Abstract
Purpose
To assess the effects of topiramate on C-fiber function, nerve fiber morphology, and metabolism (including insulin sensitivity, obesity, and dyslipidemia) in type 2 diabetes.
Patients and methods
We conducted an 18-week, open-label trial treating patients with topiramate. Twenty subjects with type 2 diabetes and neuropathy (61.5 ± 1.29 years; 15 male, 5 female) were enrolled and completed the trial. Neuropathy was evaluated by total neuropathy scores, nerve conduction studies, quantitative sensory tests, laser Doppler skin blood flow, and intraepidermal nerve fibers in skin biopsies.
Results
Topiramate treatment improved symptoms compatible with C-fiber dysfunction. Weight, blood pressure, and hemoglobin A1c also improved. Laser Doppler skin blood flow improved significantly after 12 weeks of treatment, but returned to baseline at 18 weeks. After 18 weeks of treatment there was a significant increase in intraepidermal nerve fiber length at the forearm, thigh, and proximal leg. Intraepidermal nerve fiber density was significantly increased by topiramate in the proximal leg.
Conclusion
This study is the first to demonstrate that it is possible to induce skin intraepidermal nerve fiber regeneration accompanied by enhancement of neurovascular function, translating into improved symptoms as well as sensory nerve function. The simultaneous improvement of selective metabolic indices may play a role in this effect, but this remains to be determined.
Introduction
The leading cause of nontraumatic extremity amputation is complications of diabetes, with over 96,000 amputations per year.Citation1 Neuropathy associated with diabetes predisposes to pain, numbness, ulceration, infection, gangrene, and amputation. Somatic and autonomic diabetic neuropathy contribute to 87% of these amputations.Citation2 It is now appreciated that there are different forms of neuropathy in diabetes.Citation1 Damage occurs to both large, myelinated nerve fibers and small, unmyelinated fibers (C-fibers). The small, unmyelinated C-fibers subserve thermal and pain perception, and the small autonomic fibers affect sweating and vascular control.Citation3 Damage to small, unmyelinated C-fibers has the greatest impact on survival and quality of life, producing initial symptoms such as pain, numbness, and anhidrotic skin with disordered skin blood flow (SKBF) predisposing to foot ulcers, infection, gangrene and limb loss.Citation4 Diabetic peripheral neuropathy is the primary cause of diabetic ulcers and the most predictive diagnosis for an eventual amputation. Current therapies for diabetic peripheral neuropathy are for symptomatic relief of pain and not for the underlying disorder.Citation5–Citation8 Any addition to the therapeutic armamentarium would be welcome.
It has been shown that small fiber neuropathies are quantifiable with newer tests of C-fiber integrity that include quantitative measures of SKBF and corneal confocal microscopy,Citation9–Citation11 quantification of intraepidermal nerve fibers (IENF),Citation12–Citation16 and quantitative sensory testing (QST).Citation17 Heat- induced vasodilation (44°C), is reduced in subjects with impaired glucose tolerance, and in type 2 diabetic patients with and without neuropathy.Citation18
We have reported that one of the earliest quantitative sensory abnormalities found in people with diabetic peripheral neuropathy is the impairment of small fiber sensory perception that cosegregates with disordered neurovascular function.Citation19,Citation20 Furthermore, there is evidence to suggest that one of the early manifestations of C-fiber dysfunction can be based upon skin biopsies, with measurement of the density of thin, unmyelinated nerve fibers using immunohistochemistry for Protein Gene Product 9.5 (PGP-9.5) as a neuronal marker.Citation12,Citation13,Citation15,Citation16,Citation21,Citation22 Since description of the utility of PGP- 9.5 as a marker for IENF in human skin,Citation23 it has been used for identification of small nerve fibers in the dermis and epidermis in a range of small fiber neuropathies, including human immunodeficiency virus, and idiopathic small fiber and postherpetic neuralgia, among others.Citation13,Citation15,Citation24–Citation29 In addition, we have now established that there are characteristic changes in IENF that distinguish the metabolic syndrome from diabetes. Citation30 IENF density was recently given a level A recommendation by the European Federation of the Neurological Societies and the Peripheral Nerve Society as a reliable and efficient technique to confirm the clinical diagnosis of small fiber neuropathy.Citation31 The IENF density has been shown to correlate inversely with cold and heat detection thresholds.Citation32 A oneyear diet and exercise intervention program in patients with small fiber neuropathy and impaired glucose tolerance led to increased IENF density.Citation33 IENF loss is evident early in the disease process, declines with increasing neuropathic pain, and can be used as an outcome measure in clinical trials.Citation31,Citation33 Apart from the one-year trial on diet and exercise,Citation33 no drug has been shown to induce C-fiber regeneration.
Topiramate, a structurally novel antiepileptic drug, is effective in treatment of various types of epilepsy and prevention of migraine headaches. A sulfamate-substituted derivative of d-fructose, topiramate has several pharmacologic properties suggesting it may have potential for overcoming the programmed cell death implicated in the pathogenesis of neuropathy.Citation4 It enhances gamma aminobutyric acid (GABA) activity by interacting with a nonbenzodiazepine site on GABA receptors, has negative modulatory effects on voltage-activated Na+ channels,Citation34 selectively blocks AMPA/kainate glutamate receptors, has negative modulatory effects on L-type high voltage-activated Ca2+ channels,Citation35 and inhibits the carbonic anhydrase isozymes, CA-I and CA-II.Citation34 These multiple mechanisms of action may contribute to its anticonvulsive, antinociceptive, and putative neuroprotective properties. There has been no report on the ability of topiramate to influence the structure and function of IENF, although there are animal studies to suggest that it may exercise these properties.Citation36,Citation37
Topiramate thus clearly offers an advantage over agents currently used for neuropathy in as much as it relieves pain and, in animal studies, is neurotrophic and neuroprotective, and may have beneficial effects on weight, blood pressure, and lipids. The American Diabetes Association and the American Society of Pain have recently added topiramate and other anticonvulsant medications to the diabetic neuropathy treatment regimen.Citation38 There may be an added benefit with topiramate in treating diabetic patients with neuropathy, because it exerts both neurotrophic and metabolic effects that have not been shown by other anticonvulsants.Citation7,Citation8,Citation39
We have reported on pain reduction with topiramateCitation7 which persisted for at least six monthsCitation40 and had salutary effects on weight, blood pressure, and serum lipids. The aim of this study was to determine whether topiramate induces regeneration of small cutaneous nerve fibers in concert with improved SKBF and sensory measures of C-fiber function.
Material and methods
Twenty subjects were recruited and completed the study. The Eastern Virginia Medical School Institutional Review Board approved the study and all subjects gave written informed consent prior to any study procedures. All subjects participating in this study had type 2 diabetes, were aged 35–75 years, and had documented evidence of diabetic peripheral neuropathy. Their baseline demographic and clinical data are shown in . The study was a pure within-subject repeated-measure design comparing skin biopsy data, sensory responses, and SKBF before and after treatment with topiramate in subjects with diabetic peripheral neuropathy. All assessments occurred once prior to treatment and again at the end of the 18-week treatment period. In addition, SKBF testing was performed at week 12. After initial evaluation, all patients received active treatment with topiramate.
Table 1 Baseline clinical and demographic data (n = 20)
Quantitative neuropathy testing
All patients had a complete history, and a physical and neurologic examination. Neurologic symptom scores and neurologic disability scores were generated by completion of a questionnaire modified from Dyck.Citation41 The sum of the three scores (symptom, motor, and sensory scores) is the total neuropathy score. Neuropathy was established by the criteria suggested by the American Diabetes Association and American Academy of Neurology.Citation42 QST included measures of temperature and touch perception thresholds. Quantitative autonomic function was assessed by three tests, ie, heart rate variability during deep breathing at six breaths per minute (E:I ratio), the R:R variation in response to the Valsalva maneuver, and the R:R variation is response to postural change as suggested by the neurologic disability score position statement on neuropathy.Citation38
QST was performed using the Medoc device (TSA2001/VSA3001) following previously published procedures. Touch pressure was measured using graded monofilaments (Semmes–Weinstein).Citation17 Measurements were taken 2 cm proximal to the skin biopsy sites on the nondominant limbs.
Nerve conduction studies were performed on the nondominant peroneal motor, sural sensory, and ulnar motor and sensory nerves, using standard techniques of supramaximal percutaneous nerve stimulation, surface recording, and appropriate filtering and signal amplification. Stimulation-to- recording electrode distances, electrode placement, and limb surface temperatures were defined for each nerve conduction study to ensure that all studies were performed under similar conditions.
Skin blood flow
SKBF was measured by continuous laser Doppler assessment of the response to varying stimuli, as previously described.Citation20,Citation43 Testing was done on the nondominant foot and proximal calf at baseline, after six weeks of maintenance treatment (ie, a total of 12 weeks’ treatment) and at the end of 12 weeks of maintenance treatment. The SKBF and temperature probes were placed over the external aspect of the nondominant leg 10 cm below the knee over the area where the skin biopsy sample was taken and on the dorsum of the foot. SKBF examinations were done with the patient in a reclined position with the legs elevated and completely extended. After a 10-minute baseline period, the temperature was increased to 32°C for 10 minutes, 40°C for 10 minutes, and then to 44°C for 20 minutes.
Skin biopsy
Skin punch biopsies (3 mm) were performed under local anesthesia. Biopsies were collected from each patient’s dorsal forearm, lateral thigh (10 cm proximal to patella), lateral proximal leg (10 cm distal to fibular head), and lateral distal leg (10 cm proximal to lateral malleolus). Tissue samples were immediately fixed in 2% buffered paraformaldehyde/lysine/periodate solution for 12–24 hours at 4°C. They were subsequently cryoprotected in phosphate buffer with 20% glycerol overnight and frozen for later cryosectioning.
Procedures for identifying neurons in skin biopsies employed immunofluorescence techniques in a modification of the protocol described by McCarthy et al.Citation13 The processing and cutting of the slides were done following procedures previously described.Citation30 The skin biopsy data from this cohort of patients was also compared with healthy control patients taken from the large skin biopsy database created and maintained at our institute.
Fasting blood chemistries
Blood samples were obtained at the screening and final visits for determination of glycosylated hemoglobin (HbA1c), lipid profile including total serum cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, free fatty acids, and triglycerides, and fasting serum glucose and C-peptide. We also measured serum B12 and rapid plasma reagin at screening in order to rule out occult neuropathies. In addition, liver enzymes were measured at screening, and at weeks 4, 6, 12, and 18.
Statistical analysis
The primary endpoints were SKBF, QST, and indices of IENF density and length, all of which are continuous (parametric) data. The independent variable was topiramate treatment. Repeated measures analysis of variance was used to examine the treatment effects for SKBF, QST, and skin biopsies. Significant differences were accepted as P < 0.05. Where significant treatment differences were observed, contrast testing was used to determine the significance at each level, while allowing for multiplicity of comparisons. In addition, nonparametric Spearman rank correlations were done to examine the relationship between IENF, SKBF, and measures of neurologic function.
Results
The patients entered into this study were predominantly Caucasian, overweight, male, and hypertensive type 2 diabetics with clinical evidence of distal symmetric polyneuropathy (). Our previous experience prescribing topiramate led us to use a low starting dosage and a slow dosage-escalation protocol. Oral topiramate was administered initially at a dose of 25 mg/day and gradually titrated over six weeks to a dose of 100 mg/day or the maximum tolerated dose. Fifteen of the 20 subjects were able to tolerate 100 mg/day, two subjects were maintained on 75 mg/day, and three were on 50 mg/day. A 12-week maintenance period followed the titration phase. During this period, the dose of study medication remained constant. One of the 20 patients was discontinued from the study early due to cognitive effects of the medication, including psychomotor slowing, word finding difficulty, and fatigue. All other patients tolerated their maximally titrated dose with little cognitive effect.
We have previously reportedCitation16 that mean dendritic length and IENF density progressively decreased from proximal to distal sites in patients with neuropathy. In this cohort of patients, there was a similar decrease in IENF density and mean dendritic length from proximal to distal sites (). Nerve fiber density in skin taken from patients before topiramate treatment was significantly lower than in skin taken from comparable sites in healthy control patients in our large skin biopsy database. Comparing the results at each site, IENF density in the forearm was significantly lower in patients (13.2 ± 3.5) compared with controls (32.9 ± 3.2; P < 0.001). Similar deficits in IENF were seen in the thigh (8.4 ± 5.7 versus 35.6 ± 7.3; P < 0.01), proximal leg (3.1 ± 2.2 versus 17.4 ± 2.0; P < 0.001), and distal leg (4.6 ± 4.6 versus 28.0 ± 3.9; P < 0.001).
Figure 1 A) Mean ± SE dendritic length (Microns) at 4 sites before and after 18 weeks of topiramate treatment. Significant differences (ANOVA) are shown. B) Mean ± SE nerve fiber density (Fibers/mm) in skin at different sites before and after 18 weeks of topiramate treatment. A significant change was only found in proximal leg.
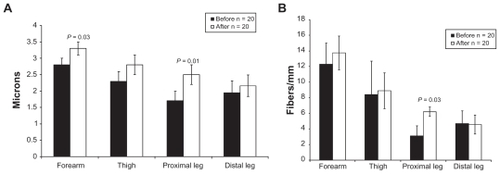
Mean dendritic length of nerve fibers in skin from controls was similar, regardless of site, ie, forearm (3.28 ± 0.18 μm), thigh (3.69 ± 0.3 μm), proximal leg (3.34 ± 0.23 μm), and distal leg (3.31 ± 0.3 μm). There was a progressive shortening of fibers in patients before treatment with topiramate from forearm to distal leg. In addition, mean dendritic length in skin from patients before topiramate treatment was significantly lower than skin taken from comparable sites in control subjects, ie, thigh (2.28 ± 0.23; P < 0.001), proximal leg (1.79 ± 0.26; P < 0.001), and distal leg (1.94 ± 0.35; P < 0.005). Mean dendritic length was not different from controls in the forearm (2.86 ± 0.19; P < 0.05).
Treatment with topiramate significantly increased mean dendritic length in the forearm and proximal leg () and IENF density in the proximal leg (). A representative sample is shown in . This was associated with improvement in total neuropathy scores, including touch, vibration, and prickling pain thresholds, and reduction in weight, body mass index, systolic and diastolic blood pressures, and HbA1c (). SKBF was measured at baseline, 12 weeks, and 18 weeks. A significant increase in SKBF was seen at week 12, but returned to baseline at week 18. SKBF in the leg increased from 87.7 ± 0.1 to 101.3 ± 0.1 (P < 0.001) and in the foot from 102.6 ± 0.2 to 143.7 ± 0.6 (P < 0.001) laser Doppler units at 12 weeks. No correlations were found between the changes in measures of neurologic function, IENF, and the changes in metabolic parameters.
Figure 2 A skin biopsy sample before and after treatment with topiramate shows an increase in the intraepidermal nerve fiber density (epidermis indicated by box at arrow) and dendritic length after treatment.
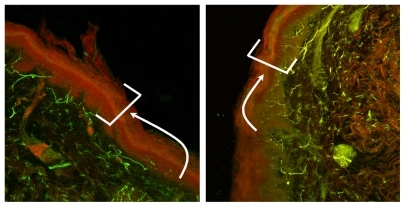
Table 2 Variables with significant changes from baseline to 18 weeks post-initiation of treatment with topiramate
Conclusion
In this small within-subject pilot study, we have shown that 18 weeks of treatment with topiramate induced improvement in neurologic disability scores, including prickling, vibration, and touch perception. This was associated with improvement in SKBF after 12 weeks of treatment, but this returned to baseline at 18 weeks. Quantification of IENF density and mean dendritic length in skin biopsies, carried out at entry into the study and repeated at the same sites after 18 weeks of treatment, showed an increase in nerve fiber length at the forearm and proximal leg after treatment with topiramate, and an increase in nerve fiber density at the proximal leg.
We have previously shownCitation4,Citation44 that the earliest change found in patients with the metabolic syndrome without hyperglycemia is a reduction in mean dendritic length and that the decrease in IENF density occurs after at least five years of diabetes and is most prominent at the distal site.Citation44 Thus, the patients in this study most closely resemble those with diabetes, including those with features of the current definition of the metabolic syndrome ().
There is a distinct clinical entity of neuropathy associated with the metabolic syndrome in the absence of glucose intolerance. However, up to 50% of patients with painful neuropathy may have impaired glucose tolerance.Citation17,Citation45,Citation46 This suggests that treatment of the nonhyperglycemic components of the metabolic syndrome may be important. While we do show an improvement in HbA1c, blood pressure, and weight similar to that reported for topiramate in previous neuropathy studies,Citation7,Citation39 we could not find correlations between changes in nerve fibers or cognitive function and changes in the metabolic parameters.
In this study we showed that 18 weeks of treatment with topiramate improves total neuropathy scores, touch, prickling pain, and vibration perception, as well as IENF. We have reportedCitation16,Citation44 that distal leg IENF density showed significant negative correlations with warm (P < 0.02) and cold (P < 0.05) thermal threshold, heat pain (P < 0.05), pressure sense (P < 0.05), sensory score (P < 0.03), and total neuropathy score (P < 0.03), and thus objective measures are likely to be related. It is not clear, at this point in time, if these changes can be sustained for greater periods. It has been shown that pain improvement persists for at least six months,Citation40 and anecdotally our patients appeared to continue to improve beyond the defined study period. Clearly, longer duration studies are needed to determine if the cross-sectional correlates of nerve fiber densities and mean dendritic length with different sensory modalities can be realized.
We have reported that there is a direct correlation between distal leg IENF density and duration of diabetes,Citation47 suggesting that there is a loss of about one nerve fiber per mm per year. A reduction of one nerve fiber per mm translates into clinically significant changes in total neuropathy scores and objective measures of cognitive function. Furthermore, an improvement in the proximal leg of three nerve fibers per mm was found to provide clinically meaningful changes in objective parameters of nerve function. Therefore, we would propose that a conservative estimate of double the value for change in function, ie, two nerve fibers per mm, could be considered a minimal requirement for success in future studies of agents affecting nerve biology. Furthermore, we have also reported that there is a progressive shortening of the mean dendritic length in the distal leg.Citation47 Since this change occurs in the metabolic syndrome independent of blood glucose,Citation44 it seems that this could be a valuable endpoint in patients being treated for components of the metabolic syndrome other than hyperglycemia. The pattern of regeneration is unique and dictates a need to use IENF length, rather than density, as an endpoint in clinical studies at sites where viable nerve fibers still exist.
Because of the demonstrated effects of topiramate on various metabolic aspects, it could be an important addition to therapies aimed at the metabolic syndrome and its sequelae, including neuropathy and diabetes. Topiramate has been reported to have positive effects on pain relief in diabetic peripheral neuropathy,Citation7 an effect which has been shown to be durableCitation40 in clinical trials for the management of diabetic peripheral neuropathy pain syndromes. In these studies it was noted that weight loss and changes in metabolic parameters accompanied pain relief, but the role of topiramate in disease modification of neuropathy is limited.Citation48 Although the mechanisms underlying the neuroprotective effect of topiramate are not fully understood, there may be added benefits for people with type 2 diabetes. Topiramate inhibits weight gain in animals on a high-fat diet, but the mechanism through which change in energy balance is achieved is unclear.Citation49 Topiramate causes weight lossCitation50 sustained for one year.Citation51 In our studies, treatment with topiramate not only improved symptoms of neuropathy, but also reduced body weight, body mass index, systolic and diastolic blood pressure, and HbA1c. These findings are not unlike those previously reported with topiramate treatment in normal healthy patients, as well as in patients with diabetes.Citation50,Citation51
The caveats, however, are that this was a small open-label trial, with careful attention paid to minimizing the untoward side effects known to occur at higher doses of topiramate. Effects of topiramate on cognitive function, including psychomotor slowing, short-term memory loss, fatigue, and anorexia have been reported with topiramate treatment. These common side effects make it difficult to design a true placebo-controlled trial. In our short study, we found if there was a low starting dose (15 mg), and a slow taper to a low maximum dose of 100 mg, many of these side effects are mitigated. What would be attractive is the discovery of an agent with the beneficial neurologic and metabolic effects of topiramate, but free of cognitive dysfunction and intensive dosing requirements, which would allow a true placebocontrolled trial to be performed.
Disclosure
The authors report no conflicts of interest in this work. This was an inhouse study with no outside funding source.
References
- Vinik A Pittenger G McNitt P Stansberry KB Diabetic neuropathies: An overview of clinical aspects, pathogenesis, and treatment LeRoith D Taylor SI Olefsky JM Diabetes Mellitus: A Fundamental and Clinical Text 2nd ed Philadelphia, PA Lippincott, Williams and Wilkins 2000
- Vinik AI Suwanwalaikorn S Autonomic neuropathy DeFronzo RA Current Therapy of Diabetes Mellitus St Louis MO Mosby 1997
- Vinik AI Erbas T Park TS Methods for evaluation of peripheral neurovascular dysfunction Diabetes Technol Ther 2001 3 29 50 11469707
- Vinik A Pittenger G Anderson A Stansberry K McNear E Barlow P Topiramate improves C-fiber neuropathy and features of the dysmetabolic syndrome in Type 2 diabetes Diabetes 2003 52 Suppl 1 A130
- Goldstein DJ Lu Y Detke MJ Lee TC Iyengar S Duloxetine vs placebo in patients with painful diabetic neuropathy Pain 2005 116 109 118 15927394
- Rosenstock J Tuchman M LaMoreaux L Sharma U Pregabalin for the treatment of painful diabetic peripheral neuropathy: A double-blind, placebo-controlled trial Pain 2004 110 628 638 15288403
- Raskin P Donofrio PD Rosenthal NR Topiramate vs placebo in painful diabetic neuropathy: Analgesic and metabolic effects Neurology 2004 63 865 873 15365138
- Ben Menachem E Axelsen M Johanson EH Stagge A Smith U Predictors of weight loss in adults with topiramate-treated epilepsy Obes Res 2003 11 556 562 12690085
- Mehra S Tavakoli M Kallinikos PA Corneal confocal microscopy detects early nerve regeneration after pancreas transplantation in patients with type 1 diabetes Diabetes Care 2007 30 2608 2612 17623821
- Vinik EJ Hayes RP Oglesby A The development and validation of the Norfolk QOL-DN, a new measure of patients’ perception of the effects of diabetes and diabetic neuropathy Diabetes Technol Ther 2005 7 497 508 15929681
- Stansberry KB Primary nociceptive afferents mediate the blood flow dysfunction in non-glabrous (hairy) skin of type 2 diabetes Diabetes Care 1999 22 1549 1554 10480524
- Griffin JW Hsieh ST McArthur JC Cornblath DR Laboratory testing in peripheral nerve disease Neurol Clin 1996 14 119 133 8676840
- McCarthy BG Hsieh ST Stocks A Cutaneous innervation in sensory neuropathies: Evaluation by skin biopsy Neurology 1995 45 1848 1855 7477980
- Kennedy WR Said G Sensory nerves in skin Neurology 1999 53 1614 1615 10563599
- Periquet MI Novak V Collins MP Painful sensory neuropathy: Prospective evaluation using skin biopsy Neurology 1999 53 1641 1647 10563606
- Pittenger GL Ray M Burcus NI McNulty P Basta B Vinik AI Intraepidermal nerve fibers are indicators of small-fiber neuropathy in both diabetic and nondiabetic patients Diabetes Care 2004 27 1974 1979 15277426
- Vinik AI Suwanwalaikorn S Stansberry KB Holland MT McNitt PM Colen LE Quantitative measurement of cutaneous perception in diabetic neuropathy Muscle Nerve 1995 18 574 584 7753119
- Krishnan ST Rayman G The LDI flare: A novel test of C-fiber function demonstrates early neuropathy in type 2 diabetes Diabetes Care 2004 27 2930 2935 15562209
- Vinik AI Erbas T Park T Stansberry KB Pittenger G Platelet and neurovascular dysfunction in diabetes mellitus Diabetes Care 2001 24 1476 1485 11473089
- Stansberry KB Hill MA Shapiro SA McNitt PM Bhatt BA Vinik AI Impairment of peripheral blood flow responses in diabetes resembles an enhanced aging effect Diabetes Care 1997 20 1711 1716 9353614
- McArthur JC Stocks EA Hauer P Cornblath DR Griffin JW Epidermal nerve fiber density: Normative reference range and diagnostic efficiency Arch Neurol 1998 55 1513 1520 9865794
- Kennedy W Said G Sensory nerves in skin: Answers about painful feet? Neurology 1999 53 1614 1615 10563599
- Dalsgaard CJ Rydh M Haegerstrand A Cutaneous innervation in man visualized with protein gene product 9.5 (PGP 9.5) antibodies Histochemistry 1989 92 385 390 2531128
- Polydefkis M Yiannoutsos CT Cohen BA Reduced intraepidermal nerve fiber density in HIV-associated sensory neuropathy Neurology 2002 58 115 119 11781415
- Holland NR Crawford TO Hauer P Small-fiber sensory neuropathies: Clinical course and neuropathology of idiopathic cases Ann Neurol 1998 44 47 59 9667592
- Petersen KL Rice FL Suess F Berro M Rowbotham MC Relief of post-herpetic neuralgia by surgical removal of painful skin Pain 2002 98 119 126 12098623
- Griffin JW McArthur JC Polydefkis M Assessment of cutaneous innervation by skin biopsies Curr Opin Neurol 2001 14 655 659 11562579
- Kennedy WR Wendelschafer-Crabb G Johnson T Quantitation of epidermal nerves in diabetic neuropathy Neurology 1996 47 1042 1048 8857742
- Chien H Tseng T Lin W Quantitative pathology of cutaneous nerve terminal degeneration in the human skin Acta Neuropathol 2001 102 455 461 11699558
- Pittenger G Mehrabyan A Simmons K Small fiber neuropathy is associated with the metabolic syndrome Metab Syndr Relat Disord 2005 3 113 121 18370718
- Lauria G Lombardi R Skin biopsy: A new tool for diagnosing peripheral neuropathy BMJ 2007 334 1159 1162 17540945
- Shun CT Chang YC Wu HP Skin denervation in type 2 diabetes: Correlations with diabetic duration and functional impairments Brain 2004 127 Pt 7 1593 1605 15128619
- Smith AG Russell J Feldman EL Lifestyle intervention for prediabetic neuropathy Diabetes Care 2006 29 1294 1299 16732011
- Dodgson SJ Shank RP Maryanoff BE Topiramate as an inhibitor of carbonic anhydrase isoenzymes Epilepsia 2000 41 Suppl 1 S35 S39 10768298
- Zhang X Velumian AA Jones OT Carlen PL Modulation of high- voltage-activated calcium channels in dentate granule cells by topiramate Epilepsia 2001 41 Suppl 1 S52 S60 10768302
- Yang Y Shuaib A Muzaffar Q Siddiqui M Neuroprotection by delayed administration of topiramate in a rat model of middle cerebral artery embolization Brain Res 1998 804 169 176 9757028
- Lee SR Kim SP Kim JE Protective effect of topiramate against hippocampal neuronal damage after global ischemia in the gerbils Neurosci Lett 2000 281 183 186 10704773
- Boulton AJ Vinik AI Arezzo JC Diabetic neuropathies: A statement by the American Diabetes Association Diabetes Care 2005 28 956 962 15793206
- Thienel U Neto W Schwabe SK Vijapurkar U Topiramate in painful diabetic polyneuropathy: Findings from three double-blind placebocontrolled trials Acta Neurol Scand 2004 110 221 231 15355485
- Donofrio PD Raskin P Rosenthal NR Safety and effectiveness of topiramate for the management of painful diabetic peripheral neuropathy in an open-label extension study Clin Ther 2005 27 1420 1431 16291415
- Dyck PJ Detection, characterization and staging of polyneuropathy: Assessed in diabetes Muscle Nerve 1988 11 21 32 3277049
- Consensus Statement. Report and recommendations of the San Antonio conference on diabetic neuropathy. American Diabetes Association American Academy of Neurology Diabetes Care 1988 11 592 597 3060328
- Stansberry KB Hill M McNitt PM Bhatt BA Vinik AI Skin blood flow reactivity and neuropathy Diabetes 1994 43 Suppl 1 107A
- Pittenger G Simmons K Anandacoomaraswamy D Rice A Barlow P Vinik A Topiramate improves intraepidermal nerve fiber morphology and quantitative neuropathy measures in diabetic neuropathy patients J Peripher Nerv Syst 2005 10 Suppl 1 73
- Sumner C Sheth S Griffin J Cornblath D Polydefkis M The spectrum of neuropathy in diabetes and impaired glucose tolerance Neurology 2003 60 108 111 12525727
- Smith AG Ramachandran P Tripp S Singleton JR Epidermal nerve innervation in impaired glucose tolerance and diabetes-associated neuropathy Neurology 2001 57 1701 1704 11706115
- Pittenger G Diabetic neuropathy induces N1E-115 neuroblastoma cell apoptosis: protective role of topiramate Grant from RW Johnson Pharmaceutical Research Institute 2004
- Edwards K Glantz MJ Button J Efficacy and safety of topiramate in the treatment of painful diabetic neuropathy: A double-blind, placebocontrolled study Neurology 2000 54 Suppl 3 A81
- York DA Singer L Thomas S Bray GA Effect of topiramate on body weight and body composition of Osborne-Mendel rats fed a high-fat diet: Alterations in hormones, neuropeptide, and uncoupling-protein mRNAs Nutrition 2000 16 967 975 11054603
- Li Z Maglione M Tu W Meta-analysis: Pharmacologic treatment of obesity Ann Intern Med 2005 142 532 546 15809465
- Astrup A Toubro S Topiramate: A new potential pharmacological treatment for obesity Obes Res 2004 12 Suppl S167 S173