
Abstract
Background
Psoriasis is associated with an increased prevalence of cardiovascular risk factors, including metabolic syndrome (MetS). To date, it is unclear whether MetS causes differences in cardiovascular outcomes in psoriatic patients with coronary artery disease.
Methods
We conducted a retrospective cohort study to determine the effects of MetS in psoriatic patients with coronary artery disease. Comparisons were made between patients with and without MetS. Cox regression analysis and Kaplan–Meier survival analysis were used to evaluate the association between variables.
Results
Of the 307 psoriatic patients with coronary artery disease, 94 met criteria (30.6%) for MetS. Individuals with MetS were more likely to be female (p <0.001). Levels of platelet counts and high-sensitivity C-reactive protein were higher in the MetS group (p = 0.038 and 0.005, respectively). After a mean follow-up of 35.32 months, major adverse cardiovascular events (MACEs) and non-fatal myocardial infarction were more likely in the MetS than the non-MetS group (33.3% vs 20.6%, p = 0.02; 26.4% vs 15.7%, p = 0.032, respectively). Kaplan–Meier estimates showed the same trend. Cox regression analysis showed that MetS (hazard ratio 1.738; 95% confidence interval 1.045–2.891; p = 0.033) and left ventricular ejection fraction (hazard ratio 0.968; 95% confidence interval 0.945–0.991; p = 0.006) were associated with an increased risk of MACEs.
Conclusion
In psoriatic patients with coronary artery disease, MetS independently predicted MACEs. In addition, left ventricular ejection fraction was negatively associated with an increased risk of MACEs. To reduce the cardiovascular disease risk, it is necessary to increase awareness of MetS in psoriatic patients with coronary artery disease.
Introduction
Metabolic syndrome (MetS) occurs when a person has several risk factors, such as central obesity, high triglycerides, hypertension, diabetes, or reduced levels of high-density lipoprotein cholesterol (HDL-c).Citation1 The prevalence of MetS in China is around 33.9% overall, with 31.0% in men and 36.8% in women.Citation2 Meanwhile, MetS has been linked to future cardiovascular diseases (CVDs) incidence and death.Citation3–5 There are many reasons for this, including factors associated with MetS that may increase coronary calcification and subclinical atherosclerosis.Citation6 However, in patients with established CVDs, the prognostic value of MetS remained inconclusive.Citation7–9
Psoriasis is a chronic inflammatory multisystemic skin condition, many other conditions could be associated with it, such as psoriatic arthritis, uveitis, depression, and inflammatory bowel diseases.Citation10,Citation11 Scaly skin patches, plaques, and pustules are common signs of the disease, along with episodes of remission and relapse. Over 50% of cases of psoriasis develop during the first three decades of life, with the prevalence of the disease being approximately 2% worldwide.Citation10 It has been reported that the chronic inflammation associated with psoriasis is also associated with an elevated prevalence of risk factors associated with CVDs, including MetS components, such as obesity, diabetes, hyperlipidemia, and hypertension.Citation12,Citation13 Among them, obesity and psoriasis share a low-grade chronic inflammatory state. In obese patients, there is a shift from production of inactive to active macrophages, with an increase in pro-inflammatory cytokines such as tumor necrosis factor alpha.Citation13
In comparison with control groups, individuals with psoriasis have a life expectancy that is nearly six years shorter, and most deaths related to psoriasis are associated with cardiovascular morbidities.Citation14 Therefore, timely adjustment and control of the factors contributing to CVDs in psoriatic patients may have a role in improving the clinical outcome. However, it is not clear whether MetS causes differences in the cardiovascular outcomes of psoriatic patients who have already suffered from coronary artery disease. To the best knowledge of the authors, this study is the first to investigate this issue. The results will provide valuable information for improving the prognosis of psoriatic patients with coronary artery disease.
Materials and Methods
Study Population
All consecutive psoriatic patients who underwent coronary angiography because of coronary artery disease in Fuwai hospital from January 2017 to May 2022 were retrospectively included. Inclusion criteria were as follows: 1) age ≥18 years; 2) patients who were diagnosed with coronary artery disease and underwent coronary angiography; 3) patients with a history of psoriasis or who were diagnosed with psoriasis at this visit. Some patients were admitted to hospital for several reviews during the study period, but only the clinical records of patients’ first admissions were kept and analyzed. The clinical records, laboratory measurements, pharmacological treatments, and coronary angiography reports of patients were collected. The study was approved by the Institute Ethics Committee of Fuwai hospital (Approval No.2021–1544) and in accordance with the Declaration of Helsinki.
Definitions
The National Cholesterol Education Program–Adult Treatment Panel III criteriaCitation1 provides five risk factors for the diagnosis of MetS, including central obesity (waist circumference), high triglycerides, hypertension, diabetes, and reduced HDL-c. As waist circumference was not available, we used body mass index (BMI) as a surrogate measure, which has previously been adopted and verified.Citation7,Citation15,Citation16 Consequently, in this study, individuals were defined as MetS if they met three or more of the following criteria: (1) BMI ≥30 kg/m2 for men and ≥25 kg/m2 for women; (2) high triglycerides (≥1.695 mmol/L); (3) low HDL-c (<1.035 mmol/L in men and <1.293 mmol/L in women); (4) diabetes, and (5) hypertension. Major adverse cardiac events (MACEs) were defined as a composite of all-cause death, non-fatal myocardial infarction, unplanned revascularization, non-fatal stroke, and re-hospitalization because of heart failure or severe arrhythmias. The definition of non-fatal myocardial infarction includes both ST-elevation myocardial infarction (STEMI) and unstable angina/non-STEMI. Unstable angina was only recorded as an event when urgent hospital admission was required. An unplanned revascularization was a repeat percutaneous coronary intervention or surgical bypass of any segment of the target vessel for ischemic symptoms.Citation17 The diagnosis of stroke was confirmed based on the medical records. Nonbiologic systemic treatments for psoriasis included steroids and methotrexate, while biologics included tumor necrosis factor alpha, interleukin 12/23, and interleukin 17 inhibitors. The estimated glomerular filtration rate was calculated according to the Chronic Kidney Disease Epidemiology Collaboration equation.Citation18 All laboratory indicators were the results of patients at the first time of admission. The entire group was last followed up in November 2022. Follow-up results of all patients were obtained through outpatient records and telephone calls. The follow-up duration for patients was calculated as follows: If a patient had MACEs before the end of follow-up, the follow-up duration was the time between the date of the occurrence of MACEs and the date of discharge. If a patient did not have MACEs, the duration was the time between the date of the end of follow-up and the date of discharge.
Statistical Analysis
Histograms were used to assess the normality of continuous variables. Continuous values were reported as the mean ± standard or median (25th, 75th percentiles), and were compared using students’ t-tests or rank-sum tests between two groups. Categorical values were presented as numbers (percentages), and Pearson’s chi-square or Fisher’s exact tests were used to detect differences. The survival curves were calculated using Kaplan–Meier estimates, and the Log rank test was used to compare the endpoints. A Cox proportional hazard model was used to investigate any independent effect of MACEs. A two-tailed p value <0.05 was considered statistically significant. All statistical analyses were conducted using SPSS 25.0 (IBM Corp., Armonk, NY, USA). The Kaplan–Meier curve was performed using GraphPad Prism 8.0 (GraphPad, San Diego, CA, USA).
Results
Characteristics of the Whole Group
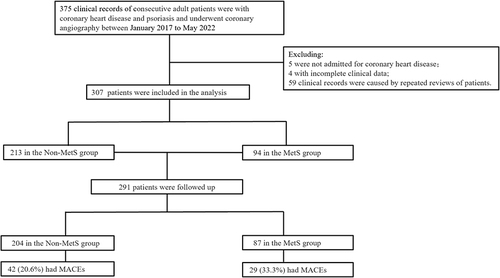
We collected 375 clinical records of patients. Of these, 59 records were excluded because they were repeat reviews of patients already included in the study. In addition, four patients had incomplete clinical information, and five patients were not admitted for coronary heart disease (including one patient with aortic aneurysm, three with valve disease, and one with peripheral vascular disease). Consequently, 307 patients’ clinical records were finally included in the analysis. The flow chart of included patients is shown in .
Figure 1 Flow chart showing the selection of patients.
The cohort had a mean age of 58.64 ± 9.99 years and a mean BMI of 26.07 ± 3.30 kg/m2. The study was predominantly composed of male patients (87.9%). Among these patients, 56.7% had hypertension, 47.9% had diabetes, 94.5% had hyperlipidemia, and 13.7% had a family history of coronary artery diseases. There were 194 patients (63.2%) admitted for acute coronary syndrome. A total of 92.1%, 81.3%, 50.8%, 83.9%, and 96.7% of patients used aspirin, P2Y12 inhibitors, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, β-blockers, and statins, respectively. The cohort had mild to moderate skin disease severity as measured by the Psoriasis Area Severity Index score (mean 8.47) and the mean psoriasis disease duration was 20 years. As for the treatment of psoriasis, a total of 12.4% of patients used phototherapy, 41.4% used nonbiologic systemic treatment, and 10.5% used biologic treatment. These results are shown in .
Table 1 Baseline Clinical Characteristics of the Non-MetS and MetS Groups
Characteristics of the Patients Grouped by MetS
Of the 307 participants, 94 (30.6%) met criteria for MetS. The MetS group had no significant differences in age (p = 0.733), history of stroke (p = 0.232), and family history of coronary artery disease (p = 0.96) when compared with the non-MetS group. The Psoriasis Area Severity Index scores (p = 0.198), disease duration of psoriasis (p = 0.2), and psoriasis-specific medication use were not significantly different between the MetS and the non-MetS groups. Individuals with MetS were more likely to be female, and were also more likely to have hypertension, diabetes, and a higher BMI (all p <0.001) than individuals without MetS (). Regarding the biochemical and coronary characteristics (), the patients in the MetS group had greater systemic inflammation by platelet counts ([(242.07 ± 67.78) ×109/L vs (225.70 ± 61.66) ×109/L; p = 0.038] and high-sensitivity C-reactive protein (hsCRP) [2.06 (1.08, 4.35) mg/L vs 1.37 (0.57, 3.2) mg/L; p = 0.005]. Despite having similar total cholesterol (p = 0.753) and low-density lipoprotein cholesterol levels (p = 0.346), participants with MetS had lower HDL-c levels [0.94 (0.82, 1.10) mmol/L vs 1.13 (0.97, 1.33) mmol/L; p < 0.001] and higher triglycerides levels [1.97 (1.34, 2.53) mmol/L vs 1.29 (1.03, 1.70) mmol/L; p < 0.001]. Left ventricular ejection fraction (LVEF) and culprit vessels were not significantly different between the MetS and non-MetS groups.
Table 2 Biochemical and Coronary Characteristics of the Non-MetS and MetS Groups
Clinical Outcomes of the Patients Between the Two Groups
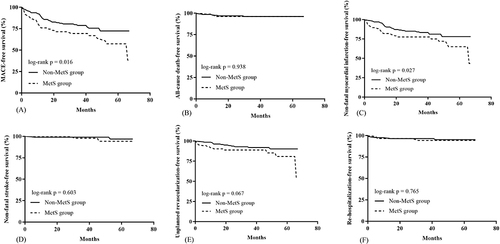
A total of 291 patients were followed up for a mean of 35.32 months, including 204 patients in the non-MetS group and 87 patients in the MetS group. At last, 29 patients (33.3%) in the MetS group had MACEs, while 42 patients (20.6%) in the non-MetS group had MACEs; the difference between the two groups was significant (p = 0.020). The incidence of non-fatal myocardial infarction was higher in the MetS group than the non-MetS group (26.4% vs 15.7%, p = 0.032), while the incidence of all-cause death (p = 1.000), non-fatal stroke (p = 0.996), unplanned revascularization (p = 0.058), and re-hospitalization (p = 1.000) were not significantly different between the two groups (). Kaplan–Meier estimates showed the same trend (). The results showed there were significant differences in MACEs (log rank p = 0.016) and non-fatal myocardial infarction (log rank p = 0.027) between the MetS and non-MetS groups (). Cox regression analysis was used to detect any independent effect of MACEs. According to the results of univariate and multivariate Cox regression analysis, in the whole study, MetS (hazard ratio 1.738; 95% confidence interval 1.045–2.891; p = 0.033) and LVEF (hazard ratio 0.968; 95% confidence interval 0.945–0.991; p = 0.006) were related to the increased risk of MACEs ().
Table 3 Clinical Outcomes of the Two Groups
Table 4 Univariate and Multivariate Cox Regression Analysis of Risk Factors for MACEs in All Patients
Figure 2 Kaplan–Meier estimated event rates for patients with and without MetS. (A) Survival curves for the outcome of MACE in patients between two groups; (B) survival curves for the outcome of all-cause death in patients between two groups; (C) survival curves for the outcome of non-fatal myocardial infarction in patients between two groups; (D) survival curves for the outcome of non-fatal stroke in patients between two groups; (E) survival curves for the outcome of unplanned revascularization in patients between two groups; (F) survival curves for the outcome of re-hospitalization in patients between two groups.
Discussion
We performed a retrospective study to assess the effects of MetS on cardiovascular outcomes in psoriatic patients with coronary artery disease. The incidence of MetS in these patients was approximately 30.6%, and MetS was more common in females. The rate of MACEs was higher in the MetS group than the non-MetS group. Cox analysis showed that MetS and LVEF were independent risk factors for MACEs in these patients.
According to recent evidence, MetS has been recognized as an important comorbidity of psoriasis.Citation19 There is a prevalence of 32% for MetS among adult patients with psoriasis globally.Citation20 The prevalence is different between locations. The prevalence is highest in Latin America at 47%, followed by Africa at 37%, Europe at 34%, Asia at 29%, while North America has the lowest prevalence of 26%.Citation20 In our study, there were 30.6% psoriatic patients with coronary artery disease who had MetS, which is consistent with the above reports.
We also found that individuals with MetS were more often female, which has been previously reported. In a study by Adışen et al,Citation21 the prevalence of MetS was higher in women than in men (60.5% vs 39.4%). In another study,Citation22 compared with men with psoriasis, there were more female psoriatic patients with MetS (47.9% vs 30.6%). In a report by Mebazaa et al,Citation23 compared with psoriatic males, psoriatic females had a significantly higher prevalence of MetS (47.4% vs 35%). Multiple factors may contribute to develop MetS mainly in females such as physical inactivity, sedentary behavior, diet quality, and a tendency toward central obesity.Citation23 Moreover, psychophysiological response to stress may influence subsequent eating behavior and lifestyle in women and, over time, these alterations affect abdominal obesity and dyslipidemia.Citation24 However, in other studies, the prevalence of MetS among females was lower than that in males.Citation25,Citation26 These conflicting findings suggest that the prevalence of MetS may also be influenced by other factors, such as genetic background, different lifestyles, or the different definitions of MetS used in different studies.
The pathophysiological mechanisms linking MetS and psoriasis are not easy to understand; however, it is important to identify these, as the information may provide the basis for novel pharmacologic approaches. Chronic inflammatory diseases have an important place in dermatology.Citation27 Psoriasis is an inflammatory disease mediated by T cells, which is characterized by the overproduction of pro-inflammatory mediators in the skin by lymphocytes and keratinocytes.Citation28 Locally overproduced pro-inflammatory mediators can move into the systemic circulation, causing insulin resistance, increased oxidative stress, endothelial dysfunction, increased angiogenesis, and hypercoagulation.Citation29–31 A chronic inflammatory state and a shift between types of macrophages may also play an important role in the association between psoriasis and MetS.Citation13 Treatments with biological agents provide advantages by reducing or preventing comorbidities and psoriasis lesions by reducing inflammation parameters.Citation32 In addition to the physical effects of psoriasis, its psychosocial effects can negatively impact quality of life. As a result of the negative psychosocial effects, the chronic course of the disease, the lack of a cure, and the economic burden, unhealthy living habits are more likely to appear in patients with psoriasis, such as alcohol use, smoking, poor nutritional habits, and a sedentary lifestyle that predisposes this patient group to obesity.Citation21,Citation33,Citation34 Obesity, especially abdominal obesity, is also an important component of MetS. Hao et alCitation35 have suggested alternative mechanisms underlying the association between psoriasis and MetS, such as changed levels of adipocytokines and dysbiosis of the gut microbiota.
MetS is well known to increase the risk of CVDs and to increase mortality.Citation3–5 In patients with established CVDs, however, the prognostic value of MetS remains inconclusive. Nigam. et alCitation9 reported an increase in long-term mortality in patients with coronary heart disease if they also had MetS. In a study by Kajimoto et al, mortality was higher in nondiabetic patients with MetS undergoing coronary artery bypass grafting than those without MetS; however, among the patients with diabetes, the presence of MetS was not related to long-term mortality.Citation8 In another study,Citation7 the long-term survival of MetS and non-MetS patients undergoing coronary artery bypass grafting was similar, although MetS was associated with higher risks of myocardial infarction and recurrent admissions for congestive heart failure. Here, we studied another patient population, namely psoriatic patients who have coronary artery disease, as studies have not been conducted on how MetS affects prognosis in these patients. Our results show that MetS is an independent risk factor for MACEs in psoriatic patients with coronary artery disease. This finding emphasizes that systematic screening for MetS in psoriatic patients with coronary artery disease is of great importance to prevent poor cardiovascular outcomes. A timely diagnosis of MetS in these patients may help to identify individuals in need of cardiovascular preventive measures and then prompt consideration for early treatment.
Another finding in this study was that LVEF was negatively related to the increased risk of MACEs, which means that patients with low LVEF are more likely to have MACEs. Indeed, previous studies have showed that LVEF is a powerful predictor of adverse events and the preferred functional marker for routine risk stratification and therapeutic decision making. In the Canadian Assessment of Myocardial Infarction study, compared with patients with LVEF >50%, the odds ratio for 1-year mortality after myocardial infarction was 9.48 for patients with LVEF ≤ 30%, 2.94 for patients with LVEF 30–40%, and 1.41 for patients with LVEF 40–50%.Citation36 In the Autonomic Tone and Reflexes after Myocardial Infarction study, patients with LVEF of 35–50% had a relative risk of 2.5 for cardiac mortality compared with patients with LVEF >50%, whereas in patients with LVEF < 35%, the relative risk was 7.3.Citation37 Another study reported that an LVEF ≤ 30% predicted all-cause mortality, cardiac mortality, and sudden cardiovascular death at 5 years in post-infarction patients.Citation38 The Noninvasive Evaluation cohort study showed that a reduced LVEF (≤30%) was a significant predictor of cardiac death or resuscitated cardiac arrest in patients early after myocardial infarction with LVEF <50%.Citation39 All of the studies described support the results of our study. However, the effects of MetS on LVEF are controversial. In a study by Gharipour et al,Citation40 the mean LVEF in patients with left bundle branch block and MetS was lower than that in patients without MetS (p = 0.017). In a study by Burroughs et al,Citation41 normal-weight individuals with MetS had decreased left ventricular systolic function; however, in overweight individuals with MetS, MetS was associated with increased LVEF. Zhou et alCitation15 found that in patients with multivessel coronary artery disease and acute coronary syndrome, there was no significant difference in LVEF between patients with and without MetS (p = 0.23). In another study,Citation42 patients with and without MetS also had similar LVEF (p=0.443). The different conclusions in these studies may be because of the different study participants. Although our study did not show a difference in LVEF between the two groups, low LVEF was still a predictive factor of subsequent MACE events in psoriatic patients with coronary artery disease, and clinicians should be aware of this information.
Participants with MetS had elevated markers of systemic inflammation, such as hsCRP and platelet counts. Raised hsCRP levels have been consistently associated with coronary heart disease and MetS.Citation43–45 In a study by Yang et al,Citation44 there was a higher level of hsCRP in the MetS group. This finding suggests a higher level of inflammation and oxidative stress in these patients, which creates a conducive pathophysiological environment for high-risk plaque development. Routine hsCRP tests may enhance risk assessment in the identification of individuals who require cardioprotective drugs, as well as increase the emphasis on healthy lifestyle changes.Citation43 It is well known that platelets are also immune cells, and that they can trigger and regulate inflammatory processes, contributing significantly to the pathogenesis of psoriasis.Citation46 Platelet activation and aggregation are critically involved in the pathophysiology of various diseases such as hypertension, diabetes, and cardiac diseases.Citation47,Citation48
MetS increases the difficulty of managing psoriatic patients with coronary artery diseases, and because of the increased risk of cardiovascular events associated with these conditions, it is vital to detect, prevent, and treat them as early as possible. Dermatologists are often the first to patients, and they need to identify MetS early and manage it.
The study’s major strength was the enrollment of a large number of Chinese psoriatic patients with coronary artery disease, and to our knowledge, the current study is the largest to date regarding the effects of MetS on psoriatic patients with coronary artery disease. Our study also had some limitations. First, since this study was conducted in a single medical center in China, patients enrolled in this study may not be representative of the general population. Second, bias was inevitable because of the retrospective study design. Although our study provides useful information for the effects of MetS in psoriatic patients with coronary artery disease, further work in this patient group is needed.
Conclusion
Rather than only simply dealing with the skin lesions, psoriatic patients should undergo appropriate screening and relevant health education during their treatment. In this study, in psoriatic patients with coronary artery disease, MetS was an independent risk factor for MACEs. In addition, LVEF was also significantly related to an increased risk of MACEs. To reduce the CVDs risk associated with MetS, it is vital to increase awareness of the condition among these patients.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author(s).
Statement of Ethics
This study was approved by the Institute Ethics Committee of Fuwai hospital and was conducted in accordance with the declaration of Helsinki. Written informed consents were obtained from all participants. Data was also anonymized before analysis.
Disclosure
The authors declare no conflict of interest.
Additional information
Funding
References
- Expert Panel on Detection E. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
- Lu J, Wang L, Li M, et al. Metabolic syndrome among adults in China: the 2010 China noncommunicable disease surveillance. J Clin Endocrinol Metab. 2017;102(2):507–515. doi:10.1210/jc.2016-2477
- Lakka HM, Laaksonen DE, Lakka TA, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA. 2002;288(21):2709–2716. doi:10.1001/jama.288.21.2709
- Hess PL, Al-Khalidi HR, Friedman DJ, et al. The metabolic syndrome and risk of sudden cardiac death: the atherosclerosis risk in communities study. J Am Heart Assoc. 2017;6(8). doi:10.1161/JAHA.117.006103
- Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol. 2010;56(14):1113–1132. doi:10.1016/j.jacc.2010.05.034
- Ryu J, Yong HS, Huh S, Kang EY, Woo OH. Relation of coronary atherosclerosis and metabolic syndrome in asymptomatic subjects: evaluation with coronary CT angiography. Int J Cardiovasc Imaging. 2013;29(Suppl 2):101–107. doi:10.1007/s10554-013-0319-2
- Deo SV, Sundaram V, Wilson B, et al. Adverse events after coronary artery bypass grafting in patients with preoperative metabolic syndrome: a 10-year follow-up of the Veterans affairs database. J Thorac Cardiovasc Surg. 2022;163(6):2096–2103.e2093. doi:10.1016/j.jtcvs.2020.08.018
- Kajimoto K, Kasai T, Miyauchi K, et al. Metabolic syndrome predicts 10-year mortality in non-diabetic patients following coronary artery bypass surgery. Circ J. 2008;72(9):1481–1486. doi:10.1253/circj.CJ-07-0928
- Nigam A, Bourassa MG, Fortier A, Guertin MC, Tardif JC. The metabolic syndrome and its components and the long-term risk of death in patients with coronary heart disease. Am Heart J. 2006;151(2):514–521. doi:10.1016/j.ahj.2005.03.050
- Gisondi P, Bellinato F, Girolomoni G, Albanesi C. Pathogenesis of chronic plaque psoriasis and its intersection with cardio-metabolic comorbidities. Front Pharmacol. 2020;11:117. doi:10.3389/fphar.2020.00117
- Diotallevi F, Paolinelli M, Radi G, Offidani A. Latest combination therapies in psoriasis: narrative review of the literature. Dermatol Ther. 2022;35(10):e15759. doi:10.1111/dth.15759
- Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB, Gelfand JM. Prevalence of cardiovascular risk factors in patients with psoriasis. J Am Acad Dermatol. 2006;55(5):829–835. doi:10.1016/j.jaad.2006.08.040
- Trovato E, Rubegni P, Prignano F. Place in therapy of anti-IL-17 and 23 in psoriasis according to the severity of comorbidities: a focus on cardiovascular disease and metabolic syndrome. Expert Opin Biol Ther. 2022;22(12):1443–1448. doi:10.1080/14712598.2022.2093106
- Abuabara K, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Cause-specific mortality in patients with severe psoriasis: a population-based cohort study in the U.K. Br J Dermatol. 2010;163(3):586–592. doi:10.1111/j.1365-2133.2010.09941.x
- Zhou J, Liu C, Zhou P, et al. Prevalence and impact of metabolic syndrome in patients with multivessel coronary artery disease and acute coronary syndrome. Nutr Metab Cardiovasc Dis. 2021;31(9):2693–2699. doi:10.1016/j.numecd.2021.05.029
- Rejas J, Bobes J, Arango C, Aranda P, Carmena R, Garcia-Garcia M. Concordance of standard and modified NCEP ATP III criteria for identification of metabolic syndrome in outpatients with schizophrenia treated with antipsychotics: a corollary from the CLAMORS study. Schizophr Res. 2008;99(1–3):23–28. doi:10.1016/j.schres.2007.10.015
- Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115(17):2344–2351. doi:10.1161/CIRCULATIONAHA.106.685313
- Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
- Holmannova D, Borsky P, Borska L, et al. Metabolic syndrome, clusterin and elafin in patients with psoriasis vulgaris. Int J Mol Sci. 2020;21(16):5617. doi:10.3390/ijms21165617
- Liu L, Cai XC, Sun XY, et al. Global prevalence of metabolic syndrome in patients with psoriasis in the past two decades: current evidence. J Eur Acad Dermatol Venereol. 2022;36(11):1969–1979. doi:10.1111/jdv.18296
- Adışen E, Uzun S, Erduran F, Gürer MA. Prevalence of smoking, alcohol consumption and metabolic syndrome in patients with psoriasis. An Bras Dermatol. 2018;93(2):205–211. doi:10.1590/abd1806-4841.20186168
- Love TJ, Qureshi AA, Karlson EW, Gelfand JM, Choi HK. Prevalence of the metabolic syndrome in psoriasis: results from the national health and nutrition examination survey, 2003–2006. Arch Dermatol. 2011;147(4):419–424. doi:10.1001/archdermatol.2010.370
- Mebazaa A, El Asmi M, Zidi W, et al. Metabolic syndrome in Tunisian psoriatic patients: prevalence and determinants. J Eur Acad Dermatol Venereol. 2011;25(6):705–709. doi:10.1111/j.1468-3083.2010.03856.x
- Epel E, Lapidus R, McEwen B, Brownell K. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology. 2001;26(1):37–49. doi:10.1016/S0306-4530(00)00035-4
- Kokpol C, Aekplakorn W, Rajatanavin N. Prevalence and characteristics of metabolic syndrome in South-East Asian psoriatic patients: a case-control study. J Dermatol. 2014;41(10):898–902. doi:10.1111/1346-8138.12614
- Koku Aksu AE, Saraçoğlu ZN, Metintaş S, Sabuncu İ, Çetin Y. Age and gender differences in Framingham risk score and metabolic syndrome in psoriasis patients: a cross-sectional study in the Turkish population. Anatol J Cardiol. 2017;17(1):66–72. doi:10.14744/AnatolJCardiol.2016.6679
- Daye M, Temiz SA, Isık B. The relationship between lichen planus and metabolic syndrome. J Cosmet Dermatol. 2021;20(8):2635–2639. doi:10.1111/jocd.13905
- Luan L, Han S, Wang H, Liu X. Down-regulation of the Th1, Th17, and Th22 pathways due to anti-TNF-α treatment in psoriasis. Int Immunopharmacol. 2015;29(2):278–284. doi:10.1016/j.intimp.2015.11.005
- Frieder J, Ryan C. Psoriasis and cardiovascular disorders. G Ital Dermatol Venereol. 2016;151(6):678–693.
- Grozdev I, Korman N, Tsankov N. Psoriasis as a systemic disease. Clin Dermatol. 2014;32(3):343–350. doi:10.1016/j.clindermatol.2013.11.001
- Arican O, Aral M, Sasmaz S, Ciragil P. Serum levels of TNF-alpha, IFN-gamma, IL-6, IL-8, IL-12, IL-17, and IL-18 in patients with active psoriasis and correlation with disease severity. Mediators Inflamm. 2005;2005(5):273–279. doi:10.1155/MI.2005.273
- Ataseven A, Temiz SA, Eren G, Özer İ, Dursun R. Comparison of anti-TNF and IL-inhibitors treatments in patients with psoriasis in terms of response to routine laboratory parameter dynamics. J Dermatolog Treat. 2022;33(2):1091–1096. doi:10.1080/09546634.2020.1801975
- Herron MD, Hinckley M, Hoffman MS, et al. Impact of obesity and smoking on psoriasis presentation and management. Arch Dermatol. 2005;141(12):1527–1534. doi:10.1001/archderm.141.12.1527
- Gupta MA, Gupta AK. Psychodermatology: an update. J Am Acad Dermatol. 1996;34(6):1030–1046. doi:10.1016/S0190-9622(96)90284-4
- Hao Y, Zhu YJ, Zou S, et al. Metabolic syndrome and psoriasis: mechanisms and future directions. Front Immunol. 2021;12:711060. doi:10.3389/fimmu.2021.711060
- Rouleau JL, Talajic M, Sussex B, et al. Myocardial infarction patients in the 1990s--their risk factors, stratification and survival in Canada: the Canadian Assessment of Myocardial Infarction (CAMI) study. J Am Coll Cardiol. 1996;27(5):1119–1127. doi:10.1016/0735-1097(95)00599-4
- La Rovere MT, Bigger JT Jr., Marcus FI, Mortara A, Schwartz PJ. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (autonomic tone and reflexes after myocardial infarction) investigators. Lancet. 1998;351(9101):478–484. doi:10.1016/S0140-6736(97)11144-8
- Bauer A, Barthel P, Schneider R, et al. Improved stratification of autonomic regulation for risk prediction in post-infarction patients with preserved left ventricular function (ISAR-Risk). Eur Heart J. 2009;30(5):576–583. doi:10.1093/eurheartj/ehn540
- Exner DV, Kavanagh KM, Slawnych MP, et al. Noninvasive risk assessment early after a myocardial infarction the REFINE study. J Am Coll Cardiol. 2007;50(24):2275–2284. doi:10.1016/j.jacc.2007.08.042
- Gharipour M, Hashemi Jazi M, Nilforoush P, Batvandi A, Mohammadi R, Najafi R. Metabolic syndrome and its association with left ventricular dysfunction in patients with left bundle branch block. Acta Biomed. 2015;86(2):157–161.
- Burroughs Peña M, Swett K, Schneiderman N, et al. Cardiac structure and function with and without metabolic syndrome: the Echocardiographic Study of Latinos (Echo-SOL). BMJ Open Diabetes Res Care. 2018;6(1):e000484. doi:10.1136/bmjdrc-2017-000484
- Chen J, Wang X, Dong B, et al. Cardiac function and exercise capacity in patients with metabolic syndrome: a cross-sectional study. Front Cardiovasrc Med. 2022;9:974802. doi:10.3389/fcvm.2022.974802
- Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the centers for disease control and prevention and the American heart association. Circulation. 2003;107(3):499–511. doi:10.1161/01.CIR.0000052939.59093.45
- Yang X, Luo W, Han S, et al. Prevalence of high-risk coronary plaques in patients with and without metabolic syndrome and the relationship with prognosis. BMC Cardiovasc Disord. 2020;20(1):73. doi:10.1186/s12872-020-01358-8
- Ramírez-Terán AL, Vega-Memije ME, Torres-Tamayo M, Martínez-Alvarado MR. Carotid intima-media thickness in patients with psoriasis with and without metabolic syndrome. Arch Cardiol Mex. 2022;92(3):305–311. doi:10.24875/ACM.21000106
- Fan Z, Wang L, Jiang H, Lin Y, Wang Z. Platelet dysfunction and its role in the pathogenesis of psoriasis. Dermatology. 2021;237(1):56–65. doi:10.1159/000505536
- Zhao L, Meng X, Mei Q, et al. Risk factors for cardiac complications in patients with pheochromocytoma and paraganglioma: a retrospective single-center study. Front Endocrinol. 2022;13:877341. doi:10.3389/fendo.2022.877341
- Ouviña SM, La Greca RD, Zanaro NL, Palmer L, Sassetti B. Endothelial dysfunction, nitric oxide and platelet activation in hypertensive and diabetic type II patients. Thromb Res. 2001;102(2):107–114. doi:10.1016/S0049-3848(01)00237