
Abstract
Diabetes is a chronic illness. Hyperglycemia is the characteristic of this disorder. Diabetes is a global crisis which affects the economy and health of all nations. Over the last decades, the number of individuals living with diabetes has significantly increased worldwide. Asia is a key epicenter of the emerging diabetes epidemic, with China and India the two nations having the highest number of diabetic people. Economic development, modernization, unhealthy diet, population aging, and sedentary lifestyles are the major factors responsible for the increasing diabetes epidemic. Diabetes is associated with several complications, and cardiovascular disease is the most important cause of morbidity and mortality among people with diabetes. These life-threatening problems can be prevented or delayed by proper management of diabetes. Lifestyle modification is an important factor to decrease the diabetes risk. The frequency of diabetic complications will rise if there is a lack of cost-effective and sustainable interventions. Hence, prevention of diabetes and its complications such as diabetic retinopathy and cardiovascular disease should be a crucial part of all future health-related public policies among all nations. This review summarizes current epidemiological aspects of diabetes in the world along with its complications, preventive measures, and treatment.
Introduction
Diabetes is a chronic disorder where the human body cannot secrete any insulin hormone or produces ineffective or insufficient insulin, which causes an increase in blood glucose levels. The pancreas gland secretes insulin hormone, and it transports glucose from blood to cells where glucose is broken down in the presence of oxygen. Insufficient insulin or incapability to effectively respond to insulin causes hyperglycemia or high blood sugar levels, which is the hallmark sign of diabetes. Unchecked hyperglycemia for a long time period can cause damage to several body organs which leads to critical health problems such as nephropathy, neuropathy, retinopathy and heart-related disease. These life-threatening problems can be prevented or delayed by proper management of diabetes.Citation1 According to the International Diabetes Federation (IDF), approximately 463 million people (ages 20–79 years) were living with diabetes worldwide in 2019. This age group represents 9.3% of the world population. This number is projected to rise to 578 and 700 million by 2030 and 2045, respectively, and the biggest rises will occur in the areas where economies are moving from low- to middle-income status. Economic development, modernization, unhealthy diet intake, population aging and sedentary lifestyles are the major factors responsible for the increasing diabetes epidemic.Citation2,Citation3 In this review, we discuss the classification and world picture of diabetes. We then describe the prevalence, incidence and complications of diabetes. We also discuss recommendations from various studies for preventing diabetes.
Diagnosis and Classification of Diabetes
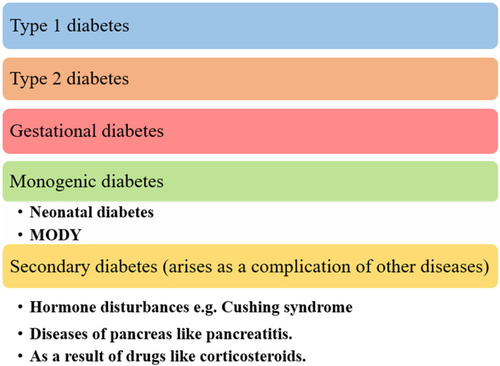
Diabetes has been mainly classified into three types: type 1 diabetes (T1D), type 2 diabetes (T2D) and gestational diabetes (GD). Monogenic diabetes and secondary diabetes are less common forms of diabetes ().Citation4 T1D results from the destruction of insulin-secreting pancreatic beta-cells which results in a complete deficiency of insulin. An interaction of genetic susceptibility and environmental agents (such as toxins, viral infections, or a few dietary elements) has been implicated in triggering this destructive process. T1D can develop at any age but is mostly seen in adolescents and children. Almost 90% of all cases of diabetes belong to T2D. T2D is mostly found in middle-aged individuals and incidence in children and, young adults has increased in recent times due to increasing levels of unhealthy eating habits, obesity, and sedentary lifestyle. T2D is characterized by hyperglycemia linked to inability to adequately respond to insulin. However, the specific etiologies of the disease are unknown. Gestational diabetes usually occurs during the 2nd or 3rd trimester of pregnancy. However, it can affect at any time of pregnancy. First-diagnosed high blood glucose level during pregnancy is categorized as GD or hyperglycemia in pregnancy. During pregnancy, GD accounts for about 75–90% of all incidents of high sugar levels. GD arises because of insulin resistance due to production of placental hormones. An autosomal dominant mutation in a single gene causes monogenic diabetes. Neonatal diabetes and maturity onset diabetes of young (MODY) conditions are examples of monogenic diabetes. Hyperglycemia onset at an early age or before 25 years of age is characteristic of MODY. However, MODY can occur at older ages as well. When diabetes is diagnosed within the first six months of life it is called congenital or neonatal diabetes. Secondary diabetes occurs due to other disease complications including due to drugs (corticosteroids), pancreatic disease (pancreatitis) or hormonal disturbances (Cushing syndrome).Citation5–Citation7 Blurred vision, frequent urination, tiredness, and excessive thirst are common T1D and T2D symptoms. Among other symptoms, persistent fungal infections in skin, numbness in feet and hands and slow healing wounds are some specific T2D symptoms.Citation4 Symptoms of hyperglycemia in pregnancy are not clear and it is hard to differentiate them from usual pregnancy signs and symptoms.Citation2 Diabetes can be diagnosed by observing increased glucose levels in blood. For diagnosing diabetes, 2-h plasma glucose (2-h PG) value or fasting plasma glucose (FPG) value is observed during the 75-g glucose tolerance test. Diabetes can also be diagnosed by a glycated hemoglobin (HbA1c) test (). In absence of symptoms of hyperglycemia, if one lab test result comes between the range of diabetes, a repeat confirmatory lab test (FPG, 2-h PG, HbA1c in 75-g OGTT) should be done on the next day.Citation8 However, the actual time of T2D onset is hard to determine. Consequently, about 1/3rd cases of type 2 diabetes may not be diagnosed as people do not show any symptoms for years. When remaining undiagnosed for many years, chronic hyperglycemic complications may arise. In some T2D patients, it is diagnosed when long-term hyperglycemic problems arise such as foot ulcers, kidney infection, kidney failure, and vision loss.Citation4,Citation7,Citation9 The etiology of T2D is not completely understood but significant linkage of T2D with increasing weight and age and history in the family has been reported. Physical inactivity, high intake of sugar-sweetened beverages and low-intake of high fibre food, depression, race/ethnicity, smoking, prediabetes, and complications associated with polycystic ovary syndrome (PCOS), hypertension or dyslipidemia are some key risk factors involved in T2D development.Citation9 Excessive weight gain in pregnancy, PCOS, obesity, continuing smoking, family history of diabetes, older age are some risk factors of gestational diabetes.Citation2
Table 1 Diagnosis of Diabetes
Figure 1 Classification of diabetes.
Key factors in T2D development are modern lifestyle and urbanization which include unhealthy diet intake and sedentary lifestyle. Several studies have confirmed that modification in lifestyle and healthier diet can prevent or delay T2D onset.Citation10 Studies have also demonstrated that diabetes risk is not completely attributed to genetic factors. A study found that in Pima Indians, newborns of mothers with GD were at 3.7 times more risk in developing diabetes and obesity compared with newborns with healthy mothers.Citation11 Therefore, there is a need to focus on fetal diet during the prenatal period and in early life years.Citation12
Diabetes as an Epidemic
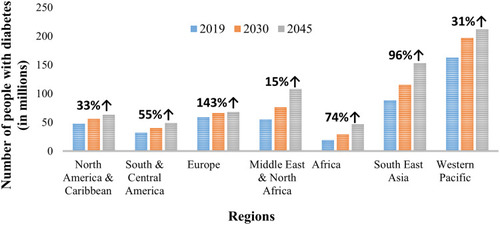
In 1994, the IDF reported that over 100 million individuals had diabetes and projected that this number will increase in future decades across the world.Citation13 Recent studies projected that by 2045 about 700 million adults (ages 20–79 years) which will be 10.9% of the world’s adult population will have diabetes ().Citation2 A National Diabetic Statistic report revealed that about 30 million individuals were living with diabetes in 2015 and around 23% of these individuals were projected to be undiagnosed.Citation7
Figure 2 Number of people with diabetes globally in 2019, 2030 and 2045 (in millions).
Global Situation
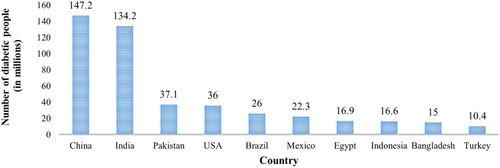
In 2019, 9.3% of the world’s adults (ages 20–79 years) had diabetes. This represents 463 million people and this number is more than the number predicted by the World Health Organization (WHO) in 2014.Citation2,Citation14 The IDF provided data of 10 nations worldwide with the most diabetic patients in 2019 () and predicted the top nations with most diabetic patients by 2030 and 2045 ( and ). Out of all the top countries, four countries in 2019, 2030 and five countries in 2045 are from Asia.Citation2 Due to rapid urbanization, modernization and economic development, Asia will become the epicenter of world diabetes epidemic.Citation15 These factors are also causing significant increase in the number of people with diabetes among Gulf countries of the Middle East.Citation16 The highest diabetes prevalence was observed in developing countries instead of developed nations. About 80% of diabetic patients are living in middle- and low-income societies and nations.Citation17 Most of the people having diabetes in these countries have insufficient treatment resources, which is one more vital challenge in the future.Citation18 Increased premature mortality and morbidity rate will have key economic and social results among these societies and countries.Citation19,Citation20
Figure 3 Number of diabetic people in 2019 (in millions).
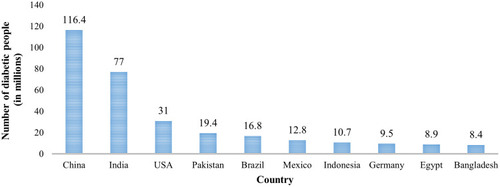
Figure 4 Number of diabetic people by 2030 (in millions).
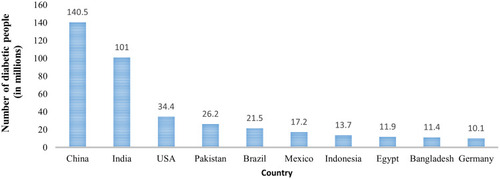
Figure 5 Number of diabetic people by 2045 (in millions).
Challenges in developing countries related to diabetes are different from challenges in developed countries. First, in developing countries health systems are more concerned towards the cure of single diseases, instead of managing several overlapping chronic diseases. Second, the increasing diabetes prevalence is more in younger individuals (ages < 60 years) in developing countries. Diabetes at this age also has an impact on peoples’ work and careers. Third, the indigenous people of developing countries also have a higher number of complications such as coronary artery disease and kidney related disorders in comparison with European white populations.Citation21 The therapeutic research focuses on novel, but costly medicines and millions of diabetes patients in developing countries cannot afford these drugs.Citation22
Diabetes Prevalence by Types of Diabetes
According to IDF, around 1.1 million children and young adults had T1D in 2019 and the number of newly diagnosed cases (ages 0–19 years) each year are 128,900.Citation2 Hyperglycemia during pregnancy (ages 20–49 years) was found in 20.4 million of live births in 2019 which will reduce to 18.3 million by 2030. Current data reported that there are about 373.9 million individuals (ages 20–79 years) with impaired glucose tolerance (IGT) worldwide and it is projected that this number will increase to 453.8 and 548.4 million by 2030 and 2045, respectively.Citation23,Citation24
Diabetes Prevalence by Age and Sex
The diabetes prevalence considerably increases with age.Citation25 According to studies, most diagnosed cases of diabetes are between the 4th and 7th decade of a person’s life. Studies revealed that working age individuals (ages 25–69 years) have more diabetes in comparison with older individuals (ages > 69 years).Citation26 T1D incidence is increasing in children and teenagers (ages < 15 years) in many regions of the world. IDF projected that every year approximately 98,200 children (ages < 15 years) are diagnosed with T1D and it rises to 128,900 when the age group expands to ≤ 19 years.Citation2 Gender plays a vital role in presentation, incidence and management of the disease.Citation27 In 2019, the projected diabetes prevalence was slightly higher in men (9.6%) in comparison with women (9.0%) aged 20—79 years. IDF estimated that approximately 17.2 million more males are diagnosed with diabetes than females. The variation in diabetes prevalence among males and females will be reduced in future as the number is expected to rise to 10.4 and 11.1% in males by 2030 and 2045, respectively and 10 and 10.8% in females by 2030 and 2045, respectively.Citation2
Diabetes Prevalence by Urban and Rural Regions, Income Status
Prevalence of diabetes differs across all countries worldwide. Socioeconomic factors such as modernization, urbanization, industrialization, sedentary lifestyle and migration from rural to urban regions may influence diabetes differently among developing and developed countries. Studies reported that ethnicity plays a vital role in prevalence of diabetes in low-, middle- and high-income countries.Citation28 Diabetes prevalence is maximum in high-income nations (10.4%), followed by middle-income nations (9.5%) and lowest in low-income nations (4%). Although, the diabetes prevalence will rise to 11.9, 11.8 and 4.7% in high-, middle- and low-income nations, respectively.Citation2,Citation24 Urbanization is positively and strongly associated with prevalence of diabetes.Citation29 Previous studies revealed that diabetes has been more frequently reported in urban populations in comparison with rural populations.Citation28 The prevalence of diabetes is higher in urban regions (10.8%) in comparison with rural regions (7.2%).Citation2 Out of all the diabetes patients, 67% of patients are living in urban regions. In 2019, around 310.3 million people living in urban regions had diabetes and it is predicted that this number will increase to 415.4 and 538.8 million by 2030 and 2045, respectively.Citation2,Citation24 Although, a meta-analysis study also found that the diabetes prevalence in rural areas of middle- and low-income nations was increased almost 5 times in 2005–2010 (8.6%) from 1985–1989 (1.8%).Citation30
Trends in Diabetes Incidence
Increase in Diabetes Prevalence
Over decades, the trends of diabetes demonstrate the speed and direction of evolution of the diabetes epidemic. Due to phosphate deposits mining in Nauru region, this island population experienced great wealth which caused changes in their lifestyle and due to modernization their diabetes prevalence increased from nearly 0 (in the 1960s) to 35% by the 1970s.Citation31 The inactive lifestyle of the Nauru population resulted in a substantial increase in prevalence of T2D.Citation32 The T2D prevalence in Nauru was about 50% in 1994. Though the diabetes prevalence in Nauru region was an alert for the worldwide diabetes epidemic in future, the situation in Mauritius was also a sign for the diabetes epidemic across the world.Citation33 A 23-year study of diabetes within different ethnic groups (mainly Asian Indians, Africans and Chinese) of Mauritius showed a growing diabetes prevalence (from 12.8% in 1987 to 23.4% in 2009) due to changes in traditional risk factors such as ethnicity, smoking, circumference of waist, hypertension, family history, body mass index, and age in its population.Citation33 Ethnicity of India and China was similar to Mauritius ethnic groups and in 1990 Dowse and his colleagues predicted that due to globalization and modern lifestyles, diabetes prevalence would grow significantly in coming years in these regions.Citation34 Data from India and Chinese population studies confirmed their prediction.Citation4
The study in India covered a 6-year duration and its data represent the growing diabetes prevalence in rural and urban regions of India from 6.4 and 13.9% to 9.2 and 18.2%, respectively.Citation35 Another study also observed the growing diabetes prevalence in India over a period of time in urban as well as in rural areas.Citation31 IDF Diabetes Atlas 9th edition reported that in 2019, 116.4 million individuals (ages 20–79 years) in China are affected with diabetes and it has more individuals with diabetes in the world in comparison with any other country. Several findings suggested that China is home to the largest number of diabetes patients (ages 20–79 years) in the world, followed by India.Citation2 The diabetes prevalence in China increased substantially in 20 years. In 1980, the diabetes prevalence in China was 0.67%, which increased to 11.6% in 2010.Citation36 In urban areas of China like Qingdao, diabetes prevalence had increased significantly (11.3% to 16.5%) in 5 years (2001–2006). Furthermore, other findings suggested similar growing diabetes prevalence in Chinese rural regions.Citation37 Brazil is another example of the growing prevalence of diabetes over 30 years.Citation38 A comprehensive study in Brazil reported that the diabetes prevalence was 4.7% in 1996, which increased to 10.3% in 2012, a more than 100% increase in a 16-year time period.Citation39 But the country with highest prevalence in 2019 was the Marshall Islands with a 30.5% diabetes prevalence rate followed by Kiribati and Sudan with 22.5 and 22.1% rate of diabetes prevalence, respectively.Citation2 Forouhi et al. (2019) reported that T1D incidence has been increasing with an average increase of approximately 3% per year around the world. The most noticeable rise has been observed in the 0–4 years age group.Citation40 Increase in diabetes prevalence has also been seen in European populations. In only one decade (1995–2005), there was a rise of 69% of prevalence of diabetes in Ontario, Canada.Citation41 Data from the USA demonstrate an annual increase in T2D in youth (ages 10–19 years) of around 5% in 2002–2012.Citation42 Similarly, the GD prevalence is significantly rising, primarily in high risk type 2 diabetes individuals and it may increase the diabetes prevalence worldwide.Citation43
Decrease in Diabetes Prevalence
Due to mining of valuable phosphate deposits, Nauruans became very rich which caused changes in their lifestyle and due to modernization in 1975, the prevalence of diabetes was very high in Nauru.Citation31 The Nauru population had an inactive lifestyle which resulted in a substantial increase in the prevalence of T2D.Citation32 The T2D prevalence in Nauru was about 50% in 1994. After a decade, Nauru’s economy went down, and it became a poor country from being a very rich country, and its diabetes prevalence also reduced.Citation3 Similarly, there was a reduction in prevalence of diabetes in Cuba during an economic crisis.Citation44 These results suggested the impact of socio-economic factors in incidence and prevalence of T2D.Citation3
Diabetes: Global Healthcare Expenditure
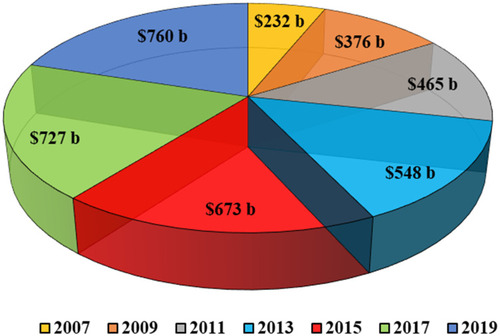
The economic burden of diabetes is huge, and it is expected to continue growing. In 2019, the world’s healthcare expenditure on diabetes was expected to reach $760 billion. It was $232 billion in 2007 and projected to reach $825 billion and $845 billion by 2030 and 2045, respectively ().Citation2,Citation45
Figure 6 World healthcare expenditure (in billion/b) on diabetes (2007–2019).
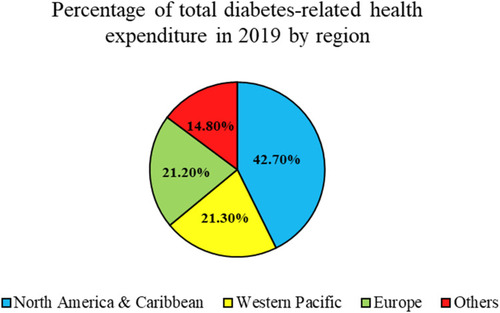
Diabetes-related health expenditure is not the same in different nations. In 2019, Caribbean and North America regions expended about $324.5 billion on diabetes and this was 42.7% of global diabetes care expenditure. These regions had the maximum diabetes care expenditure per individual (ages 20–79 years) while the Southeast Asia region had the least per person diabetes expenditure among all regions. The Middle East, Africa, Southeast Asia and Central-South America regions spent considerably less and altogether contributed only 14.8% of total diabetes care expenditure (). The USA had the highest expenditure in 2019 ($294.6 billion), followed by China and Brazil with $109 billion and $52.3 billion, respectively on diabetes. Tuvalu, Principe and Sao Tome were among the nations with the lowest healthcare expenditure on diabetes.Citation2
Figure 7 Percentage of total diabetes-related health expenditure in 2019 by region.Citation2
Health-care expenditure on diabetes depends on a nation’s income.Citation18 In the USA, health-care expenditure on diabetes increased almost three times from $132 billion (2002) to $327 billion in 2017.Citation46,Citation47 One of the reasons for this rise was the use of expensive and new treatments and medications for diabetes complications. Due to the growing use of costly treatments and medications for diabetes, increase in medical expenditure attributed to diabetes in future is of major concern in developing nations.Citation18
Due to growing prevalence of diabetes, the need for expensive treatments and drugs for diabetes will increase and it will lead to an unsustainable rise in global health-care expenditure. This will be a big challenge in the future for developed as well as developing countries.Citation18 There is a crucial requirement of feasible and cost-effective interventions for prevention of diabetes and its complications to reduce future economic collapse.Citation48
Complications of Diabetes
Diabetes is characterized by hyperglycemia. Long-term hyperglycemia may cause various complications and it is associated with long-term dysfunction, damage and failure of numerous organs, predominantly kidneys, eyes, blood vessels and nerves. Diabetic complications can be chronic (long term) or acute (short term). Chronic complications are characterized by damage to the vascular system and categorized into macrovascular complications (damage to larger blood vessels) and microvascular complications (damage to small blood vessels).Citation49 Diabetic people have a higher risk of developing macrovascular diseases or heart disease. Heart disease is a disorder of the large arteries and an inflammatory process which leads to stroke, peripheral arterial disease and arteriosclerosis.Citation50 Cardiovascular conditions are the leading cause of mortality and morbidity in T1D and T2D patients.Citation51 Risk of heart disease can be decreased by lowering the increased blood pressure and blood glucose levels and by using medications that can lower cholesterol levels in diabetic patients.Citation52 Microvascular complications lead to diabetic retinopathy, neuropathy and nephropathy and they are the key reason for mortality and morbidity in people with diabetes.Citation50 Among all microvascular diseases, diabetic retinopathy (DR) is an extremely complicated disease, and it is one of the important and common causes of visual defect and loss of sight in adults (ages 20–74 years).Citation53 The prevalence of DR is associated with hypertension, level of glycemic control and duration of T1D or T2D. Other risk factors such as nephropathy, chronic hyperglycemia and dyslipidemia are also associated with DR.Citation54 Blindness and visual impairment can be prevented by timely diagnosis and treatment of the DR.Citation2 Diabetic neuropathy may damage the autonomic and peripheral nervous systems and occurs in about 50% of all diabetic patients. Duration of diabetes and HbA1c level are the major risk factors of diabetic neuropathy.Citation55 Peripheral neuropathy in diabetic patients can result from diabetic neuropathy. Peripheral neuropathy damages distal nerves of limbs and typically affects nerves in the feet. This condition encourages the development of ulcers and leads to diabetic foot complications.Citation56,Citation57 Diabetic nephropathy occurs in approximately 25–35% of T1D or T2D patients.Citation58 Both chronic kidney disease and diabetes are linked with CVD and risk related to disease can be reduced by controlling blood pressure and blood glucose levels.Citation2,Citation59 Acute complications of diabetes such as hypoglycemia, hyperglycemic hyperosmolar state (HHS), diabetic ketoacidosis and lactic acidosis are easily preventable but still cause high morbidity and mortality in diabetic patients.Citation60 Diabetes increases the risk of complications in the digestive, musculoskeletal and liver systemsCitation9,Citation61 and in depression and mental health-related problems too.Citation62 Type 2 diabetes might also enhance the risk of liver, pancreas and colorectal cancers.Citation63 Some comorbidities such as obstructive sleep apnea, non-alcoholic fatty liver disease, and oral health diseases are also associated with diabetes.Citation2,Citation9 The consistent characteristic between T1D and T2D is hyperglycemia. Hence, treatment of hyperglycemia would be the prime preventive measure for complications of diabetes.Citation2
Diabetes and Musculoskeletal Disorders
Several muscular and skeletal disorders occur in diabetes. These musculoskeletal disorders can cause function loss and pain and can also restrict the physical exercise programmes to maintain and manage the body weight of diabetes patients.Citation64 Muscle infarction, neuropathic joints, reflex sympathetic dystrophy syndrome, Dupuytren’s contracture, muscle cramps, carpal tunnel syndrome, tenosynovitis, peripheral neuropathy, adhesive capsulitis of the shoulder, diffuse idiopathic skeletal hyperostosis, stiff hands syndrome and loss of deep tendon reflexes are common musculoskeletal effects of diabetes.Citation65 Management and assessment of musculoskeletal disorders among people with diabetes can reduce mortality, morbidity and pain.Citation64
Diabetes and Duchenne Muscular Dystrophy
Duchenne muscular dystrophy (DMD) is an X-linked recessive condition which influences around 1 live-born male out of 3600–6000 live-born males. This disease generally begins early during childhood with delayed motor development and waddling gait.Citation66 For development of diseases like T2D, insulin resistance and hyperinsulinemia are vital risk factors and the incidence of these factors rises (about 80%) when patients with DMD are obese.Citation67
Diabetes and Sarcopenia
Sarcopenia is a syndrome characterized by loss of muscle function and mass and it has been associated as a cause as well as a consequence of T2D.Citation68 Sarcopenia risk is found to be increased among people with T2D. But sarcopenia in senior adults may increase the risk of development of T2D. The Hong et al. study of 89,854 Korean women and 113,913 men (mean age = 40 years) observed that the people with lowest muscle mass related to weight of body quartiles had two-fold more risk of T2D development in comparison with the people in the highest quartile.Citation69 Factors such as inflammation and insulin resistance can influence several muscle health components and reduced health of muscle can cause the progression and development of T2D.Citation68
Diabetic Neuropathic Cachexia
Diabetic neuropathic cachexia (DNC) is a very rare type of diabetic neuropathy with weakly identified pathogenesis. DNC is a condition in which severe weight loss occurs quickly, generally over a period of 3–6 months. This disease is not associated with the duration or the severity of diabetes.Citation70 Mostly cases of DNC start with quite sudden improvement in glycemic control, triggered by insulin initiation. Within a short duration of time, usually some days to weeks, people report serious neuropathic pain, and it is the characteristic feature of this disease.Citation71
Prevention of Diabetes
Mostly countries (especially developed countries) have formed several schemes to tackle type 2 diabetes. Many studies report the clinical efficiency of lifestyle and pharmacologic interventions in prevention of T2D.Citation72 Sustainable effects have been observed in T2D prevention by change in lifestyle, while pharmacologic treatment imitates glucose-lowering therapy.Citation73 Although clinical trials results provide a successful method for prevention of T2D, the success of this idea depends on acceptance of intervention programs among populations.Citation74
Lifestyle intervention prevents or delays T2D onset. Therefore, International Diabetes Federation has given some suggestions for healthy eating plans ().Citation4 Results from long-term follow-up studies in India, Finland, China and the USA showed that lifestyle intervention caused reduction in prevalence of T2D which lasts for some years even after discontinuing the intervention.Citation75–Citation80 Tuomilehto and his colleagues also reported that a 3.2-year intervention in physical activity and diet in a Finnish population resulted in a 58% reduction of T2D risk.Citation72 Moreover, studies suggested that environment of early life and in utero has a significant impact on T2D risk in adulthood. So, there is a need to focus on fetal diet during prenatal period and in early life years.Citation12 But in the case of T1D, while it is possible to manage the disease at present, there is no effective and safe intervention to prevent it.Citation81
Table 2 IDF Recommended Nutritional Diet
In 2017, about 4 million people are projected to die due to diabetes and that is equal to 1 death in every 8 seconds.Citation4 Deaths caused by diabetes are more than the total deaths due to infectious disorders (0.4 million, 1.1 million and 1.8 million deaths from malaria, AIDS and tuberculosis, respectively in 2015).Citation82 Several studies suggested that lifestyle intervention, intensive control of lipid and blood pressure and glycemic management are cost-saving methods in prevention of diabetes.Citation83 The Indian Diabetes Prevention Program (IDPP-1), which was a 3-year randomized control trial, reported that metformin and lifestyle modification helped to prevent T2D in patients with IGT.Citation84 Another 3-year randomized control study, the Diabetes Community Lifestyle Improvement Program (D-CLIP) of 578 obese Asian Indians reported that step by step prevention of diabetes in prediabetic people can efficiently decrease incidence of diabetes.Citation85
Treatment of Diabetes
Healthy lifestyle is the main determinant in diabetes treatment. Physical exercise, food intake, body weight maintenance, quit smoking plan, reduction in alcohol consumption are important factors in maintaining a healthy lifestyle. If change in lifestyle is not enough to control blood glucose levels, then oral medications are used to treat hyperglycemia. Metformin is the most highly used antidiabetic medication in the treatment of T1D and T2D globally. When single oral medication is not enough for the treatment of diabetes, several combination therapies are now present which include SGLT2 inhibitors, amylin analogues, gliptins inhibitors (for T1D and T2D) and sulfonylureas, glitazones, GLP-1R agonists, AG inhibitors, dopamine agonists (for T2D). In cases where oral drugs are not able to regulate hyperglycemia, injections of insulin may be advised. Along with blood glucose level, it is important to control blood pressure. With the management of lifestyle and medications, people with diabetes can live long and healthy lives.Citation86,Citation87
Therapeutic Intervention of Phytochemicals in Diabetes
In the last few years, use of traditional or conventional medicines has received considerable recognition around the globe. Several varieties of conventional medicines have been used such as Unani medicines, conventional Chinese medicines and Ayurvedic medicines.Citation88 Long-term usage of insulin and oral hypoglycemic drugs in diabetes patients can result in several side-effects such as gastrointestinal diseases (nausea, diarrhea and vomiting), hypoglycemic episodes, hepatorenal and edema syndromes.Citation89,Citation90 These side-effects lead to increased usage of traditional medicines in diabetes patients.Citation91,Citation92 Medicinal plants contain numerous phytochemicals, and some compounds are medically and therapeutically efficient. Mostly plants have amino acids, sterols, carotenoids, tannins, mucilages, coumarins, flavonoids, saponins, and essential oils. Therapeutic actions of medicinal plants depend on the different phytochemicals classes interactions.Citation93 Several studies have reported the antidiabetic activities of numerous isolated plant compounds.Citation94 Plants such as soybean, bitter melon, garlic, cocoa, walnut, aloe, caper, nettle, fenugreek, melon, coffee, sage, yerba mate, black and green tea have medicinal properties and are commonly utilized in diabetes and its associated comorbidities treatment. Compounds of these medicinal plants are used as antidiabetic agents with main consideration to compounds like berberine, trigonelline, gurmarin, fukugetin, phlorizin, amorfrutins, palmatine, gymnemic acids and honokiol.Citation95 Anti-hyperglycemic effects can resultfrom plant treatments which are commonly recognized by their ability to enhance the function of pancreatic tissue resulting from reduced absorption of glucose in the intestine or increased secretion of insulin.Citation96
Conclusion
In the last 2–3 decades, diabetes has reached epidemic levels worldwide. Diabetes is a global crisis which affects the economy and health of all nations. This epidemic is predominantly driven by urbanization, rapid industrialization and sedentary lifestyles. Rapid economic growth and changes in lifestyle are the major reasons for the increased prevalence of diabetes. Several studies have determined the effect of intrauterine environment to understand the future risk of T2D. Diabetes increases the risk of several life-threatening and serious problems and if not effectively controlled or managed, it can lead to premature death. Lifestyle modification is an important factor to decrease the risk of diabetes and its associated complications. The frequency of diabetic complications will rise with a lack of cost-effective and sustainable interventions. Hence, prevention of diabetes and its complications such as diabetic retinopathy and cardiovascular disease should be a crucial part of all future health-related public policies among all nations.
Ethics Approval and Consent to Participate
The current review does not require ethical approval.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors of the current review declared they do not have any conflicts of interest for this work.
Additional information
Funding
References
- DeFronzo RA , Ferrannini E , Zimmet P , Alberti G . International Textbook of Diabetes Mellitus . John Wiley & Sons; 2015.
- IDF Diabetes Atlas. IDF diabetes atlas, 9th edn. Brussels and Belgium; 2019. Available from: https://www.diabetesatlas.org. Accessed 5 11, 2021.
- Zimmet PZ . Diabetes and its drivers: the largest epidemic in human history? Clin Diabetes Endocrinol . 2017;3(1):1. doi:10.1186/s40842-016-0039-3 28702255
- International Diabetes Federation. IDF diabetes atlas 8th edition. IDF Executive Office; 2017. Available from: http://www.diabetesatlas.org/. Accessed 5 11, 2021.
- Goyal R , Jialal I . Diabetes mellitus type 2. In: StatPearls . Treasure Island (FL): StatPearls Publishing; 2020.
- American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2020. Diabetes Care . 2020;43(Supplement 1):S14–S31. doi:10.2337/dc20-S002.31862745
- Mekala KC , Bertoni AG . Chapter 4 - epidemiology of diabetes mellitus. In: Orlando G , Piemonti L , Ricordi C , Stratta RJ , Gruessner RWG , editors. Transplantation, Bioengineering, and Regeneration of the Endocrine Pancreas . Academic Press; 2020:49–58.
- Punthakee Z , Goldenberg R , Katz P . Definition, classification and diagnosis of diabetes, prediabetes and metabolic syndrome. Can J Diabetes . 2018;42:S10–S15. doi:10.1016/j.jcjd.2017.10.003 29650080
- Zheng Y , Ley SH , Hu FB . Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol . 2018;14(2):2. doi:10.1038/nrendo.2017.151
- American Diabetes Association. 3. Prevention or delay of type 2 diabetes: standards of medical care in diabetes—2020. Diabetes Care . 2020;43(Supplement 1):S32–S36. doi:10.2337/dc20-S003.31862746
- Vaiserman AM . Early-Life nutritional programming of type 2 diabetes: experimental and quasi-experimental evidence. Nutrients . 2017;9(3):236. doi:10.3390/nu9030236
- Bhutta ZA . Early nutrition and adult outcomes: pieces of the puzzle. Lancet . 2013;382(9891):486–487. doi:10.1016/S0140-6736(13)60716-3 23541369
- International Diabetes Federation. Diabetes Atlas . Brussels: International Diabetes Federation; 2003.
- Lovic D , Piperidou A , Zografou I , Grassos H , Pittaras A , Manolis A . The growing epidemic of diabetes mellitus. 2020. Available from: https://www.ingentaconnect.com/content/ben/cvp/2020/00000018/00000002/art00003. Accessed 3 15, 2020
- Yang W , Lu J , Weng J , et al. Prevalence of diabetes among men and women in China. N Engl J Med . 2010;362(12):1090–1101. doi:10.1056/NEJMoa0908292 20335585
- Abuyassin B , Laher I . Diabetes epidemic sweeping the Arab world. World J Diabetes . 2016;7(8):165–174. doi:10.4239/wjd.v7.i8.165 27114755
- International Diabetes Federation. IDF Diabetes Atlas . Brussels: International Diabetes Federation, Executive Office; 2011.
- Zimmet PZ , Magliano DJ , Herman WH , Shaw JE . Diabetes: a 21st century challenge. Lancet Diabetes Endocrinol . 2014;2(1):56–64. doi:10.1016/S2213-8587(13)70112-8 24622669
- Tillin T , Hughes AD , Godsland IF , et al. Insulin resistance and truncal obesity as important determinants of the greater incidence of diabetes in Indian Asians and African Caribbeans compared with Europeans: the Southall and Brent REvisited (SABRE) cohort. Diabetes Care . 2013;36(2):383–393. doi:10.2337/dc12-0544 22966089
- Wändell PE , Johansson SE , Gåfvels C , Hellénius ML , de Faire U , Sundquist J . Estimation of diabetes prevalence among immigrants from the Middle East in Sweden by using three different data sources. Diabetes Metab . 2008;34(4):328–333. doi:10.1016/j.diabet.2008.01.012 18539497
- Grant P . Management of diabetes in resource-poor settings. Clin Med . 2013;13(1):27–31. doi:10.7861/clinmedicine.13-1-27
- van der Gronde T , Uyl-de Groot CA , Pieters T . Addressing the challenge of high-priced prescription drugs in the era of precision medicine: a systematic review of drug life cycles, therapeutic drug markets and regulatory frameworks. PLoS One . 2017;12(8). doi:10.1371/journal.pone.0182613
- Campbell MD , Sathish T , Zimmet PZ , et al. Benefit of lifestyle-based T2DM prevention is influenced by prediabetes phenotype. Nat Rev Endocrinol . 2020;16:395–400. doi:10.1038/s41574-019-0316-1.32060416
- Saeedi P , Petersohn I , Salpea P , et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9th edition. Diabetes Res Clin Pract . 2019;157:107843. doi:10.1016/j.diabres.2019.107843 31518657
- Zhou B , Lu Y , Hajifathalian K , et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4·4 million participants. Lancet . 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8 27061677
- Ogurtsova K , da Rocha Fernandes JD , Huang Y , et al. IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract . 2017;128:40–50. doi:10.1016/j.diabres.2017.03.024 28437734
- Kautzky-Willer A , von Euler M , Oertelt-Prigione S . Editorial: sex and gender aspects in diabetes. Front Endocrinol . 2019;10. doi:10.3389/fendo.2019.00813.
- Dagenais GR , Gerstein HC , Zhang X , et al. Variations in diabetes prevalence in low-, middle-, and high-income countries: results from the prospective urban and rural epidemiological study. Diabetes Care . 2016;39(5):780–787. doi:10.2337/dc15-2338 26965719
- Goryakin Y , Rocco L , Suhrcke M . The contribution of urbanization to non-communicable diseases: evidence from 173 countries from 1980 to 2008. Econ Hum Biol . 2017;26:151–163. doi:10.1016/j.ehb.2017.03.004 28410489
- Hwang CK , Han PV , Zabetian A , Ali MK , Venkat Narayan KM . Rural diabetes prevalence quintuples over twenty-five years in low- and middle-income countries: a systematic review and meta-analysis. Diabetes Res Clin Pract . 2012;96(3):271–285. doi:10.1016/j.diabres.2011.12.001 22261096
- Unnikrishnan R , Pradeepa R , Joshi SR , Mohan V . Type 2 diabetes: demystifying the global epidemic. Diabetes . 2017;66(6):1432–1442. doi:10.2337/db16-0766 28533294
- Zimmet P , Taft P , Guinea A , Guthrie W , Thoma K . The high prevalence of diabetes mellitus on a Central Pacific island. Diabetologia . 1977;13(2):111–115. doi:10.1007/BF00745137 852640
- Magliano DJ , Soderberg S , Zimmet PZ , et al. Explaining the increase of diabetes prevalence and plasma glucose in mauritius. Diabetes Care . 2012;35(1):87–91. doi:10.2337/dc11-0886 22100964
- Dowse GK , Gareeboo H , Zimmet PZ , et al. High prevalence of NIDDM and impaired glucose tolerance in Indian, Creole, and Chinese Mauritians. Diabetes . 1990;39(3):390–396. doi:10.2337/diab.39.3.390 2307296
- Ramachandran A , Mary S , Yamuna A , Murugesan N , Snehalatha C . High prevalence of diabetes and cardiovascular risk factors associated with urbanization in India. Diabetes Care . 2008;31(5):893–898. doi:10.2337/dc07-1207 18310309
- Wang L , Gao P , Zhang M , et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA . 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596 28655017
- Ning F , Pang ZC , Dong YH , et al. Risk factors associated with the dramatic increase in the prevalence of diabetes in the adult Chinese population in Qingdao, China. Diabetic Med . 2009;26(9):855–863. doi:10.1111/j.1464-5491.2009.02791.x 19719705
- de Almeida-pititto B , Dias ML , de Moraes ACF , Ferreira SR , Franco DR , Eliaschewitz FG . Type 2 diabetes in Brazil: epidemiology and management. Diabetes Metab Syndr Obes . 2015;8:17–28. doi:10.2147/DMSO.S72542 25609989
- Bertoldi AD , Kanavos P , França GVA , et al. Epidemiology, management, complications and costs associated with type 2 diabetes in Brazil: a comprehensive literature review. Global Health . 2013;9(1):62. doi:10.1186/1744-8603-9-62 24299125
- Forouhi NG , Wareham NJ . Epidemiology of diabetes. Medicine . 2019;47(1):22–27. doi:10.1016/j.mpmed.2018.10.004
- Lipscombe LL , Hux JE . Trends in diabetes prevalence, incidence, and mortality in Ontario, Canada 1995–2005: a population-based study. Lancet . 2007;369(9563):750–756. doi:10.1016/S0140-6736(07)60361-4 17336651
- Mayer-Davis EJ , Lawrence JM , Dabelea D , et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002–2012. N Engl J Med . 2017;376(15):1419–1429. doi:10.1056/NEJMoa1610187 28402773
- Reece EA , Leguizamón G , Wiznitzer A . Gestational diabetes: the need for a common ground. Lancet . 2009;373(9677):1789–1797. doi:10.1016/S0140-6736(09)60515-8 19465234
- Franco M , Bilal U , Ordunez P , et al. Population-wide weight loss and regain in relation to diabetes burden and cardiovascular mortality in Cuba 1980–2010: repeated cross sectional surveys and ecological comparison of secular trends. BMJ . 2013;346:f1515. doi:10.1136/bmj.f1515 23571838
- Bommer C , Heesemann E , Sagalova V , et al. The global economic burden of diabetes in adults aged 20–79 years: a cost-of-illness study. Lancet Diabetes Endocrinol . 2017;5(6):423–430. doi:10.1016/S2213-8587(17)30097-9 28456416
- American Diabetes Association. Hogan P , Dall T , Nikolov P . Economic costs of diabetes in the US in 2002. Diabetes Care . 2003;26(3):917–932. doi:10.2337/diacare.26.3.917 12610059
- A. D. Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care . 2018;dci180007. doi:10.2337/dci18-0007
- Herman WH . The economic costs of diabetes: is it time for a new treatment paradigm? Diabetes Care . 2013;36(4):775–776. doi:10.2337/dc13-0270 23520368
- Chawla A , Chawla R , Jaggi S . Microvasular and macrovascular complications in diabetes mellitus: distinct or continuum? Indian J Endocrinol Metab . 2016;20(4):546–551. doi:10.4103/2230-8210.183480 27366724
- Petrie JR , Guzik TJ , Touyz RM . Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol . 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005 29459239
- Skinner MK . Epigenetic transgenerational inheritance. Nat Rev Endocrinol . 2016;12(2):68–70. doi:10.1038/nrendo.2015.206 26585656
- Beckman JA , Paneni F , Cosentino F , Creager MA . Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Eur Heart J . 2013;34(31):2444–2452. doi:10.1093/eurheartj/eht142 23625211
- Jonas JB , Sabanayagam C . Epidemiology and risk factors for diabetic retinopathy. Diabetic Retinopathy Cardiovasc Dis . 2019;27:20–37. doi:10.1159/000486262
- Solomon SD , Chew E , Duh EJ , et al. Diabetic retinopathy: a position statement by the American Diabetes Association. Diabetes Care . 2017;40(3):412–418. doi:10.2337/dc16-2641 28223445
- Feldman EL , Callaghan BC , Pop-Busui R , et al. Diabetic neuropathy. Nat Rev Dis Primers . 2019;5(1):1–8. doi:10.1038/s41572-019-0092-1 30617281
- Watterworth B , Wright TB . Diabetic peripheral neuropathy. In: Abd-Elsayed A , editor. Pain: A Review Guide . Cham: Springer International Publishing; 2019:911–913.
- Davies M , Brophy S , Williams R , Taylor A . The prevalence, severity, and impact of painful diabetic peripheral neuropathy in type 2 diabetes. Diabetes Care . 2006;29(7):1518–1522. doi:10.2337/dc05-2228 16801572
- Khoury CC , Chen S , Ziyadeh FN . Chapter 19 - pathophysiology of diabetic nephropathy. In: Kimmel PL , Rosenberg ME , editors. Chronic Renal Disease . 2nd ed. Academic Press; 2020:279–296.
- Steinke JM . The natural progression of kidney injury in young type 1 diabetic patients. Curr Diab Rep . 2009;9(6):473–479. doi:10.1007/s11892-009-0077-7 19954694
- Harding JL , Pavkov ME , Magliano DJ , Shaw JE , Gregg EW . Global trends in diabetes complications: a review of current evidence. Diabetologia . 2019;62(1):3–16. doi:10.1007/s00125-018-4711-2 30171279
- Krishnan B , Babu S , Walker J , Walker AB , Pappachan JM . Gastrointestinal complications of diabetes mellitus. World J Diabetes . 2013;4(3):51–63. doi:10.4239/wjd.v4.i3.51 23772273
- Lin EHB , Rutter CM , Katon W , et al. Depression and advanced complications of diabetes: a prospective cohort study. Diabetes Care . 2010;33(2):264–269. doi:10.2337/dc09-1068 19933989
- Tsilidis KK , Kasimis JC , Lopez DS , Ntzani EE , Ioannidis JPA . Type 2 diabetes and cancer: umbrella review of meta-analyses of observational studies. BMJ . 2015;350. doi:10.1136/bmj.g7607.
- Sözen T , Başaran NÇ , Tınazlı M , Özışık L . Musculoskeletal problems in diabetes mellitus. Eur J Rheumatol . 2018;5(4):258–265. doi:10.5152/eurjrheum.2018.18044 30388074
- Wyatt LH , Ferrance RJ . The musculoskeletal effects of diabetes mellitus. J Can Chiropr Assoc . 2006;50(1):43–50.17549168
- Bushby K , Finkel R , Birnkrant DJ , et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and psychosocial management. Lancet Neurol . 2010;9(1):77–93. doi:10.1016/S1474-4422(09)70271-6 19945913
- García JJM , Pérez GGR , Sicairos NML . Prevalencia de resistencia a la insulina y síndrome metabólico en niños obesos que acuden a la Clínica de Obesidad del Hospital Pediátrico de Sinaloa. Pediatr Mex . 2010;12(1):18–22.
- Mesinovic J , Zengin A , De Courten B , Ebeling PR , Scott D . Sarcopenia and type 2 diabetes mellitus: a bidirectional relationship. Diabetes Metab Syndr Obes . 2019;12:1057–1072. doi:10.2147/DMSO.S186600 31372016
- Hong S , Chang Y , Jung HS , Yun KE , Shin H , Ryu S . Relative muscle mass and the risk of incident type 2 diabetes: a cohort study. PLoS One . 2017;12(11):e0188650. doi:10.1371/journal.pone.0188650 29190709
- Yusof NA , Idris NS , Zin FM . Diabetic neuropathic cachexia in a young woman. Korean J Fam Med . 2019;40(3):194–198. doi:10.4082/kjfm.17.0127 30497111
- Gibbons CH . Treatment-induced neuropathy of diabetes. Curr Diab Rep . 2017;17(12):127. doi:10.1007/s11892-017-0960-6 29064042
- Tuomilehto J , Schwarz P , Lindström J . Long-term benefits from lifestyle interventions for type 2 diabetes prevention: time to expand the efforts. Diabetes Care . 2011;34(Supplement 2):S210–S214. doi:10.2337/dc11-s222 21525457
- Gillies CL , Abrams KR , Lambert PC , et al. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: systematic review and meta-analysis. BMJ . 2007;334(7588):299. doi:10.1136/bmj.39063.689375.55 17237299
- Schwarz PEH , Riemenschneider H . Slowing down the progression of type 2 diabetes: we need fair, innovative, and disruptive action on environmental and policy levels! Diabetes Care . 2016;39(Supplement 2):S121–S126. doi:10.2337/dcS15-3001 27440824
- Cederholm J , Gudbjörnsdottir S , Eliasson B , et al. Blood pressure and risk of cardiovascular diseases in type 2 diabetes: further findings from the Swedish National Diabetes Register (NDR-BP II). J Hypertens . 2012;30(10):2020. doi:10.1097/HJH.0b013e3283577bdf 22871895
- Eeg-Olofsson K , Cederholm J , Nilsson PM , et al. Glycemic control and cardiovascular disease in 7,454 patients with type 1 diabetes: an observational study from the Swedish National Diabetes Register (NDR). Diabetes Care . 2010;33(7):1640–1646. doi:10.2337/dc10-0398 20424222
- Davis WA , Davis TME . Cardiovascular risk prediction in adults with type 1 diabetes: the Fremantle Diabetes Study. Diabetes Res Clin Pract . 2010;90(3):e75–e78. doi:10.1016/j.diabres.2010.09.015 20950885
- Kautzky-Willer A , Stich K , Hintersteiner J , et al. Sex-specific-differences in cardiometabolic risk in type 1 diabetes: a cross-sectional study. Cardiovasc Diabetol . 2013;12(1):78. doi:10.1186/1475-2840-12-78 23705959
- Koivisto VA , Stevens IK , Mattock M , et al. Cardiovascular disease and its risk factors in IDDM in Europe. Diabetes Care . 1996;19(7):689–697. doi:10.2337/diacare.19.7.689 8799621
- Stettler C , Bearth A , Allemann S , et al. QTc interval and resting heart rate as long-term predictors of mortality in type 1 and type 2 diabetes mellitus: a 23-year follow-up. Diabetologia . 2007;50(1):186–194. doi:10.1007/s00125-006-0483-1 17096116
- Atkinson MA , Eisenbarth GS , Michels AW . Type 1 diabetes. Lancet . 2014;383(9911):69–82. doi:10.1016/S0140-6736(13)60591-7 23890997
- Ullah F , Afridi AK , Rahim F , et al. Knowledge of diabetic complications in patients with diabetes mellitus. J Ayub Med Coll Abbottabad . 2015;27(2):360–363.26411116
- Saha S , Gerdtham U-G , Johansson P . Economic evaluation of lifestyle interventions for preventing diabetes and cardiovascular diseases. Int J Environ Res Public Health . 2010;7(8):3150–3195. doi:10.3390/ijerph7083150 20948954
- Ramachandran A , Snehalatha C , Yamuna A , Mary S , Ping Z . Cost-effectiveness of the interventions in the primary prevention of diabetes among Asian Indians: within-trial results of the Indian diabetes prevention programme (IDPP). Diabetes Care . 2007;30(10):2548–2552. doi:10.2337/dc07-0150 17670917
- Weber MB , Ranjani H , Staimez LR , et al. The stepwise approach to diabetes prevention: results from the D-CLIP randomized controlled trial. Diabetes Care . 2016;39(10):1760–1767. doi:10.2337/dc16-1241 27504014
- Marín-Peñalver JJ , Martín-Timón I , Sevillano-Collantes C , Del Cañizo-Gómez FJ . Update on the treatment of type 2 diabetes mellitus. World J Diabetes . 2016;7(17):354–395. doi:10.4239/wjd.v7.i17.354 27660695
- Álvarez-almazán S , Filisola-Villaseñor JG , Alemán-González-Duhart D , Tamay-Cach F , Mendieta-Wejebe JE . Current molecular aspects in the development and treatment of diabetes. J Physiol Biochem . 2020;76(1):13–35. doi:10.1007/s13105-019-00717-0 31925679
- Teoh SL , Das S . Phytochemicals and their effective role in the treatment of diabetes mellitus: a short review. Phytochem Rev . 2018;17(5):1111–1128. doi:10.1007/s11101-018-9575-z
- Mahomoodally MF , Mootoosamy A , Wambugu S . Traditional therapies used to manage diabetes and related complications in Mauritius: a comparative ethnoreligious study. Evid Based Complement Alternat Med . 2016;2016:1–25. doi:10.1155/2016/4523828
- Maruthur NM , Tseng E , Hutfless S , et al. Diabetes medications as monotherapy or metformin-based combination therapy for type 2 diabetes. Ann Intern Med . 2016;164(11):740–751. doi:10.7326/M15-2650 27088241
- Ezuruike UF , Prieto JM . The use of plants in the traditional management of diabetes in Nigeria: pharmacological and toxicological considerations. J Ethnopharmacol . 2014;155(2):857–924. doi:10.1016/j.jep.2014.05.055 24929108
- Lee AL , Chen BC , Mou CH , Sun MF , Yen HR . Association of traditional Chinese medicine therapy and the risk of vascular complications in patients with type II diabetes mellitus. Medicine . 2016;95(3). doi:10.1097/MD.0000000000002536
- Katiyar D , Singh V , Gilani SJ , Goel R , Grover P , Vats A . Hypoglycemic herbs and their polyherbal formulations: a comprehensive review. Med Chem Res . 2015;24(1):1–21. doi:10.1007/s00044-014-1080-3
- Salehi B , Ata A , V Anil Kumar N , et al. Antidiabetic potential of medicinal plants and their active components. Biomolecules . 2019;9(10):551. doi:10.3390/biom9100551
- Ríos JL , Francini F , Schinella GR . Natural products for the treatment of type 2 diabetes mellitus. Planta Med . 2015;81(12–13):975–994. doi:10.1055/s-0035-1546131 26132858
- Arumugam G , Manjula P , Paari N . A review: anti diabetic medicinal plants used for diabetes mellitus. J Acute Dis . 2013;2(3):196–200. doi:10.1016/S2221-6189(13)60126-2