
Abstract
Nonalcoholic fatty liver disease (NAFLD), as a multisystemic disease, is the most prevalent chronic liver disease characterized by extremely complex pathogenic mechanisms and multifactorial etiology, which often develops as a consequence of obesity, metabolic syndrome. Pathophysiological mechanisms involved in the development of NAFLD include diet, obesity, insulin resistance (IR), genetic and epigenetic determinants, intestinal dysbiosis, oxidative/nitrosative stress, autophagy dysregulation, hepatic inflammation, gut-liver axis, gut microbes, impaired mitochondrial metabolism and regulation of hepatic lipid metabolism. Some of the new drugs for the treatment of NAFLD are introduced here. All of them achieve therapeutic objectives by interfering with certain pathophysiological pathways of NAFLD, including fibroblast growth factors (FGF) analogues, peroxisome proliferator-activated receptors (PPARs) agonists, glucagon-like peptide-1 (GLP-1) agonists, G protein-coupled receptors (GPCRs), sodium-glucose cotransporter-2 inhibitors (SGLT-2i), farnesoid X receptor (FXR), fatty acid synthase inhibitor (FASNi), antioxidants, etc. This review describes some pathophysiological mechanisms of NAFLD and established targets and drugs.
Introduction
The global prevalence of nonalcoholic fatty liver disease (NAFLD) is 25% and is the leading cause of cirrhosis and hepatocellular carcinoma.Citation1 NAFLD is defined as the presence of steatosis and metabolic risk factors (especially obesity and type 2 diabetes) in more than 5% of liver cells and the absence of excessive alcohol consumption (≥ 30 g per day for men and ≥ 20 g per day for women) or other chronic liver diseases.Citation2 NAFLD is a series of histopathological changes. It can be divided into nonalcoholic simple fatty liver (NAFL) and nonalcoholic steatohepatitis (NASH). NAFL can be considered present when there is more than 5% steatosis in the liver. The presence of steatosis, hepatic ballooning, and hepatic lobular inflammation can be considered NASH. NASH is characterized by necrotic inflammation and faster fibrotic progression than nonalcoholic fatty liver disease. Both two of these stages have the potential to progress to cirrhosis.Citation3 NAFLD is bidirectionally associated with components of metabolic syndrome.Citation4 Type 2 diabetes increases the risk of cirrhosis and related complications. Although the leading causes of death in patients with NAFLD are cardiovascular disease and extrahepatic malignancy, advanced liver fibrosis is a key prognostic indicator for liver-related outcomes and overall mortality.Citation5 The degree of fibrosis can be assessed by a variety of non-invasive tests. Although several drugs to treat NAFLD are currently in the advanced stages of development, there are currently no approved NAFLD treatments. Due to the complex pathophysiology and heterogeneity of the disease phenotype, many patients with NAFLD may require combination therapy. A healthy lifestyle and weight loss remain important in the prevention and treatment of NAFLD.Citation6
In this review, we discuss NAFLD, the underlying molecular mechanisms of NASH pathogenesis and the development of novel drugs associated with it.
Pathogenesis of Nonalcoholic Fatty Liver Disease
NAFLD Development Mechanism
The pathogenic mechanism of NAFLD’s development and progression to NASH is quite complex and has not been fully understood by scientific research over the past decade. Once the two-factor theory is replaced by the multifactorial hypothesis, it will show that more than just one or two mechanisms can explain the pathogenesis of NAFLD and progression to NASH. It is more likely that multiple factors play a role in the same time.Citation7
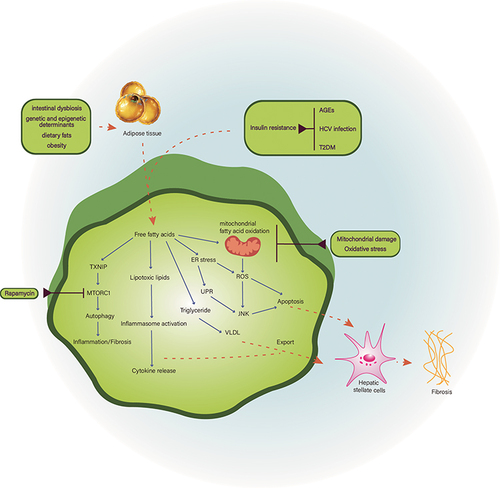
The main feature of hepatic steatosis is excessive fat accumulation in liver cells, which is formed due to the breakdown of the liver’s homeostasis between lipid acquisition and breakdown. There are two main sources of liver lipids in the form of free fatty acids (FFA), namely lipolysis of triglycerides (TG) in adipose tissue and synthesis by de novo lipogenesis (DNL) pathways. Lipids are broken down by mitochondrial fatty acid oxidation (FAO) and production of very low-density lipoprotein (VLDL). If the injury occurs somewhere on the way, it can lead to the production of toxic lipid metabolites that further induce hepatocellular stress, in other words, lipotoxicity. This is the first step in the pathway from simple steatosis to NASH.Citation8
Multiple parallel hypotheses promote several factors that collectively contribute to the development of NAFLD, such as diet, obesity, insulin resistance (IR), genetic and epigenetic determinants and intestinal dysbiosis. The key factor in this theory may be IR. IR dysregulation causes fat breakdown in adipose tissue, thereby increasing the accumulation of FFAs in the liver. On the other hand, in obese patients, adipose tissue dysfunction eventually occurs, which also leads to increased uptake of FFAs by the liver, inducing lipid synthesis and gluconeogenesis, which further promotes insulin resistance in the liver.Citation9 Animal studies have shown that obesity in mice stimulate the secrets of dipeptidyl peptidase 4 (DPP4), which promotes insulin resistance and liver inflammation.Citation10 Studies have shown higher levels of advanced glycation end products (AGEs) in NASH compared with healthy controls or patients with simple steatosis.Citation11 These findings suggest that AGEs are associated with inflammation. Whether IR was before or after NAFLD occurred is difficult to say, but the link between them is undeniable. Recently, studies have shown that eradication of HCV infection (with direct-acting antivirals) improves IR and thereby reduces the chance of developing diabetes and cardiovascular disease.Citation12–14 This new observation indirectly confirms the role of IR in the relationship between NAFLD and atherosclerotic disease. In summary, IR is the most associated common causative feature of NAFLD and metabolic syndrome, as well as a common clinical feature of these disorders.Citation14,Citation15 In addition, results reported by Masarone suggest that liver injury is associated with progressive clinical manifestations of IR, and the histological features of NASH are observed on liver biopsy in 98% of T2DM patients, suggesting that NASH may be one of the early complications of T2DM, as they are both pathophysiologic associated with IR.Citation16
Dysfunction of the endocannabinoid system (ES) has been found to be associated with metabolic disorders related to nonalcoholic fatty liver disease (NAFLD). Studies show both of ES and cannabinoid receptor type 1 (CB1) are associated with oxidative/nitrosative stress and may also play a role in modulating liver inflammation, ultimately promoting disease progression toward steatohepatitis.Citation17,Citation18 Studies have shown that endocannabinoids can contribute to oxidative stress in NAFLD through CB1 receptors. Oxidative stress and inflammation are linked bidirectionally. Additionally, liver cell injury and apoptosis can be promoted by lipid peroxidation, increased production of cytokines and ROS, as well as induction of Fas ligand, ultimately accelerating the transition to NASH.Citation17 CB1 receptors are expressed in low amounts in normal liver, but they are significantly upregulated in stellate cells, hepatic vascular endothelial cells, and monocytes during hepatic pathology due to endocannabinoid system activation. Animal studies showed that high fat diet (HFD) increases hepatic levels of CB1 density which prove CB1 might lead to hepatic steatosis when linked to a high fat diet, obesity, and alcohol.Citation19 In relation to, hepatic fat production can be reduced by lowering CB1 receptors in the liver, thereby improving dyslipidemia and slowing down the progression of liver cell damage.Citation20 In this approach, CB1 receptor antagonists may be effective in the treatment of NAFLD. CB1 receptor antagonists have been found to possibly improve hepatocellular damage to iron-related oxidative stress by improving disorders of iron metabolism.Citation17
Autophagy dysregulation is related to the progression of NASH, with studies showing that upregulation of hepatic TXNIP (thioredoxin interacting protein) genes in both NAFLD patients and mice fed MCD diets is positively associated with autophagy dysregulation. Mechanistically, TXNIP regulates the inactivation of mechanistic target of rapamycin kinase complex 1 (MTORC1), thereby promoting autophagy. Inhibition of MTORC1 and induction of autophagy by rapamycin has been shown to attenuate diet-induced steatosis, inflammation, and fibrosis in MCD. Therefore, targeting TXNIP may be a potential approach for treating NASH.Citation21
Nonalcoholic fatty liver disease (NAFLD) associated with type 2 diabetes mellitus (T2DM) is frequently characterized by decreasing gut barrier function and a disturbed gut-liver axis, perhaps due to exposure to hazardous chemicals such as antigens, metabolites, and gut microorganisms. This may worsen hepatic inflammation, eventually leading to severe liver disease characterized by cirrhosis and portal hypertension.Citation22,Citation23 Bacterial endotoxin-induced metabolic endotoxemia can result in intestinal barrier dysfunction, which has been identified as a cause of systemic inflammation.Citation24 Self-maintaining macrophages, immune cells that help maintain intestinal homeostasis and regulate intestinal motility and secretion, rely heavily on the presence of intestinal microbiota.Citation25,Citation26 Research has demonstrated that the gut microbiota can contribute to diet-induced obesity by affecting FXR signaling and bile acid profiles, ultimately promoting hepatic steatosis.Citation27
Progression to NASH-Lipotoxicity, Organelle Distress, and Inflammasome Activation
There is a strong correlation at the cellular and organ levels in the pathogenesis of NASH, especially given the fat-liver and gut-liver axis relationships. Once toxic lipids are metabolized, hepatocytes enter different types of states, which then trigger cascading processes that lead to the development of NASH. In addition to saturated fatty acids such as palmitate and stearate, these toxic lipid molecules include diacylglycerol, ceramides, lysophosphatidylcholine (LPC), and free cholesterol. At the molecular level, lipotoxicity leads to organelle stress and dysfunction, inflammasome activation, and ultimately cell death and activation of inflammatory responses.Citation3,Citation28 Hepatic lipotoxicity may occur because the accumulated liver lipids stimulate the secretion and increase the activity of IL-11 protein, which upregulate NOX4 expression to increase the production of reactive oxygen species. Hepatocytes mitochondria and fatty acid metabolism could be damaged by reactive oxygen species, which accelerate the progression of hepatic steatosis. IL-11 can also promotes fibrosis in hepatic stellate cells.Citation29 Given the major role of hepatic lipid balance in the pathogenesis of NASH, treatment strategies can be considered in terms of reducing fat inflow into the liver or enhancing fat metabolism in the liver. This can be achieved, for example, by increasing fatty acid oxidation (FAO), inhibiting de novo lipogenesis (DNL), increasing fatty acid desaturation, and improving IR. Hepatocyte injury will lead to macrophage-mediated inflammation and hepatic stellate cell activation, which constitute a key triad for the development of NASH. Lipotoxic substances may activate the mechanism of apoptosis in hepatocytes through intrinsic or extrinsic (death receptor) pathways. Major molecular signaling occurs via c-Jun-N terminal kinase (JNK).Citation30 The JNK pathway is known to be stimulated by oxidative stress (OS) and endoplasmic reticulum (ER) stress. At the organelle level, FFA and its derivatives induce mitochondrial hyperfunction, followed by mitochondrial dysfunction, leading to elevated levels of reactive oxygen radicals (ROS), the culprit of oxidative stress.Citation31 Saturated FFAs, especially lipoprotein complexes (LPCs) derived from them, can also accumulate in the endoplasmic reticulum (ER) and trigger ER stress, which stimulates an unfolded protein response (UPR), an attempt by ER to re-establish its homeostasis. However, prolonged activation of UPR leads to activation of JNK, glycogen synthase kinase 3 (GSK3), and transcription factor CCAAT/enhancer-binding homologous protein (CHOP), all of which upregulate pro-death proteins such as p53 up-regulation of apoptosis regulators (PUMA) and extrinsic pathways including tumor necrosis factor (TNF)-associated apoptosis-inducing ligands (TRAIL) to induce cell death through transcriptional upregulation of TRAIL receptor 2 (TRAIL-R2) expression. When the outer mitochondrial membrane is permeabilized, both pathways converge at the mitochondrial level, resulting in cytochrome C release, caspase activation, and apoptosisCitation32 ().
Figure 1 Pathogenesis of nonalcoholic fatty liver disease. The pathogenesis of NAFLD is complex and currently considered to be associated with insulin resistance, mitochondrial damage, oxidative stress and intestinal dysbiosis, etc.
The Latest Therapeutic Targets and Representative Drugs of NAFLD
FGF Analogues
FGF21
FGF21 is one of the members of the FGF family. Because of its insulin-sensitizing and hepatoprotective properties, it has become one of the therapeutic hormones for NAFLD.Citation33 In addition, FGF21 has shown its triglyceride-lowering effect in animal models as well as human studies.Citation34 The latter increases the morbidity and mortality of NASH by increasing cardiovascular events. In addition, FGF21 increases the level of adiponectin, which is a kind of adipokine with insulin sensitization, anti-fat, anti-inflammatory and anti-fibrotic effects.Citation35,Citation36
Pegbelfermin, the FGF21 analog, demonstrated by a recent Phase IIa clinical trial, that it can reduce hepatic fat content in patients with NASH. However, in chronic treatments with pegbelfermin, there is a high chance that anti-pegbelfermin and anti-FGF21 antibodies will form, which have been raised concerns about immunogenicity issues.Citation24 Besides, NGMBio is developing a once-monthly formulation, the antibody NGM313, which reduces liver fat content, HbA1c, and transaminases in non-diabetic NAFLD patients by activating the β-Klotho-FGFR1c complex.
Finally, some safety issues for long-term treatment of FGF21 analogues, such as cardiovascular side effects and bone loss, remain unresolved.Citation37
FGF19
FGF19 is a regulator of bile acid synthesis produced by intestinal cells after meals in response to farnesoid X receptor (FXR) stimulation. Because this nutritionally regulated hormone is positively correlated with food intake and there is insufficient evidence that this effect still works in the fasted state, its target population is the NAFLD patients with metabolic syndrome or insulin resistance.Citation38 In addition, FGF19 also has the effect of regulating energy homeostasis, stimulating sugar production, and inhibiting gluconeogenesis. It also reduces lipogenesis by blocking insulin signaling, thereby reducing fat accumulation in the liver.Citation39,Citation40
Recent FGF19-targeted drug developments related to NAFLD include the FGF19 analogue NGM282 and FXR agonists. Obeticholic acid (OCA) is the most reported one as a member of FXR agonists.Citation41
PPARs
There are three different isoforms of peroxisome proliferator-activated receptors (PPARs), namely α, β/δ, and γ. They have the effect of regulating lipid and carbohydrate metabolism.
In NASH, PPARα not only improves lipid metabolism by controlling lipid flux, regulating fatty acid transport, and β oxidation,Citation42 but also reduces liver inflammation by reducing visceral inflammation and intestinal permeability. In the case of cirrhosis, PPARα can reduce portal pressure glucose and lipoprotein metabolism and insulin resistance in skeletal muscle.
PPARβ/δ is highly expressed in human sinusoidal endothelial cells and hepatic macrophages, regulating the expression of key genes involved in innate immunity and inflammation.Citation43
PPARγ regulates insulin sensitivity in adipose tissue, prevents activation of hepatic stellate cells, and thus reduces the incidence of liver fibrosis.Citation44 In addition, against the background of cirrhosis, PPARγ reduces portal venous pressure, visceral inflammation, angiogenesis, and portosystemic shunting.
Pioglitazone is a PPAR gamma agonist (thiazolidinedione) that has been shown to reduce the occurrence of hepatic steatosis and lobular inflammationCitation45 and has cardiometabolic benefits.Citation46,Citation47 However, long-term use has been reported to alter bone metabolism and increase fracture riskCitation48 and increase mortality in patients with heart failure due to its fluid retention effects.Citation49
GLP-1
Glucagon-like peptide-1 (GLP-1) is a naturally occurring hormone secreted by enteroendocrine cells (EEC) of the gastrointestinal tract (GIT) and affected by dietary intake. It can regulate glucose metabolism and energy homeostasis by regulating the secretion of islet hormones and glucagon, and can also achieve weight loss by delaying gastric emptying and inhibiting small intestinal peristalsis leading to decreased appetite and delayed food absorption.Citation50 GLP-1R analogues mimic the effects of glucagon-like peptide-1 (GLP-1)Citation51 GLP-1 also regulates the immune system by suppressing inflammation.Citation52 This suggests that GLP-1 analogues can improve insulin sensitivity in NAFLD patients.
StudiesCitation50,Citation53 have shown GLP-1 analogues, liraglutide, and exenatide, to reduce the levels of liver enzymes in the serum of NAFLD patients.Citation54 It has also been shown to reduce liver enzymes in patients with diabetes and obesity.Citation55 Not only that, but they have also been found to improve the histological characteristics of the liver by promoting the oxidation of fatty acids,Citation56 steatosis of the liver,Citation57 significantly reducing liver fat content (LFC),Citation58 effectively regulating inflammation caused by fat accumulation in the liver.Citation54 Finally, exenatide treatment appears to be more effective than liraglutide treatment in improving liver enzymes and weight loss.Citation59
GPCRs
G protein-coupled receptors (GPCRs) are an umbrella term for a large class of membrane proteins that mediate a variety of extracellular ligands, including hormones, neurotransmitters, and chemokines.Citation60
Many GPCRs affect NAFLD metabolism by being activated by short-chain fatty acids (SCFAs) and bile acids (BAs). SCFAs activate intestinal cells and regulate intestinal immune responses by activating GPCRs (for example, GPR41/FFAR3 and GPR43/FFAR2) and inhibiting histone deacetylase.Citation61 In addition, GPCRs regulate SCFA-mediated inflammatory responses. SCFAs have also been associated with fructo-oligosaccharides for the improvement of steatohepatitis and chronic inflammation.Citation62 BAs may reduce the incidence of liver and gastrointestinal inflammation by activating nuclear FXR and GPCR signaling.Citation63,Citation64 GPCRs are also members of the intestinal-hepatic axis and regulate the secretion of intestinal hormones (for example, GLP-1) to improve lipid accumulation and fibrosis.Citation65,Citation66
Compared with other NAFLD therapies, targeted GPCRs have outstanding advantages in the treatment of NAFLD. Functional selection of GPCR ligands helps reduce side effects of treatment. GPCRs act on the entire process of NAFLD development, such as lipid accumulation, inflammation and fibrosis. Therefore, targeted GPCRs can be applied to different stages of NAFLD treatment, such as steatosis, NASH, liver fibrosis, and liver cancer.
SGLT-2i
Sodium-glucose co-transporter-2 (SGLT-2) is highly expressed in the proximal tubular cells of the kidneys and is responsible for filtering glucose reabsorption.Citation67
In animal study, Nasiri-Ansari et al found empagliflozin, SGLT-2 inhibitor can attenuate the progress of NAFLD in apoE((-/-)) mice by activating autophagy and reducing ER stress and apoptosis.Citation68
SGLT2i lowers blood glucose by inhibiting glucose reabsorption and increasing the excretion of glucose in the urine. In addition, they can reduce blood volume, reduce body weight and fat mass, and lower blood pressure through osmotic diuresis.Citation61,Citation69,Citation70 They have also been shown to have cardioprotective properties for the heart and kidneys.Citation71–73 And it is currently approved for use in patients with T2DM.
More than half of patients with T2DM also have NAFLD. This seems to prove a bidirectional pathological relationship between type 2 diabetes and NAFLD. In other words, having one disease increases the probability of the other.Citation74 This may be due to their pathophysiologic association with insulin resistance.
Several studies have shown that SGLT2i can reduce the incidence of NAFLD in patients with T2DM, improve liver aminotransferases, blood lipids, blood glucose, insulin resistance and reduce body weight.Citation75,Citation76 And it further attenuates liver fat deposition, liver inflammation and liver fibrosis.Citation65,Citation77 However, YAN H reported that it shows no apparent effect in improving IR in NAFLD compared with GLP-1 RAs.Citation78
FXR
The farnesoid X receptor (FXR) belongs to the gene family of nuclear receptors and is highly expressed in the gastrointestinal tract. As an endogenous ligand for bile acids, FXR regulates bile acid production and integrates and regulates glucose, lipid, and energy metabolism.Citation79,Citation80 The FXR nuclear receptor plays a key role in preserving hepatic homeostasis. By blocking de novo lipogenesis via SREBP-1c, this receptor is engaged to lessen lipotoxicity while also boosting mitochondrial β-oxidation and cholesterol excretion. These activities slow the growth of fibrosis, inflammation, and insulin resistance. In addition, Bile acids can stimulate the production of antimicrobial peptides by binding to FXR. These peptides can inhibit the growth of intestinal probiotics and disrupt intestinal barrier function.Citation81
Obeticholic acid (OCA), the natural agonist of the farnesoid X receptor, could decreases insulin resistance and hepatic steatosis in preclinical research. In a Phase 2 trial, patients with type 2 diabetes mellitus and nonalcoholic fatty liver disease were randomly assigned to given placebo, 25 or 50 mg OCA for 6 weeks, it shows increased insulin sensitivity (by 28.0% from baseline with 25 mg OCA (P=0.019) and 20.1% from baseline with 50 mg OCA (P=0.060)), and decreased biological indicators of liver inflammation and fibrosis (NCT00501592).Citation82
In a multicentre, randomised trial, 282 patients with biopsy evidence of non-alcoholic steatohepatitis, 25 mg OCA or placebo was randomly assigned to patients once a day. Patients given obeticholic acid showed improvement in fibrosis, hepatocellular ballooning, steatosis, lobular inflammation, the mean change in the NAFLD activity score (change from baseline=–1·7 vs –0·7; p<0.0001) and biochemical markers for the liver, like serum alanine aminotransferase and aspartate aminotransferase, when compared to placebo. Although there have been improvements in the individual histological features of nonalcoholic steatohepatitis (NASH), the proportion of patients with resolution of NASH remained unchanged. Pruritus was the only adverse event occurring more frequently with obeticholic acid than with placebo. Overall, the drug was well-received with no other significant adverse events reported (NCT01265498).Citation83
FASN Inhibitor
Fatty acid synthase (FASN) is a multi-enzyme protein that catalyzes the synthesis of palmitate from acetyl-CoA and malonyl-CoA in the de novo lipogenesis (DNL) pathway. There are studies confirmed that those with NAFLD have higher levels of FFA due to hepatic DNL which promotes liver fibrosis in various ways.Citation84 Additionally, it was confirmed that the level of FASN gene is significantly higher in the NAFLD patients compared with healthy individuals.Citation85 Therefore, FASN may be a potential therapeutic target for NAFLD treatment.
There is a a randomized, placebo-controlled trial, showing TVB-2640, a fatty acid synthase inhibitor, can significantly reduce excessive hepatic fat production, reduce insulin resistance, inflammation and reactive oxygen species production, and improve liver fibrosis in a dose-dependent manner (NCT03938246).Citation86
Antioxidant Treatment for NAFDL
The antioxidant activity of vitamins C and E reduces liver cell damage, and changes in serum vitamin D, vitamin B12, and folate levels are strongly associated with the severity of NAFLD.
Vitamin E
Vitamin E is a fat-soluble and powerful chain-breaking antioxidant in the human body that has the most significant evidence of therapeutic benefits in liver disease.Citation87 Vitamin E has the ability to reduce oxidative stress and slow the onset of NASH.Citation88 Vitamin E reduces the inflammatory response by increasing the expression of adiponectin and inhibits the expression of a variety of cytokines, including tumor necrosis factor-α (TNF-α), IL-1, IL-2, IL-4, IL-6, and IL-8. It also acts as a scavenger of hydroxyl, peroxyl, and superoxide radicals and stimulates superoxide dismutase (SOD) production. The proportional relationship between BCL2-associated with X (BAX) and Bcl-2 proteins is a key factor in determining the strength of inhibition of apoptosis. Vitamin E exerts an anti-apoptotic effect by enhancing levels of the anti-apoptotic protein, BCL-2, and reducing BCL2-associated with X (BAX) protein and p53 BCL-2. Although there is no standard regimen for the treatment of NAFLD/NASH, patients with NAFLD often require vitamin E supplementation.Citation89
Vitamin C
Vitamin C (ascorbic acid) is a powerful antioxidant that keeps the body healthy, slowing the progression of liver fibrosis by scavenging free oxygen radicalsCitation90 to reduce inflammation and activation of hepatic stellate cells (HSCs). Vitamin C treatment reduces oxidative stress in the liver. Ascorbic acid has also been suggested to modulate adiponectin to reduce lipid accumulation in the liver, systemic insulin resistance and inflammation, and to prevent NAFLD.Citation91,Citation92 In addition, ascorbic acid supplementation inhibits hepatic steatosis and stress by increasing mRNA levels in the liver ().
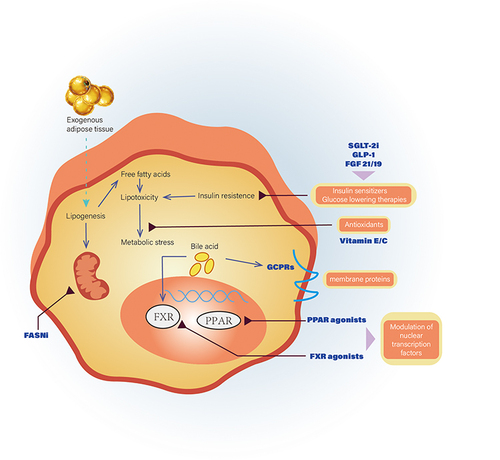
Figure 2 The latest therapeutic targets and representative drugs of NAFLD. This article lists a series of pathophysiological pathways of NAFLD, including fibroblast growth factors (FGF) analogues, peroxisome proliferator-activated receptors (PPARs) agonists, glucagon-like peptide-1 (GLP-1) agonists, G protein-coupled receptors (GPCRs), sodium-glucose cotransporter-2 inhibitors (SGLT-2i), farnesoid X receptor (FXR), fatty acid synthase inhibitor (FASNi) and antioxidants.
Conclusion
NAFLD, the most prevalent chronic liver disease in the world, places a significant burden on the world’s healthcare system because mortality and morbidity are not only connected to the liver but also to a number of extrahepatic organ systems. This article lists a series of pathophysiological pathways of NAFLD, including fibroblast growth factors (FGF) analogues, peroxisome proliferator-activated receptors (PPARs) agonists, glucagon-like peptide-1 (GLP-1) agonists, G protein-coupled receptors (GPCRs), sodium-glucose cotransporter-2 inhibitors (SGLT-2i), farnesoid X receptor (FXR), fatty acid synthase inhibitor (FASNi), antioxidants, etc. Recent studies have continued to provide new evidence strongly indicating that the gut microbiota may be a key link in the pathogenesis of NAFLD and its progression to NASH and cirrhosis. This is in addition to the previously established links between the various signaling pathways involved in the development of NAFLD. New treatments and targets are now being created concurrently with the rapid appearance of new data, which includes certain targets and pathways that are the subject of the aforementioned drug development. A multidisciplinary approach is needed for the evaluation of NAFLD in order to detect and treat this multisystem disease early and lessen the effects of this important public health issue. However, regardless of the progress of drug therapy in the treatment of NAFLD, maintaining a healthy lifestyle and losing weight remains important measures to prevent the onset of NAFLD and slow its progression.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
- European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–1402. doi:10.1016/j.jhep.2015.11.004
- Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S. Nonalcoholic Steatohepatitis: a review. JAMA. 2020;323(12):1175–1183. doi:10.1001/jama.2020.2298
- Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
- Powell EE, Jonsson JR, Clouston AD. Steatosis: co-factor in other liver diseases. Hepatology. 2005;42(1):5–13. doi:10.1002/hep.20750
- Wong VWS, Wong GLH, Chan RSM, et al. Beneficial effects of lifestyle intervention in non-obese patients with non-alcoholic fatty liver disease. J Hepatol. 2018;69(6):1349–1356. doi:10.1016/j.jhep.2018.08.011
- Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–1048. doi:10.1016/j.metabol.2015.12.012
- Tilg H, Moschen AR. Evolution of inflammation in nonalcoholic fatty liver disease: the multiple parallel hits hypothesis. Hepatology. 2010;52(5):1836–1846. doi:10.1002/hep.24001
- Friedman SL, Neuschwander-Tetri BA, Rinella M, Sanyal AJ. Mechanisms of NAFLD development and therapeutic strategies. Nat Med. 2018;24(7):908–922. doi:10.1038/s41591-018-0104-9
- Ghorpade DS, Ozcan L, Zheng Z, et al. Hepatocyte-secreted DPP4 in obesity promotes adipose inflammation and insulin resistance. Nature. 2018;555(7698):673–677. doi:10.1038/nature26138
- Takeuchi M. Toxic AGEs (TAGE) theory: a new concept for preventing the development of diseases related to lifestyle. Diabetol Metab Syndr. 2020;12(1):105. doi:10.1186/s13098-020-00614-3
- Adinolfi LE, Petta S, Fracanzani AL, et al. Reduced incidence of type 2 diabetes in patients with chronic hepatitis C virus infection cleared by direct-acting antiviral therapy: a prospective study. Diabetes Obes Metab. 2020;22(12):2408–2416. doi:10.1111/dom.14168
- Adinolfi LE, Petta S, Fracanzani AL, et al. Impact of hepatitis C virus clearance by direct-acting antiviral treatment on the incidence of major cardiovascular events: a prospective multicentre study. Atherosclerosis. 2020;296:40–47. doi:10.1016/j.atherosclerosis.2020.01.010
- Sasso FC, Pafundi PC, Caturano A, et al. Impact of direct acting antivirals (DAAs) on cardiovascular events in HCV cohort with pre-diabetes. Nutr Metab Cardiovasc Dis. 2021;31(8):2345–2353. doi:10.1016/j.numecd.2021.04.016
- Rinaldi L, Pafundi PC, Galiero R, et al. Mechanisms of non-alcoholic fatty liver disease in the metabolic syndrome. A narrative review. Antioxidants. 2021;10(2):270. doi:10.3390/antiox10020270
- Masarone M, Rosato V, Aglitti A, et al. Liver biopsy in type 2 diabetes mellitus: steatohepatitis represents the sole feature of liver damage. PLoS One. 2017;12(6):e0178473. doi:10.1371/journal.pone.0178473
- Jorgačević B, Mladenović D, Ninković M, et al. Rimonabant improves oxidative/nitrosative stress in mice with nonalcoholic fatty liver disease. Oxid Med Cell Longev. 2015;2015:842108. doi:10.1155/2015/842108
- Gornicka A, Morris-Stiff G, Thapaliya S, Papouchado BG, Berk M, Feldstein AE. Transcriptional profile of genes involved in oxidative stress and antioxidant defense in a dietary murine model of steatohepatitis. Antioxid Redox Signal. 2011;15(2):437–445. doi:10.1089/ars.2010.3815
- Alswat KA. The role of endocannabinoids system in fatty liver disease and therapeutic potentials. Saudi J Gastroenterol. 2013;19(4):144–151. doi:10.4103/1319-3767.114505
- Bartelt A, Orlando P, Mele C, et al. Altered endocannabinoid signalling after a high-fat diet in Apoe(-/-) mice: relevance to adipose tissue inflammation, hepatic steatosis and insulin resistance. Diabetologia. 2011;54(11):2900–2910. doi:10.1007/s00125-011-2274-6
- Park HS, Song JW, Park JH, et al. TXNIP/VDUP1 attenuates steatohepatitis via autophagy and fatty acid oxidation. Autophagy. 2021;17(9):2549–2564. doi:10.1080/15548627.2020.1834711
- Trebicka J, Bork P, Krag A, Arumugam M. Utilizing the gut microbiome in decompensated cirrhosis and acute-on-chronic liver failure. Nat Rev Gastroenterol Hepatol. 2021;18(3):167–180. doi:10.1038/s41575-020-00376-3
- Trebicka J, Macnaughtan J, Schnabl B, Shawcross DL, Bajaj JS. The microbiota in cirrhosis and its role in hepatic decompensation. J Hepatol. 2021;75(Suppl 1):S67–S81. doi:10.1016/j.jhep.2020.11.013
- Cani PD, Amar J, Iglesias MA, et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007;56(7):1761–1772. doi:10.2337/db06-1491
- Honda M, Surewaard BGJ, Watanabe M, et al. Perivascular localization of macrophages in the intestinal mucosa is regulated by Nr4a1 and the microbiome. Nat Commun. 2020;11(1):1329. doi:10.1038/s41467-020-15068-4
- De Schepper S, Verheijden S, Aguilera-Lizarraga J, et al. Self-maintaining gut macrophages are essential for intestinal homeostasis. Cell. 2018;175(2):400–415.e13. doi:10.1016/j.cell.2018.07.048
- Parséus A, Sommer N, Sommer F, et al. Microbiota-induced obesity requires farnesoid X receptor. Gut. 2017;66(3):429–437. doi:10.1136/gutjnl-2015-310283
- Pierantonelli I, Svegliati-Baroni G. Nonalcoholic fatty liver disease: basic pathogenetic mechanisms in the progression from NAFLD to NASH. Transplantation. 2019;103(1):e1–e13. doi:10.1097/TP.0000000000002480
- Dong J, Viswanathan S, Adami E, et al. Hepatocyte-specific IL11 cis-signaling drives lipotoxicity and underlies the transition from NAFLD to NASH. Nat Commun. 2021;12(1):66. doi:10.1038/s41467-020-20303-z
- Parthasarathy G, Revelo X, Malhi H. Pathogenesis of nonalcoholic steatohepatitis: an overview. Hepatol Commun. 2020;4(4):478–492. doi:10.1002/hep4.1479
- Simões ICM, Fontes A, Pinton P, Zischka H, Wieckowski MR. Mitochondria in non-alcoholic fatty liver disease. Int J Biochem Cell Biol. 2018;95:93–99. doi:10.1016/j.biocel.2017.12.019
- Mota M, Banini BA, Cazanave SC, Sanyal AJ. Molecular mechanisms of lipotoxicity and glucotoxicity in nonalcoholic fatty liver disease. Metabolism. 2016;65(8):1049–1061. doi:10.1016/j.metabol.2016.02.014
- Zarei M, Pizarro-Delgado J, Barroso E, Palomer X, Vázquez-Carrera M. Targeting FGF21 for the treatment of nonalcoholic steatohepatitis. Trends Pharmacol Sci. 2020;41(3):199–208. doi:10.1016/j.tips.2019.12.005
- Kharitonenkov A, DiMarchi R. Fibroblast growth factor 21 night watch: advances and uncertainties in the field. J Intern Med. 2017;281(3):233–246. doi:10.1111/joim.12580
- Saxena NK, Anania FA. Adipocytokines and hepatic fibrosis. Trends Endocrinol Metab. 2015;26(3):153–161. doi:10.1016/j.tem.2015.01.002
- Hui X, Feng T, Liu Q, Gao Y, Xu A. The FGF21-adiponectin axis in controlling energy and vascular homeostasis. J Mol Cell Biol. 2016;8(2):110–119. doi:10.1093/jmcb/mjw013
- Dushay J, Lai M. Is trimming the fat enough? Fibroblast growth factor 21 as an emerging treatment for nonalcoholic fatty liver disease. Hepatology. 2019;70(5):1860–1862. doi:10.1002/hep.30789
- Alvarez-Sola G, Uriarte I, Latasa MU, et al. Fibroblast growth factor 15/19 (FGF15/19) protects from diet-induced hepatic steatosis: development of an FGF19-based chimeric molecule to promote fatty liver regeneration. Gut. 2017;66(10):1818–1828. doi:10.1136/gutjnl-2016-312975
- Cicione C, Degirolamo C, Moschetta A. Emerging role of fibroblast growth factors 15/19 and 21 as metabolic integrators in the liver. Hepatology. 2012;56(6):2404–2411. doi:10.1002/hep.25929
- Bhatnagar S, Damron HA, Hillgartner FB. Fibroblast growth factor-19, a novel factor that inhibits hepatic fatty acid synthesis. J Biol Chem. 2009;284(15):10023–10033. doi:10.1074/jbc.M808818200
- Sciarrillo CM, Keirns BH, Koemel NA, Anderson KL, Emerson SR. Fibroblast growth factor 19: potential modulation of hepatic metabolism for the treatment of non-alcoholic fatty liver disease. Liver Int. 2021;41(5):894–904. doi:10.1111/liv.14802
- Bougarne N, Weyers B, Desmet SJ, et al. Molecular actions of PPARα in lipid metabolism and inflammation. Endocr Rev. 2018;39(5):760–802. doi:10.1210/er.2018-00064
- Sanderson LM, Boekschoten MV, Desvergne B, Müller M, Kersten S. Transcriptional profiling reveals divergent roles of PPARalpha and PPARbeta/delta in regulation of gene expression in mouse liver. Physiol Genomics. 2010;41(1):42–52. doi:10.1152/physiolgenomics.00127.2009
- Zardi EM, Navarini L, Sambataro G, et al. Hepatic PPARs: their role in liver physiology, fibrosis and treatment. Curr Med Chem. 2013;20(27):3370–3396. doi:10.2174/09298673113209990136
- Brown E, Hydes T, Hamid A, Cuthbertson DJ. Emerging and established therapeutic approaches for nonalcoholic fatty liver disease. Clin Ther. 2021;43(9):1476–1504. doi:10.1016/j.clinthera.2021.07.013
- Spence JD, Viscoli CM, Inzucchi SE, et al. Pioglitazone therapy in patients with stroke and prediabetes: a post hoc analysis of the IRIS randomized clinical trial. JAMA Neurol. 2019;76(5):526–535. doi:10.1001/jamaneurol.2019.0079
- DeFronzo RA, Inzucchi S, Abdul-Ghani M, Nissen SE. Pioglitazone: the forgotten, cost-effective cardioprotective drug for type 2 diabetes. Diab Vasc Dis Res. 2019;16(2):133–143. doi:10.1177/1479164118825376
- Kernan WN, Viscoli CM, Furie KL, et al. Pioglitazone after ischemic stroke or transient ischemic attack. N Engl J Med. 2016;374(14):1321–1331. doi:10.1056/NEJMoa1506930
- Francque S, Szabo G, Abdelmalek MF, et al. Nonalcoholic steatohepatitis: the role of peroxisome proliferator-activated receptors. Nat Rev Gastroenterol Hepatol. 2021;18(1):24–39. doi:10.1038/s41575-020-00366-5
- Gupta NA, Mells J, Dunham RM, et al. Glucagon-like peptide-1 receptor is present on human hepatocytes and has a direct role in decreasing hepatic steatosis in vitro by modulating elements of the insulin signaling pathway. Hepatology. 2010;51(5):1584–1592. doi:10.1002/hep.23569
- Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696–1705. doi:10.1016/S0140-6736(06)69705-5
- Drucker DJ. The cardiovascular biology of glucagon-like peptide-1. Cell Metab. 2016;24(1):15–30. doi:10.1016/j.cmet.2016.06.009
- Seino Y, Yabe D. Glucose-dependent insulinotropic polypeptide and glucagon-like peptide-1: incretin actions beyond the pancreas. J Diabetes Investig. 2013;4(2):108–130. doi:10.1111/jdi.12065
- Armstrong MJ, Gaunt P, Aithal GP, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled phase 2 study. Lancet. 2016;387(10019):679–690. doi:10.1016/S0140-6736(15)00803-X
- Fadini GP, Frison V, Rigato M, et al. Trend 2010–2018 in the clinical use of GLP-1 receptor agonists for the treatment of type 2 diabetes in routine clinical practice: an observational study from Northeast Italy. Acta Diabetol. 2020;57(3):367–375. doi:10.1007/s00592-019-01445-z
- Svegliati-Baroni G, Saccomanno S, Rychlicki C, et al. Glucagon-like peptide-1 receptor activation stimulates hepatic lipid oxidation and restores hepatic signalling alteration induced by a high-fat diet in nonalcoholic steatohepatitis. Liver Int. 2011;31(9):1285–1297. doi:10.1111/j.1478-3231.2011.02462.x
- Eguchi Y, Kitajima Y, Hyogo H, et al. Pilot study of liraglutide effects in non-alcoholic steatohepatitis and non-alcoholic fatty liver disease with glucose intolerance in Japanese patients (LEAN-J). Hepatol Res. 2015;45(3):269–278. doi:10.1111/hepr.12351
- Sathyanarayana P, Jogi M, Muthupillai R, Krishnamurthy R, Samson SL, Bajaj M. Effects of combined exenatide and pioglitazone therapy on hepatic fat content in type 2 diabetes. Obesity. 2011;19(12):2310–2315. doi:10.1038/oby.2011.152
- Teshome G, Ambachew S, Fasil A, Abebe M. Efficacy of glucagon-like peptide-1 analogs in nonalcoholic fatty liver disease: a systematic review. Hepat Med. 2020;12:139–151. doi:10.2147/HMER.S265631
- Tripathi A, Debelius J, Brenner DA, et al. The gut-liver axis and the intersection with the microbiome. Nat Rev Gastroenterol Hepatol. 2018;15(7):397–411. doi:10.1038/s41575-018-0011-z
- Vinolo MAR, Rodrigues HG, Nachbar RT, Curi R. Regulation of inflammation by short chain fatty acids. Nutrients. 2011;3(10):858–876. doi:10.3390/nu3100858
- Takai A, Kikuchi K, Ichimura M, et al. Fructo-oligosaccharides ameliorate steatohepatitis, visceral adiposity, and associated chronic inflammation via increased production of short-chain fatty acids in a mouse model of non-alcoholic steatohepatitis. BMC Gastroenterol. 2020;20(1):46. doi:10.1186/s12876-020-01194-2
- Chiang JYL. Bile acid metabolism and signaling. Compr Physiol. 2013;3(3):1191–1212. doi:10.1002/cphy.c120023
- Jia W, Xie G, Jia W. Bile acid-microbiota crosstalk in gastrointestinal inflammation and carcinogenesis. Nat Rev Gastroenterol Hepatol. 2018;15(2):111–128. doi:10.1038/nrgastro.2017.119
- Hirasawa A, Tsumaya K, Awaji T, et al. Free fatty acids regulate gut incretin glucagon-like peptide-1 secretion through GPR120. Nat Med. 2005;11(1):90–94. doi:10.1038/nm1168
- Larraufie P, Martin-Gallausiaux C, Lapaque N, et al. SCFAs strongly stimulate PYY production in human enteroendocrine cells. Sci Rep. 2018;8(1):74. doi:10.1038/s41598-017-18259-0
- Sala-Rabanal M, Hirayama BA, Ghezzi C, et al. Revisiting the physiological roles of SGLTs and GLUTs using positron emission tomography in mice. J Physiol. 2016;594(15):4425–4438. doi:10.1113/JP271904
- Nasiri-Ansari N, Nikolopoulou C, Papoutsi K, et al. Empagliflozin attenuates Non-Alcoholic Fatty Liver Disease (NAFLD) in High Fat Diet Fed ApoE(-/-) mice by activating autophagy and reducing ER stress and apoptosis. Int J Mol Sci. 2021;22(2):818. doi:10.3390/ijms22020818
- Inoue M, Hayashi A, Taguchi T, et al. Effects of canagliflozin on body composition and hepatic fat content in type 2 diabetes patients with non-alcoholic fatty liver disease. J Diabetes Investig. 2019;10(4):1004–1011. doi:10.1111/jdi.12980
- Katsuno K, Fujimori Y, Takemura Y, et al. Sergliflozin, a novel selective inhibitor of low-affinity sodium glucose cotransporter (SGLT2), validates the critical role of SGLT2 in renal glucose reabsorption and modulates plasma glucose level. J Pharmacol Exp Ther. 2007;320(1):323–330. doi:10.1124/jpet.106.110296
- Zinman B, Inzucchi SE, Lachin JM, et al. Empagliflozin and cerebrovascular events in patients with type 2 diabetes mellitus at high cardiovascular risk. Stroke. 2017;48(5):1218–1225. doi:10.1161/STROKEAHA.116.015756
- Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
- Ismail-Beigi F, Moghissi E, Kosiborod M, Inzucchi SE. Shifting paradigms in the medical management of type 2 diabetes: reflections on recent cardiovascular outcome trials. J Gen Intern Med. 2017;32(9):1044–1051. doi:10.1007/s11606-017-4061-7
- Yokono M, Takasu T, Hayashizaki Y, et al. SGLT2 selective inhibitor ipragliflozin reduces body fat mass by increasing fatty acid oxidation in high-fat diet-induced obese rats. Eur J Pharmacol. 2014;727:66–74. doi:10.1016/j.ejphar.2014.01.040
- Pradhan R, Yin H, Yu O, Azoulay L. Glucagon-like peptide 1 receptor agonists and sodium-glucose cotransporter 2 inhibitors and risk of nonalcoholic fatty liver disease among patients with type 2 diabetes. Diabetes Care. 2022;45(4):819–829. doi:10.2337/dc21-1953
- Ding C, Tang Y, Zhu W, et al. Sodium-glucose cotransporter protein-2 inhibitors and glucagon-like peptide-1 receptor agonists versus thiazolidinediones for non-alcoholic fatty liver disease: a network meta-analysis. Acta Diabetol. 2022;59(4):519–533. doi:10.1007/s00592-021-01830-7
- Raj H, Durgia H, Palui R, et al. SGLT-2 inhibitors in non-alcoholic fatty liver disease patients with type 2 diabetes mellitus: a systematic review. World J Diabetes. 2019;10(2):114–132. doi:10.4239/wjd.v10.i2.114
- Yan H, Huang C, Shen X, Li J, Zhou S, Li W. GLP-1 RAs and SGLT-2 inhibitors for insulin resistance in nonalcoholic fatty liver disease: systematic review and network meta-analysis. Front Endocrinol. 2022;13:923606. doi:10.3389/fendo.2022.923606
- Chiang JYL. Bile acid metabolism and signaling in liver disease and therapy. Liver Res. 2017;1(1):3–9. doi:10.1016/j.livres.2017.05.001
- Li T, Chiang JYL, Ma Q. Bile acid signaling in metabolic disease and drug therapy. Pharmacol Rev. 2014;66(4):948–983. doi:10.1124/pr.113.008201
- Inagaki T, Moschetta A, Lee YK, et al. Regulation of antibacterial defense in the small intestine by the nuclear bile acid receptor. Proc Natl Acad Sci U S A. 2006;103(10):3920–3925. doi:10.1073/pnas.0509592103
- Mudaliar S, Henry RR, Sanyal AJ, et al. Efficacy and safety of the farnesoid X receptor agonist obeticholic acid in patients with type 2 diabetes and nonalcoholic fatty liver disease. Gastroenterology. 2013;145(3):574–582.e1. doi:10.1053/j.gastro.2013.05.042
- Neuschwander-Tetri BA, Loomba R, Sanyal AJ, et al. Farnesoid X nuclear receptor ligand obeticholic acid for non-cirrhotic, non-alcoholic steatohepatitis (FLINT): a multicentre, randomised, placebo-controlled trial. Lancet. 2015;385(9972):956–965. doi:10.1016/S0140-6736(14)61933-4
- Lambert JE, Ramos-Roman MA, Browning JD, Parks EJ. Increased de novo lipogenesis is a distinct characteristic of individuals with nonalcoholic fatty liver disease. Gastroenterology. 2014;146(3):726–735. doi:10.1053/j.gastro.2013.11.049
- Mitsuyoshi H, Yasui K, Harano Y, et al. Analysis of hepatic genes involved in the metabolism of fatty acids and iron in nonalcoholic fatty liver disease. Hepatol Res. 2009;39(4):366–373. doi:10.1111/j.1872-034X.2008.00464.x
- Loomba R, Mohseni R, Lucas KJ, et al. TVB-2640 (FASN inhibitor) for the treatment of nonalcoholic steatohepatitis: FASCINATE-1, a randomized, placebo-controlled Phase 2a trial. Gastroenterology. 2021;161(5):1475–1486. doi:10.1053/j.gastro.2021.07.025
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. 2012;55(6):2005–2023. doi:10.1002/hep.25762
- Oseini AM, Sanyal AJ. Therapies in non-alcoholic steatohepatitis (NASH). Liver Int. 2017;37(Suppl 1):97–103. doi:10.1111/liv.13302
- Sarkhy AA, Al-Hussaini AA, Nobili V. Does vitamin E improve the outcomes of pediatric nonalcoholic fatty liver disease? A systematic review and meta-analysis. Saudi J Gastroenterol. 2014;20(3):143–153. doi:10.4103/1319-3767.132983
- Moser MA, Chun OK. Vitamin C and heart health: a review based on findings from epidemiologic studies. Int J Mol Sci. 2016;17(8):1328. doi:10.3390/ijms17081328
- Kim JY, van de Wall E, Laplante M, et al. Obesity-associated improvements in metabolic profile through expansion of adipose tissue. J Clin Invest. 2007;117(9):2621–2637. doi:10.1172/JCI31021
- Rose FJ, Webster J, Barry JB, Phillips LK, Richards AA, Whitehead JP. Synergistic effects of ascorbic acid and thiazolidinedione on secretion of high molecular weight adiponectin from human adipocytes. Diabetes Obes Metab. 2010;12(12):1084–1089. doi:10.1111/j.1463-1326.2010.01297.x