
Abstract
Renal cysts and diabetes syndrome (RCAD) is a rare disease caused by abnormalities in the HNF1B gene, which often leads to dysfunction in the renal, genital tracts, and pancreas. In this report, we present a rare case of a 27-year-old female with muscle mass loss who experienced a delayed diagnosis of RCAD. The patient had been misdiagnosed as “type 1 diabetes” for a long period. Her main clinical manifestations included muscle loss, renal magnesium loss, and an incomplete longitudinal uterus. Ultimately, the diagnosis of RCAD syndrome was confirmed through genetic testing. Reduction of muscle mass, although rarely reported, can progress to sarcopenia. Therefore, early intervention should be strongly emphasized. Furthermore, in future research, it is crucial to explore the mechanisms and relationships underlying these patients and their unusual manifestations.
Introduction
Renal cysts and diabetes (RCAD) syndrome is a rare disease with hepatocyte nuclear factor-1-beta (HNF1B) gene mutations.Citation1 According to reports, the syndrome often involves the urinary tract, diabetes mellitus (maturity-onset diabetes of the young type 5, MODY 5), reproductive system malformations, hypomagnesemia and neuropsychiatric disorders.Citation1,Citation2 Here, we firstly report a case of a delayed diagnosis of renal cysts and diabetes syndrome with loss of muscle mass loss.
Case Presentation
A 27-year-old woman was diagnosed with “type 1 diabetes” with negative of GADA, IA-2A, ZnT8A and IAA for 3 years. The patient was first referred for diabetic ketosis and had a low C-peptide level (0.96 ng/mL, chemiluminescence Roche Cobas e601 Analyzer) and glycated haemoglobin (6.4 mmol/L, Premier Hb9210, Primus) at the time of admission. Initial insulin therapy was effective. However, her blood glucose levels fluctuated widely, and a postprandial hypoglycaemic coma developed. Low blood magnesium levels were persistent during the course of diabetes, but the physician did not pay great attention to it. Her menstrual cycle was irregular, as her last menstrual period occurred six months prior. There was no history of conception. Her mother and grandmother were diagnosed with “type 2 diabetes”.
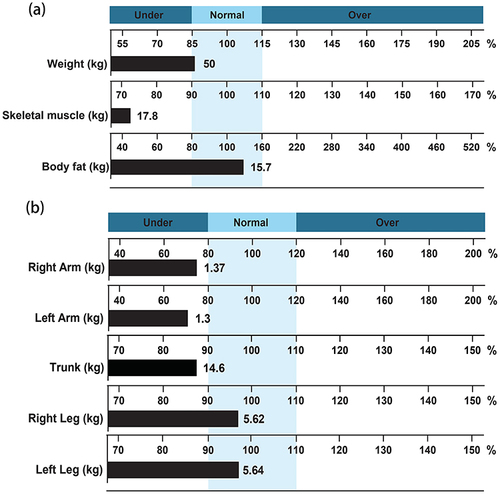
On admission, she was lean with a body mass index of 18.6 kg/m2, while the albumin, prealbumin, serum lipid showed a normal range. Laboratory tests revealed a blood magnesium concentration of 0.54 (normal range 0.75–1.02, Beckmann AU5800) mmol/L and a 24-hour urinary magnesium concentration of 3.19 (normal range 0.98–10.49, Beckmann AU5800) mmol, suggesting renal magnesium loss. The luteinizing hormone concentration was 9.70 (corpus luteum phase, normal range 1.2–12.86) mIU/mL, follicle-stimulating hormone concentration was 2.28 (corpus luteum phase, normal range 1.79–5.12) mIU/mL, the oestrogen concentration was 241.70 (corpus luteum phase, normal range 30.3–274.2) pg/mL, and testosterone concentration was 0.74 (normal range 0.1–0.75). The sex hormones above were detected by Beckman DXI800. A renal ultrasound was completed and revealed a left renal cyst. As the patient had abnormal levels of sex hormones, a gynaecological ultrasound was performed and revealed an incomplete longitudinal uterus and polycystic ovary. Moreover, due to the patient’s low BMI, further body composition analysis was refined by bioimpedance analysis (InBody 770, Korea, InBody Co, Lid). The results showed a height of 1.64 m, body weight of 50.0 kg, and skeletal muscle mass of 17.8 kg (normal range 22.0–27.0), suggesting muscle loss (). Fat mass was 15.7 kg (normal range 11.6–18.5), and the body fat rate was 31.4% (normal range 18–28%). The left arm muscle mass was only 1.30 kg (normal range 1.46–2.19), the right arm muscle mass was 1.37 kg (normal range 1.46–2.19), which was notably reduced, the right leg muscle mass was 5.62 kg (normal range 5.20–6.36), the left leg muscle mass was 5.64 kg (normal range 5.20–6.36), the trunk muscle mass was 14.6 kg (normal range 14.97–18.29) (), and the fat-free mass index was 6.6 kg/m2 (normal range 13.3–17.8).Citation3
Figure 1 Body composition analysis of the patient. (a) A graph of muscle-fat analysis of the skeletal muscle mass detected by InBody 770 (Korea, InBody Co, Lid). (b) A graph of segmental lean analysis of the arm and trunk muscle mass detected by InBody 770 (Korea, InBody Co, Lid).
Considering that the patient exhibited renal magnesium loss with a left renal cyst and an incomplete longitudinal uterus, RCAD syndrome was suspected. According to the Consensus Report,Citation4 the next-generation sequencing was performed to confirm RCAD syndrome. There was a heterozygous fragment deletion of 1.3 Mb in size on 17q12 at the interval from chr17: 34806179 to 36104883, of which hepatocyte nuclear factor-1-beta (HNF1B) and 21 other genes were missing, including MYO19, and ACACA. Subsequently, we found that the patient’s mother also had a fragment deletion on 17q12, which suggested that it was inherited from her mother.
Discussion
RCAD syndrome is a rare recurrent chromosomal aberration that can be caused by deletion of the long arm region of chromosome 17. The diagnosis of this syndrome relies on genetic testing. In this patient, the expression of 22 genes, including the HNF1B gene, was affected.
Notably, decreased muscle mass was the prominent clinical manifestation in this patient. Previous understanding suggested that age-related factors contribute to muscle mass loss, but recent studies have highlighted the involvement of multiple mechanisms, including mitochondrial dysfunction, satellite cell dysfunction, neuromuscular dysfunction, reduced anabolic hormone production or sensitivity, undernutrition, and increased inactivity.Citation5,Citation6 Additionally, various systemic diseases, such as cancer, cardiovascular disease, and metabolic diseases, can also lead to muscle mass and strength reduction.Citation7,Citation8 The reduction of muscle protein homeostasis occurs when muscle protein breakdown exceeds muscle protein synthesis, and decreased dietary protein intake can further facilitate muscle mass loss. However, in the case of the 27-year-old female patient with a regular diet described here, laboratory tests showed normal levels of albumin, prealbumin, and serum lipids, indicating fair nutritional status. Thus, it is evident that other factors are involved in the breakdown of muscle protein homeostasis. First, glucose metabolism disorder in this patient contributed to chronic inflammation and mitochondrial metabolism oxidative stress, leading to muscle injuries.Citation9 In addition, a heterozygous deletion of the MYO19 gene fragment was identified. MYO19 is a myosin related to mitochondria that provides power for muscle contraction,Citation10 and mitochondrial metabolism plays a crucial role in skeletal muscle mass and function.Citation11 Moreover, another heterozygous gene, ACACA, was located in the deleted fragment. Pathogenic variants in ACACA cause acetyl-CoA carboxylase deficiency, characterized by hypotonia and motor and intellectual developmental delays.Citation12 Acetyl-CoA carboxylase 2, primarily expressed in the heart and skeletal muscles, is coupled to the mitochondrial outer membrane, and muscle weakness has been reported in patients with acetyl-CoA carboxylase deficiency.Citation13 Furthermore, an in vivo study demonstrated that Mg2+-deficient rats exhibited various ultrastructural changes in skeletal muscle tissue, including swelling mitochondria and disorganization of the sarcoplasmic reticulum network.Citation14 In summary, multiple mechanisms may be involved in the reduction of muscle mass. The ratio of luteinizing hormone and follicle-stimulating hormone was observed to be increased in this patient with polycystic ovary changes, leading us to believe that polycystic ovarian syndrome and reproductive system abnormalities may cause her irregular menstrual cycles.
The progression of muscle mass loss can result in sarcopenia, which increases the risk of falls, fractures, frailty, cognitive impairment, and mortality. This, in turn, leads to a reduced quality of life for patients and a significant increase in economic burden and health care costs.Citation15,Citation16 Therefore, it is crucial to recognize and intervene early in patients with 17q12 deletion syndrome to prevent muscle mass loss.
Conclusion
RCAD syndrome is a rare type of diabetes that requires attention because it can be easily misdiagnosed as type 1 or type 2 diabetes. Hypomagnesemia may serve as a clue for diagnosis. Additionally, due to the involvement of multiple genes in the deletion, multiple systems can be affected. Here, we highlight a young woman with 17q12 deletion syndrome who experienced muscle mass loss. Early intervention should be emphasized for such patients. The underlying mechanisms of the relationship between the conditions of these patients and their unusual manifestations should be further explored in the future.
Ethical Approval and Consent
The institution has given approval for this article to be published in this journal. A written consent was obtained from the patient included in the study for publication.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Cheng Y, Zhong DP, Ren L, Yang H, Tian CF. Unusual manifestations of young woman with MODY5 based on 17q12 recurrent deletion syndrome. Bmc Endocr Disord. 2022;22(1). doi:10.1186/s12902-022-00989-6
- Roehlen N, Hilger H, Stock F, et al. 17q12 deletion syndrome as a rare cause for diabetes mellitus type MODY5. J Clin Endocr Metab. 2018;103(10):3601–3610. doi:10.1210/jc.2018-00955
- Kim CH, Chung S, Kim H, et al. Norm references of fat-free mass index and fat mass index and subtypes of obesity based on the combined FFMI-%BF indices in the Korean adults aged 18–89 yr. Obes Res Clin Pract. 2011;5(3):e169–e266. doi:10.1016/j.orcp.2011.01.004
- Chung WK, Erion K, Florez JC, et al. Precision medicine in diabetes: a consensus report from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2020;43(7):1617–1635. doi:10.2337/dci20-0022
- Sasaki K, Fukumoto Y. Sarcopenia as a comorbidity of cardiovascular disease. J Cardiol. 2022;79(5):596–604. doi:10.1016/j.jjcc.2021.10.013
- Tipton KD. Muscle protein metabolism in the elderly: influence of exercise and nutrition. Can J Appl Physiol. 2001;26(6):588–606. doi:10.1139/h01-033
- Kim Y, Han BD, Han K, et al. Optimal cutoffs for low skeletal muscle mass related to cardiovascular risk in adults: the Korea National Health and Nutrition Examination Survey 2009–2010. Endocrine. 2015;50(2):424–433. doi:10.1007/s12020-015-0577-y
- Cruz-Jentoft AJ, Sayer AA. Sarcopenia (vol 393, pg 2636, 2019). Lancet. 2019;393(10191):2590.
- Pottecher J, Adamopoulos C, Lejay A, et al. Diabetes worsens skeletal muscle mitochondrial function, oxidative stress, and apoptosis after lower-limb ischemia-reperfusion: implication of the RISK and SAFE pathways? Front Physiol. 2018;9. doi:10.3389/fphys.2018.00579
- Quintero OA, DiVito MM, Adikes RC, et al. Human Myo19 is a novel myosin that associates with mitochondria. Curr Biol. 2009;19(23):2008–2013. doi:10.1016/j.cub.2009.10.026
- Migliavacca E, Tay SKH, Patel HP, et al. Mitochondrial oxidative capacity and NAD biosynthesis are reduced in human sarcopenia across ethnicities. Nat Commun. 2019;10(1):10. doi:10.1038/s41467-018-07709-6
- Lou XT, Zhou XY, Li HY, et al. Biallelic mutations in cause a disruption in lipid homeostasis that is associated with global developmental delay, microcephaly, and dysmorphic facial features. Front Cell Dev Biol. 2021;9. doi:10.3389/fcell.2021.618492
- Shafieipour N, Khamirani HJ, Kamal N, Tabei SMB, Dianatpour M, Dastgheib SA. The third patient of ACACA-related acetyl-CoA carboxylase deficiency with seizure and literature review. Eur J Med Genet. 2023;66(4):104707. doi:10.1016/j.ejmg.2023.104707
- Rock E, Astier C, Lab C, et al. Dietary magnesium-deficiency in rats enhances free-radical production in skeletal-muscle. J Nutr. 1995;125(5):1205–1210. doi:10.1093/jn/125.5.1205
- Muvhulawa N, Mazibuko-Mbeje SE, Ndwandwe D, et al. Sarcopenia in a type 2 diabetic state: reviewing literature on the pathological consequences of oxidative stress and inflammation beyond the neutralizing effect of intracellular antioxidants. Life Sci. 2023;332:122125. doi:10.1016/j.lfs.2023.122125
- Mager DR, Hager A, Gilmour S. Challenges and physiological implications of sarcopenia in children and youth in health and disease. Curr Opin Clin Nutr Metab Care. 2023;26(6):528–533. doi:10.1097/MCO.0000000000000969