
Abstract
Purpose
To assess the diabetes mellitus (DM) knowledge, attitudes, preventive practices, and associated factors among a sample of adult non-diabetic Saudi residents.
Methods
The present survey was conducted in April-June 2022. People from the general population were invited to participate in the study, and the data were collected using a validated questionnaire.
Results
A total of 1207 non-diabetic subjects participated in the study [females 798(66.1%) and males 409(33.9%)], and the response rate was 80% (1207/1500). Two-thirds (66.86%) of non-diabetic adult community members had good knowledge of DM, 47.8% had positive attitudes, and 62.14% maintained a healthy lifestyle to avoid DM. There was a family history of DM in more than half of the subjects 723(59.9%). Participants who had a direct relative with diabetes scored higher on the knowledge question than those who did not (p<0.001). Practice questions responses for preventing DM showed that about 459(38%) were using fatty food less frequently, and only 338(28%) and 153(12.7%) were doing physical activities 30–60 minutes per day frequently and very frequently, respectively. Most participants were smoking tobacco, 890(73.7%), and getting checked their BP, 704(58.3%), very frequently. The participants with a master’s and Ph.D. degree were likelier to have positive attitudes and good practices than students. Individuals with a history of DM in their families were 2.10 times (OR=2.10, p<0.001), 1.95 times (OR=1.95, p<0.001), and 2.03 times (OR=2.03, p<0.001) more likely to be knowledgeable, had positive attitudes and good practices than those with no DM in their family, respectively.
Conclusion
Over half of the individuals possessed a positive mindset, adequate knowledge, and good practicing behavior for preventing DM. Having Master’s and Ph.D. degrees and a family history of DM were associated with a positive attitude and good practices. There is a need to expand community awareness campaigns utilizing social media channels.
Introduction
Westernization of dietary patterns in the Kingdom of Saudi Arabia (KSA) has negatively affected the residents’ health. It has increased the frequency of overweight and obesity among the younger generation, which is considered a significant contributing factor in the development of DM.Citation1,Citation2 DM is among the most prevalent non-communicable diseases (NCDs) threatening the world irrespective of geography, nationality, color, race, and gender.
Diabetes is frequent in KSA, which ranks second in the Middle East and seventh worldwide. There are around seven million individuals with diabetes and three million pre-diabetes in KSA.Citation3 Prediabetes, a precursor to diabetes, affects 88 million people over 18 years, and nine out of ten people are unaware that they have prediabetes.Citation4 According to estimates, DM was one of the top 10 causes of mortality for adults worldwide in 2017 and resulted in four million fatalities.Citation5 Of those with diabetes, one in two (50%) are unaware that they have the disease.Citation6
A recent study reported prevalence of obesity and overweight among Saudi residents is 23% and 33%, respectivelyCitation7 that is alarming. They also reported fewer sleeping hours, more sedentary activities, and the use of more fizzy drinks. All of these have been linked to the progression of DM.Citation8,Citation9 As being overweight and obese are two major risk factors for T2DM, KAP studies are more important for designing effective preventive strategies in such a population. Therefore, it is necessary to investigate what non-diabetic individuals know and think about DM. Moreover, educating the masses can avoid or delay DM and its complications.Citation10
Chronic DM comorbidities, which substantially impact diabetic individuals’ quality of life, can be avoided with proper DM education. Individuals’ knowledge regarding DM may help identify their DM risk, urge them to get the treatment they need and motivate them to take care of their health.Citation11 Adequate DM knowledge improves life quality and prevents complications and may help with diabetes management, complications prevention, and diabetes development in those at risk.Citation12 However, ignorance increases DM risk.Citation13
Several studies assessed the KAPs of non-diabetic individuals in KSACitation14–16 and stated variable results. The assessment of non-diabetic individuals’ awareness of the most common endocrinal problem in the world and its associated factors would provide baseline information on how the non-diabetic individual perceive DM, its risk factors, signs and symptoms, control and management and complications. It also describes their attitude about DM screening, avoidance of excessive use of sugar, the importance of physical activities and consumption of fatty food. Abundant literature is available for diabetic people about physical activities and dietary patterns, but less literature is known about the prevention of diabetes for non-diabetic individuals. Such type of studies not only helps to explore non-diabetic individuals’ awareness of DM but also their misconceptions.
The KAP investigations provide baseline information on the topic. We may identify gaps between knowledge and practices for establishing management plans and implementing prompt measures to lessen the strain on the healthcare system. Such type of research not only serves to reduce the occurrence of the illness but also its complications. Furthermore, to establish future health policies, services, and communication campaigns, it is necessary to understand people’s diabetes awareness, attitudes, and perceptions. Therefore, the study objectives were to assess the DM knowledge, attitudes, preventive practices, and associated factors among a sample of adult non-diabetic Saudi residents.
Materials and Methods
The present cross-sectional survey was carried out at the Faculty of Medicine, Rabigh, King Abdulaziz University in Jeddah, KSA in April-June 2022. The researchers invited people from the general population to participate. People of both genders above the age of 18 were included. Those with DM, severe illness, and physically inactive were excluded. The bioethical unit of King Abdulaziz University Jeddah provided ethical approval (Reference No. 286-22). The independent variables in the current study were gender, nationality, marital status, educational level, monthly income, and family history of DM, while the dependent variables were DM knowledge, attitude toward DM, and preventive practices.
An online questionnaire was used to collect the data. The questionnaire link was sent via social media like Twitter, WhatsApp, and Facebook. The first part of the questionnaire was related to the consent and all study participants provided consent prior to the start of the survey. They could proceed if they agreed to the study objectives, non-diabetic and wanted to participate voluntarily.
The sample size was computed on a sample size calculator by Raosoft Incorporation. After employing a 5% margin of error, a 95% confidence level, and a 50% response rate, the sample size needed to reach appropriate statistical power was 383. However, looking at the nature of the study and people’s non-participation in such studies, the sample size was increased to get the desired results. Selection bias, information bias, and confounding bias are the three most common biases. To avoid selection bias, we included the question “Are you diabetic?” in our online questionnaire, with the response options “Yes” or “No”. If the participants answered yes, they could not proceed. We used an already tested and validated questionnaire to overcome the information bias. There are usually no significant confounders in this type of study.
A total of 1500 participants were invited to participate in this survey, and 1207 non-diabetic individuals returned completed questionnaires with an 80% response rate. The participants were chosen using the convenience sampling technique. We used an already validated questionnaire that has been translated and used in KSA previously,Citation15 and its reliability was 0.75 (Cronbach’s alpha). Originally, the present questionnaire was developed by Kassahun and Mekonen.Citation17
The validated questionnaire contained three knowledge, attitudes, and practices sections. “The scoring of the knowledge questions was done as ≤ 50% score = not knowledgeable, >50% score= knowledgeable. For the attitude, scoring was done as correct answer = 1 score, incorrect (No) = minus score, unsure= 0 scores. The plus score was considered positive, while the 0 or minus score was considered negative. The practice questions were coded as correct (yes) answer = 1 score, incorrect (No) = zero scores, unsure= 0 scores, and >50% score were considered good”.Citation15
Statistical Analysis
Data were analyzed on SPSS version 26. For each variable, the frequency and percentages were calculated. The Chi-square test was performed to compare various variables. The binary logistic regression analysis assessed the relationship between DM knowledge, attitude, practice scores, and other variables. The p-values below 0.05 were deemed significant.
Results
A total of 1207 non-diabetic subjects participated in the study [females 798(66.1%) and males 409(33.9%)]. The mean age and BMI were 27.68±10.9 and 23.49±5.10, respectively. There was a family history of DM in more than half of the subjects, 723(59.9%) ().
Table 1 General Characteristics of the Study Participants (n = 1207)
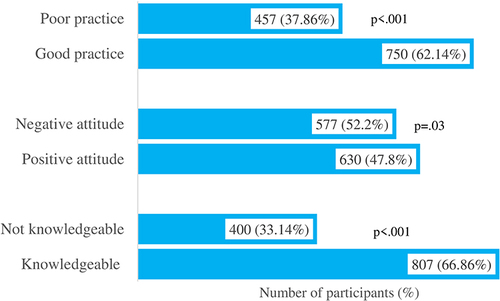
Two-thirds (66.86%) of non-diabetic adult community members had a good knowledge of DM, 47.8% had positive attitudes, and 62.14% maintained a healthy lifestyle to avoid DM. Participant responses varied widely in distinct groups, such as knowledgeable and not knowledgeable (p<0.001), positive and negative attitudes (p=0.03), and good and poor practices (p<0.001) ().
Figure 1 Comparison of participants responses according to knowledgeable and not knowledgeable, positive and negative attitudes and good and poor practices groups.
depicts the difference between knowledgeable and not knowledgeable participants across different study variables. The participants with a family history of DM (type 1 or type 2) had significantly higher scores than those without a family history of DM (p<0.001).
Table 2 Difference Between Knowledgeable and Not Knowledgeable Participants Scores Across Different Study Variables (N = 1207)
The difference between participants’ positive and negative attitude scores, good and poor practice scores, and across different study variables are depicted in . Participants with a family history of diabetes had significantly higher positive attitude scores and good practice scores than those without a family history of DM (p<0.001).
Table 3 Difference Between Participants’ Positive and Negative Attitude Scores, Good and Poor Practice Scores Across Different Study Variables (N = 1207)
The frequency distribution of participants’ responses of knowledge towards DM showed that 753(62.39%) stated DM is a condition of high blood sugar level, 842(69.76%) said its incurable, and 512(42.2%) considered it a condition of insufficient insulin production. The participants’ responses regarding various categories of DM knowledge are shown in .
Table 4 Frequency Distribution of Participants’ Response of Knowledge Towards Diabetes Mellitus (n = 1207)
Participants’ responses to attitude questions showed that more than two-thirds agreed to DM examination, screening, avoiding too much sugar, preventing DM by physical activity, and maintaining a healthy weight ().
Table 5 Frequency Distribution of Participants’ Response to Attitude Questions Towards Diabetes Mellitus (n = 1207)
Practice questions responses for preventing DM showed that about 459(38%) were using fatty food less frequently, and only 338(28%) and 153(12.7%) were doing physical activities 30–60 minutes per day frequently and very frequently, respectively. The majority of the participants were smoking tobacco, 890(73.7%), and getting checked their BP, 704(58.3%), very frequently ().
Table 6 Frequency Distribution of Participants’ Response to Practice Questions Regarding Diabetes Mellitus (n = 1207)
The participants with a master’s and Ph.D. degree were 2.35 times (OR=2.35, p=0.036) and 1.91 times (OR=1.91, p=0.001) likely to have positive attitudes compared to students. Likewise, the participants with a master’s and Ph.D. degree were 3.21 times (OR=3.21, p=0.001), and 3.15 times (OR=3.15, p=0.028) good practices compared to students. Individuals with a history of DM in their families were 2.10 times (OR=2.10, p<0.001) more likely to be knowledgeable than those with no family history. Similarly, such individuals have 1.95 times (OR=1.95, p<0.001) positive attitudes and 2.03 times (OR=2.03, p<0.001) more good practices than those with no family history of DM ().
Table 7 Binary Logistic Regression Predicting Diabetes Mellitus-Related Knowledge, Attitudes, and Practices Among Study Participants (N = 1207)
Discussion
According to this community-based survey, two-thirds (66.86%) of non-diabetic adult community members had a favorable knowledge of DM, 47.8% had positive attitudes, and 62.14% maintained a healthy lifestyle to avoid DM. Our KAP results are similar to other studiesCitation17,Citation18 while different from several other studies.Citation19–21 The difference in the percentage of knowledge can be attributed to a variation in the analysis’s score, the number of items utilized to measure knowledge, sociocultural traits, and the use of the different questionnaires. Among study participants, responses were better in several questions regarding DM knowledge than in an Ethiopian study.Citation17 A study reported moderate knowledge among healthy adults regarding DM, while the attitude and practices were good and poor, respectively.Citation22 An Indian study reported adequate DM knowledge among study participants, while their attitude and practices toward DM prevention were not good.Citation23 The disparity in results may be attributed to educational level differences. The literacy rate in KSA is 99.38%,Citation24 which is substantially higher than in several other countries and could be one of the causes for superior knowledge among our study participants.
In the current study, less than half of the participants had positive attitudes, while two-thirds practiced good DM-avoidance behavior. This contrasts with the fact that fewer people had positive attitudes than those who demonstrated good practicing behavior. In most cases, the attitude is mirrored in practice. One plausible explanation is that approximately half of the study participants were students, and the younger generation is more physically active and goes to gyms to stay fit and healthy. According to a recent Ethiopian study, two-thirds of the participants were knowledgeable about DM, nearly half had positive attitudes, and one-third had good practicing behavior.Citation25 This study’s KAP results were favorable because 89% of study participants had a family history of diabetes and 6% had diabetes.
Our study results regarding participants with a family history of DM concur with a few other studies.Citation26,Citation27 In our study, about 60% of the participants had a family history of DM, which is a much higher percentage than in a few other studies.Citation22,Citation28 The greater incidence of diabetes in SA could be one factor for the higher frequency of diabetes in the family. In contrast to our study, one study found that 89% of study participants had a family history of diabetes.Citation25 This is the highest percentage of participants with a family history of diabetes reported in the literature. The authors did not explain the high percentage of diabetes in the family, despite the fact that the overall DM prevalence in Ethiopia is around 6.5%.Citation29 The reason could be a small size (less than 400), and selection criteria.
In the current study, participants with a family history of DM were likelier to have better knowledge, positive attitudes, and good preventive practices than those without DM family history. Our results are like another Saudi study.Citation15 These results were expected because they had someone with the disease in the family and found them having various food restrictions and not enjoying the religious and non-religious festivities. Their celebrations on different occasions were generally limited due to their DM problems.Citation30 As a result, their implicit knowledge and attitude towards diabetes, as well as prevention strategies, improved compared to individuals who did not have a DM member in their family. Another reason could be that they want to take diligent care of their loved ones; therefore, they educate themselves on diabetes. According to Karim and Habib (2022), having a close friend or family member who has diabetes can pique a person’s interest in learning more about the disease.Citation31
Most participants had good preventive practices. Our study results are higher than a Kenyan studyCitation32 because Kenyan comprised both urban and rural communities, each with a varied level of knowledge. In contrast to the present study results, a Pakistani study reported that self-care in the form of a yearly checkup by the physician, monitoring their body weights, avoiding tobacco, taking adequate sleep, and doing moderate exercise was not up to the mark among students.Citation33
Similar to our results, no gender-wise differences have been reported in participants knowledge by various studies.Citation23,Citation34,Citation35 Unlike our findings, a Saudi study reported better knowledge scores among females than males and a significant association of the feminine gender with knowledge and attitude.Citation15 Pakistani and Bangladeshi studies have reported higher knowledge among men than women.Citation18,Citation36 The lack of gender differences could be explained by the fact that males and females have more than 90% literacy rate and equal access to knowledge resources.
The present study found that master’s and Ph.D. degree holders were likelier to have positive attitudes and good practices for averting DM. These results are understandable because people with higher qualifications generally have better attitudes and practices for preventing communicable and non-communicable diseases. Because of their education, they have more awareness and access to knowledge. Another reason could be that people with lower levels of education may be less able to read and comprehend the information they encounter.
Our results are similar to another study that explained patients with higher levels of education are more likely to acquire diabetes-related informative resources such as brochures and manuals.Citation17 Additionally, they have better time management skills and give time to themselves by performing physical activities and excursions. They can also easily interact with medical professionals if they have questions.Citation17
Our study showed that monthly income did not significantly correlate with good knowledge and positive attitude; these results are incompatible with a few other studies showing that better knowledge was associated with higher income.Citation20,Citation28,Citation37 For this result, we do not have an appropriate explanation.
Our results did not find an association between age and DM knowledge similar to a Qatari study.Citation38 In contrast to our findings, Austrian, Gambian and Saudi studies found that older people have better DM knowledge than younger people.Citation39–41 Our results found that good knowledge, positive attitudes, and good practice scores were not associated with each other. These results are similar to another Saudi study.Citation42 They explained this non-association between variables knowledge, attitudes, and practices by stating that because all participants in the survey were non-diabetic individuals, their knowledge and attitudes toward the disease may not have been influenced by personal considerations or worries associated with having DM or deeming they are prone to DM.
The present study results showed that there is still a need to work more to enhance common peoples’ DM knowledge. More public awareness about any disease could help to reduce its prevalence. Diabetes education focusing on amendable risk factors is more valuable than pharmacological therapies for the disease.Citation38 Adequate knowledge, optimism, and proactive commitment to healthy behavior are the foundations of preventive and early intervention to combat the diabetes epidemic.Citation38
There is a need to start a campaign on social media regarding DM prevention strategies. Booklets, pamphlets, and flyers should be distributed among the masses to increase their awareness regarding this silent but dangerous disease. Universities and medical schools should hold small camps and awareness seminars in big shopping malls, along the corniche, and in schools and colleges to educate students and the general public about the importance of maintaining healthy body weight, quitting smoking, getting regular exercise, having their blood sugar and blood pressure checked regularly, and avoiding fast food.Citation43 There is a need to initiate community awareness campaigns by involving the community and local religious leaders because they have direct contact and influence on the general public, and they can convince them easily to adopt a healthy lifestyle necessary to avoid DM and its consequences.
The present study has a few limitations. Firstly, one issue with questionnaire research is that people tend to choose the “right” answer rather than the one that reflects their real-life knowledge, perspectives, and behavior. Secondly, the online nature of the study was one of the drawbacks and we were unable to reach the participants who did not use social media apps. Thirdly, regarding the KAP of the people residing Makkah region, it’s possible that in the other areas, people have different KAP. Therefore, the results cannot be generalized.
Conclusion
Diabetes prevention is built on knowledge, optimism, and an active commitment to healthy behavior. The present KAP study results are promising because more than half of the participants showed positive attitudes, enough knowledge, and effective behavior toward DM prevention. Diabetes education that addresses risk factors will be more effective. Public awareness of any disease could lower its prevalence. The current study’s findings are useful for policymakers in targeting at-risk populations by filling in gaps in information, attitudes, and practices related to DM, an important health issue in KSA. Effective mass campaigns utilizing digital and social media channels should be the emphasis of future efforts to enhance common people’s knowledge and educate them.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
The authors would like to thank all of the medical students who assisted with data collection, particularly Abdulmalik Saleh Almarshad, Razan Omer Alsubhi, Mashael Ahmed Alamri, Fatemah Mohammad Alshariff, Zainab Ali Khamis, and Yara Basim Alahmadi.
References
- Khabaz MN, Bakarman MA, Baig M, et al. Dietary habits, lifestyle pattern and obesity among young Saudi university students. J Pak Med Assoc. 2017;67:1541–1546.
- Baig M, Gazzaz ZJ, Gari MA, et al. prevalence of obesity and hypertension among University students’ and their knowledge and attitude towards risk factors of Cardiovascular Disease (CVD) in Jeddah, Saudi Arabia. Pak J Med Sci. 2015;31:816–820. doi:10.12669/pjms.314.7953
- Al Dawish MA, Robert AA, Braham R, et al. Diabetes mellitus in Saudi Arabia: a review of the recent literature. Curr Diabetes Rev. 2016;12:359–368. doi:10.2174/1573399811666150724095130
- CDC. National diabetes statistic report; 2020.
- International Diabetes Federation. IDF Diabetes Atlas. 8th ed. Brussels, Belgium: International Diabetes Federation; 2017.
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
- Alsulami S, Baig M, Ahmad T, et al. Obesity prevalence, physical activity, and dietary practices among adults in Saudi Arabia. Front Public Health. 2023;11:1124051. doi:10.3389/fpubh.2023.1124051
- Kyrou I, Tsigos C, Mavrogianni C, et al. Sociodemographic and lifestyle- related risk factors for identifying vulnerable groups for type 2 diabetes: a narrative review with emphasis on data from Europe. BMC Endocr Disord. 2020;20. doi:10.1186/s12902-019-0463-3
- Ganu D, Fletcher N, Caleb NK. Physical disability and functional impairment resulting from type 2 diabetes in sub-Saharan Africa: a systematic review. African J Diabetes Med. 2016;24:10–14.
- Cranor CW, Christensen DB. The Asheville project: short-term outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc. 2003;43:149–159.
- Moodley L, Rambiritch V. An assessment of the Level of knowledge about diabetes mellitus among diabetic patients in a primary healthcare setting. South African Fam Pract. 2007;49:16. doi:10.1080/20786204.2007.10873652
- Alemayehu AM, Dagne H, Dagnew B. Knowledge and associated factors towards diabetes mellitus among adult non-diabetic community members of Gondar city, Ethiopia 2019. PLoS One. 2020;15:e0230880. doi:10.1371/journal.pone.0230880
- Spronk I, Kullen C, Burdon C, et al. Relationship between nutrition knowledge and dietary intake. Br J Nutr. 2014;111:1713–1726. doi:10.1017/S0007114514000087
- Alzahrani S, Alshammari M, Alsebyani A, et al. Knowledge, attitude, and practice regarding diabetes mellitus among general public and diabetic patients in Riyadh, Saudi Arabia. Asian J Pharma. 2018;12:154.
- Gazzaz ZJ. Knowledge, attitudes, and practices regarding diabetes mellitus among university students in Jeddah, Saudi Arabia. Diabetes Metab Syndr Obes. 2020;13:5071. doi:10.2147/DMSO.S287459
- Oraibi OH, Sanguf M, Gadi W, et al. Awareness of diabetes mellitus and its risk factors among the Saudi non-diabetic population in Jazan Region, Saudi Arabia. Int J Diabetes Dev Ctries. 2022;6:1369–1374.
- Kassahun CW, Mekonen AG. Knowledge, attitude, practices and their associated factors towards diabetes mellitus among non diabetes community members of Bale Zone administrative towns, South East Ethiopia. A cross-sectional study. PLoS One. 2017;12:e0170040. doi:10.1371/journal.pone.0170040
- Fatema K, Hossain S, Natasha K, et al. Knowledge attitude and practice regarding diabetes mellitus among non-diabetic and diabetic study participants in Bangladesh. BMC Public Health. 2017;17:364. doi:10.1186/s12889-017-4285-9
- Ulvi OS, Chaudhary RY, Ali T, et al. Investigating the awareness level about diabetes mellitus and associated factors in Tarlai (rural Islamabad). J Pak Med Assoc. 2009;59:798–801.
- Minhat HS, Hamedon TR. Understanding towards diabetes mellitus among rural adult community in Malaysia. World J Med Sci. 2014;11:217–221.
- Moira A, Souza PD, Kundapur R, et al. A cross sectional study to determine the prevalence of diabetes mellitus and its household awareness in the rural field practice areas of a medical college in Mangalore—a pilot study. Nitte Univ J Heal Sci. 2015;5:4–7.
- Tekanene MU, Mohammadnezhad M, Khan S, et al. Knowledge, attitude and practice (KAP) related to type 2 diabetes mellitus (T2DM) among healthy adults in Kiribati. Glob J Health Sci. 2021;13:1. doi:10.5539/gjhs.v13n5p10
- Chandrethia R. KAP–knowledge, attitude, and practice & prevalence study of diabetes mellitus among morning walkers in the City of Ahmedabad. Nati J Med Res. 2022;12:64–68.
- Literary rate in Saudi Arabia. Available from: https://www.globaldata.com/data-insights/macroeconomic/literacy-rate-in-saudi-arabia. Accessed May 11, 2023.
- Simachew A, Temesgen H. Knowledge, Attitude, practice, and their associated factor towards Diabetes Mellitus among peoples live in Debre Markos Town, North West Ethiopia, Amhara Regional State, Ethiopia 2020 GC. J Nov Psy. 2022;3:65–75.
- Xu Y, Zhang D, Liu K, et al. Self-reported knowledge on diabetes and its related factors among Chinese college students: a cross-sectional study. BMJ Open. 2016;6:e011963. doi:10.1136/bmjopen-2016011963
- Al Shafaee MA, Al-Shukaili S, Rizvi SG, et al. knowledge and perceptions of diabetes in a semi-urban Omani population. BMC Public Health. 2008;8:249. doi:10.1186/1471-2458-8-249
- Asmamaw A, Asres G, Negese D, et al. Knowledge and attitude about diabetes mellitus and its associated factors among people in Debre Tabor Town, Northwest Ethiopia: cross sectional study. Sci J Public Heal. 2015;3:199–209. doi:10.11648/j.sjph.20150302.17
- Zeru MA, Tesfa E, Mitiku AA, et al. Prevalence and risk factors of type-2 diabetes mellitus in Ethiopia: systematic review and meta-analysis. Sci Rep. 2021;11:21733. doi:10.1038/s41598-021-01256-9
- Gazzaz ZJ, Baig M, Kanpurwala MA, Jamil T, Mojaddidi MA, Murad MA. Eid-al-Fitr festivity and Ramadan fasting attitude among individuals with diabetes from Saudi Arabia and Pakistan: a cross-sectional study. BMJ Open. 2022;12(9):e054902. doi:10.1136/bmjopen-2021-054902
- Karim RA, Habib HA. Awareness regarding diabetes risk factors, prevention and management among community members in Diyala/Baqubah. AL-Kindy Coll Med J. 2022;18:24–29. doi:10.47723/kcmj.v18i1.272
- Maina WK, Ndegwa ZM, Njenga EW, et al. Knowledge, attitude, and practices related to dia- betes among community members in four provinces in Kenya: a cross-sectional study. African J Diabetes Med. 2011;19:15–18.
- Khan R, Rehman R, Baig M, et al. Dimensions of physical wellness among medical students of public and private medical colleges in Pakistan. Saudi Med J. 2015;36:754. doi:10.15537/smj.2015.6.11108
- Ahmed IB, Alateeq FA, Alharbi SH, et al. Awareness and knowledge towards type 2 diabetes mellitus risk factors in Northern Saudi Arabia. Int J Med Res Health Sci. 2018;7:33–40. doi:10.15537/smj.2018.10.22938
- Wadaani FA. The knowledge attitude and practice regarding diabetes and diabetic retinopathy among the final year medical students of King Faisal University Medical College of Al Hasa region of Saudi Arabia: a cross sectional survey. Niger J Clin Pract. 2013;16(2):164–168. doi:10.4103/1119-3077.110133
- Memon MS, Shaikh SA, Shaikh AR, et al. An assessment of knowledge, attitude and practices (KAP) towards diabetes and diabetic retinopathy in a suburban town of Karachi. Pak J Med Sci. 2015;31:183–188. doi:10.12669/pjms.311.6317
- Rathod GB, Rathod S, Parmar P, et al. Study of knowledge, attitude and practice of general population of Waghodia towards Diabetes mellitus. Int J Cur Res Rev. 2014;6:63–68.
- Al-Mutawaa KA, Farghaly AH, Nasir R, et al. Level of knowledge, attitude and practice towards diabetes among nationals and long-term residents of Qatar: a cross-sectional study. BMJ Open. 2022;12:e052607. doi:10.1136/bmjopen-2021-052607
- Aljofan M, Altebainawi A, Alrashidi MN. Public knowledge, attitude and practice toward diabetes mellitus in hail region, Saudi Arabia. Int J Gen Med. 2019;12:255–262. doi:10.2147/IJGM.S214441
- Dorner TE, Lackinger C, Schindler K, et al. Health information regarding diabetes mellitus reduces misconceptions and underestimation of consequences in the general population. Public Health Nutr. 2013;16:2032–2039. doi:10.1017/S1368980012003886
- Nkoka O, Ntenda PA, Phiri YV, et al. Knowledge of diabetes among Gambian adults: evidence from a nation-wide survey. BMC Cardiovasc Disord. 2022;22:145. doi:10.1186/s12872-022-02591-z
- Abdullah I, Ahmed B, Alosaimi ME, et al. Knowledge, attitude, and practices towards diabetes mellitus among non-diabetes community members of Riyadh, Kingdom of Saudi Arabia. Int J Pharm Res Allied Sci. 2020;9:41–51.
- Alsulami S, Althagafi N, Hazzazi E, et al. Obesity and its associations with gender, smoking, consumption of sugary drinks, and hour of sleep among King Abdulaziz University Students in Saudi Arabia. Diabetes Metab Syndr Obes. 2023;16:925–934. doi:10.2147/DMSO.S405729