al. A pragmatic, randomized clinical trial of gestational diabetes screening. N Engl J Med . 2021;384(10):895–904. doi:10.1056/NEJMoa2026028 33704936
- Fadl H , Saeedi M , Montgomery S , et al. Changing diagnostic criteria for gestational diabetes in Sweden - a stepped wedge national cluster randomised controlled trial - The CDC4G Study protocol. BMC Pregnancy Childbirth . 2019;19(1). doi:10.1186/s12884-019-2547-5
- Abebe KZ , Scifres C , Simhan HN , et al. Comparison of two screening strategies for gestational diabetes (GDM(2)) trial: design and rationale. Contemp Clin Trials . 2017;62:43–49. doi:10.1016/j.cct.2017.08.012 28823926
- Lowe WL , Scholtens DM , Lowe LP , et al. Association of gestational diabetes with maternal disorders of glucose metabolism and childhood adiposity. J Am Med Assoc . 2018;320(10):1005–1016. doi:10.1001/jama.2018.11628
- Lowe WL , Lowe LP , Kuang A , et al. Maternal glucose levels during pregnancy and childhood adiposity in the hyperglycemia and adverse pregnancy outcome follow-up study on behalf of the HAPO follow-up study cooperative research group HHS public access. Diabetologia . 2019;62(4):598–610. doi:10.1007/s00125-018-4809-6 30648193
- Lowe WL , Scholtens DM , Kuang A , et al. Hyperglycemia and adverse pregnancy outcome follow-up study (HAPO FUS): maternal gestational diabetes mellitus and childhood glucose metabolism. Diabetes Care . 2019;42(3):372–380. doi:10.2337/dc18-1646 30655380
- NICE Guideline. Diabetes in pregnancy: management from preconception to the postnatal period. Guidance. NICE. 2015.
- Health Service Executive of Ireland. Guidelines for the management of pre-gestational and gestational diabetes mellitus from preconception to the postnatal period. 2010.
- Le Collège national des gynécologues et obstétriciens français et par la Société francophone du diabète. Recommendations pour la pratique clinique: le diabète gestationnel. 2010.
- Richtlijn van de Nederlands Vereniging voor Obstetrie en Gynaecologie (NVOG) diabetes mellitus en zwangerschap. 2018.
- Benhalima K , Van Crombrugge P , Moyson C , et al. Risk factor screening for gestational diabetes mellitus based on the 2013 WHO criteria. Eur J Endocrinol . 2019;180(6):353–363. doi:10.1530/EJE-19-0117 31120231
- Arora D , Arora R , Sangthong S , Leelaporn W , Sangratanathongchai J . Universal screening of gestational diabetes mellitus: prevalence and diagnostic value of clinical risk factors. J Med Assoc Thai . 2013;96(3):266–271.23539927
- Dahanayaka NJ , Agampodi SB , Ranasinghe OR , et al. Inadequacy of the risk factor based approach to detect gestational diabetes mellitus. Ceylon Med J . 2012;57(1):5–9. doi:10.4038/cmj.v57i1.4193 22453704
- Agbozo F , Abubakari A , Narh C , Jahn A . Accuracy of glycosuria, random blood glucose and risk factors as selective screening tools for gestational diabetes mellitus in comparison with universal diagnosing. BMJ Open Diabetes Res Care . 2018;6(1):e000493. doi:10.1136/bmjdrc-2017-000493
- Cosson E , Benchimol M , Carbillon L , et al. Universal rather than selective screening for gestational diabetes mellitus may improve fetal outcomes. Diabetes Metab . 2006;32(2):140–146. doi:10.1016/S1262-3636(07)70260-4 16735962
- Avalos GE , Owens LA , Dunne F . Applying current screening tools for gestational diabetes mellitus to a European population: is it time for change? Diabetes Care . 2013;36(10):3040–3044. doi:10.2337/dc12-2669 23757431
- Herath HM , Weerarathna TP , Weerasinghe NP . Is risk factor-based screening good enough to detect gestational diabetes mellitus in high-risk pregnant women? A Sri Lankan experience. Int J Prev Med . 2016;7(99).
- Miailhe G , Kayem G , Girard G , Legardeur H. M , Elbrot L . Selective rather than universal screening for gestational diabetes mellitus? Eur J Obstet Gynecol Reprod Biol . 2015;191:95–100. doi:10.1016/j.ejogrb.2015.05.003 26112365
- Olagbuji BN , Atiba AS , Olofinbiyi BA , et al. Prevalence of and risk factors for gestational diabetes using 1999, 2013 WHO and IADPSG criteria upon implementation of a universal one-step screening and diagnostic strategy in a Sub-Saharan African population. Eur J Obstet Gynecol Reprod Biol . 2015;189:27–32. doi:10.1016/j.ejogrb.2015.02.030 25855324
- Matta-Coelho C , Monteiro AM , Fern EV , Pereira ML , Souto SB . Universal vs. risk-factor-based screening for gestational diabetes-an analysis from a 5-year Portuguese cohort. Endocrine . 2019;63(3):507–512. doi:10.1007/s12020-018-1760-8 30255292
- Hod M , Kapur A , Sacks DA , et al. The international federation of gynecology and obstetrics (FIGO) initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care. Int J Gynecol Obstet . 2015;131:173–211.
- Committee on Obstetric Practice. Practice bulletin no. 137: gestational diabetes mellitus. Obstet Gynecol . 2013;122(2 Pt 1):406–416. doi:10.1097/01.AOG.0000433006.09219.f1 23969827
- Vandorsten JP , Dodson WC , Espeland MA , et al. NIH consensus development conference: diagnosing gestational diabetes mellitus. NIH Consens State Sci Statements . 2013;29(1):1–31.23748438
- Kleinwechter H , Schäfer-Graf U , Bührer C , et al. Gestational diabetes mellitus (GDM) diagnosis, therapy and follow-up care: practice guideline of the German diabetes association (DDG) and the German association for gynaecology and obstetrics (DGGG). Exp Clin Endocrinol Diabetes . 2014;122(07):395–405. doi:10.1055/s-0034-1366412 25014091
- Benhalima K , Minschart C , Van CP , et al. The 2019 Flemish consensus on screening for overt diabetes in early pregnancy and screening for gestational diabetes mellitus. Acta Clin Belg . 2019;1–8.
- Donovan L , Hartling L , Muise M , Guthrie A , Vandermeer B , Dryden DM . Screening tests for gestational diabetes: a systematic review for the U.S. preventive services task force. Ann Intern Med . 2013;159(2):115–122. doi:10.7326/0003-4819-159-2-201307160-00657 23712349
- Benhalima K , Van Crombrugge P , Moyson C , et al. The sensitivity and specificity of the glucose challenge test in a universal two-step screening strategy for gestational diabetes mellitus using the 2013 World Health Organization criteria. Diabetes Care . 2018;41(7):e111–e112. doi:10.2337/dc18-0556 29748432
- Dickson LM , Buchmann EJ , van Rensburg C , Norris SA . Fasting plasma glucose and risk factor assessment: comparing sensitivity and specificity in identifying gestational diabetes in urban black African women. S Afr Med J . 2020;110(1):21–26. doi:10.7196/SAMJ.2019.v110i1.14089
- Saeedi M , Hanson U , Simmons D , Fadl H . Characteristics of different risk factors and fasting plasma glucose for identifying GDM when using IADPSG criteria: a cross-sectional study. BMC Pregnancy Childbirth . 2018;18(1):225. doi:10.1186/s12884-018-1875-1 29898685
- Maesa JM , Fern E-RP , Sanchez-Margalet V , Gonzalez-Rodriguez C . Fasting glycemia as screening tool to rule-out gestational diabetes in low-risk population. Clin Lab . 2018;64(4):461–465. doi:10.7754/Clin.Lab.2017.170920 29739067
- Göbl CS , Bozkurt L , Rivic P , et al. A two-step screening algorithm including fasting plasma glucose measurement and a risk estimation model is an accurate strategy for detecting gestational diabetes mellitus. Diabetologia . 2012;55(12):3173–3181. doi:10.1007/s00125-012-2726-7 23001377
- McIntyre HD , Gibbons KS , Lowe J , Oats JJN . Development of a risk engine relating maternal glycemia and body mass index to pregnancy outcomes. Diabetes Res Clin Pract . 2018;139:331–338. doi:10.1016/j.diabres.2018.02.036 29550360
- Cooray SD , Boyle JA , Soldatos G , et al. Protocol for development and validation of a clinical prediction model for adverse pregnancy outcomes in women with gestational diabetes. BMJ Open . 2020;10(11):e038845. doi:10.1136/bmjopen-2020-038845
- Lowe LP , Coustan DR , Metzger BE , et al. Hyperglycemia and adverse pregnancy outcome (HAPO) Study: associations of maternal A1C and glucose with pregnancy outcomes. Diabetes Care . 2012;35(3):574–580. doi:10.2337/dc11-1687 22301123
- Renz PB , Cavagnolli G , Weinert LS , Silveiro SP , Camargo JL . HbA1c test as a tool in the diagnosis of gestational diabetes mellitus. PLoS One . 2015;10(8):e0135989. doi:10.1371/journal.pone.0135989 26292213
- O’Connor C , O’Shea PM , Owens LA , et al. Trimester-specific reference intervals for haemoglobin A1c (HbA1c) in pregnancy. Clin Chem Lab Med . 2012;50(5):905–909. doi:10.1515/cclm.2011.397
- Khalafallah A , Phuah E , Al-Barazan AM , et al. Glycosylated haemoglobin for screening and diagnosis of gestational diabetes mellitus. BMJ Open . 2016;6(4):e011059. doi:10.1136/bmjopen-2016-011059
- Odsaeter IH , Åsberg A , Vanky E , et al. Hemoglobin A1c as screening for gestational diabetes mellitus in Nordic Caucasian women. Diabetol Metab Syndr . 2016;8(1):43. doi:10.1186/s13098-016-0168-y 27453735
- Renz PB , Chume FC , Timm JRT , Pimentel AL , Camargo JL . Diagnostic accuracy of glycated hemoglobin for gestational diabetes mellitus: a systematic review and meta-analysis. Clin Chem Lab Med . 2019;57(10):1435–1449. doi:10.1515/cclm-2018-1191 30893053
- Ghosh P , Luque-Fernandez MA , Vaidya A , et al. Plasma glycated CD59, a novel biomarker for detection of pregnancy-induced glucose intolerance. Diabetes Care . 2017;40(7):981–984. doi:10.2337/dc16-2598 28450368
- Ma DD , Luque-Fernandez MA , Bogdanet D , Desoye G , Dunne F , Halperin JA . Plasma glycated CD59 predicts early gestational diabetes and large for gestational age newborns. J Clin Endocrinol Metab . 2020;105(4):E1033–E1040. doi:10.1210/clinem/dgaa087
- Bogdanet D , O’Shea PM , Halperin J , Dunne F . Plasma glycated CD59 (gCD59), a novel biomarker for the diagnosis, management and follow up of women with Gestational Diabetes (GDM) - protocol for prospective cohort study. BMC Pregnancy Childbirth . 2020;20(1):412. doi:10.1186/s12884-020-03090-9 32682411
- Powe CE . Early pregnancy biochemical predictors of gestational diabetes mellitus. Curr Diab Rep . 2017;17(2):12. doi:10.1007/s11892-017-0834-y 28229385
- Faal S , Abedi P , Jahanfar S , et al. Sex hormone binding globulin for prediction of gestational diabetes mellitus in pre-conception and pregnancy: a systematic review. Diabetes Res Clin Pract . 2019;152:39–52. doi:10.1016/j.diabres.2019.04.028 31063851
- Kwong W , Tomlinson G , Feig DS . Maternal and neonatal outcomes after bariatric surgery; a systematic review and meta-analysis: do the benefits outweigh the risks? Am J Obstet Gynecol . 2018;218(6):573–580. doi:10.1016/j.ajog.2018.02.003 29454871
- Feichtinger M , Stopp T , Hofmann S , et al. Altered glucose profiles and risk for hypoglycaemia during oral glucose tolerance testing in pregnancies after gastric bypass surgery. Diabetologia . 2017;60(1):153–157. doi:10.1007/s00125-016-4128-8 27757488
- Freitas C , Araújo C , Caldas R , Lopes DS , Nora M , Monteiro MP . Effect of new criteria on the diagnosis of gestational diabetes in women submitted to gastric bypass. Surg Obes Relat Dis . 2014;10(6):1041–1046. doi:10.1016/j.soard.2014.03.013 25066444
- Rottenstreich A , Elazary R , Ezra Y , Kleinstern G , Beglaibter N , Elchalal U . Hypoglycemia during oral glucose tolerance test among post–bariatric surgery pregnant patients: incidence and perinatal significance. Surg Obes Relat Dis . 2018;14(3):347–353. doi:10.1016/j.soard.2017.11.031 29306610
- Benhalima K , Minschart C , Ceulemans D , et al. Screening and management of gestational diabetes mellitus after bariatric surgery. Nutrients . 2018;10(10):1479. doi:10.3390/nu10101479
- McIntyre HD , Moses RG . The diagnosis and management of gestational diabetes mellitus in the context of the COVID-19 pandemic. Diabetes Care . 2020;43(7):1433–1434. doi:10.2337/dci20-0026 32409503
- McIntyre HD , Gibbons KS , Ma RCW , et al. Testing for gestational diabetes during the COVID-19 pandemic. An evaluation of proposed protocols for the United Kingdom, Canada and Australia. Diabetes Res Clin Pract . 2020;167:108353. doi:10.1016/j.diabres.2020.108353 32739381
- Meek CL , Lindsay RS , Scott EM , et al. Approaches to screening for hyperglycaemia in pregnant women during and after the COVID-19 pandemic. Diabet Med . 2020;38(1):e14380. doi:10.1111/dme.14380 32750184
- Thangaratinam S , Cooray SD , Sukumar N , et al. Endocrinology in the time of COVID-19: diagnosis and management of gestational diabetes mellitus. Eur J Endocrinol . 2020;183(2):G49–g56. doi:10.1530/EJE-20-0401 32454456
- Seshiah V , Balaji V , Banerjee S . et al. Diagnosis and principles of management of gestational diabetes mellitus in the prevailing COVID-19 pandemic. Int J Diabetes Dev Ctries ;2020. 1–6. doi:10.1007/s13410-020-00860-1
- Torlone E , Festa C , Formoso G , et al. Italian recommendations for the diagnosis of gestational diabetes during COVID-19 pandemic: position statement of the Italian Association of Clinical Diabetologists (AMD) and the Italian Diabetes Society (SID), diabetes, and pregnancy study group. Nutr Metab Cardiovasc Dis . 2020;30(9):1418–1422. doi:10.1016/j.numecd.2020.05.023 32675009
- Nachtergaele C , Vicaut E , Tatulashvili S , et al. Limiting the use of oral glucose tolerance tests to screen for hyperglycemia in pregnancy during pandemics. J Clin Med . 2021;10(3):397. doi:10.3390/jcm10030397 33494289
- van Gemert TE , Moses RG , Pape AV , Morris GJ . Gestational diabetes mellitus testing in the COVID-19 pandemic: the problems with simplifying the diagnostic process. Aust N Z J Obstet Gynaecol . 2020;60(5):671–674. doi:10.1111/ajo.13203 32662072
- Zhu S , Meehan T , Veerasingham M , Sivanesan K . COVID-19 pandemic gestational diabetes screening guidelines: a retrospective study in Australian women. Diabetes Metab Syndr . 2021;15(1):391–395. doi:10.1016/j.dsx.2021.01.021 33571889
- Van-de-l’isle Y , Steer PJ , Watt Coote I , Cauldwell M . Impact of changes to national UK guidance on testing for gestational diabetes screening during a pandemic: a single-centre observational study. BJOG . 2020;128(5):917–920. doi:10.1111/1471-0528.16482 32888369