
Abstract
Aims/Hypothesis
Only a few studies reported the incidence of type 2 diabetes (T2D). Understanding recent trends in diabetes is vital for planning future diabetes care. This study updated national trends in the prevalence and incidence of type 2 diabetes (T2D) in the Netherlands from 2004–2020.
Methods
The DIAbetes, MANagement and Treatment (DIAMANT) cohort was used. A cross-sectional design with yearly measurements for the study period was used. The prevalence was calculated by dividing the total number of people with T2D by the total number of all residents. The incidence was calculated by dividing new cases of T2D by the resident population at risk during the calendar year of interest.
Results
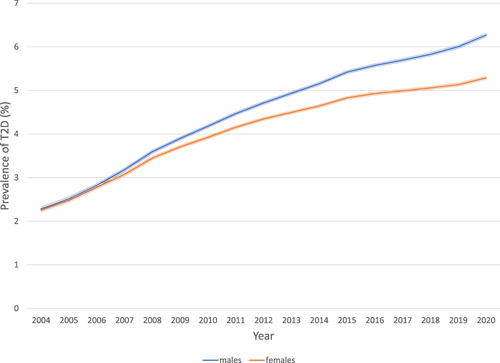
Among men, the prevalence of T2D in the Netherlands increased from 2.3% in 2004 to 6.3% in 2020. Women’s prevalence increased from 2.3% in 2004 to 5.3% in 2020. During 2005–2009, the incidence rate for both men and women was relatively stable Between 2010 and 2020, the incidence rate fell about 1.5 per 1000 in both men and women.
Conclusion
From 2004–2020, the prevalence of T2D in the Netherlands more than doubled, with a decreasing incidence from 2010 onwards.
Plain Language Summary
Research in context
What is already known about this subject?
Many studies have reported the increasing prevalence of type 2 diabetes (T2D). However, only a few studies reported the incidence.
In a recent systematic review of all these studies, the incidence fell in over a third of the most high-income populations and increased in a minority of populations. Data from the Netherlands were included, but they date back to 1996.
Understanding recent trends in diabetes, the prevalence and incidence are vital for planning future diabetes care.
What is the key question?
To update national trends in the prevalence and incidence of T2D in the Netherlands for 2004-2020.
What are the new findings?
During 2004-2020, the prevalence of T2D in the Netherlands more than doubled, with a decreasing incidence from 2010 onwards.
How might this impact on clinical practice in the foreseeable future?
It demonstrates the effectiveness of preventive strategies, public health education and awareness campaigns contributing to this trend.
Introduction
Type 2 diabetes (T2D) is a severe public health concern with a high impact on human life and health expenditure. Many studies worldwide have reported the increasing prevalence of T2D.
Only a few studies reported the incidence. In a systematic review of all these studies, the incidence fell in over a third of the most high-income populations and increased in a minority of populations.Citation1 The countries that showed stable or decreasing trends from 2005 on were Europe and East Asia. Understanding trends in diabetes, the prevalence and the incidence is vital for planning future diabetes care. This study aimed to update national trends in the prevalence and incidence of T2D in the Netherlands for 2004–2020, in the total population and per sex and age category.
Research Design and Methods
Design and Setting
Data for this study was obtained from the DIAbetes, MANagement and Treatment (DIAMANT) cohort. DIAMANT is a large and complete population-based, dynamic, prospective cohort of persons with diabetes derived from anonymized electronic medical records of Dutch general practitioners who consented to have their regular care electronic file extracted in the PHARMO General Practitioner (GP) Database for research purposes. The Dutch PHARMO GP data is a population-based database containing ~3.2 million Dutch inhabitants in 2020 (~20% of the Dutch population).Citation2,Citation3 The PHARMO GP data are representative of the Dutch population with regard to the demographic characteristics (sex, age and degree of urbanization) and diagnoses in primary care.Citation3 The DIAMANT cohort contains structured information on people with diabetes using electronic GP information systems, eg examinations, medication, and diagnoses (including symptoms). In addition, the cohort contains basic information on all citizens registered in the practice. Due to the Dutch healthcare system, nearly every citizen is registered with one GP practice, resulting in a complete population-based patient file representative for the Dutch population. Therefore, a cross-sectional design with yearly measurements for the study period was used.
Definition of type 2 diabetes
T2D was defined as (1) a GP-recorded diagnosis of T2D (ICPC code T90.02) or (2) two or more recorded prescriptions of drugs used in diabetes (ATC code A10B) within six months. The date of T2D diagnosis was defined as the date of the first recorded diagnosis for T2D or the first prescription, whichever occurred first.
Study population
All people in the patient file who were registered as present in the GP practice (active) on January 1st of each calendar year were included for the prevalence. In addition, all people with T2D in the cohort who had T2D prior to or on January 1st of each calendar year were included in determining the prevalence on January 1st. The observed prevalence was calculated by dividing the sum of people with T2D by the total number of residents in the patient file per calendar year by sex. The observed prevalence was also calculated per calendar year by sex and age category (0–29 years, 30–54 years, 55–74 years and ≥75 years).
For the incidence, all people in the patient file who were registered as being present in the GP practice (active) on January 1st of each calendar year and who were registered for at least one year in the patient file were included. All people with diabetes before January 1st of each calendar year were excluded. The observed incidence of T2D was determined among all people in the patient file who had at least one year of data available, defined as the population at risk. At least one year of data availability was required to ensure each person had an equal chance of being marked as an incident person with T2D. The observed incidence was calculated by dividing the sum of people with incident T2D by the total number of person-time at risk in the patient file for both females and males during the calendar year. Person-time at risk in the patient file was defined as the time between January 1st of the year, or start follow-up in the GP practice, whatever came last, and diagnosis date of T2D, December 31st of the year or end of follow-up in the GP practice, whatever came first.
The guidelines outlined in the Declaration of Helsinki were followed. The ethics research committee of the VU Medical Centre approved the DIAMANT study and appreciated that the study used anonymous data and, therefore, was not subjected to ethics review according to the Medical Research Involving Human Subjects Act (WMO).
Statistical analyses
Descriptive statistics were used for all analyses. In addition, 95% confidence intervals were calculated around all prevalence and incidence estimates. All data were analyzed using SAS programs in SAS Enterprise Guide version 8.2 (SAS Institute Inc., Cary, NC, USA) and conducted in Windows using SAS version 9.4.
Results
Over 2004–2020, the number of active people in the patient file (ie still registered as being present) increased from almost 1 million on January 1st, 2004, to approximately 3.2 million on January 1st 2020. As a result, the number of people with T2D increased from nearly 22.000 on January 1st 2004, to almost 190.000 on January 1st 2020. In 2004, the mean age of people with T2D was 63 years (SD: 12); 49% were men. In 2020, the mean age was 68 years (SD: 13), and the percentage of men was 53%.
shows the observed prevalence of T2D between 2004–2020 by sex. In women and men, the observed prevalence increases over time to a percentage of approximately 6.3 among men and 5.3 among women.
Figure 1 Prevalence of T2D over time by sex.
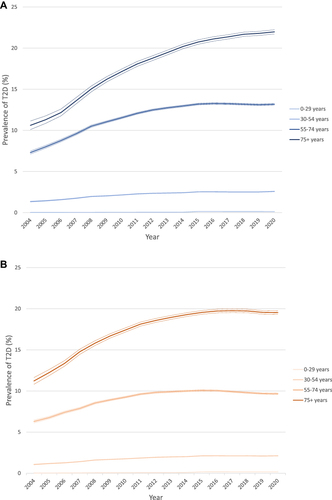
shows the prevalence of T2D between 2004–2020 among men (a) and women (b), stratified by age category. The prevalence has increased in the older age groups, equally in women and men.
Figure 2 Prevalence of T2D over time by age – men (a) and women (b).
shows the observed incidence of T2D in the Netherlands between 2005–2020 among women and men. The incidence decreased from 2010 to 2020, with exception of 2015.
Figure 3 Incidence of T2D over time by sex.
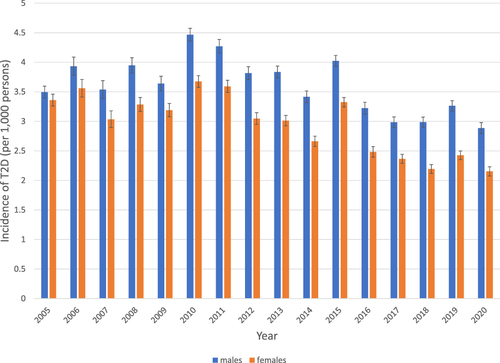
During 2005–2009, the incidence rate for both men and women fluctuated between 3.5 and 4 per 1000 persons in men and between 3 and 3.5 per 1000 persons in women. The incidence rate per 1000 persons decreased from 4.5 in men and 3.5 in women in 2010 to 3.0 in men and 2.0 in women in 2020.
Discussion
This study shows that the prevalence of T2D increased between 2004 and 2020, and the incidence decreased after 2011, mainly in the older age categories, equal for women and men.
The slowing of the prevalence and the decreased incidence of T2D suggests a slowing of the diabetes epidemic. The study results confirm what has already been seen in Europe, the United States, and East Asia in the last decade.Citation1,Citation4 This discordance underlines the importance of reporting prevalence and incidence rates.
Several explanations for the decreased incidence with a stabilizing prevalence can be suggested. First, the ageing of the population combined with improved survival can explain the increased prevalence. A possible explanation for the decreasing incidence rate can be that the proportion of people with overweight and obesity has stabilized since 2014 in the Netherlands. In 2021, the proportion of overweight was reported to have stabilized at 36% with mild overweight and 14% with obesity.Citation5 Also, the Dutch population eats more fruit and vegetables, less meat and fewer sugar-containing beverages.Citation6 Furthermore, studies in the United States mentioned the adoption of HbA1c for the diagnosis of diabetes as a possible explanation for the decreasing incidence rate.Citation4 However, in the Netherlands, this was not adopted in the national diabetes guidelines. Finally, improved screening for diabetes has been suggested as an explanation for the slowing epidemic. In the Netherlands, the guidelines for diagnosing and treating diabetes in primary care changed in 2013. They advised screening with fasting plasma glucose every three years in people aged 45 and older with risk factors for developing diabetes.Citation7 In the previous study by our group, we already reported a diminishing proportion of undetected diabetes between 1989 and 2007.Citation8 Therefore, it could well be that, during our study period, the pool of undetected diabetes (ie the denominator for calculating incidence) is diminishing faster than the number of newly diagnosed persons with diabetes (ie the numerator for calculating incidence) and, therefore, the incidence of diabetes is decreasing.
The strengths of this study are the representativeness of the cohort for the Dutch population, covering 16 recent years. Moreover, we used data from primary care physicians who diagnosed diabetes with fasting plasma glucose throughout the total period. In addition, GPs are financially incentivized to record patients with T2D correctly, so few patients with T2D are not registered. Nonetheless, there are several limitations. First, we do not know the proportion of undetected diabetes. However, this proportion likely decreased in the last decade, as shown in previous population studies.Citation8,Citation9 Still, we possibly underestimate diabetes prevalence and incidence because of undetected diabetes. Second, the population included in our study increased over time. However, we are convinced this will not have influenced the accuracy of the results.
To conclude, this study showed an increased prevalence of T2D with a decreased incidence between 2010 and 2020. This result was more explicit at an older age. The results are relevant for clinical practice in the foreseeable future. It demonstrates that preventive strategies, public health education, and awareness campaigns might have decreased incidence.
Data Sharing Statement
Requests for sharing study data must be made on specific grounds, either to corroborate the study results in the interest of Public Health or the context of an audit by a competent authority. Sufficient information needs to be provided to confirm that the request is made for one of the purposes mentioned above, including a wound justification and, in case of a request to corroborate study results, a protocol on the research for which the data will be used or a plan for quality control checks, as applicable.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
JO, KS and RH are PHARMO Institute for Drug Outcomes Research employees. This independent research institute performs financially supported studies for the government, related healthcare authorities, and several pharmaceutical companies. GN, MB and PE declare no conflict of interest.
Acknowledgments
The authors would like to thank all the healthcare providers who are contributing information to the PHARMO Data Network.
Additional information
Funding
References
- Magliano DJ, Islam RM, Barr ELM, et al. Trends in incidence of total or type 2 diabetes: systematic review. BMJ. 2019;366:l5003. doi:10.1136/bmj.l5003
- Kuiper JG, Bakker M, Beest FJA P-V, Herings RMC. Existing data sources for clinical epidemiology: the PHARMO database network. Clin Epidemiol. 2020;12:415–422. doi:10.2147/CLEP.S247575
- Overbeek JA, Swart KMA, Houben E, Beest FJA P-V, Herings RMC. Completeness and representativeness of the PHARMO General Practitioner (GP) data: a comparison with national Statistics. Clin Epidemiol. 2023;15:1501–1511. doi:10.2147/CLEP.S389598
- Geiss LS, Wang J, Cheng YJ, et al. Prevalence and incidence trends for diagnosed diabetes among adults aged 20 to 79 years, United States, 1980–2012. JAMA. 2014;312(12):1218–1226. doi:10.1001/jama.2014.11494
- Statistics Netherlands (CBS). Obesity, smoking and alcohol consumption barely down since 2018; 2022. Available from: https://www.cbs.nl/nl-nl/nieuws/2022/10/overgewicht-roken-en-alcoholgebruik-nauwelijks-gedaald-sinds-2018#:~:text=In%202021%20hadden%20nagenoeg%20evenveel,naar%2021%20procent%20in%202021. Accessed Feb 24, 2023.
- Rijksinstituut voor Volksgezondheid en Milieu (RIVM). Dutch are eating increasingly healthier: more plant-based and less red and processed meat; 2022. Available from: https://www.wateetnederland.nl/conclusies. Accessed Feb 24, 2023.
- Rutten GEHM, De Grauw WJC, Nijpels G, et al. NHG-Standaard Diabetes mellitus type 2 (derde herziening). Huisarts Wet. 2013;56(10):512–525.
- Riet E, Alssema M, Rijkelijkhuizen JM, Kostense PJ, Nijpels G, Dekker JM. Relationship between A1C and glucose levels in the general Dutch population: the new Hoorn study. Diabetes Care. 2010;33(1):61–66. doi:10.2337/dc09-0677
- Mooy JM, Grootenhuis PA, de Vries H, et al. Prevalence and determinants of glucose intolerance in a Dutch caucasian population. the Hoorn study. Diabetes Care. 1995;18(9):1270–1273. doi:10.2337/diacare.18.9.1270