
Abstract
Purpose
To investigate the association between diabetic retinopathy (DR), DR intensity, and estimated glucose disposal rate (eGDR) in individuals with type 2 diabetes mellitus (T2DM).
Patients and Methods
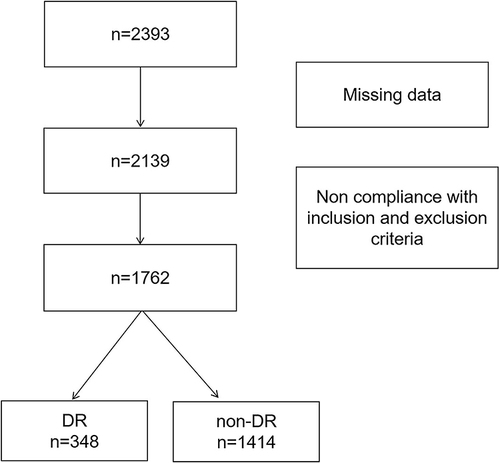
This study comprised 1762 T2DM patients who were admitted between January and December, 2021. Overall, the DR was identified in 430 patients. Based on the eGDR, the participants were divided into four study groups. One-way analysis of variance was used to compare the groups. The correlations between eGDR and DR risk, eGDR, and DR severity were analyzed using regression analysis. Furthermore, these relationships were analyzed in different sex groups.
Results
Patients with T2DM had a 19.75% (348/1762) DR detection rate, whereas those with DR had a 22.41% (78/348) proliferative DR detection rate. The DR group had substantially reduced levels of eGDR compared with the non-DR group. Multivariate logistic regression analysis demonstrated that reduced eGDR was an independent risk factor for DR, after adjusting for confounding variables. eGDR correlated significantly with proliferative DR in women but not in men.
Conclusion
In Chinese individuals with T2DM, lower eGDR was independently associated with a higher risk of DR.
Introduction
Diabetes mellitus (DM) is a major global health concern. By 2045, there will be 693 million individuals living with DM, up from the current projection of 425 million.Citation1,Citation2 Type 2 DM (T2DM) is the more prevalent type of DM. Diabetic retinopathy (DR), a highly frequent visual consequence of T2DM, affects approximately 25% of the T2DM patients.Citation3 DR frequency among T2DM patients ranged from 8% in the first 3 years to 25% in the 5th year, 60% in the 10th year, and 80% in the 15th year.Citation4,Citation5 DR is the leading cause of blindness among adults.Citation6 An estimated 191 million people will be affected by DR by 2030.Citation7 According to a meta-analysis of 20 epidemiological studies,Citation8 patients with any degree of DR have a 61% increased risk of cardiovascular disease (CVD)-related and all-cause mortalities. Since diabetes impairs microcirculation, DR has historically been considered a microcirculatory illness of the retina. DR is thought to be a reliable biomarker of the deleterious effects of diabetes on individuals. Consequently, DR has established that DM is an independent risk factor for CVD and cardiovascular mortality, in addition to a significant risk of various microangiopathic consequences (diabetic nephropathy, diabetic neuropathy, and diabetic foot).Citation9,Citation10 Hyperglycemia, caused by impaired insulin action resulting from insulin resistance (IR) or insulin deficiency, is the main pathogenic mechanism of DR.Citation11 IR always results in damage to small blood vessels, especially DR.Citation12 The clinical evidence for IR as a risk factor for DR came from several clinical trials, including the Diabetes Control and Complication Trial and the EURODIAB Prospective Complications studies.Citation13,Citation14 Studies indicated that local IR in the retina was not only an important factor that caused DR, but also important for assessing the severity of DR.Citation15
The euglycemic hyperinsulinemia clamp is the standard method used for IR measurement.Citation16 However, this method is expensive and intrusive, making it unsuitable for regular clinical use. To detect IR more readily, a validated method for estimating the glucose disposal rate (eGDR) was proposed based on clinical variables (waist circumference, hypertension, and glycated hemoglobin HbA1c). eGDR showed a good correlation with IR, as determined by euglycemic hyperinsulinemic clamp.Citation17,Citation18 Lower eGDR scores correlate with larger IR.According to data from the Pittsburgh Epidemiology of Diabetes Complications Study, individuals with DM who have low eGDR had a higher chance of developing nephropathy,Citation19 peripheral vascular disease,Citation20,Citation21 and coronary artery disease (CAD).Citation22 Kilpatrick et al discovered that patients with DM with lower levels of eGDR had a considerably higher risk of developing both microvascular and macrovascular illnesses.Citation23 The findings of the study by Helliwell et alCitation24 demonstrated that eGDR levels are related to both microvascular and macrovascular complications, independent of HbA1c. Therefore, eGDR helped stratify the risk of diabetes complications better than using each of its components separately. However, no studies have investigated the association between eGDR and DR in T2DM patients. Therefore, the present study aimed to investigate whether eGDR correlates with DR risk in Chinese T2DM patients.
Materials and Methods
Study Population
The Ethics Committee of the Hebei General Hospital in China gave its approval for conducting this study, which adhered to the Declaration of Helsinki. The patients in this study were admitted to the Hebei General Hospital in Shijiazhuang, China, between January 1 and December 31, 2020. All participants signed an informed consent form to participate in this study. Patients were screened and assessed based on the inclusion and exclusion criteria.
The following were the inclusion criteria: The World Health Organization’s criteria for 1999 were employed to diagnose T2DM.Citation10 Diabetes mellitus diagnoses based on the results of fasting glucose of ≥7 mmol/l, abnormal 2 h oral glucose tolerance test, and symptoms (polyuria, polydipsia, and unexplained weight loss) of hyperglycaemia with a random blood glucose of >11.1 mmol/l. The participants included in the study were diagnosed with T2DM.
The following were the exclusion requirements:Citation1 patients under the age of 18 years;Citation2 those with other forms of diabetes (such as type 1 DM, gestational DM, or other particular types);Citation3 those who had a history of myocardial infarction, cerebral hemorrhage, severe hepatic dysfunction, acute infection, or stress conditions in the previous 3 months;Citation4 pregnant and lactating women; andCitation5 participants with malignant tumors, liver surgery, severe medical disorders, or mental illnesses that made it difficult for them to comply with research requirements.
Study Methods
A thorough clinical history was obtained upon registration, including information on age, sex, waist circumference(WC), blood pressure, and body mass index (BMI). Following admission, venous blood was drawn from the patients in the early morning hours of the following day while fasting. The Clinical Detection Department performed all laboratory tests using the same equipment and reagents. Blood samples were examined for the following biomarkers: creatinine (Cr), uric acid (UA), high-density lipoprotein cholesterol (HDL), total cholesterol (TC), low-density lipoprotein cholesterol (LDL), triglyceride (TG), γ-glutamyl transpeptidase (GGT), alanine aminotransferase (ALT), aspartate aminotransferase (AST), HbA1c, blood urea nitrogen (BUN), fasting blood glucose (FBG), albumin (Alb), systolic blood pressure (SBP), and diastolic blood pressure (DBP). To ensure data accuracy, one assessor recorded the information into a spreadsheet, while another, a neutral assessor, double-checked it.
Definition and Severity Scale for DR
DR was graded according to the 2002 International Academy of Ophthalmology grading criteria.Citation25 It is a practical way to screen for DR to take at least two 45° fundus color images in each eye, one with the optic disc centered and the other with the macula centered, by trained professionals employing non-mydriatic fundus cameras.Citation26 For patients with moderate or more than moderate nonproliferative retinopathy found during screening, ophthalmologists made a further grading diagnosis.
Calculation of eGDR
eGDR was calculated using the following formula:Citation17 eGDR = 21.158 − (0.09 * WC) − (3.407 * HT) − (0.551 * HbA1c); WC = waist circumference (cm), HT = hypertension (yes = 1/no = 0), and HbA1c = HbA1c (%). Enrolled patients were classified into four groups according to eGDR quartiles, with the lowest eGDR quartile representing the highest IR. The Q4 group (the highest quartile) was used as the control group.
Statistical Analysis
Version 25.0 of the Statistical Package for the Social Sciences statistical software was employed to conduct the statistical analysis. Data were continuously gathered, and normality and homogeneity were assessed. Means ± standard deviations were used to express normally distributed data, and one-way analysis of variance was employed for the comparison of the groups. Non-parametric testing was conducted, and non-normally distributed data were presented as median (interquartile range). As a result of enumeration, the numbers (percentages) were calculated and compared using χ2 test. The Spearman correlation was used to analyze the relationships between variables. The relationship between eGDR and DR was investigated using multiple logistic regression analysis. Statistical significance was set at P < 0.05. The eGDR was divided into four groups according to quartiles: Q1 (lowest), Q2, Q3, and Q4 (highest). A subgroup analysis was performed to evaluate the robustness of the findings.
Results
Basic Characteristics of Participants with and without DR
Overall, 1762 patients, having a mean age of 56.68±10.17 years, including 879 men and 883 women, were recruited for this research (). Patients with T2DM had a 19.75% (348/1762) DR detection rate, whereas those with DR had a 22.41% (78/348) proliferative DR detection rate.In comparison to the non-DR group, the age, SBP, FPG, HbA1c, and BUN were increased and BMI, DBP, Alb, ALT, AST, and eGDR significantly were decreased in the DR group (). There were no significant differences in sex, WC, GGT, TC, LDL, HDL, TG, UA, or Cr between the DR and non-DR groups.
Table 1 Characteristics of Patients Included in This Study
Figure 1 Flowchart of the patient selection process.
In comparison to the non-DR group in women, the FPG, HbA1c, and HDL were increased and Alb was decreased in the DR group, with a significant difference (). In comparison to the non-DR group in men, the SBP, FPG, HbA1c, and BUN were increased and age, BMI, DBP, Alb, ALT, and AST were decreased in the DR group, with statistically significant differences ().
In women, the eGDR level was decreased significantly in the DR group, and the same result was observed in men.
Participants’ Fundamental Traits in the Four eGDR Groups
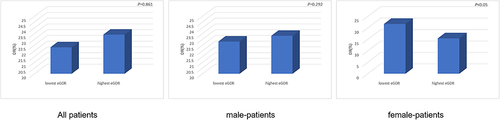
The patients’ baseline characteristics according to eGDR quartiles are shown in . Age, BMI, WC, SBP, DBP, FPG, HbA1c, GGT, TC, HDL, TG, ALT, BUN, and UA levels differed among the different eGDR groups. Participants with a higher eGDR had lower SBP and DBP. In the Q1 group, BMI, HbA1c, WC, GGT, FPG, and TG levels were substantially elevated compared to the other three groups. Age, TC, UA, and ALT levels were greater in the Q1 group than in the Q4 group. The Q4 group had higher HDL levels than the other three groups. The BUN levels in the Q4 group were lower than those in the other three groups. There were no differences in Alb, LDL, AST, and Cr levels between the groups. Patients with a higher eGDR showed a lower prevalence of DR. The highest DR incidence was observed in the Q1 group ().Female-patients who had a lower eGDR showed a higher prevalence of proliferative DR ().
Table 2 Characteristics of Patients Included in This Study by eGDR Levels
Figure 2 Comparison of the prevalence of DR in patients with T2DM who have different eGDR.
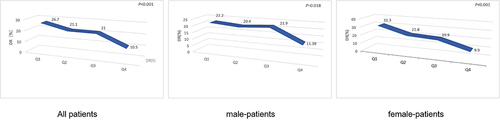
Figure 3 Comparison of the prevalence of PDR in patients with DR who have different eGDR.
Correlation of eGDR with Potential DR Risk Factors
The Spearman correlation analysis revealed that the eGDR was positively correlated with HDL (r=0.155, P<0.001) but negatively correlated with BMI (r=−0.402, P<0.001), FPG (r=−0.442, P<0.001), GGT (r=−0.244 P<0.001), Alb (r=−0.057 P=0.017), TC (r=−0.086, P<0.001), TG (r=−0.226, P<0.001), ALT (r=−0.164, P<0.001), BUN (r=−0.107 P<0.001), UA (r=−0.090 P<0.001), and age (r=−0.134, P<0.001).
Association Between eGDR and DR
Multivariate logistic regression analysis indicated that a low eGDR was an independent risk factor for DR after adjusting for age, sex, BMI, FPG, GGT, Alb, TC, LDL, HDL, TG, ALT, AST, Cr, BUN, and UA (odds ratio [OR] 0.634, 95% confidence interval [CI], 0.528–0.762, P<0.001; ).To ensure the robustness of the results, the eGDR was processed as a categorical variable (quartiles) for analysis. The risk of DR gradually decreased as the eGDR level increased when unadjusted for any variable. After adjustment for confounders, it was found that low-level eGDR was an independent risk factor for DR. Additionally, the Q1 group had the highest risk of developing DR (OR 5.603, 95% CI, 2.375–13.217, P<0.001; ).
Table 3 Logistic Regression Analysis of eGDR for DR in Patients with T2DM
Subgroup Analysis
Subgroup analyses were conducted based on sex to further evaluate how sex affected the connection between eGDR and DR. In the multivariate logistic regression analysis model, after adjustments for age, BMI, gender, hypertension, WC, FPG, GGT, ALT, AST, Alb, TC, TG, HDL-C, LDL-C, Cr, BUN, UA and course, low level of eGDR was an independent risk factor for DR in women with T2DM (OR 7.292, 95% CI 2.073–25.652 P=0.002) ().Consistently, significant association between eGDR and DR was found in men with T2DM under logistic regression analysis adjusted for age, BMI, gender, hypertension, WC, FPG, GGT, ALT, AST, Alb, TC, TG, HDL-C, LDL-C, Cr, BUN, UA and course (OR 4.682, 95% CI 1.412–15.529, P=0012) ().
Among patients with DR, a logistic regression analysis was performed with proliferative DR as the independent variable and age, BMI, gender, hypertension, WC, FPG, GGT, ALT, AST, Alb, TC, TG, HDL-C, LDL-C, Cr, BUN, UA and course as dependent variables. Multivariate logistic regression analysis demonstrated that low eGDR was an independent risk factor for proliferative DR in women (OR 8.537, 95% CI 1.613–45.169, P=0.03) (). In contrast, there was no statistically significant link between proliferative DR and eGDR in men with DR (OR 0.558, 95% CI 0.157–1.986, P=782) ().
Table 4 Logistic Regression Analysis of eGDR for Proliferative DR in Female-Patients
Discussion
The current study examined the potential connection between eGDR and DR. To further investigate whether a difference could be detected in subgroups of different sexes, we examined the association not only with the whole sample, but also in subgroups of different sexes. Some studies have revealed that the prevalence of DR ranged from 11.9 to 43.1% in China, Citation27–29 which was similar to our study. In this study, the eGDR significantly decreased in the DR group. The risk of DR increased with a decrease in eGDR. A high DR risk was independently associated with low eGDR levels in the present study. This association persisted even after adjusting for various potential confounding factors. This relationship can be clearly seen independently in women, and in men. Additionally, among DR patients, women, but not men, showed a significant connection between low eGDR levels and a higher likelihood of proliferative DR. Previous studies have focused on exploring the link between eGDR and DR in type 1 DM.Citation30–32 These analyses indicated that elevated eGDR levels were linked to a reduced risk of DR. A study by Pop et alCitation31 found that eGDR was more strongly associated than some identified risk factors for DR in type 1 DM. Moreover, Rowe et al confirmed a relationship between IR and more severe DR in patients with type 1 DM.Citation33 It was also demonstrated by Duţă et alCitation34 that eGDR was the most important factor of proliferative DR.
The use of eGDR has been recently advocated as a useful way to assess IR.Several studies have demonstrated that a lower eGDR is associated with higher IR.Citation18,Citation30,Citation32 It has been concluded that IR was responsible for elevation of oxidative stress.Citation35 Oxidative stress was closely related to apoptosis and endothelial cell dysfunction, which could lead to DR.Citation36 Insulin binding to its receptor activated the phosphatidylinositol-3-kinase (PI3-K/Akt) signaling pathway, leading to upregulation of hypoxy-inducing factor, and its direct interaction with vascular endothelial growth factor (VEGF) promoter led to increased VEGF expression.Citation37 Over-expression of VEGF will activate a series of signal pathways, and further disrupt the blood-retinal barrier (BRB), increase vascular permeability, induce cell proliferation and promote neovascularization.Citation38 Along with increased IR, the expression of free fatty acids in adipocytes and dimethylarginine in plasma increased, which could inhibit the activation of endogenous nitric oxide synthetase, resulting in vasomotor dysregulation and microcirculation disorders.Citation39 Due to the increased retinal vascular permeability, VEGF through the BRB and into retinal tissue, which facilitated neovascularization of the retina, resulting in DR.IR could promote the expression of retinal VEGF, so it might lead to or aggravate DR to some degree.Furthermore, the expression of plasminogen activator inhibitor-1 (PAI-1) was also increased significantly in the setting of IR.Citation40 PAI-1 could selectively inhibit the vasodilatory effects, leading to occlusion of the retinal capillaries and subsequent contributing to ischemia-induced vasculogenesis.
It has been shown that eGDR was linked to lipid levels and inflammation.Citation30 The present study also showed that as eGDR increased, the levels of TC and TG decreased. Inflammation is considered to play a substantial role in DR progression.Citation41 Hyperlipidemia is thought to be the main risk variable for DR development.Citation42 Inflammation promotes the transformation of nonproliferative DR to proliferative DR.Citation43,Citation44 Cluster speckle hemorrhage and retinal vessel permeability are features of nonproliferative DR.Citation45 DR with proliferative features is characterized by frequent retinal exudation and retinal hemorrhage.Citation46 Inflammation is one of the main contributors to vascular problems in T2DM patients.Citation47 The pathogenesis of diabetic microangiopathy involves inflammation (such as tumor necrosis factor-alpha and C-reactive protein) and vascular endothelial growth factor (VEGF)Citation48 VEGF-induced retinal expression of inflammation and entrapment of leukocytes have been observed in animal models of DR.Citation49 Hyperglycemia is a determinant of changes in retinal structure and vision.Citation50,Citation51 Inflammation and oxidative damage caused by chronic hyperglycemia increases endothelial permeability and barrier disruption.Citation52,Citation53 Subsequent microthrombi development, cell adhesion molecules, leukostasis, and cytokine activation are linked to the weakening of retinal ganglion cells and nerve fiber layers.Citation54–56
In the current study, it was found that the link between eGDR and DR was stronger in women than in men, and that eGDR was associated with proliferative DR in women only among T2DM patients. The results of our study demonstrated that female sex was another independent risk factor for DR. A growing body of research has shown a link between sex and the risk of DR in T2DM. In addition, a study by Li et alCitation29 found that women with T2DM had an increased incidence of DR in comparison to men, and the female sex was an independent element of risk for developing DR. Although the exact mechanism is unclear, this increase in DR prevalence in women may be due to estrogen levels. Indeed, RGC-5 cells are protected from high glucose-induced damage by 17hough the exaE2) via the mitochondrial pathway.Citation57 Furthermore, estrogen was found to be an important regulator of retinal blood flow and reduced vascular resistance in the large vessels of the eyes by reducing the amount of cholesterol.Citation58 It was unknown whether sex itself, or some other related risk factor(s), such as cultural socioeconomic factors or etiology, contributed to the male-female differences in DR.
As a systemic disease, oxidative stress, inflammation, vascular alterations, angiogenesis, and apoptosis can play a role in the development of DR.Citation59–61 Evidence from emerging studies has also suggested that complex gene-environment interactions facilitate the pathogenesis of diabetes-related microvascular complications.Citation62
Our study found no statistically significant difference in WC among T2DM patients with or without DR, which was consistent with previously published findings.Citation63,Citation64 Results by Iwasaki et al showed that WC was not associated with the presence of DR in Japanese patients with T2DM.Citation65 A study published in 2022Citation66 announced that abdominal obesity was not associated with DR in patients with diabetes.WC of participants in this study was similar to that in previous studies.Citation66–68
In our study, we found that ALT and GGT levels decreased with the increase of eGDR.Fabrice Bonnet et.alCitation69 found increased GGT and ALT were biomarkers of both systemic and hepatic IR with concomitant increased insulin secretion and decreased hepatic IR. ALT level may be a marker of visceral fat deposits in the liver and thus reflflect the status of IR.Citation70 ALT level is correlated with subclinical systemic inflflammation, increased oxidative stress and higher hepatic cytokine production. These factors may cause impaired insulin signaling.Citation71
The current study had several limitations. First, because this study was cross-sectional, no conclusions about causal correlations could be drawn. Second, information on current/previous smoking was lacking; thus, we were unable to adjust for this important confounder. The single ethnicity of the study population calls into question the generalizability of the findings. Large studies in multiple centers and different countries are required to understand the prospective significance of eGDR in routine clinical practice. Another limitation of our study is that we lacked detailed laboratory markers of inflammation, such as C-reactive protein which was associated DR.Finally, eGDR has previously been shown to be a reliable approximation of IR; however, its equations only contain clinical variables, which might be another limitation. This advantage could also be attributed to the fact that the eGDR equation provides reliable information for clinical decision making and is easy to calculate. Therefore, eGDR could serve as a risk marker for DR, and future longitudinal studies are needed to investigate this possibility.
Conclusion
In summary, our study showed that the occurrence of DR was independently correlated with a lower eGDR level. Among women with DR, low-level eGDR was associated with proliferative DR. There was no relationship between eGDR and proliferative DR in men. In addition, larger prospective cohort studies can further assess the utility of eGDR in risk stratification for diabetes complications and how eGDR compares to currently used measures such as HbA1c.
Disclosure
The authors declared no conflicts of interest.
References
- Zimmet PZ, Magliano DJ, Herman WH, Shaw JE. Diabetes: a 21st century challenge. Lancet Diabetes Endocrinol. 2014;2(1):56–64. doi:10.1016/S2213-8587(13)70112-8
- Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
- Robles-Rivera RR, Castellanos-González JA, Olvera-Montaño C, et al. Adjuvant therapies in diabetic retinopathy as an early approach to delay its progression: the importance of oxidative stress and inflammation. Oxid Med Cell Longev. 2020;2020:3096470. doi:10.1155/2020/3096470
- Jerneld B, Algvere P. Relationship of duration and onset of diabetes to prevalence of diabetic retinopathy. Am J Ophthalmol. 1986;102(4):431–437. doi:10.1016/0002-9394(86)90069-3
- Jaross N, Ryan P, Newland H. Prevalence of diabetic retinopathy in an Aboriginal Australian population: results from the Katherine region diabetic retinopathy study (KRDRS). Report no. 1. Clin Experiment Ophthalmol. 2003;31(1):32–39.
- American Diabetes Association. 10. Microvascular complications and foot care: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl1):S105–s18.
- Ding J, Wong TY. Current epidemiology of diabetic retinopathy and diabetic macular edema. Curr Diab Rep. 2012;12(4):346–354.
- Kramer CK, Rodrigues TC, Canani LH, Gross JL, Azevedo MJ. Diabetic retinopathy predicts all-cause mortality and cardiovascular events in both type 1 and 2 diabetes: meta-analysis of observational studies. Diabetes Care. 2011;34(5):1238–1244.
- Pearce I, Simó R, Lövestam-Adrian M, Wong DT, Evans M. Association between diabetic eye disease and other complications of diabetes: implications for care. A systematic review. Diabetes Obes Metab. 2019;21(3):467–478.
- Rosenson RS, Fioretto P, Dodson PM. Does microvascular disease predict macrovascular events in type 2 diabetes? Atherosclerosis. 2011;218(1):13–18. doi:10.1016/j.atherosclerosis.2011.06.029
- Gardner TW, Abcouwer SF, Barber AJ, Jackson GR. An integrated approach to diabetic retinopathy research. Arch Ophthalmol. 2011;129(2):230–235. doi:10.1001/archophthalmol.2010.362
- Tzeng TF, Liu WY, Liou SS, Hong TY, Liu IM. Antioxidant-rich extract from plantaginis semen ameliorates diabetic retinal injury in a streptozotocin-induced diabetic rat model. Nutrients. 2016;8:9. doi:10.3390/nu8090572
- Zhang L, Krzentowski G, Albert A, Lefebvre PJ. Risk of developing retinopathy in Diabetes Control and Complications Trial type 1 diabetic patients with good or poor metabolic control. Diabetes Care. 2001;24(7):1275–1279. doi:10.2337/diacare.24.7.1275
- Chaturvedi N, Sjoelie AK, Porta M, et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in type 1 diabetes. Diabetes Care. 2001;24(2):284–289. doi:10.2337/diacare.24.2.284
- Parvanova A, Iliev I, Filipponi M, et al. Insulin resistance and proliferative retinopathy: a cross-sectional, case-control study in 115 patients with type 2 diabetes. J Clin Endocrinol Metab. 2004;89(9):4371–4376. doi:10.1210/jc.2003-032076
- DeFronzo RA, Tobin JD, Andres R. Glucose clamp technique: a method for quantifying insulin secretion and resistance. Am J Physiol. 1979;237(3):E214–23. doi:10.1152/ajpendo.1979.237.3.E214
- Williams KV, Erbey JR, Becker D, Arslanian S, Orchard TJ. Can clinical factors estimate insulin resistance in type 1 diabetes? Diabetes. 2000;49(4):626–632. doi:10.2337/diabetes.49.4.626
- Nyström T, Holzmann MJ, Eliasson B, Svensson AM, Sartipy U. Estimated glucose disposal rate predicts mortality in adults with type 1 diabetes. Diabetes Obes Metab. 2018;20(3):556–563. doi:10.1111/dom.13110
- Orchard TJ, Chang YF, Ferrell RE, Petro N, Ellis DE. Nephropathy in type 1 diabetes: a manifestation of insulin resistance and multiple genetic susceptibilities? Further evidence from the Pittsburgh epidemiology of diabetes complication study. Kidney Int. 2002;62(3):963–970. doi:10.1046/j.1523-1755.2002.00507.x
- Olson JC, Erbey JR, Forrest KY, Williams K, Becker DJ, Orchard TJ. Glycemia (or, in women, estimated glucose disposal rate) predict lower extremity arterial disease events in type 1 diabetes. Metabolism. 2002;51(2):248–254. doi:10.1053/meta.2002.30021
- Pané A, Conget I, Boswell L, et al. Insulin resistance is associated with preclinical carotid atherosclerosis in patients with type 1 diabetes. Diabetes Metab Res Rev. 2020;36:e3323. doi:10.1002/dmrr.3323
- Orchard TJ, Olson JC, Erbey JR, et al. Insulin resistance-related factors, but not glycemia, predict coronary artery disease in type 1 diabetes: 10-year follow-up data from the Pittsburgh epidemiology of diabetes complications study. Diabetes Care. 2003;26(5):1374–1379. doi:10.2337/diacare.26.5.1374
- Kilpatrick ES, Rigby AS, Atkin SL. Insulin resistance, the metabolic syndrome, and complication risk in type 1 diabetes: “double diabetes” in the Diabetes Control and Complications Trial. Diabetes Care. 2007;30(3):707–712. doi:10.2337/dc06-1982
- Helliwell R, Warnes H, Kietsiriroje N, et al. Body mass index, estimated glucose disposal rate and vascular complications in type 1 diabetes: beyond glycated haemoglobin. Diabet Med. 2021;38(5):e14529. doi:10.1111/dme.14529
- Wilkinson CP, Ferris FL 3rd, Klein RE, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110(9):1677–1682. doi:10.1016/S0161-6420(03)00475-5
- Agardh E, Tababat-Khani P. Adopting 3-year screening intervals for sight-threatening retinal vascular lesions in type 2 diabetic subjects without retinopathy. Diabetes Care. 2011;34(6):1318–1319. doi:10.2337/dc10-2308
- Hu Y, Teng W, Liu L, et al. Prevalence and risk factors of diabetes and diabetic retinopathy in Liaoning province, China: a population-based cross-sectional study. PLoS One. 2015;10(3):e0121477. doi:10.1371/journal.pone.0121477
- Wang FH, Liang YB, Zhang F, et al. Prevalence of diabetic retinopathy in rural China: the Handan eye study. Ophthalmology. 2009;116(3):461–467. doi:10.1016/j.ophtha.2008.10.003
- Li M, Wang Y, Liu Z, et al. Females with type 2 diabetes mellitus are prone to diabetic retinopathy: a twelve-province cross-sectional study in China. J Diabetes Res. 2020;2020:5814296. doi:10.1155/2020/5814296
- Chillarón JJ, Goday A, Flores-Le-Roux JA, et al. Estimated glucose disposal rate in assessment of the metabolic syndrome and microvascular complications in patients with type 1 diabetes. J Clin Endocrinol Metab. 2009;94(9):3530–3534. doi:10.1210/jc.2009-0960
- Pop A, Clenciu D, Anghel M, et al. Insulin resistance is associated with all chronic complications in type 1 diabetes. J Diabetes. 2016;8(2):220–228. doi:10.1111/1753-0407.12283
- Epstein EJ, Osman JL, Cohen HW, Rajpathak SN, Lewis O, Crandall JP. Use of the estimated glucose disposal rate as a measure of insulin resistance in an urban multiethnic population with type 1 diabetes. Diabetes Care. 2013;36(8):2280–2285. doi:10.2337/dc12-1693
- Rowe CW, Haider AS, Viswanathan D, et al. Insulin resistance correlates with maculopathy and severity of retinopathy in young adults with Type 1 Diabetes Mellitus. Diabetes Res Clin Pract. 2017;131:154–160. doi:10.1016/j.diabres.2017.06.022
- Duţă I, Fica S, Ion DA. The association between insulin resistance and proliferative retinopathy in type 1 diabetes. Rom J Intern Med. 2015;53(3):261–266. doi:10.1515/rjim-2015-0034
- Newsholme P, Cruzat VF, Keane KN, Carlessi R, de Bittencourt PI. Molecular mechanisms of ROS production and oxidative stress in diabetes. Biochem J. 2016;473(24):4527–4550. doi:10.1042/BCJ20160503C
- Kowluru RA, Tang J, Kern TS. Abnormalities of retinal metabolism in diabetes and experimental galactosemia. VII. Effect of long-term administration of antioxidants on the development of retinopathy. Diabetes. 2001;50(8):1938–1942. doi:10.2337/diabetes.50.8.1938
- Koch CA, Anderson D, Moran MF, Ellis C, Pawson T. SH2 and SH3 domains: elements that control interactions of cytoplasmic signaling proteins. Science. 1991;252(5006):668–674. doi:10.1126/science.1708916
- Bai Y, Ma JX, Guo J, et al. Müller cell-derived VEGF is a significant contributor to retinal neovascularization. J Pathol. 2009;219(4):446–454. doi:10.1002/path.2611
- Artunc F, Schleicher E, Weigert C, Fritsche A, Stefan N, Häring HU. The impact of insulin resistance on the kidney and vasculature. Nat Rev Nephrol. 2016;12(12):721–737. doi:10.1038/nrneph.2016.145
- Jin R, Krasinskas A, Le NA, et al. Association between plasminogen activator inhibitor-1 and severity of liver injury and cardiovascular risk in children with non-alcoholic fatty liver disease. Pediatr Obes. 2018;13(1):23–29. doi:10.1111/ijpo.12183
- Tang J, Kern TS. Inflammation in diabetic retinopathy. Prog Retin Eye Res. 2011;30(5):343–358. doi:10.1016/j.preteyeres.2011.05.002
- Raman R, Ganesan S, Pal SS, Kulothungan V, Sharma T. Prevalence and risk factors for diabetic retinopathy in rural India. Sankara nethralaya diabetic retinopathy epidemiology and molecular genetic study III (SN-DREAMS III), report no 2. BMJ Open Diabetes Res Care. 2014;2(1):e000005. doi:10.1136/bmjdrc-2013-000005
- Tenconi PE, Bermúdez V, Oresti GM, Giusto NM, Salvador GA, Mateos MV. High glucose-induced phospholipase D activity in retinal pigment epithelium cells: new insights into the molecular mechanisms of diabetic retinopathy. Exp Eye Res. 2019;184:243–257. doi:10.1016/j.exer.2019.04.028
- Lv P, Yu J, Xu X, Lu T, Xu F. Eriodictyol inhibits high glucose-induced oxidative stress and inflammation in retinal ganglial cells. J Cell Biochem. 2019;120(4):5644–5651. doi:10.1002/jcb.27848
- Rodríguez ML, Pérez S, Mena-Mollá S, Desco MC, Ortega ÁL. Oxidative stress and microvascular alterations in diabetic retinopathy: future therapies. Oxid Med Cell Longev. 2019;2019:4940825. doi:10.1155/2019/4940825
- Kumari N, Karmakar A, Ganesan SK. Targeting epigenetic modifications as a potential therapeutic option for diabetic retinopathy. J Cell Physiol. 2020;235(3):1933–1947. doi:10.1002/jcp.29180
- Pollack RM, Donath MY, LeRoith D, Leibowitz G. Anti-inflammatory agents in the treatment of diabetes and its vascular complications. Diabetes Care. 2016;39(Suppl 2):S244–52. doi:10.2337/dcS15-3015
- Roy MS, Janal MN, Crosby J, Donnelly R. Inflammatory biomarkers and progression of diabetic retinopathy in African Americans with type 1 diabetes. Invest Ophthalmol Vis Sci. 2013;54(8):5471–5480. doi:10.1167/iovs.13-12212
- Das A, Rangasamy S, McGuire PG, Das P. Diabetic retinopathy and inflammation: novel therapeutic targets. Middle East Afr J Ophthalmol. 2012;19(1):52–59. doi:10.4103/0974-9233.92116
- Shafabakhsh R, Aghadavod E, Mobini M, Heidari-Soureshjani R, Asemi Z. Association between microRNAs expression and signaling pathways of inflammatory markers in diabetic retinopathy. J Cell Physiol. 2019;234(6):7781–7787.
- Dehdashtian E, Mehrzadi S, Yousefi B, et al. Diabetic retinopathy pathogenesis and the ameliorating effects of melatonin; involvement of autophagy, inflammation and oxidative stress. Life Sci. 2018;193:20–33.
- Rangasamy S, Monickaraj F, Legendre C, et al. Transcriptomics analysis of pericytes from retinas of diabetic animals reveals novel genes and molecular pathways relevant to blood-retinal barrier alterations in diabetic retinopathy. Exp Eye Res. 2020;195:108043.
- Lenin R, Thomas SM, Gangaraju R. Endothelial activation and oxidative stress in neurovascular defects of the retina. Curr Pharm Des. 2018;24(40):4742–4754.
- Hui Y, Yin Y. MicroRNA-145 attenuates high glucose-induced oxidative stress and inflammation in retinal endothelial cells through regulating TLR4/NF-κB signaling. Life Sci. 2018;207:212–218.
- Cui RZ, Wang L, Qiao SN, et al. ON-type retinal ganglion cells are preferentially affected in STZ-Induced diabetic mice. Invest Ophthalmol Vis Sci. 2019;60(5):1644–1656.
- Nadri G, Saxena S, Stefanickova J, et al. Disorganization of retinal inner layers correlates with ellipsoid zone disruption and retinal nerve fiber layer thinning in diabetic retinopathy. J Diabetes Complications. 2019;33(8):550–553.
- Hao M, Li Y, Lin W, et al. Estrogen prevents high-glucose-induced damage of retinal ganglion cells via mitochondrial pathway. Graefes Arch Clin Exp Ophthalmol. 2015;253(1):83–90.
- Schmidl D, Schmetterer L, Garhöfer G, Popa-Cherecheanu A. Gender differences in ocular blood flow. Curr Eye Res. 2015;40(2):201–212.
- Rübsam A, Parikh S, Fort PE. Role of Inflammation in Diabetic Retinopathy. Int J Mol Sci. 2018;19:4.
- Wu W, Zhou G, Han H, et al. PI3Kδ as a novel therapeutic target in pathological angiogenesis. Diabetes. 2020;69(4):736–748.
- Suzuki Y, Yao T, Okumura K, Seko Y, Kitano S. Elevation of the vitreous body concentrations of oxidative stress-responsive apoptosis-inducing protein (ORAIP) in proliferative diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2019;257(7):1519–1525.
- Khullar M, Cheema BS, Raut SK. Emerging evidence of epigenetic modifications in vascular complication of diabetes. Front Endocrinol. 2017;8:237.
- Wan H, Wang Y, Xiang Q, et al. Associations between abdominal obesity indices and diabetic complications: Chinese visceral adiposity index and neck circumference. Cardiovasc Diabetol. 2020;19(1):118.
- Matuszewski W, Stefanowicz-Rutkowska MM, Szychlińska M, Bandurska-Stankiewicz E. Differences in risk factors for diabetic retinopathy in type 1 and type 2 diabetes mellitus patients in north-east Poland. Medicina. 2020;56:4.
- Iwasaki T, Togashi Y, Ohshige K, et al. Neither the presence of metabolic syndrome as defined by the IDF guideline nor an increased waist circumference increased the risk of microvascular or macrovascular complications in Japanese patients with type 2 diabetes. Diabetes Res Clin Pract. 2008;79(3):427–432.
- Wu Z, Yu S, Kang X, et al. Association of visceral adiposity index with incident nephropathy and retinopathy: a cohort study in the diabetic population. Cardiovasc Diabetol. 2022;21(1):32.
- Li X, Li HY, Yu ZW, Zhang YT, Tong XW, Gao XY. Association among lipid accumulation product, Chinese visceral obesity index and diabetic retinopathy in patients with type 2 diabetes: a cross-sectional study. Diabetes Metab Syndr Obes. 2021;14:4971–4979.
- Zhou JB, Yuan J, Tang XY, et al. Is central obesity associated with diabetic retinopathy in Chinese individuals? An exploratory study. J Int Med Res. 2019;47(11):5601–5612.
- Bonnet F, Ducluzeau PH, Gastaldelli A, et al. Liver enzymes are associated with hepatic insulin resistance, insulin secretion, and glucagon concentration in healthy men and women. Diabetes. 2011;60(6):1660–1667.
- Hu FB, Meigs JB, Li TY, Rifai N, Manson JE. Inflammatory markers and risk of developing type 2 diabetes in women. Diabetes. 2004;53(3):693–700.
- Wang CS, Chang TT, Yao WJ, Wang ST, Chou P. Impact of increasing alanine aminotransferase levels within normal range on incident diabetes. J Formos Med Assoc. 2012;111(4):201–208.