
Abstract
Background
Some research have indicated that Bariatric and metabolic surgery (BMS) can reduce the risk of cardiovascular disease (CVD) among individuals with obesity. However, there are few reports available that focuses on assessing effect of BMS on the risk of CVD in Chinese population using multiple models.
Objective
This research aims to assess the function of BMS on the risk of CVD in Chinese patients with obesity using multiple CVD risk models.
Methods
We performed a retrospective analysis of the basic data and glycolipid metabolism data preoperatively and postoperatively from patients with obesity at our hospital. Subgroup analysis was carried out according to different surgical procedures. Then, the function of BMS on the risk of CVD in the Chinese population was assessed using four models, including: China-PAR risk model, Framingham risk score (FRS), World Health Organization (WHO) risk model, and Globorisk model.
Results
We enrolled 64 patients, 24 (37.5%) of whom underwent laparoscopic sleeve gastrectomy (LSG) while 40 (62.5%) underwent Roux-en-Y gastric bypass (RYGB). The 10-year CVD risk for patients calculated using the China-PAR risk model decreased from 6.3% preoperatively to 2.0% at 1 year postoperatively and was statistically significantly different. Similarly, the 10-year CVD risk of patients calculated using the FRS, WHO, Global risk model decreased significantly at 1 year postoperatively compared to preoperatively. When the FRS risk model was used to calculate the patients’ 30-year postoperative CVD risk, there was a significant decrease at 1 year after surgery compared to the preoperative period. When employing various models to evaluate the 10-year CVD risk for LSG and RYGB, no statistically significant difference was found in the 1-year postoperative RRR between the procedures.
Conclusion
The CVD risk after BMS was significantly reduced compared to preoperatively. In terms of improving cardiovascular risk, SG and RYGB appear to be equally effective.
Introduction
In recent years, the rate of obesity has dramatically risen worldwide.Citation1,Citation2 Compared to males, who had an increase from 31 million to 281 million, women saw a rise from 69 million to 390 million people with obesity globally in 2016.Citation1 Obesity rates among children were also increasing dramatically.Citation3 Obesity and type 2 diabetes mellitus (T2DM) raise the risk of comorbid conditions such cardiovascular disease and dyslipidemia, which can cause both microvascular and macrovascular diseases.Citation4 In 2005, over 400 million cases of cardiovascular disease (CVD) and 17 million CVD-related deaths occurred worldwide.Citation5,Citation6 While T2DM was the second leading cause of BMI-related deaths in 2015, resulting in 600,000 deaths.Citation7
Obesity predisposes to atherosclerotic cardiovascular disease (ACVD), the direct mechanisms of which include hemodynamic changes, increased sympathetic tone, tissue inflammation, and endothelial changes, leading to myocardial remodeling and consequent myocardial damage.Citation8,Citation9 The distribution of obesity is commonly classified into visceral or subcutaneous categories. Visceral obesity poses greater harm due to its adverse effects on cardiometabolism. Visceral fat plays a pivotal role in producing pro-inflammatory cytokines such as tumor necrosis factor (TNF)-α, interleukin (IL)-1, and IL-6, all known inducers of atherosclerosisCitation9,Citation10 These inflammatory cytokines may induce oxidative stress in the endothelium of coronary arteries, facilitating the formation of damage to blood vessel walls, ultimately resulting in endothelial dysfunction and promoting the progression of atherosclerosis.Citation11 Inflammatory cytokines are also known to have direct toxic effects on cardiomyocytes, especially pro-inflammatory cytokines, which are elevated in obesity and have direct cardiac depressant properties, leading to cardiac systolic and diastolic dysfunction.Citation12
Currently, the approaches to loss weight include dietary modification, regular exercise, and bariatric and metabolic surgery (BMS). BMS has been demonstrated to be more successful and valuable when it comes to weight loss than traditional methods.Citation13,Citation14 Moreover, it can improve metabolic syndrome, reduce obesity comorbidities,Citation15,Citation16 decrease the CVD risk, etc.,Citation17,Citation18 and improve patients’ overall quality of life.Citation19 It is remarkable that BMS is associated with a lower risk of all-cause mortality, incident heart failure, myocardial infarction, and stroke.Citation20–22 Shobini Jayaraman et al have shown that the modifications in low-density lipoprotein (LDL) play a pivotal role in the accelerated development of cardiovascular diseases (CVD) in obesity. Subsequent to bariatric surgery, weight loss exhibits the potential to partially rectify these LDL alterations by alleviating systemic inflammation associated with obesity.Citation23 Arunkumar Krishnan et al have also shown that the BMS is associated with significantly reduced incidence of cardiovascular diseases and mortality in patients with obesity.Citation21 In order to better predict and assess the risk of obesity combined with cardiovascular-related diseases, up to now, many models have been developed to evaluate the risk of CVD, including the China-PAR risk model, WHO risk model, Global Risk Model, and FRS. These models have been widely used in clinical work, for example, Sazzli Shahlan Kasim et al assessed the risk of CVD in the general population and its risk stratification using different risk models such as FRS and WHO risk models.Citation24–26 However, to our knowledge, no relevant studies have explored the effect of BMS on the risk of CVD in Chinese patients with obesity using multiple models.
The objective of the study is to evaluate the effect of BMS on the CVD risk in the Chinese patients with obesity using China-PAR risk, Global Risk, WHO risk, and FRS model. This study also provides new insight into evaluating the risk reduction of CVD by BMS in early-stage.
Materials and Methods
Patients and Data Collection
We retrospectively gathered information, including Weight, Body Mass Index (BMI), Waist Circumference (WC), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Fasting Plasma Glucose (FPG), Postprandial Blood Glucose (PBG), Glycosylated Hemoglobin A1C (HbA1C), Total Cholesterol (TC), Triglyceride (TG), High Density Lipoprotein (HDL), Low Density Lipoprotein (LDL), on patients with obesity treated with BMS at our hospital between March 2010 and October 2019 using hospital case system (HaiTai Medical Information Systems) and telephone follow-ups (3 months, 6 months, 1 year after surgery). The inclusion criteria were: 1) Individuals with obesity (BMI ≥ 32.5 kg/m2) or individuals with a body mass index (BMI) ≥ 27.5 kg/m2 who have difficulty controlling their weight through dietary modifications or medications and have at least two metabolic syndrome-related factors or comorbidities; 2) the age at the time of surgery ranging from 16 to 65; 3) eligibility for the China-PAR risk model, FRS, WHO risk model, Global Risk Model; 4) the surgery’s informed consent. The exclusion criteria were: 1) a history of CVD including stroke or acute coronary syndrome; 2) loss to follow-up. The Institutional Review Board (IRB) of Beijing Shijitan Hospital approved this study [Approval No. sjtkyll-lx-2023(041)]. The 1964 Helsinki Declaration and its subsequent revisions, or comparable ethical norms, are followed in all research processes involving human participants.
Relative risk reduction (RRR), as well as the LSG and RYGB methods and CVD risk models are detailed in Supplementary File 1. In addition, the CVD risk model is further detailed in Table S1 in Supplementary File 1 to facilitate understanding.
Definition of Diabetes in Remission
According to a recent expert consensus organized by the American Diabetes Association,Citation27 remission is defined as a glycated hemoglobin (HbA1c) level < 6.5%, occurring spontaneously or after intervention and lasting for at least 3 months without conventional glucose-lowering medication.
Statistical Analysis
SPSS version 26.0 was used to conduct the statistical analysis. Data for continuous variables are reported as mean ± standard deviation for normal distributions and as median (quartiles) for non-normal distributions. The data are represented as a number (%) for categorical variables. Chi-square tests were run on categorical variables. For unpaired measures, the Mann–Whitney U-test was used for non-normally distributed data, while Student’s t-test (independent-samples t-test) was used for normally distributed data. ANOVA was used to compare different metrics against one another. A p-value < 0.05 or below was regarded as statistically significant.
Results
Statistical Analysis of Metabolic Indicators
We enrolled 64 patients, including 32(50%) men and 32(50%) women, with a mean age of 45(38.25,50.75) years. 24(37.5%) patients underwent LSG, and 40(62.5%) patients underwent RYGB surgery. The overall prevalence of diabetes was 84.38%, and the overall BMI was 32.30(29.13,37.65) kg/m2, with a BMI of 37.33(32.90,39.56) kg/m2 in the LSG group and 30.98(27.95,33.42) kg/m2 in the RYGB group. The other preoperative indicators included in the analysis were shown in .
Table 1 Patient Demographics Grouped According to LSG and RYGB
BMI and WC were strikingly lower (P < 0.05) at 3 months and 1 year after surgery compared to those before surgery. The BMI of patients decreased from 32.97(30.28,37.64) kg/m2 before surgery to 25.35(21.45,26.34) kg/m2 (P < 0.05) at 1 year after surgery (P < 0.05). The WC of patients decreased from 108(99.50,116.5) cm before surgery to 88(83,96) cm (P < 0.05) at 1 year after surgery (P < 0.05). Further, the BMI and WC were strikingly lower at 12 months after surgery compared to those 3 months after surgery (). Fasting plasma glucose (FPG), HbA1c, and Postprandial Blood Glucose (BPG) were significantly lower (P < 0.05) at 3 months and 1 year after BMS compared to those before surgery. The FPG decreased from 7.53(6.13,11.62) mmol/L before surgery to 5.13(4.66,6.18) mmol/L (P < 0.05) at 1 year after surgery. The HbA1c decreased from 6.90(5.95,9.1)% before surgery to 5.7(5.3,6.6)% (P < 0.05) at 1 year after surgery. The BPG decreased from 14.90(9.61,21.33) mmol/L before surgery to 5.81(4.12,10.15) mmol/L (P < 0.05) at 1 year after surgery, and those did not differ significantly 12 months postoperatively compared to 3 months after surgery. HDL cholesterol levels were strikingly higher at 1 year after surgery compared to preoperatively, increasing from 1.00(0.88,1.11) mmol/L preoperatively to 1.22(1.06,1.37) mmol/L at 1 year after surgery (P < 0.05). Compared to 3 months postoperatively, HDL cholesterol levels did not differ preoperatively but had decreased significantly at 12 months after surgery. Low-density lipoprotein (LDL) cholesterol levels were significantly lower 1 year postoperatively compared to those before surgery, decreasing from 2.84(2.19,3.31) mmol/L preoperatively to 2.39(1.89,3.00) mmol/L at 1 year after surgery. Compared to 3 months postoperatively, LDL cholesterol levels did not differ preoperatively but had decreased significantly 12 months postoperatively.
Figure 1 Trends in weight loss and metabolic indicators from baseline to 3 months and 12 months postoperative for the overall and in both LSG and RYGB data sets. (A-I) represents trends in weight loss and metabolic markers in the total, LSG, and RYGB datasets from baseline to 3 and 12 months post-operative.
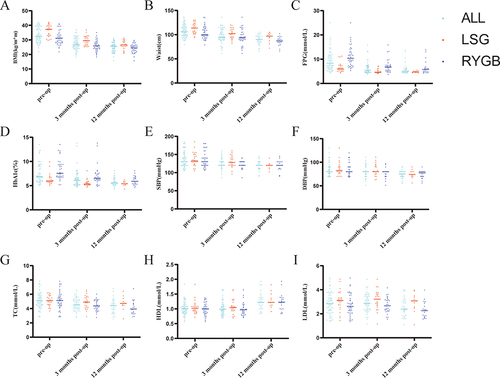
The metabolism-related data at baseline for both the LSG and RYGB subgroups are similarly depicted in , both before, at 3 and 12 months following the surgery. As shown in , in the LSG subgroup, BMI was significantly lower (P < 0.05) at 3 and 12 months after surgery compared to preoperatively, decreasing from 37.33(32.90,39.56) kg/m2 before surgery to 26.58(25.54,29.07) kg/m2 1 year after surgery. WC was significantly lower (P < 0.05) at 3 and 12 months after surgery compared to those before surgery, decreasing from 113.5(103.5,122) cm preoperatively to 97(88.63,101.5) cm 1 year after surgery. FPG was strikingly lower (P < 0.05) at 3 and 12 months after surgery compared to preoperatively, decreasing from 9.57 (7.23,14.32) mmol/L preoperatively to 4.70 (4.53,5.13) mmol/L 1 year after surgery. HDL cholesterol levels increased from 1.02(0.91,1.10) mmol/L preoperatively to 1.22(1.11,1.50) mmol/L 1 year after surgery, a significant increase (P < 0.05) compared to preoperative values. There was a significant reduction (P < 0.05) in LDL cholesterol levels at 12 months after surgery in comparison to preoperative levels. The levels decreased from 3.11(2.58,3.64) mmol/L before the surgery to 3.07(2.45,3.49) mmol/L 1 year after the surgery.
As shown in , in the RYGB group, BMI was strikingly lower (P < 0.05) at 3 and 12 months after surgery compared to preoperatively, decreasing from 31.32(28.48,34.56) kg/m2 preoperatively to 24.77(21.67,26.06) kg/m2 1 year postoperatively. WC was strikingly lower (P < 0.05) 3 and 12 months postoperatively compared to preoperatively, decreasing from 105.25(97.75,114.5) cm preoperatively to 87(83.25,92.5) cm at 1 year after surgery. FPG was notably lower (P < 0.05) at 3 and 12 months after surgery compared to preoperatively, decreasing from 10.39(7.29,14.21) mmol/L preoperatively to 5.65(4.68,6.38) mmol/L 1 year after surgery. HDL cholesterol levels were prominently higher (P < 0.05) at 12 months after the surgery compared to preoperatively, increasing from 0.99(0.84,1.12) mmol/L preoperatively to 1.23(1.00,1.38) mmol/L 1 year postoperatively. There was a noteworthy reduction (P < 0.05) in LDL cholesterol levels 12 months after the operation in comparison to preoperative levels, with levels dropping from 2.51(2.06,3.18) mmol/L prior to surgery to 2.27(1.76,2.82) mmol/L one year after the surgery.
Statistical Analysis of the 10-Year CVD Risk
Different models were employed to determine the CVD risk among Chinese individuals with obesity, and the findings are exhibited in . As shown in , when the CVD risk was worked out using the China-PAR model for entire data, the CVD risk of 10-year for patients with obesity had decreased from 6.3(2.85,11.28)% before the surgery to 2.0(0.95,4.85)% at 1 year after the surgery. The 10-year CVD risk for patients worked out using FRS based on laboratory data and non-laboratory data had decreased 1 year after surgery. Similarly when compared to before surgery, the risk of CVD was lower 1 year later according to the WHO risk model and the Global Risk Model.
Table 2 10-Year Change in CVD Risk Calculated by Different Cardiovascular Risk Models in LSG and RYGB
CVD risk alterations prior to, 3 month and 1-year following LSG and RYGB are similarly demonstrated in and . As shown in , 10-year CVD risk calculated by China-PAR risk model decreased after surgery in the LSG and RYGB group. According to FRS, the preoperative CVD risk value for the two subgroup had fallen at 1 year after surgery. Prior to surgery, the CVD risk values determined through non-laboratory data were 11.7(4.73,20.03)% for LSG and 14.55(9.78,19.93)% for RYGB. At 1 year post-surgery, the CVD risk value for LSG dropped to 4.6(1.9,7.4)%, while that for RYGB decreased to 6.9(4.1,10.4)%, both of which were significant reductions. The CVD risks calculated using the other two models were also significantly lower after surgery compared to preoperatively. As shown in , We found no statistically significant difference between the LSG and RYGB groups by briefly comparing their RRR at one year postoperatively versus preoperatively.
Table 3 Comparison of the 10-Year Risk of CVD After LSG and RYGB by Different Risk Models
Statistical Analysis of the 30-Year CVD Risk
illustrates the modifications in 30-year CVD risk that were calculated using the data of all patients with obesity before, 3 months after, and 12 months after surgery. Based on laboratory data, the patients’ full CVD risk fell from 53.5(33.5,69.25)% before surgery to 20(10,38.5)% one year afterwards. Based on laboratory data, the patients’ hard CVD risk also decreased one year later. The full CVD risk for patients determined by non-laboratory data dropped significantly from 59.5(40.25,72)% before surgery to 30(16,37.5)% one year after the operation. The hard CVD risk for patients determined by non-laboratory data also decreased significantly one year after the operation.
Table 4 30-Year Change in CVD Risk Calculated by FRS in LSG and RYGB
Changes in the 30-year CVD risk before, at 3 month and 12 month after LSG and RYGB are similarly presented in . The full CVD risk in patients determined by laboratory data decreased from 44(24.5,69.75)% before surgery to 17.5(9.5,35)% 1 year postoperatively in the LSG subgroup and from 59.5(40.75,69.25)% before surgery to 22(8,46)% 1 year postoperatively in the RYGB subgroup. The full CVD risk in patients determined by non-laboratory data as well decreased 1 year after surgery in the LSG and RYGB group. The CVD risk was also significantly lower at 1 year after surgery compared to preoperatively in both subgroups when calculated using FRS. As shown in , a simple comparison of RRR in the LSG and RYGB groups at 1 year after surgery and before surgery showed no statistical difference in calculating patients’ CVD risk at 30 years after surgery.
Table 5 Comparison of the 30-Year Risk of CVD After LSG and RYGB by Different Risk Models
Discussion
Obesity is associated with an increased risk in individuals with CVD.Citation7,Citation28 Patients with obesity are more likely to have a higher risk of cardiovascular mortality and morbidity.Citation29–31 BMS significantly and consistently reduces weight in patients with obesity compared to conventional methods. However, there are few studies using multiple models to evaluate the effect of BMS on the risk of CVD in Chinese patients with obesity.
Firstly, we compared modifications in metabolic indicators prior to, at 3 months, and 12 months following the surgery. Metabolic parameters had decreased strikingly 3 months postoperatively. In middle-aged men, the presence of abdominal obesity was identified as a distinct independent risk factor for coronary artery disease (CAD).Citation32–34 A considerable decrease in WC following BMS can lead to a reduced CVD risk in patients with obesity. Individuals with elevated levels of LDL cholesterol are at an increased risk of developing CAD, which can be relieved by BMS to bring down LDL cholesterol levels.Citation35,Citation36 The HDL cholesterol levels in the current study were considerably higher 12 months after surgery when compared to pre-surgery. In previous studies, HDL cholesterol levels were significantly higher 12 months after BMS compared to preoperatively.Citation36,Citation37 Similarly, Adam et al’s study showed that HDL cholesterol levels were elevated and that HDL cholesterol function was enhanced as early as 6 months after surgery.Citation38 HDL is a protective factor against CVD.Citation39,Citation40 The reduced CVD risk after BMS may be associated with elevated HDL cholesterol levels and enhanced function after surgery.Citation38,Citation41 At one year following BMS, the percentage of diabetes remission in the current study’s individuals with obesity was 77.27%.Additional metabolic syndromes such as hypertension and dyslipidemia also improved significantly, and these metabolic benefits may have contributed to the reduction in CVD risk after BMS. Furthermore, BMI, WC, FPG, and HbA1c were strikingly reduced at 3 months post BMS compared to preoperative values in subgroup analyses of LSG and RYGB. The findings of the present study are consistent with those of earlier studies.Citation42–44
This study aimed to evaluate the effect of BMS on CVD risk among Chinese individuals with obesity through the utilization of multiple models. The findings from all four models revealed that individuals with obesity had considerably lower 10-year CVD risk at 3 and 12 months post-surgery compared to pre-surgery. Elsaid et al looked explored the relationship between BMS and the risk of CVD in individuals who had nonalcoholic fatty liver disease and extreme obesity. Mohamed I. Elsaid et al’s study on the relationship between BMS and CVD risk in people with severe obesity and NAFLD found that at the end of the investigation, BMS reduced the risk of CVD by about 49% compared to non-surgery and could lower the risk of primary composite CVD by 47% versus 50% of secondary composite CVD.Citation45 Similarly, Oliveira et al also demonstrated a substantial decrease in the 10-year CVD risk following BMS, with this decline being particularly prominent in the first year following surgery.Citation13 Among the overall CVD risks in patients with obesity calculated using the China-PAR equation, the relative risk was reduced by 65% 1 year postoperatively compared to those before surgery. In a similar vein, Ke et al discovered that using the China-PAR risk model, the overall atherosclerotic CVD risk 1 year postoperatively decreased from 4.2% to 2.3% in the patient subgroup with a BMI 30 kg/m2 and from 25.3% to 13.9% in the patient subgroup with a BMI > 30 kg/m2.Citation46 The cardiovascular age, general CVD risk, and risk of atherosclerotic CVD also decreased significantly after LSG in Huang et al’s study using the original and recalibrated Framingham 10-year coronary heart disease risk score and three other CVD risk models.Citation4 Similar results were obtained in this study using FRS. At one year after surgery, the 10-year CVD risk calculated using FRS based on laboratory data decreased 63% compared to the pre-surgery level, and the 10-year CVD risk calculated using FRS based on non-laboratory data decreased 56%. Furthermore, according to FRS, the patients’ 30-year CVD risk 1 year postoperatively had also significantly decreased compared to those before surgery. When patients’ 10-year CVD risk was calculated based on laboratory data and non-laboratory data adopting the WHO risk model, the risk was also strikingly reduced one year post-surgery compared to pre-surgery. When the 10-year CVD risk based on laboratory data was calculated using the Global Risk Model, it was shown to be reduced by 71% one year after surgery compared to the pre-operative risk. The risk had greatly decreased 1 year postoperatively compared to those before surgery, but with a lesser reduction compared to laboratory-based data when the patients’ 10-year CVD risk was computed based on non-laboratory data. The reduction in cardiovascular risk in obese patients after bariatric surgery may be related to patients’ reduced body weight and improved metabolic markers. Related studies indicate that the mechanism may be associated with hemodynamic alterations, heightened sympathetic tone, tissue inflammation, and endothelial modifications.Citation8,Citation9
Subsequently, we carried out subgroup analysis according to the type of surgical procedure. In both the LSG and RYGB groups, there was a significant reduction in CVD risk one year after BMS compared to pre-surgery. When patients’ CVD risk was calculated using the China-PAR risk model, the 10-year CVD risk one year after surgery was 70% lower in the LSG group and 62% lower in the RYGB group compared to the pre-surgery risk. Using the WHO risk model based on laboratory data, the 1-year relative CVD risk after LSG was reduced by 50% compared to the pre-operative risk, and the 1-year relative CVD risk after RYGB was reduced by 59% compared to the pre-operative risk. The Global Risk Model revealed a 75% reduction in the relative CVD risk 1 year postoperatively in the LSG group and a 70% reduction in the relative CVD risk 1 year postoperatively in the RYGB group compared to the preoperative risk based on laboratory data. In addition, based on non-laboratory data on post-operative risk, the relative risk of patients in several model groups was significantly reduced. Wei et al used the United Kingdom Prospective Diabetes Study (UKPDS) model to demonstrate a 47.4% reduction in the 10-year CVD risk 1 year postoperatively with LSG and a 50.1% reduction in the 10-year CVD risk 1 year postoperatively with RYGB compared to the preoperative period. The results of this study were similar, in , when multiple models were used to calculate the patients’ 10-year CVD risk, the difference in the effect of cardiovascular risk reduction after surgery was not statistically significant between the LSG and RYGB groups. Also, in , the difference in postoperative cardiovascular risk reduction between the LSG and RYGB groups was not statistically different when calculating the patients’ 30-year CVD risk.
The novelty of this study is the use of multiple models of CVD risk in Chinese patients with obesity before and after BMS. Among them, the WHO risk model and Global Risk Model were applied to assess the CVD risk before and after BMS, which is novel and provides additional theoretical support for the clinical assessment of BMS to reduce the CVD risk in patients with obesity. In the subgroup analysis, various CVD risk models were applied to assess the CVD risk in Chinese patients with obesity before and after LSG and RYGB, adding further theoretical foundation for assessing the CVD risk following various surgical treatments.
There are some limitations to this study. First, this is a retrospective study with a relatively limited sample size. In addition, the follow-up period was relatively short. To get around these, additional research on the advantages of BMS in lowering the CVD risk in people with obesity should be conducted with a large sample size and prolonged follow-up.
Conclusions
In this study, the CVD risk after BMS was significantly reduced compared to the preoperative risk using multiple models. In terms of improving cardiovascular risk, SG and RYGB appear to be equally effective.
Author Contributions
Zheng Wang; Guangzhong Xu; Guanyang Chen; Dongbo Lian; Nengwei Zhang designed the study. Zheng Wang and Guanyang Chen analyzed data and wrote the manuscript. Guangzhong Xu, Dongbo Lian; Nengwei Zhang revising or critically reviewing the article. All authors supervised the study, examine the data, and inspect the manuscript. All authors read and approved the final submitted manuscript.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
Zheng Wang, Guangzhong Xu, Guanyang Chen are co-first authors.
Additional information
Funding
References
- Jaacks LM, Vandevijvere S, Pan A, et al. The obesity transition: stages of the global epidemic. Lancet Diabetes Endocrinol. 2019;7(3):231–240. doi:10.1016/S2213-8587(19)30026-9
- La Sala L, Pontiroli AE. Prevention of diabetes and cardiovascular disease in obesity. Int J Mol Sci. 2020;21(21):8178. doi:10.3390/ijms21218178
- Abarca-Gómez L, Abdeen ZA, Hamid ZA, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390:2627–2642.
- Huang YM, Wang W, Wei SC, et al. Evaluation of persistent efficacy of diabetes remission and decline of cardiovascular risk after laparoscopic sleeve gastrectomy: a preliminary 1-year study. OBES Surg. 2022;32(10):3289–3297. doi:10.1007/s11695-022-06201-x
- Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392:1736–1788.
- Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet. 2016;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
- Liu Y, Douglas PS, Lip G, et al. Relationship between obesity severity, metabolic status and cardiovascular disease in obese adults. Eur J Clin Invest. 2023;53(3):e13912. doi:10.1111/eci.13912
- Alpert MA, Lavie CJ, Agrawal H, Aggarwal KB, Kumar SA. Obesity and heart failure: epidemiology, pathophysiology, clinical manifestations, and management. Transl Res. 2014;164(4):345–356. doi:10.1016/j.trsl.2014.04.010
- Carbone S, Lavie CJ, Arena R. Obesity and heart failure: focus on the obesity paradox. Mayo Clin Proc. 2017;92(2):266–279. doi:10.1016/j.mayocp.2016.11.001
- Hotamisligil GS. Foundations of immunometabolism and implications for metabolic health and disease. Immunity. 2017;47(3):406–420. doi:10.1016/j.immuni.2017.08.009
- Sebastian SA, Co EL, Kanagala SG, Padda I, Sethi Y, Johal G. Metabolic surgery in improving arterial health in obese individuals. Curr Prob Cardiol. 2024;49(3):102359. doi:10.1016/j.cpcardiol.2023.102359
- Hanna A, Frangogiannis NG. Inflammatory cytokines and chemokines as therapeutic targets in heart failure. Cardiovasc Drug Ther. 2020;34(6):849–863. doi:10.1007/s10557-020-07071-0
- Oliveira SC, Neves JS, Souteiro P, et al. Impact of bariatric surgery on long-term cardiovascular risk: comparative effectiveness of different surgical procedures. OBES Surg. 2020;30(2):673–680. doi:10.1007/s11695-019-04237-0
- Gronroos S, Helmio M, Juuti A, et al. Effect of laparoscopic sleeve gastrectomy vs roux-en-y gastric bypass on weight loss and quality of life at 7 years in patients with morbid obesity: the sleevepass randomized clinical trial. JAMA Surg. 2021;156(2):137–146. doi:10.1001/jamasurg.2020.5666
- Aminian A, Wilson R, Al-Kurd A, et al. Association of bariatric surgery with cancer risk and mortality in adults with obesity. JAMA-J Am Med Assoc. 2022;327(24):2423–2433. doi:10.1001/jama.2022.9009
- Schauer DP, Feigelson HS, Koebnick C, et al. Bariatric surgery and the risk of cancer in a large multisite cohort. Ann Surg. 2019;269(1):95–101. doi:10.1097/SLA.0000000000002525
- Fisher DP, Johnson E, Haneuse S, et al. Association between bariatric surgery and macrovascular disease outcomes in patients with type 2 diabetes and severe obesity. JAMA-J Am Med Assoc. 2018;320(15):1570–1582. doi:10.1001/jama.2018.14619
- Singh P, Adderley N, Subramanian A, et al. The impact of bariatric surgery on incident microvascular complications in patients with type 2 diabetes: a matched controlled population-based retrospective cohort study. Diabetes Care. 2021;44(1):116–124. doi:10.2337/dc20-0571
- Aminian A, Al-Kurd A, Wilson R, et al. Association of bariatric surgery with major adverse liver and cardiovascular outcomes in patients with biopsy-proven nonalcoholic steatohepatitis. JAMA-J Am Med Assoc. 2021;326(20):2031–2042. doi:10.1001/jama.2021.19569
- Yang W, Zhan M, Li Z, Sun X, Zhang K. Major adverse cardiovascular events among obese patients with diabetes after metabolic and bariatric surgery: a meta-analysis of matched cohort and prospective controlled studies with 122,361 participates. OBES Surg. 2023;33(7):2098–2107. doi:10.1007/s11695-023-06634-y
- Krishnan A, Hadi Y, Alqahtani SA, et al. Cardiovascular outcomes and mortality after bariatric surgery in patients with nonalcoholic fatty liver disease and obesity. JAMA Network Open. 2023;6(4):e237188. doi:10.1001/jamanetworkopen.2023.7188
- Cui B, Wang G, Li P, et al. Disease-specific mortality and major adverse cardiovascular events after bariatric surgery: a meta-analysis of age, sex, and BMI-matched cohort studies. Int J Surg. 2023;109(3):389–400. doi:10.1097/JS9.0000000000000066
- Jayaraman S, Perez A, Minambres I, Sanchez-Quesada JL, Gursky O. LDL binding to cell receptors and extracellular matrix is proatherogenic in obesity but improves after bariatric surgery. J Lipid Res. 2023;64(11):100451. doi:10.1016/j.jlr.2023.100451
- Yan LD, Lookens PJ, Rouzier V, et al. Comparing six cardiovascular risk prediction models in Haiti: implications for identifying high-risk individuals for primary prevention. BMC Public Health. 2022;22(1):549. doi:10.1186/s12889-022-12963-x
- Chen X, Tu Q, Wang D, et al. Effectiveness of China-PAR and Framingham risk score in assessment of 10-year cardiovascular disease risk in Chinese hypertensive patients. Public Health. 2023;220:127–134. doi:10.1016/j.puhe.2023.05.007
- Kasim SS, Ibrahim N, Malek S, et al. Validation of the general Framingham Risk Score (FRS), SCORE2, revised PCE and WHO CVD risk scores in an Asian population; 2023.
- Riddle MC, Cefalu WT, Evans PH, et al. Consensus report: definition and interpretation of remission in type 2 diabetes. Diabetes Care. 2021;44(10):2438–2444. doi:10.2337/dci21-0034
- Wang R, Olier I, Ortega-Martorell S, et al. Association between metabolically healthy obesity and risk of atrial fibrillation: taking physical activity into consideration. Cardiovasc Diabetol. 2022;21(1):208. doi:10.1186/s12933-022-01644-z
- Lopez-Jimenez F, Almahmeed W, Bays H, et al. Obesity and cardiovascular disease: mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. Eur J Prev Cardiol. 2022;29(17):2218–2237. doi:10.1093/eurjpc/zwac187
- Fuster JJ, Ouchi N, Gokce N, Walsh K. Obesity-induced changes in adipose tissue microenvironment and their impact on cardiovascular disease. Circ Res. 2016;118(11):1786–1807. doi:10.1161/CIRCRESAHA.115.306885
- Shah MS, Brownlee M. Molecular and cellular mechanisms of cardiovascular disorders in diabetes. Circ Res. 2016;118(11):1808–1829. doi:10.1161/CIRCRESAHA.116.306923
- Lakka HM, Lakka TA, Tuomilehto J, Salonen JT. Abdominal obesity is associated with increased risk of acute coronary events in men. Eur Heart J. 2002;23(9):706–713. doi:10.1053/euhj.2001.2889
- Janssen I, Katzmarzyk PT, Ross R. Waist circumference and not body mass index explains obesity-related health risk. Am J Clin Nutr. 2004;79(3):379–384. doi:10.1093/ajcn/79.3.379
- Wang Z, Hoy WE. Waist circumference, body mass index, Hip circumference and waist-to-Hip ratio as predictors of cardiovascular disease in Aboriginal people. Eur J Clin Nutr. 2004;58(6):888–893. doi:10.1038/sj.ejcn.1601891
- Ponce DLG, Sanchez-Aguilar HA, Aguilar-Salinas CA, Herrera MF. Reaching LDL-C targets in patients with moderate, high, and very high risk for cardiovascular disease after bariatric surgery according to different guidelines. OBES Surg. 2021;31(5):2087–2096. doi:10.1007/s11695-021-05221-3
- Iqbal Z, Bashir B, Adam S, et al. Glycated apolipoprotein B decreases after bariatric surgery in people with and without diabetes: a potential contribution to reduction in cardiovascular risk. Atherosclerosis. 2022;346:10–17. doi:10.1016/j.atherosclerosis.2022.01.005
- Rubio-Almanza M, Camara-Gomez R, Hervas-Marin D, Ponce-Marco JL, Merino-Torres JF. Cardiovascular risk reduction over time in patients with diabetes or pre-diabetes undergoing bariatric surgery: data from a single-center retrospective observational study. BMC Endocr Disord. 2018;18(1):90. doi:10.1186/s12902-018-0317-4
- Adam S, Ho JH, Liu Y, et al. Bariatric surgery-induced high-density lipoprotein functionality enhancement is associated with reduced inflammation. J Clin Endocr Metab. 2022;107(8):2182–2194. doi:10.1210/clinem/dgac244
- Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med. 1977;62(5):707–714. doi:10.1016/0002-9343(77)90874-9
- Xue H, Zhang M, Liu J, Wang J, Ren G. Structure-based mechanism and inhibition of cholesteryl ester transfer protein. Curr Atheroscler Rep. 2023;25(4):155–166. doi:10.1007/s11883-023-01087-1
- Stadler JT, Marsche G. Obesity-related changes in high-density lipoprotein metabolism and function. Int J Mol Sci. 2020;21(23):8985. doi:10.3390/ijms21238985
- Chew C, Tan IJ, Ng H, Lomanto D, So J, Shabbir A. Early weight loss after laparoscopic sleeve gastrectomy predicts midterm weight loss in morbidly obese Asians. Surg OBES Relat Dis. 2017;13(12):1966–1972. doi:10.1016/j.soard.2017.05.016
- Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes. New Engl J Med. 2014;370(21):2002–2013. doi:10.1056/NEJMoa1401329
- Ma S, Wang L, Chen J, Zhao Y, Jiang T. The effect of laparoscopic sleeve gastrectomy on type 2 diabetes remission outcomes in patients with body mass index between 25 kg/m 2 and 32.5 kg/m 2. Asian J Surg. 2022;45(1):315–319. doi:10.1016/j.asjsur.2021.06.001
- Elsaid MI, Li Y, Bridges J, Brock G, Minacapelli CD, Rustgi VK. Association of bariatric surgery with cardiovascular outcomes in adults with severe obesity and nonalcoholic fatty liver disease. JAMA Network Open. 2022;5(10):e2235003. doi:10.1001/jamanetworkopen.2022.35003
- Ke Z, Li F, Zhou X, Sun F, Zhu Z, Tong W. Impact of metabolic surgery on 10-year cardiovascular disease risk in Chinese individuals with type 2 diabetes. Surg OBES Relat Dis. 2021;17(3):498–507. doi:10.1016/j.soard.2020.11.013