
Abstract
Background
To evaluate the association of the baseline triglyceride-glucose (TyG) index in the first trimester of pregnancy with the risk of large for gestational age (LGA) in Southeast Chinese pregnant women.
Methods
A prospective birth cohort study recruiting 12,108 pregnant women at their first prenatal visit before 13 gestation weeks was conducted in 2019–2022. Baseline characteristics were collected from medical records or using questionnaires and blood samples were collected in the first trimester. The TyG index was obtained through the formula: ln[triglyceride (mg/dl)×fasting plasma glucose (mg/dl)/2]. The binary logistic regression model was performed to calculate the odds ratio (OR) and 95% confidence intervals (CI) to reveal the relationship between TyG index and LGA. Receiver-operating characteristic curve analysis was conducted to evaluate the ability of the TyG index to predict the risks of LGA.
Results
The overall incidence of LGA in the current study was 11.4% and the incidence of LGA increased with the baseline TyG index increasing. The risk of LGA was 2.05 (1.64, 2.57) for per unit increase in baseline TyG index. The increasing trend was found across the TyG index quartiles and the highest TyG quartiles raised the risk of LGA to 1.86 (95% CI: 1.51, 2.27) compared to the bottom TyG quartiles after full adjustment. The risk of LGA remained positive after stratification analysis. The AUC was 0.584 (95% CI: 0.569~0.600) in the entire subject, and the threshold was 8.34, with a sensitivity of 0.74 and specificity of 0.38.
Conclusion
The findings suggested that a higher TyG index in the first trimester was independently associated with higher risk of LGA and high TyG index in the first trimester may play as a early predictor for LGA.
Introduction
Large for gestational age (LGA) refers to a birth weight larger than the 90th percentage of the birth weight curve for infant sex and gestational age.Citation1 Large birth weight has adverse consequences on mothers and infants in the short and long term. For mothers, it is known that LGA is associated with cesarean section, the trauma of the birth canal, prolonged labor, and postpartum hemorrhage.Citation2,Citation3 For newborn, LGA can increase the risk of shoulder dystocia, hypoglycemia, brachial plexus injury, skeletal injury, clavicular fracture, perinatal asphyxia, and mortality.Citation4–7 Furthermore, LGA also influences long-term risks of metabolic disease in adult life. Therefore, early prediction and minimization or avoidance of LGA may help to improve adverse pregnancy outcomes.
There has been an increase in the average birth weight and the prevalence of LGA over the past decades in many countries of the world.Citation8–13 The increase was also found in China,Citation14,Citation15 which coincided with the increasing prevalence of maternal overweight and obesity, excessive weight gain during pregnancy, high parity, older maternal age, pre-gestational diabetes, and gestational diabetes mellitus after positive socioeconomic change.Citation9,Citation16 The endocrine and metabolic in the first trimester of pregnancy is crucial for fetal growth and development. It is well known that LGA is linked with adverse intrauterine exposures, such as maternal high hyperglycemia and abnormal blood lipid level, and suboptimal intrauterine environment could lead to structural and physiological changes that may ultimately affect fetal growth.Citation9 As early as 1952, the Pedersen hypothesis explained that maternal hyperglycemia due to insulin resistance can lead to fetal hyperglycemia, causing the fetus to overproduce insulin and thus overgrowth can occur.Citation17 Given the association between adverse intrauterine exposures and fetal development, early identification of pregnant women at risk for fetal overgrowth has become a matter of urgency. Recently, the triglyceride-glucose (TyG) index, calculated as ln[fasting triglycerides (mg/dl) ×fasting blood glucose (mg/dl)/2] has been pushed as a useful indicator of insulin resistance to predict the risk of adverse pregnancy outcomes including gestational diabetes mellitus and LGACitation18,Citation19 . However, there were few studies regarding the role of the first trimester TyG index about LGA, especially in the Chinese pregnant population. In this regard, we would like to elucidate the association between the quartiles of TyG index in the first trimester and the risk of LGA, especially among pregnant women in southeast China, using the hospital-based prospective birth cohort study.
Methods
Study Population
The data for analysis was derived from the Fujian Birth Cohort Study, which is a large prospective cohort study carried out in the Fujian Maternity and Child Health Hospital and pregnant women in the first trimester of pregnancy who attended to take regular prenatal visit and delivery in this facility was invited to participate in the study. Women aged less than 18 years old, or with severe liver or kidney disease, cardiovascular disease, psychiatric disorders, autoimmune disease were excluded. Each participant was contacted during pregnancy and required to finish three questionnaires in the first, second and third trimesters as well as blood samples. Detailed clinical information of delivery was collected from the medical records.
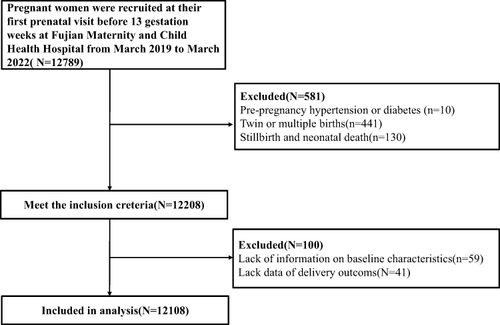
Between March 2019 and March 2022, this cohort study recruited 12,789 pregnant women who took their first prenatal visit before 13 gestation weeks and completed all the perinatal care, required questionnaires, and blood samples during the whole pregnancy. We excluded women with pre-pregnancy diabetes, hypertension. We also exclude those who lacked important information on baseline characteristics, delivery outcomes, or multiple births, and those who delivered before 28 weeks of gestation. Finally, 12,108 pregnant women with singleton birth were eligible for the final analysis. The participant flowchart is shown in . This study was approved by the Ethics Committee of Fujian Maternity and Child Health Hospital (approval number: 2017KR-030). Written informed consent was obtained from the participants before enrollment.
Figure 1 Flowchart of subject selection.
Data Collection and Definition
Baseline characteristics of maternal age, educational level, marital status, height, pre-pregnancy weight, gravidity, parity, smoking, gestational age, birth weight, delivery way, and infant sex were collected from medical records or using a questionnaire through face-to-face interview. Prepregnancy body mass index (BMI) was calculated as prepregnancy weight/height2(kg/m2) and was classified as underweight (BMI<18.5kg/m2), normal weight (18.5≤BMI<24kg/m2), overweight and obese (BMI≥24kg/m2) based on Chinese adult weight standard.Citation20 Hyperthyroidism and hypothyroidism were defined based on the American thyroid association guideline.Citation21
Blood samples were collected in the first trimester at fasting and plasma glucose (FPG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and triglyceride (TG) were tested. Blood pressure measured in the first trimester using an upper arm oscillometric device was recorded. The TyG index was calculated as ln[fasting triglycerides (mg/dl) ×fasting blood glucose (mg/dl)/2].
Statistical Analysis
Continuous variables are presented as the mean±standard deviation or medians (interquartile ranges), and categorical variables are shown as the numbers and percentages. Characteristics analysis of the participant according to the TyG index quartiles were compared using analysis of variance (ANOVA) for continuous variables with a normal distribution or Kruskal–Wallis test with skewed distribution, and Chi-square tests for categorical variables. Logistical regression models were used to estimate the odds ratio (OR) and 95% confidence interval (CI) to determine the association of TyG index level (categorized into quartiles) with the risk of LGA. We adjusted for two models. Model 1 was adjusted for maternal age (continuous variable), education level (college and above, High school or equivalent, and less than high school), marital status (married or never married), gravidity (1,2 and ≥3), parity (primiparous or multiparous), gestational age at delivery (continuous variable), prepregnancy BMI (underweight, normal weight and overweight or obese), infant sex (boy or girl) and smoking status (yes or no); Model 2 was further adjusted for baseline FPG, systolic blood pressure, diastolic blood pressure, HDL-C, LDL-C, TC, and TG.
Subgroup analyses were also conducted according to maternal age (≤35, >35 years), educational level (college and above, High school or equivalent, and Less than high school), gravidity (1, 2, and ≥3), parity (primiparous or multiparous) and infant sex (boy or girl). Potential modification effects on the LGA risk of these factors were examined by testing the corresponding interaction terms.
Furthermore, Receiver operating characteristic (ROC) curves and areas under the curve (AUCs) were used to assess the ability of the indices to detect LGA infants among different prepregnancy BMI categories. The threshold values of the TyG index were defined as optimal based on the maximizing of the Youden J-index (sensitivity+specificity-1).Citation22 Finally, to test the robustness of the results, sensitivity analysis was conducted by excluding pregnant women with hyperthyroidism, hypothyroidism, or gestational diabete mellitus (GDM). All analyses were performed using the statistical software package R software, version 4.4.2. Statistical significance was defined as P<0.05.
Results
Basic Characteristics of the Study Population
The baseline characteristics of 12,108 participants grouped by TyG index quartiles are provided in . The average TyG index was 8.46±0.34 and participants with higher TyG index values were more often with lower educational level, married, overweight or obese, high gravidity, and be multiparous (P < 0.001). The overall incidence of GDM was 15.8%, and the incidence for TyG index quartiles rose with the TyG index quartiles increased. The TyG index increased significantly with increasing baseline FPG, LDL-C, and TG but with decreasing baseline HDL-C (all P<0.001).
Table 1 Basic Characteristics of the Study Population by Triglyceride-Glucose (TyG) Index Quartile
Association Between Baseline TyG Index and Risk of LGA
Values of the TyG index were divided into quartiles and the lowest quartile was used as the reference group. We performed binary logistic regression analysis to explore the association between the quartiles of the TyG index and the risk of LGA, with adjusting for different potential confounding factors (). The incidences of LGA of baseline TyG index were 7.8%,10.5%,11.3% and 16.0%, respectively, and the overall incidence was 11.4%. The risk of LGA showed an increasing trend with the increasing of TyG index in the first trimester. The risk of LGA was 2.05 (1.64,2.57) for per unit increase in baseline TyG index. Compared with the lowest TyG index quartiles (Q1,<8.23), the risk of LGA infant in Q2 (8.23≤TyG index<8.45), Q3 (8.45≤TyG index<8.68), Q4 (≥8.68) were 1.34 (95% CI:1.10-1.57), 1.29 (95% CI:1.09–1.54), and 1.65 (95% CI:1.39–1.96), respectively, in the multivariate adjusted model 1(Ptrend<0.001). After further adjusting confounding factors (baseline FPG, systolic blood pressure, diastolic blood pressure, HDL-C, LDL-C, TC, and TG), the treads of ORs remained.
Table 2 Association of Triglyceride-Glucose (TyG) Index with Large for Gestational Age (LGA)
Stratification Analysis on the Association Between Baseline TyG Index with Risk of LGA
The results of subgroup analyses stratified by advanced age, education level, gravidity, parity, infant sex, and smoking status kept the same with the main results and no significant interactions were observed between all subgroup variables with the baseline TyG index and its quartiles categories on the risk of LGA infant, with adjustment for confounding factors (all P interaction>0.05). It is worth noting that the association of baseline TyG index quartile changes with LGA seemed to be somewhat stronger in individuals with age <35 years, educational level less than high school, low gravidity, primiparous, and smokers ().
Table 3 Stratification Analysis on the Association Between Triglyceride-Glucose (TyG) Index and Large for Gestational Age (LGA)
ROC Curve Analyses of Baseline TyG Index Predicting LGA
In the Receiver operating characteristic (ROC) curve analyses, the baseline TyG index showed significant areas under the ROC curve (AUCs), and the AUC of the baseline TyG index for LGA was 0.584 (95% CI:0.569~0.600) in the entire study subject. The threshold was 8.34, with a sensitivity of 0.74 and a specificity of 0.38. For prepregnancy BMI categories, the AUCs (95% CI) for underweight, normal weight, and overweight or obese groups were 0.563 (95% CI:0.508~0.618), 0.568 (95% CI:0.549~0.587), 0.554 (95% CI:0.518~0.589), respectively ().
Table 4 Receiver Operating Characteristic (ROC) Analysis of the Triglyceride-Glucose (TyG) Index for Predicting Large for Gestational Age (LGA)
Sensitivity Analysis
In the sensitivity analyses, consistent results were found after excluding women with hyperthyroidism or/and hypothyroidism, GDM (). That is, when excluded pregnant women with thyroid dysfunction or GDM, the ORs of LGA in the highest quartile of the TyG index were still significant after adjustment for the confounding factors.
Table 5 Association of Triglyceride-Glucose (TyG) Index with Large for Gestational Age (LGA)
Discussion
As the economy grows and the standard of living rises, the birth weight and the incidence of fetal overgrowth, including macrosomia and LGA raised over the past decades in many countries. The overall incidence of LGA in the current study was 11.4%. In the world, there is a considerable variation in the incidence of LGA, ranging from 5% to 20% in developed countries.Citation13,Citation23 The incidence of LGA varies in Chinese cities, ranging from 8.2% to 17.7%.Citation23 This discrepancy in LGA incidence might be due to the application of different standards and characteristics of the study populations. At the same time, we should also realize that in the face of such a severe epidemic trend in birth weight and increased LGA incidence,it is crucial to reduce the incidence of LGA.
Based on this prospective birth cohort study, significant associations were found between the first trimester of pregnancy maternal TyG index with risk of LGA among pregnant women. The results suggest that in the first trimester TyG index and its quartiles change are positively related to the risk of LGA after controlling for maternal age, education level, marital status, gravidity, parity, gestational age at delivery, prepregnancy BMI, infant sex, smoking status, baseline FPG, systolic blood pressure, diastolic blood pressure, HDL-C, LDL-C, TC, and TG. Furthermore, a 1-unit increase in the baseline TyG index increased 105% risk of LGA after the full adjustment. TyG index, as an insulin resistance indicator,Citation24 could be applied as an indicator for the prediction of pregnancy outcomes among pregnant women. Our finding demonstrated that the baseline TyG index in early pregnancy is a proper predictor of incident LGA, independent of other risk factors among pregnant women in Southeast China.
High levels of triglyceride and glucose are common in pregnant women and are related to birth weight.Citation18,Citation25,Citation26 Many studies found that women who delivered LGA newborns are accompanied by increasing triglyceride levels.Citation27 The ratio of triglyceride combines glucose levels could be more stable. The study was in line with previous studies.Citation18,Citation28 A prospective study carried out in Iran found that the risk of LGA in women with the top tertile of TyG index was 5.3-folds than that in women with the lowest tertile.Citation29 Liu’s research suggested that the TyG in the early trimester of pregnancy was independently related to LGA infant delivery and the TyG values in the highest tertile showed a higher risk of delivering an LGA infant.Citation28
TyG index has been widely proven to be the best indicator of insulin resistance in individuals including pregnancies.Citation30 Some researchers have promoted the TyG index as a surrogate of insulin resistanceCitation31.Several studies have articulated the predictive ability of the TyG index for pregnancy-related complications.Citation18,Citation32,Citation33 We focused our work on the power of the first trimester TyG index to predict the possibility of LGA and found that larger neonates and higher incidence of LGA were born in women with higher TyG index. A higher TyG index means an increase in IR, which leads to a decrease in lipoprotein lipase activity. The derived fatty acids enter the umbilical cord blood and are stored in fetal adipose tissue, resulting in accelerated fetal growth and obesity.Citation34 On the other hand, IR promotes the process of protein synthesis and reduces lipolysis by accelerating the rate of activation of the amino acid transfer system.Citation35 Since the TyG index has been recognized as an indicator of IR in pregnancies, we also analyzed using ROC curve analysis to detect the power of prediction on LGA infants and found a high sensitivity and specificity in identifying LGA infant delivery. These results suggested the potential clinical utility for predicting the LGA of the TyG index. To the best of our knowledge, the current study is the first effort to elucidate the predictive power of the TyG index in the early trimester of pregnancy on LGA infants in the Southeast China pregnant women.
Furthermore, we found the effect of increased TyG index on LGA risk of was stronger among individuals with age <35 years, educational level less than high school, low gravidity, primiparous, and smokers. The potential explanation for this discrepancy may be partly explained by the higher TyG index in these participants. More studies are warranted to further investigate the reasons and potential mechanisms underlying the relationship between the TyG index and LGA risk in these participants. Research suggests that pre-pregnancy obesity is the independent risk factors for LGA, but the result of ROC found that the sensitivity of TyG in underweight and overweight is lower than overall and normal weight value. The confused results are unknown and deeper research is needed. Healthcare providers and clinical workers should put more effort into these pregnant women to reduce the likelihood of delivering a LGA infant.
Detecting risk factors for pregnancy adverse outcomes in early pregnancy might be of great value in improving pregnancy outcomes. The current study confirmed that the first trimester TyG index could be used as an effective predictor of LGA in clinical practice. The greatest strength of the current study is the prospective design, with questionnaire data and blood sample collection in the first trimester. Several limitations to this study should be recognized. Firstly, we lacked information on some potential confounding factors, such as gestational weight gain, diet, physical exercise, and serum insulin, which may lead to bias of the results. Secondly, the study population consisted of women who received prenatal visit and delivery in Fujian Maternity and Child Health Hospital, which limits the generalizability to the other population. Thirdly, the level of lipid and glucose in the late trimester were not included in the adjusted models, which might affect the result and cannot fully account for the independent contribution of baseline TyG index to fetal growth. Lastly, only Chinese women were enrolled, our results cannot be generalized to be clinically effective for the western population as the rates of overweight and obese in Western are substantially higher.
Conclusion
In conclusion, in this study, a higher TyG index in the first trimester was independently and significantly associated with a higher risk of LGA, and high TyG index in the first trimester may be the early predictor for LGA. As an easily available index in the early pregnancy, the TyG index can help clinical healthcare providers early identification of high-risk groups and active intervention to improve pregnancy outcomes.
Abbreviations
LGA, large for gestational age; TyG, triglyceride-glucose; BMI, body mass index; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride; OR, odds ratio; CI, confidence interval; ROC, receiver operating characteristic; AUC, areas under the curve.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Fujian Maternity and Child Health Hospital and complied with the Declaration of Helsinki. The written informed consent was obtained from every participant before enrollment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report there are no competing interests to declare.
Acknowledgments
The authors thank the perinatal care providers at the department of obstetrics for their professional skills in managing patients.
Additional information
Funding
References
- Harvey L, Elburg RV, Beek EMVD. Macrosomia and large for gestational age in Asia: one size does not fit all. J Obstetrics Gynaecol Res. 2021;47(6):1929–1945. doi:10.1111/jog.14787
- Araujo Júnior E, Peixoto AB, Zamarian AC, Elito Júnior J, Tonni G. Macrosomia. Clin Obstetrics Gynaecol. 2017;38:83–96.
- Beta J, Khan N, Khalil A, Fiolna M, Ramadan G, Akolekar R. Maternal and neonatal complications of fetal macrosomia: systematic review and meta-analysis. Ultrasound Obstetrics Gynecol. 2019;54(3):308–318. doi:10.1002/uog.20279
- Schwartz R, Teramo KA. What is the significance of macrosomia? Diabetes Care. 1999;22(7):1201–1205. doi:10.2337/diacare.22.7.1201
- Anoon SS, Rizk DE, Ezimokhai M. Obstetric outcome of excessively overgrown fetuses (> or = 5000 g): a case-control study. J Perinat Med. 2003;31(4):295–301. doi:10.1515/JPM.2003.041
- Gu S, An X, Fang L, et al. Risk factors and long-term health consequences of macrosomia: a prospective study in Jiangsu Province, China. J Biomed Res. 2012;26(4):235–240. doi:10.7555/JBR.26.20120037
- Li G, Kong L, Li Z, et al. Prevalence of macrosomia and its risk factors in China: a multicentre survey based on birth data involving 101,723 singleton term infants. Paediatr Perinat Epidemiol. 2014;28(4):345–350. doi:10.1111/ppe.12133
- Schack-Nielsen L, Mølgaard C, Sørensen TI, Greisen G, Michaelsen KF. Secular change in size at birth from 1973 to 2003: national data from Denmark. Obesity. 2006;14(7):1257–1263. doi:10.1038/oby.2006.143
- Surkan PJ, Hsieh CC, Johansson AL, Dickman PW, Cnattingius S. Reasons for increasing trends in large for gestational age births. Obstet Gynecol. 2004;104(4):720–726. doi:10.1097/01.AOG.0000141442.59573.cd
- Leddy MA, Power ML, Schulkin J. The impact of maternal obesity on maternal and fetal health. Rev Obstet Gynecol. 2008;1(4):170–178.
- Oken E. Secular trends in birthweight. Nestle Nutr Inst Workshop Ser. 2013;71:103–114.
- Carter JH, Woolcott CG, Liu L, Kuhle S. Birth weight for gestational age and the risk of asthma in childhood and adolescence: a retrospective cohort study. Int J Med. 2019;104(2):179–183.
- Henriksen T. The macrosomic fetus: a challenge in current obstetrics. Acta Obstet Gynecol Scand. 2008;87(2):134–145. doi:10.1080/00016340801899289
- Modzelewski J, Pokropek A. Large-for-gestational-age or macrosomia as a classifier for risk of adverse perinatal outcome: a retrospective cross-sectional study. J Maternal Fetal Neonatal Med. 2022;35(25):5564–5571. doi:10.1080/14767058.2021.1887127
- Lu Y, Zhang J, Lu X, Xi W, Li Z. Secular trends of macrosomia in southeast China, 1994-2005. BMC Public Health. 2011;11(1):818. doi:10.1186/1471-2458-11-818
- Kramer MS, Morin I, Yang H, et al. Why are babies getting bigger? Temporal trends in fetal growth and its determinants. J Pediatr. 2002;141(4):538–542. doi:10.1067/mpd.2002.128029
- Pedersen J. Diabetes and pregnancy; blood sugar of newborn infants during fasting and glucose administration. Ugeskr Laeger. 1952;114(21):685.
- Pazhohan A, Rezaee Moradali M, Pazhohan N. Association of first-trimester maternal lipid profiles and triglyceride-glucose index with the risk of gestational diabetes mellitus and large for gestational age newborn. J Maternal Fetal Neonatal Med. 2019;32(7):1167–1175. doi:10.1080/14767058.2017.1402876
- Wang D, Xu S, Chen H, Zhong L, Wang Z. The associations between triglyceride to high-density lipoprotein cholesterol ratios and the risks of gestational diabetes mellitus and large-for-gestational-age infant. Clin Endocrinol. 2015;83(4):490–497. doi:10.1111/cen.12742
- Zhou B. 我国成人体重指数和腰围对相关疾病危险因素异常的预测价值 [Predictive values of body mass index and waist circumference to risk factors of related diseases in Chinese adult population]. Zhonghua Liu Xing Bing Xue Za Zhi. 2002;23(1):5–10. Chinese.
- Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid. 2017;27(3):56.
- Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3(1):32–35. doi:10.1002/1097-0142(1950)3:1<32::AID-CNCR2820030106>3.0.CO;2-3
- He JR, Li WD, Lu MS, et al. Birth weight changes in a major city under rapid socioeconomic transition in China. Scientific Reports. 2017;7(1):1031. doi:10.1038/s41598-017-01068-w
- Zhao Y, Yang X, Wu Y, et al. Association of triglyceride-glucose index and its 6-year change with risk of hypertension: a prospective cohort study. Nutr Metab Cardiovasc Dis. 2023;33(3):568–576. doi:10.1016/j.numecd.2022.12.001
- Schaefer-Graf UM, Graf K, Kulbacka I, et al. Maternal lipids as strong determinants of fetal environment and growth in pregnancies with gestational diabetes mellitus. Diabetes Care. 2008;31(9):1858–1863. doi:10.2337/dc08-0039
- Son GH, Kwon JY, Kim YH, Park YW. Maternal serum triglycerides as predictive factors for large-for-gestational age newborns in women with gestational diabetes mellitus. Acta Obstet Gynecol Scand. 2010;89(5):700–704.
- Mahindra MP, Sampurna MTA, Mapindra MP, Sutowo Putri AM. Maternal lipid levels in pregnant women without complications in developing risk of large for gestational age newborns: a study of meta-analysis. F1000Research. 2020;9:1213. doi:10.12688/f1000research.26072.2
- Liu PJ, Liu Y, Ma L, et al. The Predictive Ability of Two Triglyceride-Associated Indices for Gestational Diabetes Mellitus and Large for Gestational Age Infant Among Chinese Pregnancies: a Preliminary Cohort Study. Dove Press. 2020.
- Pazhohan A, Rezaee Moradali M, Pazhohan N. Association of first-trimester maternal lipid profiles and triglyceride-glucose index with the risk of gestational diabetes mellitus and large for gestational age newborn. j Maternal Fetal Neonatal Med. 2017;1.
- Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13(1):1–10. doi:10.1186/s12933-014-0146-3
- Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–3351. doi:10.1210/jc.2010-0288
- Kim JA, Kim J, Roh E, et al. Triglyceride and glucose index and the risk of gestational diabetes mellitus: a nationwide population-based cohort study. Diabetes Res Clin Pract. 2021;171:108533. doi:10.1016/j.diabres.2020.108533
- Massimino M, Monea G, Marinaro G. The Triglycerides and Glucose (TyG) Index Is Associated with 1-Hour Glucose Levels during an OGTT. Int J Environ Res Public Health. 2022;20(1). doi:10.3390/ijerph20010787
- Herrera E, Ortega-Senovilla H. Disturbances in lipid metabolism in diabetic pregnancy - Are these the cause of the problem? Best practice & research. Clin Endocrino Metab. 2010;24(4):515–525.
- Liang N, Zhu H, Cai X, et al. The high maternal TG level at early trimester was associated with the increased risk of LGA newborn in non-obesity pregnant women. Lipids Health Dis. 2018;17(1):294. doi:10.1186/s12944-018-0936-9