Abstract
Glucagon-like peptide-1 (GLP-1) is a hormone secreted from enteroendocrine L cells of the intestine in response to food. Exogenous GLP-1 administration at pharmacological doses results in many effects that are beneficial for treating type 2 diabetes, these include: (1) an increase in insulin secretion from β cells; (2) a suppression of glucagon secretion from α cells in the presence of hyperglycemia but not hypoglycemia; (3) a delay in gastric emptying and gut motility which in turns delays absorption of ingested nutrients and dampens post-prandial glucose excursion; and (4) an increase in the duration of postprandial satiety therefore suppressing appetite and decreasing food intake which eventually leads to weight loss. However, GLP-1 is subject to rapid enzymatic degradation, and therefore, not suitable for long-term treatment. A synthetic enzyme-resistant GLP-1 receptor agonist that reproduces the biological effects of GLP-1 is in use and more are under development. This review aims at providing a summary of the properties of GLP-1 and the development of GLP-1-based therapies for treatment of diabetes.
Keywords:
Introduction
What are incretins?
The incretin effect describes the augmentation in insulin secretion that occurs in response to oral glucose compared to intravenous glucose.Citation1–Citation3 Incretins, therefore by definition, are gut-derived factors that stimulate insulin secretion from β cells after eating. The two hormones that fulfill criteria as incretins are glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1).
GIP is a 42-amino acid peptide synthesized and released from enteroendocrine K cells mostly located in the duodenum and upper jejunum.Citation4 GLP-1, a product of the proglucagon gene, exists in two bioactive forms, GLP-1 (7–36) amide and GLP-1 (7–37), with GLP-1 (7–36) comprising up to 80% of the GLP-1 in circulation.Citation5 It is released from enteroendocrine L cells dispersed throughout the gastrointestinal tract.Citation6,Citation7 Together, the insulinotropic effect of GLP-1 and GIP accounts for up to 60% of the insulin secreted after a meal in healthy humans and plays a very important role in postprandial glucose homeostasis.Citation8
In patients with type 2 diabetes mellitus (T2DM), the ability of exogenous GIP and GLP-1 to stimulate insulin secretion is diminished by 54% and 29%, respectively, when compared to healthy subjects. However, the glucose lowering effect of GLP-1 is relatively preserved while that of GIP is absent.Citation9–Citation11 Therefore, development of therapeutic strategies for T2DM has focused on GLP-1 and not GIP.
Physiology of GLP-1
Fat and carbohydrate-rich meals are the primary physiological stimuli to GLP-1 secretion from enteroendocrine cells.Citation12 Recently, artificial sweeteners, such as sucralose, have also been shown to induce GLP-1 secretion from L cells.Citation13 Although GLP-1 has been found in taste buds and brain tissues, the majority of the GLP-1 measured in peripheral blood is synthesized in L cells.Citation7
In healthy subjects, fasting levels of plasma GLP-1 range from 5–10 pmol/L and increase by two- to three-fold after meal ingestion.Citation14 GLP-1 levels peak about 20 min after oral glucose administration and about 60 to 90 min after mixed meal ingestion, and the levels gradually decline toward fasting levels thereafter.Citation15,Citation16 GLP-1 stimulates insulin secretion in a glucose concentration dependent manner; its insulinotropic effect is lost at plasma glucose concentration below 4.3 mmol/L (77 mg/dL).Citation17
In earlier studies, patients with long-standing T2DM and poor glycemic control (HbA1c ~9.2%) were noted to have deficient GLP-1 secretion.Citation18,Citation19 Recent studies have shown that GLP-1 levels are similar among subjects with mild T2DM (HbA1c ~6.8%), impaired glucose tolerance, and normal glucose tolerance.Citation15,Citation16 Therefore, GLP-1 secretion in patients with T2DM appears to depend on their glycemic status, their medication intake, and other hormonal and metabolic abnormalities associated with worsening glycemic control.Citation16
GLP-1 has a short half-life of 2 min because it is rapidly degraded by dipeptidyl peptidase 4 (DPP 4) and neutral endopeptidase (NEP) 24.11.Citation20–Citation22 DPP 4 cleaves the N-terminal dipeptides (HisCitation7–AlaCitation8) from GLP-1 (7–36) and renders the resulting major metabolite GLP-1 (9–36) insulinotropically inactive.Citation20,Citation23 NEP 24.11, a membrane-bound zinc metallopeptidase, also degrades GLP-1 at potentially six cleavage sites.Citation21 High levels of NEP 24.11 are found in the kidney, and GLP-1 and its metabolites are rapidly cleared through the kidneys.Citation24
The action of GLP-1 is mediated through the glucagon-like peptide-1 receptor (GLP-1R), a seven-member trans-membrane G protein-coupled receptor.Citation25 GLP-1R is expressed in a variety of tissues including pancreatic β cells, hypothalamus, hippocampus, area postrema and various other parts of the brain, as well as stomach, heart, intestine, and kidney.Citation26
GLP-1-based therapy in T2DM
Regardless of the post-prandial levels of GLP-1 in T2DM, the insulin response to GLP-1 is still defective. The response of β cells to exogenously administered GLP-1 was noted to be three to five times lower in patients with T2DM when compared to healthy subjects.Citation11,Citation27 Despite the diminished response of β cells to exogenous GLP-1, overnight intravenous infusion of GLP-1 in patients with T2DM was able to lower fasting and post-prandial plasma glucose to near-normal levels, to improve β-cell function, and to restore first-phase insulin secretion.Citation28
To examine the effect of long-term GLP-1 treatment in patients with T2DM, continuous subcutaneous GLP-1 infusion was given for six and 12 weeks using an infusion pump in two separate studies.Citation29–Citation31 Both studies showed that GLP-1 infusion clearly improved β-cell function and improved insulin sensitivity. A subset of subjects in the 12-week infusion study had frequent blood sampling performed after six weeks of therapy and the results showed significant improvement in insulin pulse mass and pulsatile insulin secretion.Citation31
Exogenous GLP-1 administration at pharmacological doses also has several noninsulinotropic effects that are beneficial for treating T2DM. With exogenous GLP-1, glucagon secretion from α cells was suppressed in the presence of hyperglycemia and euglycemia but not hypoglycemia. The suppression of glucagon leads to improved hepatic insulin resistance and glycemic control in T2DM.Citation17,Citation32 Exogenous GLP-1 also delays gastric emptying and gut motility and these effects slow absorption of ingested nutrients and dampen post-prandial glucose excursion in patients with T2DM.Citation33 Exogenous GLP-1 also increases the duration of postprandial satiety, decreases energy intake and suppresses appetite; leading to less food being eaten and eventually weight loss in most people.Citation29,Citation34,Citation35
Most hypoglycemic agents work by either attempting to increase insulin secretion from β cells (sulfonylureas, meglitinides) or increasing peripheral insulin sensitivity (biguanides, thiazolidinediones). None of them actually targets the root cause of T2DM; deteriorating β-cell function and mass. In addition to stimulating insulin secretion and suppressing glucagon secretion, GLP-1 has other pleiotropic effects in the pancreas. Animal studies have suggested that chronic exogenous GLP-1 administration has the ability to increase islet size, enhance β-cell proliferation, inhibit β-cell apoptosis, and regulate islet growth.Citation36,Citation37 These trophic effects on β cells have not been tested in humans as there is no direct in vivo measure of human β-cell mass available.
Using indirect measures of β-cell function, one study showed that short-term (12 hours) GLP-1 infusion improved the ability of β cells to sense and respond to glucose in patients with impaired glucose tolerance.Citation38 Overnight GLP-1 infusion also improved first- and second-phase insulin secretion in patients with T2DM.Citation28 Six-week infusion of GLP-1 in patients with T2DM showed improvement in insulin sensitivity and β-cell function as measured by glucose utilization and first- and second-phase C-peptide response during hyperinsulinemic euglycemic clamp.Citation29 If the trophic effects seen in rodents are indeed present in humans, treatment with GLP-1 will have tremendous implications in the field of T2DM as it directly addresses one of the fundamental defects in T2DM, that is, β-cell failure.
Collectively, the biological effects of exogenous GLP-1 – increasing insulin secretion from β cells, suppressing glucagon secretion from α cells, decreasing post-prandial glucose excursion through delay in gastric emptying, increasing post-prandial satiety, and possibly enhancing the trophic effects on human β cells – make GLP-1 receptor-based therapy a highly desirable treatment option for T2DM. However, the short half-life of GLP-1 (2 min) renders the native GLP-1 peptide impractical for clinical use. Two obvious options for GLP-1 receptor-based therapies are: (1) GLP-1 analogs with longer half-lives and full efficacy at the GLP-1 receptor (GLP-1R agonists); and (2) agents such as DPP 4 inhibitors that can increase plasma levels of endogenous GLP-1. In this review, we will focus on the GLP-1R agonists. So far, no headway has been made on developing drugs to specifically increase endogenous secretion of GLP-1, though a drug in common use for T2DM, metformin, does cause about a two-fold increase in GLP-1 secretion.Citation39
GLP-1 R agonists
As mentioned earlier, GLP-1 has a half-life of only about 2 min because it is rapidly degraded by DPP 4 and NEP 24.11. To develop GLP-1R agonists with longer half-lives, various modifications of GLP-1 at HisCitation7, AlaCitation8, or GluCitation9 have been attempted so as to prevent DPP 4 from cleaving the first two N-terminal amino acids (HisCitation7, AlaCitation8) of native GLP-1.Citation40 Additional mid-chain modifications of the GLP-1 peptide to prevent hydrolysis by NEP 24.11 are also being studied. Other technologies that allow gradual drug delivery at a controlled rate are also being investigated. This review will summarize the GLP-1R agonists that have clinical efficacy data published in peer-reviewed journals and presented at major scientific meetings.
Exenatide
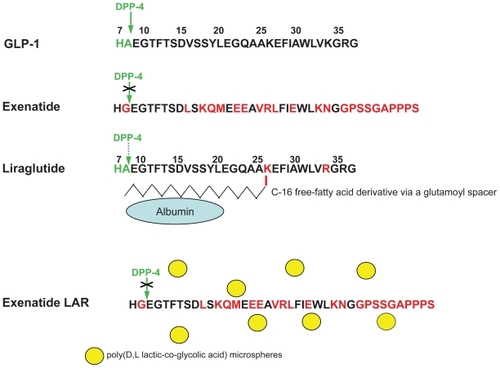
Exenatide (synthetic exendin-4) is the only GLP-1R agonist currently approved by regulatory agencies as an adjunct therapy for patients with T2DM who are not achieving satisfactory glycemic control using other hypoglycemic agents. Exendin-4 is a 39-amino acid peptide produced in the salivary glands of the Gila monster (Heloderma suspectum) (). It has 53% amino acid homology to full-length GLP-1 and binds more avidly than GLP-1 to the GLP-1R.Citation25 There appears to be no specific exendin-4 receptor; the effects of exendin-4 are expressed through the known GLP-1 receptor. Exendin-4 has a GlyCitation8 in place of an AlaCitation8 of the N-terminus, and therefore, is not a substrate for DPP 4. In addition, it lacks some of the target bonds for NEP 24.11, and its secondary and tertiary structures may also prevent NEP 24.11 hydrolysis, thus leading to a prolonged half-life.
Figure 1 Structures of native GLP-1, exenatide, and liraglutide. The N-terminal dipeptide “HA” (in green letters) of GLP-1 and liraglutide is the proteolytic cleavage site for DPP 4. Red letters indicate changes introduced in derivatives or occur naturally in exendin-4 (and replicated in the synthetic version, exenatide). A crossed-out green arrow indicates absent DPP 4 activity, and a dotted green arrow indicates reduced DPP 4 activity. Exenatide long-acting release (LAR) is formulated with exenatide and poly(D,L lactic-co-glycolic acid) microspheres (yellow circles), biodegradable medical polymers commonly used in extended drug release formulation.
Pharmacology
Since exenatide is a peptide, it must be administered subcutaneously. After its subcutaneous administration, exenatide reaches a maximum plasma concentration in 2.1 hr, and the mean half-life ranges from 3.3 to 4 hrs.Citation41 It can be detected for up to 15 hrs in the plasma after subcutaneous injection and its biological effect remains up to at least 8 hrs after dosing.Citation41 In a nonclinical study, it was shown to be eliminated by the kidneys through glomerular filtration.Citation42
Efficacy studies
Three randomized, placebo-controlled, double or triple-blind, 30-week clinical trials examined the efficacy of exenatide in subjects with T2DM not achieving adequate glycemic control on metformin and/or sulfonylurea ().Citation43–Citation45 Patients were randomized to placebo, exenatide 5 μg twice daily, or 10 μg twice daily as adjuvant treatment to sulfonylurea, metformin, or sulfonylurea/metformin. In all three studies, exenatide significantly reduced HbA1c in the treatment groups with exenatide 10 μg twice daily lowered HbA1c by 0.8%–0.9%; exenatide 5 μg twice daily lowered HbA1c by 0.4%–0.6%; while placebo increased HbA1c by 0.1%–0.2%. In the metformin/exenatide10 μg twice daily treatment arm, 41% of patients achieved HbA1c ≤ 7% and a mean weight loss of 2.8 kg. In the sulfonylurea/exenatide 10 μg twice daily treatment arm, 41% of patients achieved HbA1c of ≤ 7% and a mean weight loss of 1.6 kg. In the metformin/sulfonylurea/exenatide 10 μg twice daily treatment arm, 34% of patients achieved HbA1c of ≤ 7% and a mean weight loss of 1.6 kg.
Table 1 Clinical studies with exenatide
The above three trials and their open-label extensions were folded into one open-ended, open label trial.Citation46 Results from this three-year follow-up study showed that after treating with exenatide 10 μg twice daily, the 1.0% reduction in HgbA1c was sustained; 46% of the patients maintained a HbA1c of ≤ 7%; and progressive weight loss was noted with a net-loss of 5.3 kg at the end of three years ().Citation46
The efficacy of exenatide (10 μg twice daily) added to rosiglitazone (≥4 mg/day) alone or pioglitazone (≥30 mg/day) alone, or in combination with metformin was examined in a randomized, double-blind, placebo-controlled trial for 16 weeks (). When compared to placebo, addition of exenatide to thiazolidinediones (TZD) in the presence or absence of metformin reduced HbA1c by 0.9%, mean fasting plasma glucose by 1.6 mmol/L, and body weight by 1.8 kg. However, only 71% of subjects given exenatide as compared with 86% of subjects in the placebo group completed the study where many (14%) discontinued the study because of gastrointestinal symptoms from exenatide.Citation47
Exenatide therapy was also compared to insulin therapy as add-on to oral hypoglycemic agents. In a 26-week multicenter, open-label, randomized, controlled trial, subjects with T2DM whose glycemia was not adequately controlled by metformin and/or sulfonylurea were randomized to either adding exenatide 10 μg twice daily or insulin glargine daily (titrating to fasting blood glucose of <5.6 mmol/L). At the end of 26 weeks, both groups achieved similar improvement in glycemic control (1.1% reduction in HbA1c). However, the exenatide group had better post-prandial glucose control while the glargine group had lower fasting plasma glucose levels. An average weight loss of 2.3 kg was noted with exenatide, and an average weight gain of 1.8 kg was noted with glargine. The drop out rate was 19.4% with exenatide (6% due to nausea) and 9.7% with glargine.Citation48
Exenatide was also compared to biphasic insulin aspart (30% rapid-acting insulin aspart) in a 52-week, randomized, open-label trial in patients with T2DM whose glycemia was not optimally controlled with metformin and sulfonylurea.Citation49 The efficacy of exenatide was comparable to biphasic insulin aspart with similar reduction in HbA1c (1% versus 0.9%) and comparable reduction in fasting plasma glucose (1.8 versus 1.7 mmol/L). The exenatide group had weight reduction of 2.5 kg while the biphasic insulin group had a weight increase of 2.9 kg.
In a 24-week, randomized, double-blind, placebo-controlled, parallel-group study, patients with T2DM naïve to hypoglycemic agents and not optimally controlled with diet and exercise, were randomized to exenatide 5 μg twice daily, exenatide 10 μg twice daily, or placebo twice daily. Significant reductions in HbA1c of 0.7% and 0.9% were noted in the exenatide 5 μg and 10 μg twice daily groups, respectively, compared to reduction of 0.2% in the placebo group. A similar significant reduction in fasting serum glucose of 1.0 mmol/L was noted in the exenatide 5 μg and 10 μg twice daily groups, respectively, compared to a reduction of 0.3 mmol/L in the placebo group. Significant reduction in weight was also observed in the exenatide 5 μg and 10 μg twice daily groups; 2.8 kg and 3.1 kg, respectively, compared to 1.4 kg reduction in the placebo group.Citation50 The indication of using exenatide as monotherapy is currently under review by the United States Food and Drug Administration (FDA).Citation51
Safety and tolerability
A meta-analysis based on randomized controlled trials was conducted to evaluate the safety and efficacy of incretin therapy in T2DM.Citation52 The results from this analysis showed that the most common side effects of exenatide were nausea (57%) and vomiting (17%). The amount of nausea and vomiting was dose-dependent, usually mild to moderate in nature, lessened with dose titration, and most common during the initial weeks of therapy with a decline thereafter. Overall, 4% of patients withdrew from the studies because of gastrointestinal side effects.Citation52 In addition, severe hypoglycemia associated with exenatide use was rare, reported in only five of 2781 patients in which all five patients also received a sulfonylurea. Mild to moderate hypoglycemia was noted in 16% of patients treated with exenatide versus 7% treated with placebo, and was again mostly occurred during co-administration with a sulfonylurea. Anti-exenatide antibodies were detected in 41%–49% of patients in the treatment arms but were not associated with glycemic control.Citation43–Citation45
The most serious (but rare) potential adverse event of exenatide is pancreatitis. In May 2008, the United Kingdom Medicines and Healthcare Products Regulatory Agency (MHRA) noted 89 post-marketing cases of pancreatitis with 87 of them occurring in the United States.Citation53 In August 2008, the United States FDA reported six cases of hemorrhagic or necrotizing pancreatitis in exenatide-treated patients, and two of these patients died. In the exenatide clinical trials, the incident rate of pancreatitis was 1.79/1000 subject years for exenatide-treated patients, 1.35 for insulin comparator group, and 2.72 for placebo-treated patients.Citation53 The company that markets exenatide also tabulated incident data for pancreatitis in patients with T2DM (from insurance claims database) and noted a three- to four-fold greater incidence of acute pancreatitis in subjects with T2DM compared to patients without diabetes.Citation53 While no definite relationship has been established between exenatide and pancreatitis, the FDA has requested that information about acute pancreatitis be included in the precautions section.Citation53
Exenatide and human β-cell function
Similar to GLP-1, short-term infusion of exenatide (5 hrs) has been shown to improve first- and second-phase insulin secretion in patients with T2DM.Citation54 Thirty weeks of exenatide use also resulted in improved β-cell function based on mathematical modeling of β cell in response to test meal in patients with T2DM who were treated with metformin and/or sulfonylurea.Citation55 Furthermore, when compared to insulin glargine, exenatide treatment for 52 weeks significantly improved β-cell function as assessed by arginine-stimulated hyperglycemic clamp, and the β-cell function reverted to pre-treatment levels after discontinuation of exenatide therapy.Citation56
Liraglutide
Liraglutide is a GLP-1 analog with two modifications: a substitution of ArgCitation34 for LysCitation34 and an attachment of a C-16 free-fatty acid derivative via a glutamoyl spacer to LysCitation26 (). The free-fatty acid derivative is thought to promote noncovalent binding of liraglutide to albumin; therefore, the absorption rate of liraglutide is delayed from the injection site and the rate of renal clearance of liraglutide is also slowed.Citation57
Pharmacology
Like GLP-1 and exenatide, liraglutide must be injected subcutaneously. Peak plasma concentrations are detected 10–14 hrs after injection, and the half-life is about 11–13 hrs.Citation58,Citation59
Efficacy studies
The LEAD® programme (Liraglutide Effect and Action in Diabetes) is the Phase 3 clinical trial of liraglutide involving five randomized, controlled, double-blind studies that included about 4,000 patients with T2DM. Results from two of the studies have recently been published in peer-reviewed journals and the results from two other studies have been presented at a scientific meeting.
The LEAD-3 Mono study is a double-blind, double-dummy, active-controlled, parallel-group study in which 746 patients with T2DM (previously treated with diet or oral hypoglycemic agent monotherapy) were randomized to receive liraglutide 1.2 mg, liraglutide 1.8 mg, or glimepiride 8mg once daily ().Citation60 Patients on oral hypoglycemic agent monotherapy had their treatment discontinued at randomization. At the end of 52 weeks, a significant reduction in HbA1c was observed in all groups: 0.5% with glimepiride, 0.8% with liraglutide 1.2 mg, and 1.1% with liraglutide 1.8 mg. Significant reduction in fasting plasma glucose was also observed with an average reduction of 0.3 mmol/L, 0.8 mmol/L, and 1.4 mmol/L in the glimepiride 8 mg, liraglutide 1.2 mg, and liraglutide 1.8 mg groups, respectively. Furthermore, the percentage of patients who achieved a HbA1c of less than 7% was 28%, 43%, and 51% in the glimepiride 8 mg, liraglutide 1.2 mg, and liraglutide 1.8mg groups, respectively. Patients on liraglutide also lost weight of about 1.9 kg and 2.3 kg in the liraglutide 1.2 mg and 1.8 mg groups, respectively, while those on glimepiride 8 mg gained about 1.2 kg.Citation60
Table 2 Clinical studies with liraglutide
The LEAD-2 study is a 26-week, double-blind, doubledummy, placebo- and active-controlled, parallel-group clinical trial in which 1091 patients with T2DM were randomized to liraglutide once daily (either 0.6 mg, 1.2 mg, or 1.8 mg), glimepiride 4 mg once daily, or placebo, all in combination with metformin (1 gm twice daily) ().Citation61 All other oral hypoglycemic agents were discontinued at randomization. After 26 weeks, HbA1c was reduced by 1.0% in the liraglutide 1.2 mg/metformin, the liraglutide 1.8 mg/metformin, and the glimepiride/metformin groups; decreased by 0.7% in the liraglutide 0.6 mg/metformin group; and increased by 0.1% in the placebo/metformin group. The percentage of participants who achieved HbA1c of less than 7% was 28%, 35%, and 42% for the liraglutide/metformin groups (0.6 mg, 1.2 mg, 1.8 mg, respectively), 36% for the glimepiride/metformin group, and 11% for the placebo/metformin group. Fasting plasma glucose was decreased by 1.1 mmol/L, 1.6 mmol/L, 1.7 mmol/L in the liraglutide/metformin groups (0.6, 1.2, and 1.8 mg of liraglutide, respectively) compared to a reduction of 1.3 mmol/L in the glimepiride/metformin group and an increase of 0.4 mmol/L in the placebo/metformin group. Weight loss was also noted in the liraglutide/metformin groups in a dose-dependent fashion; weight reduction of 1.8 kg, 2.6 kg, and 2.8 kg for the liraglutide/metformin groups (liraglutide 0.6 mg, 1.2 mg, and 1.8 mg, respectively), which was significantly greater than the 1.5 kg weight loss noted in the placebo/metformin group. The glimepiride/metformin group had a 1.0 kg weight gain.Citation61
In another 26-week, randomized, double-dummy, placebo-controlled study, 1041 subjects were randomized to five different arms: liraglutide (0.6 mg, 1.2 mg, or 1.8 mg) once daily added to glimepiride once daily, placebo/glimepiride 2–4 mg daily, or rosiglitazone 4 mg/glimepiride combination once daily ().Citation62 HbA1c reduction of 0.6%, 1.1%, and 1.1%, were seen in the liraglutide (0.6 mg, 1.2 mg, 1.8 mg)/glimepiride groups, respectively. An HbA1c reduction of 0.4% was noted in the rosiglitazone/glimepiride group, and a 0.2% HbA1c increase was noted in the placebo/glimepiride group. The percentage of participants who achieved HbA1c of less than 7% was 24%, 35%, and 42% in the liraglutide (0.6 mg, 1.2 mg, and 1.8 mg)/glimepiride groups, respectively, 8% in the placebo/glimepiride group, and 22% in the rosiglitazone/glimepiride group. Weight gain of 0.7 kg, 0.3 kg, and 2.1 kg was noted in the liraglutide 0.6 mg/glimepiride, liraglutide 1.2 mg/glimepiride, and the rosiglitazone/glimepiride groups, respectively, while a weight reduction of 0.2 kg and 0.1 kg was noted in the liraglutide 1.8 mg/glimepiride group and the placebo/glimepiride group, respectively. Fasting plasma glucose was reduced by 0.7 mmol/L, 1.6 mmol/L, 1.6 mmol/L in the liraglutide (0.6 mg, 1.2 mg, 1.8 mg)/glimepiride groups, respectively, reduced by 0.9 mmol/L in the rosiglitazone/glimepiride group, and increased by 1.0 mmol/L in the placebo/glimepiride group.Citation62
In another 26-week randomized clinical trial, 581 subjects with T2DM were randomized to 1.8 mg liraglutide, placebo, or insulin glargine (open label) once daily as add-on to metformin 1 gm twice daily plus glimepiride 2–4 mg once daily ().Citation63 HbA1c reduction of 1.3%, 0.2%, and 1.1% was noted in the liraglutide/metformin/glimepiride, placebo/metformin/glimepiride, and glargine/metformin/glimepiride groups, respectively. Fasting plasma glucose reduction of 1.6 mmol/L and 1.8 mmol/L were noted in the liraglutide/metformin/glimepiride and glargine/metformin/glimepiride groups while an increased of 0.5 mmol/L was noted in the placebo/metformin/glimepiride group. Furthermore, weight reduction of 1.8 kg, 0.4 kg was noted in the liraglutide/metformin/glimepiride and placebo/metformin/glimepiride groups, and weight increased of 1.6 kg was reported in the glargine/metformin/glimepiride group. The percentage of subjects who achieved HbA1c of less than 6.5% was 37%, 11%, and 24% in the liraglutide/metformin/glimepiride, placebo/metformin/glimepiride, and glargine/metformin/glimepiride groups, respectively.Citation63
Safety and tolerability
Similar to exenatide, the most frequently report adverse events for liraglutide were nausea and vomiting, especially at the higher doses.Citation52 In the LEAD-2 study, hypoglycemia was noted in 3% of the liraglutide/metformin and placebo/metformin groups compared to 17% in the glimepiride/metformin group. Nausea was reported to occur in 11%–19% of the liraglutide/metformin groups in a dose-dependent fashion compared to 3%–4% in the placebo/metformin and glimepiride/metformin groups. Nausea was noted to decrease over the duration of the study. There were two cases of pancreatitis reported, one in the liraglutide 1.2 mg group and one in the glimepiride group, and both recovered.Citation61 In the LEAD-3 study, 12% and 8% of the liraglutide groups (1.2 mg and 1.8 mg, respectively) versus 24% of the glimepiride group suffered mild hypoglycemia. Nausea was reported in 28% and 29% of the subjects in the liraglutide groups (1.2 mg and 1.8 mg, respectively), and 9% of the glimepiride group. Again, the incidence of nausea decreased over time. Two participants, one each in the 1.2 mg and 1.8 mg liraglutide groups, developed pancreatitis during the study and both recovered.Citation60 In one of the 26-week studies, 9%–13% of the liraglutide treated subjects developed antibodies to liraglutide. Nausea was reported in 5%–11% of the liraglutide/glimepiride groups, 2% of the placebo/glimepiride group, and 3% of the rosiglitzaone/glimepiride.Citation62 In another 26-week study, 10% of the subjects in the liraglutide group developed liraglutide antibodies.Citation63 Nausea was reported in 14%, 4%, and 1% of the subjects in the liraglutide/metformin/glimepiride, placebo/metformin/glimepiride, and glargine/metformin/glimepiride groups.Citation63 Hypoglycemia was reported in 27%, 17%, and 29% of the subjects in the liraglutide/metformin/glimepiride, placebo/metformin/glimepiride, and glargine/metformin/glimepiride groups.Citation63
Liraglutide and human β cell function
In patients with T2DM, a single dose of liraglutide was able to improve β-cell sensitivity to glucose.Citation64 Two different studies have demonstrated that treatment of patients with T2DM with liraglutide for seven days improved β-cell function as assessed by a model using multiple-meal tests, arginine stimulation test, and hyperglycemic clamp.Citation65,Citation66
Exenatide long-acting release (LAR)
Exenatide LAR is formulated with exenatide and poly (D,L lactic-co-glycolic acid) microspheres, a biodegradable medical polymer commonly used in extended drug release formulation.Citation67 Once weekly subcutaneous injection is thought to be the desired frequency, and it is currently undergoing phase 3 clinical trials.
Pharmacology
With a weekly injection of 2 mg exenatide LAR, a therapeutic plasma level of 50 pg/mL was reached after the second injection. The steady state concentration of exenatide LAR (232 pg/mL) was reached by week 6. This level is similar to the peak level reached by a single injection of 10 μg of exenatide. After 15 weeks of treatment with exenatide LAR, no more injections were given, and its concentration gradually decreased to below therapeutic level by week 21.Citation68
Efficacy studies
In a randomized, placebo-controlled, phase 2 study, 45 patients with T2DM sub-optimally controlled by metformin and/or diet and exercise were randomized to exenatide LAR 0.8 mg, exenatide LAR 2.0 mg, or placebo LAR once weekly for 15 weeks ().Citation68 Subjects who were on metformin continued at the same dose. Exenatide LAR reduced HbA1c by 1.4% and 1.7% in the exenatide LAR 0.8 mg and 2.0 mg groups, respectively, compared to an increase of 0.4% in the placebo group. The percentage of subjects who achieved HbA1c of less than 7% was 36% and 86% for the exenatide LAR 0.8 mg and 2.0 mg groups, respectively, and no change in HbA1c was noted for the placebo group. Fasting plasma glucose was reduced by 2.4 mmol/L and 2.2 mmol/L in the exenatide LAR 0.8 mg and 2.0 mg groups, respectively, compared to an increase of 1.0 mmol/L in the placebo group. Subjects in the exenatide LAR 2.0 mg group lost an average weight of 3.8 kg while those in the exenatide LAR 0.8 mg and placebo groups did not have any change in weight.Citation68
Table 3 Clinical studies with exenatide LAR
In a 30-week, randomized, open-label, comparator-controlled, noninferiority study, exenatide LAR 2mg once weekly was compared to exenatide 10 μg twice daily in 295 patients with T2DM treated by diet, metformin, sulfonylurea, thiazolidinedione, or any combination of the two agents ().Citation67 Patients on exenatide LAR has HbA1c reduction of 1.9% compared to 1.5% reduction in the exenatide twice daily group. Furthermore, 77% of the subjects in the exenatide LAR group achieved HbA1c of less than 7% compared to 61% of the exenatide twice daily group. Weight reduction was comparable in that subjects in the exenatide LAR group lost 3.7 kg while subjects given exenatide twice daily lost 3.6 kg of weight. Fasting plasma glucose was also significantly reduced by 2.3 mmol/L in the exenatide LAR group compared to 1.4 mmol/L in the exenatide twice daily group. Fasting plasma glucagon levels were also significantly lower in the exenatide LAR-treated group compared to the placebo group.Citation67
Safety and tolerability
In the phase 2 study, 19% and 27% of the exenatide LAR 0.8 mg and 2.0 mg groups, respectively, experienced nausea compared to 15% in the placebo group.Citation68 Twenty-five percent of the subjects in the exenatide LAR 0.8 mg group experienced hypoglycemia with only one case confirmed by blood glucose concentration (3.1 mmol/L), while the exenatide LAR 2.0 mg and placebo groups did not report any hypoglycemia.Citation68 Sixty-seven percent of the subjects in the exenatide LAR groups developed positive anti-exenatide antibodies after 15 weeks.Citation68 In the 30-week randomized trial, anti-exenatide antibody levels were higher with exenatide LAR versus the exenatide twice daily group.Citation67 The antibody titers seems to declined progressively after 16 weeks of treatment.Citation67 Nausea was reported in 26% of the exenatide LAR group compared to 35% of the exenatide twice daily group, while vomiting was reported in 11% of the exenatide LAR group compared to 19% of the exenatide twice daily group. Injection site pruritus was also much more frequent (18%) in the exenatide LAR group compared to the exenatide twice daily group (1%).Citation67 No cases of pancreatitis were reported in either of the studies involving exenatide and exenatide LAR.Citation67
Other GLP-1R agonists under development
There are other GLP-1R agonists currently under clinical development that are anticipated to have longer half-lives and presumably less gastrointestinal side effects. LY2189265 is a GLP-1 analog-Fc fusion protein, and LY2428757 is a pegylated GLP-1 analog, both can be administered just once weekly.Citation69 CJC-1134-PC is a recombinant human serum albumin-exendin-4 conjugated protein that has a half-life of approximately eight days and Albiglutide is an albumin-GLP-1 protein complex, both can be administered once weekly.Citation70–Citation72 NN9535 is another long-acting human GLP-1 analog designed for once weekly injection using protein-acylation technology.Citation73 Taspoglutide and AVE0010 are two other GLP-1R agonists currently undergoing clinical trials.Citation74,Citation75 An oral formulation of a GLP-1R agonist is reportedly also under development.Citation76 The compounds mentioned here are just a few representations of the GLP-1R agonists under clinical development, and are by no means comprehensive. Few data are publically available regarding these compounds.
Conclusions
GLP-1R agonists are a new class of hypoglycemic agents that have generated a lot of interests in the field of diabetes. The development of GLP-1R agonists started with their potential as insulin secretagogues. Exogenous administration of GLP-1 and GLP-1R agonists at pharmacological doses showed that they not only have insulinotropic effect, but also effects on suppressing glucagon secretion in the presence of hyperglycemia, delaying post-prandial gastric emptying, inducing satiety, and promoting weight loss over prolonged administration–all of which work in synergy to normalize glucose homeostasis in patients with T2DM. Furthermore, GLP-1R agonists were noted to increase insulin synthesis, increase islet cell turnover, and decrease β cell apoptosis in animals–properties that may help slow the progression or even reverse the course of diabetes. Indirect measures of β-cell function showed that GLP-1R agonists improved β-cell responsiveness to glucose as well as first- and second-phase insulin secretion. However, the improvement in β-cell functions reverted back to pre-treatment levels after discontinuation of therapy, at least in the case of exenatide. Nausea and vomiting are the common side effects during the initial weeks of therapy, which lessen with dose titration, and generally decline with continuous use. Patients with severe gastrointestinal diseases probably should not be started on GLP-1R agonists in case of development of pancreatitis. Long-term use of exenatide (data available up to three years) has shown sustained HbA1c reduction and weight loss, which are very encouraging because these effects have not been shown by any other class of hypoglycemic agents. GLP-1R agonists as treatment modalities for diabetes have a promising future, especially with their potential to help reverse or prevent diabetes.
Acknowledgments
The writing of this manuscript was supported entirely by the Intramural Research Program of the NIH, National Institute on Aging. The views expressed in this manuscript are those of the authors and do not reflect those of the NIH. The authors report no conflicts of interest in this work.
References
- ElrickHStimmlerLHladCJ JrAraiYPlasma insulin response to oral and intravenous glucose administrationJ Clin Endocrinol Metab1964241076108214228531
- McIntyreNHoldsworthCDTurnerDSIntestinal factors in the control of insulin secretionJ Clin Endocrinol Metab19652510131713245320560
- PerleyMJKipnisDMPlasma insulin responses to oral and intravenous glucose: studies in normal and diabetic sujbjectsJ Clin Invest19674612195419626074000
- BuffaRPolakJMPearseAGESolciaEGrimeliusLCapellaCIdentification of the Intestinal Cell Storing Gastric Inhibitory PeptideHistochemistry1975432492551097380
- OrskovCHolstJJKnuhtsenSBaldisseraFGPoulsenSSNielsenOVGlucagon-like peptides GLP-1 and GLP-2, predicted products of the glucagon gene, are secreted separately from pig small intestine but not pancreasEndocrinology19861194146714753530719
- TheodorakisMJCarlsonOMichopoulosSHuman duodenal enteroendocrine cells: source of both incretin peptides, GLP-1 and GIPAm J Physiol Endocrinol Metab20062903E550E55916219666
- EisseleRGokeRWillemerSGlucagon-like peptide-1 cells in the gastrointestinal tract and pancreas of rat, pig and manEur J Clin Invest19922242832911499644
- MeierJJNauckMAGlucagon-like peptide 1(GLP-1) in biology and pathologyDiabetes Metab Res Rev20052129111715759282
- KrarupTSaurbreyNMoodyAJKuhlCMadsbadSEffect of porcine gastric inhibitory polypeptide on beta-cell function in type I and type II diabetes mellitusMetabolism19873676776823298936
- NauckMAHeimesaatMMOrskovCHolstJJEbertRCreutzfeldtWPreserved incretin activity of glucagon-like peptide 1 [7–36 amide] but not of synthetic human gastric inhibitory polypeptide in patients with type-2 diabetes mellitusJ Clin Invest19939113013078423228
- ElahiDMcAloon-DykeMFukagawaNKThe insulinotropic actions of glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (7–37) in normal and diabetic subjectsRegul Pept14199451163748036284
- FeinleCChapmanIMWishartJHorowitzMPlasma glucagon-like peptide-1 (GLP-1) responses to duodenal fat and glucose infusions in lean and obese menPeptides20022381491149512182952
- JangHJKokrashviliZTheodorakisMJGut-expressed gustducin and taste receptors regulate secretion of glucagon-like peptide-1Proc Natl Acad Sci U S A200710438150691507417724330
- ElliottRMMorganLMTredgerJADeaconSWrightJMarksVGlucagon-like peptide-1 (7–36)amide and glucose-dependent insulinotropic polypeptide secretion in response to nutrient ingestion in man: acute post-prandial and 24-h secretion patternsJ Endocrinol199313811591667852887
- KimWEganJMThe role of incretins in glucose homeostasis and diabetes treatmentPharmacol Rev200860447051219074620
- VollmerKHolstJJBallerBPredictors of incretin concentrations in subjects with normal, impaired, and diabetic glucose toleranceDiabetes200857367868718057091
- NauckMAHeimesaatMMBehleKEffects of glucagon-like peptide 1 on counterregulatory hormone responses, cognitive functions, and insulin secretion during hyperinsulinemic, stepped hypoglycemic clamp experiments in healthy volunteersJ Clin Endocrinol Metab20028731239124611889194
- Toft-NielsenMBDamholtMBMadsbadSDeterminants of the impaired secretion of glucagon-like peptide-1 in type 2 diabetic patientsJ Clin Endocrinol Metab20018683717372311502801
- VilsbollTKrarupTDeaconCFMadsbadSHolstJJReduced postprandial concentrations of intact biologically active glucagon-like peptide 1 in type 2 diabetic patientsDiabetes200150360961311246881
- KiefferTJMcIntoshCHPedersonRADegradation of glucose-dependent insulinotropic polypeptide and truncated glucagon-like peptide 1 in vitro and in vivo by dipeptidyl peptidase IVEndocrinology19951368358535967628397
- Hupe-SodmannKMcGregorGPBridenbaughRCharacterisation of the processing by human neutral endopeptidase 24.11 of GLP-1 (7–36) amide and comparison of the substrate specificity of the enzyme for other glucagon-like peptidesRegul Pept19955831491568577927
- MeierJJNauckMAKranzDSecretion, degradation, and elimination of glucagon-like peptide 1 and gastric inhibitory polypeptide in patients with chronic renal insufficiency and healthy control subjectsDiabetes200453365466214988249
- HansenLDeaconCFOrskovCHolstJJGlucagon-like peptide-1-(7–36)amide is transformed to glucagon-like peptide-1-(9–36)amide by dipeptidyl peptidase IV in the capillaries supplying the L cells of the porcine intestineEndocrinology1999140115356536310537167
- Ruiz-GrandeCAlarconCAlcantaraARenal catabolism of truncated glucagon-like peptide 1Horm Metab Res199325126126168119664
- ThorensBPorretABuhlerLDengSPMorelPWidmannCCloning and functional expression of the human islet GLP-1 receptor. Demonstration that exendin-4 is an agonist and exendin-(9–39) an antagonist of the receptorDiabetes19934211167816828405712
- KiefferTJHabenerJFThe glucagon-like peptidesEndocr Rev199920687691310605628
- KjemsLLHolstJJVolundAMadsbadSThe influence of GLP-1 on glucose-stimulated insulin secretion: effects on beta-cell sensitivity in type 2 and nondiabetic subjectsDiabetes200352238038612540611
- RachmanJGribbleFMBarrowBALevyJCBuchananKDTurnerRCNormalization of insulin responses to glucose by overnight infusion of glucagon-like peptide 1 (7–36) amide in patients with NIDDMDiabetes19964511152415308866556
- ZanderMMadsbadSMadsenJLHolstJJEffect of 6-week course of glucagon-like peptide 1 on glycaemic control, insulin sensitivity, and beta-cell function in type 2 diabetes: a parallel-group studyLancet2002359930982483011897280
- MeneillyGSGreigNTildesleyHHabenerJFEganJMElahiDEffects of 3 months of continuous subcutaneous administration of glucagon-like peptide 1 in elderly patients with type 2 diabetesDiabetes Care200326102835284114514588
- MeneillyGSVeldhuisJDElahiDDeconvolution analysis of rapid insulin pulses before and after six weeks of continuous subcutaneous administration of glucagon-like peptide-1 in elderly patients with type 2 diabetesJ Clin Endocrinol Metab200590116251625616091500
- NauckMAKleineNOrskovCHolstJJWillmsBCreutzfeldtWNormalization of fasting hyperglycaemia by exogenous glucagon-like peptide 1 (7–36 amide) in type 2 (non-insulin-dependent) diabetic patientsDiabetologia19933687417448405741
- MeierJJGallwitzBSalmenSNormalization of glucose concentrations and deceleration of gastric emptying after solid meals during intravenous glucagon-like peptide 1 in patients with type 2 diabetesJ Clin Endocrinol Metab20038862719272512788879
- VerdichCFlintAGutzwillerJPA meta-analysis of the effect of glucagon-like peptide-1 (7–36) amide on ad libitum energy intake in humansJ Clin Endocrinol Metab20018694382438911549680
- NaslundEGutniakMSkogarSRossnerSHellstromPMGlucagon-like peptide 1 increases the period of postprandial satiety and slows gastric emptying in obese menAm J Clin Nutr19986835255309734726
- BrubakerPLDruckerDJMinireview: Glucagon-like peptides regulate cell proliferation and apoptosis in the pancreas, gut, and central nervous systemEndocrinology200414562653265915044356
- EganJMBulottaAHuiHPerfettiRGLP-1 receptor agonists are growth and differentiation factors for pancreatic islet beta cellsDiabetes Metab Res Rev200319211512312673779
- ByrneMMGliemKWankUGlucagon-like peptide 1 improves the ability of the beta-cell to sense and respond to glucose in subjects with impaired glucose toleranceDiabetes1998478125912659703326
- MigoyaEMMillerJLarsonPSitagliptin, a selective DPP-4 inhibitor, and metformin have complementary effects to increase active GLP-1 concentrationsDiabetes200756S1A74
- GreenBDGaultVAO’HarteFPFlattPRStructurally modified analogues of glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) as future antidiabetic agentsCurr Pharm Des200410293651366215579061
- KoltermanOGKimDDShenLPharmacokinetics, pharmacodynamics, and safety of exenatide in patients with type 2 diabetes mellitusAm J Health Syst Pharm200562217318115700891
- SimonsenLHolstJJDeaconCFExendin-4, but not glucagon-like peptide-1, is cleared exclusively by glomerular filtration in anaesthetised pigsDiabetologia200649470671216447056
- BuseJBHenryRRHanJKimDDFinemanMSBaronADEffects of exenatide (exendin-4) on glycemic control over 30 weeks in sulfonylurea-treated patients with type 2 diabetesDiabetes Care200427112628263515504997
- DeFronzoRARatnerREHanJKimDDFinemanMSBaronADEffects of exenatide (exendin-4) on glycemic control and weight over 30 weeks in metformin-treated patients with type 2 diabetesDiabetes Care20052851092110015855572
- KendallDMRiddleMCRosenstockJEffects of exenatide (exendin-4) on glycemic control over 30 weeks in patients with type 2 diabetes treated with metformin and a sulfonylureaDiabetes Care20052851083109115855571
- KlonoffDCBuseJBNielsenLLExenatide effects on diabetes, obesity, cardiovascular risk factors and hepatic biomarkers in patients with type 2 diabetes treated for at least 3 yearsCurr Med Res Opin200824127528618053320
- ZinmanBHoogwerfBJDuran GarciaSThe effect of adding exenatide to a thiazolidinedione in suboptimally controlled type 2 diabetes: a randomized trialAnn Intern Med2007146747748517404349
- HeineRJVan GaalLFJohnsDMihmMJWidelMHBrodowsRGExenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes: a randomized trialAnn Intern Med2005143855956916230722
- NauckMAMeiningerGShengDTerranellaLSteinPPEfficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, double-blind, non-inferiority trialDiabetes Obes Metab20079219420517300595
- MorettoTJMiltonDRRidgeTDEfficacy and tolerability of exenatide monotherapy over 24 weeks in antidiabetic drug-naive patients with type 2 diabetes: a randomized, double-blind, placebo-controlled, parallel-group studyClin Ther20083081448146018803987
- Eli Lilly and CompanyAmylin, Lilly Update on FDA Review of Byetta (exenatide) Injection Monotherapy Submission2008Accessed February 17, 2009 Available from: http://newsroom.lilly.com/releasedetail.cfm?releaseid=352884
- AmoriRELauJPittasAGEfficacy and safety of incretin therapy in type 2 diabetes: systematic review and meta-analysisJAMA2007298219420617622601
- BainSCStephensJWExenatide and pancreatitis: an updateExpert Opin Drug Saf20087664364418983211
- FehseFTrautmannMHolstJJExenatide augments first-and second-phase insulin secretion in response to intravenous glucose in subjects with type 2 diabetesJ Clin Endocrinol Metab200590115991599716144950
- MariANielsenLLNanayakkaraNDeFronzoRAFerranniniEHalsethAMathematical modeling shows exenatide improved beta-cell function in patients with type 2 diabetes treated with metformin or metformin and a sulfonylureaHorm Metab Res2006381283884417163361
- BunckMCDiamantMCornerAOne-year treatment with exenatide improves beta-cell function, compared to insulin glargine, in metformin treated type 2 diabetes patients: A randomized, controlled trialDiabetes Care2009 Feb 5 Epub ahead of print
- KnudsenLBKnudsenSMWilkenMPlasma protein binding of NN2211, a long-acting derivative of GLP-1, is important for its efficacyDiabetes200352Suppl 1A321A322
- KnudsenLBNielsenPFHuusfeldtPOPotent derivatives of glucagon-like peptide-1 with pharmacokinetic properties suitable for once daily administrationJ Med Chem20004391664166910794683
- AgersoHJensenLBElbrondBRolanPZdravkovicMThe pharmacokinetics, pharmacodynamics, safety and tolerability of NN2211, a new long-acting GLP-1 derivative, in healthy menDiabetologia200245219520211935150
- GarberAHenryRRatnerRLiraglutide versus glimepiride monotherapy for type 2 diabetes (LEAD-3 Mono): a randomised, 52-week, phase III, double-blind, parallel-treatment trialLancet2009373966247348118819705
- NauckMFridAHermansenKEfficacy and safety comparison of liraglutide, glimepiride, and placebo, all in combination with metformin, in type 2 diabetes: the LEAD (liraglutide effect and action in diabetes)-2 studyDiabetes Care2009321849018931095
- MarreMShawJBrandleMLiraglutide, a once-daily human GLP-1 analog, added to a sulfonylurea (SU) offers significantly better glycemic control and favorable weight change compared with rosiglitazone and SU combination therapy in subjects with type 2 diabetes Abstract presented at San Francisco, CA American Diabetes Association 68th Scientific Sessions2008
- Russell-JonesDVaagASchmitzOSignificantly better glycemic control and weight reduction with liraglutide, a once-daily human GLP-1 analog, compared with insulin glargine: all as add-on to metformin and a sulfonylurea in type 2 diabetes Abstract presented at San Francisco, CA American Diabetes Association 68th Scientific Sessions June 6–10, 2008
- ChangAMJakobsenGSturisJThe GLP-1 derivative NN2211 restores beta-cell sensitivity to glucose in type 2 diabetic patients after a single doseDiabetes20035271786179112829647
- MariADegnKBrockBRungbyJFerranniniESchmitzOEffects of the long-acting human glucagon-like peptide-1 analog liraglutide on beta-cell function in normal living conditionsDiabetes Care20073082032203317468345
- DegnKBJuhlCBSturisJOne week’s treatment with the long-acting glucagon-like peptide 1 derivative liraglutide (NN2211) markedly improves 24-h glycemia and alpha- and beta-cell function and reduces endogenous glucose release in patients with type 2 diabetesDiabetes20045351187119415111485
- DruckerDJBuseJBTaylorKExenatide once weekly versus twice daily for the treatment of type 2 diabetes: a randomised, open-label, non-inferiority studyLancet200837296451240125018782641
- KimDMacConellLZhuangDEffects of once-weekly dosing of a long-acting release formulation of exenatide on glucose control and body weight in subjects with type 2 diabetesDiabetes Care20073061487149317353504
- Eli LillyEli Lilly Investment community Update December 112008Accessed on: March 10, 2009 Available from: http://files.shareholder.com/downloads/LLY/544477551x0x258459/5acdc123-b0e7-498c-ab5c-92c599f205f2/Eli%20Lilly%2012-11-08.pdf
- BaggioLLHuangQCaoXDruckerDJAn albumin-exendin-4 conjugate engages central and peripheral circuits regulating murine energy and glucose homeostasisGastroenterology200813441137114718313669
- ConjuChemPD-DACTM: Exendin-4 (CJC-1145-PC)2009Accessed February 7, 2009 Available from: http://www.conjuchem.com/
- GlaxoSmithKlineGSK initiates phase III programme for novel type 2 diabetes medication, Syncria® (albiglutide) February 172009Accessed March 31, 2009 Available from: http://us.gsk.com/html/media-news/pressreleases/2009/2009_pressrelease_10025.htm
- Novo NordiskOnce-weekly GLP-1 analogue (NN9535)2009Accessed March 7, 2009 Available from: http://www.novonordisk.com/science/pipeline/rd_pipeline.asp?showid=10
- F-Hoffmann-La Roche LtdRoche moves investigational diabetes drug, Taspoglutide, into Phase III clinical trials June 102008Accessed March 28, 2009 Available from: http://www.roche.com/med-cor-2008-06-10-e.pdf
- Sanofi-Aventis New diabetes compound AVE0010 showed clear dose response results with once-a-day injection in phase IIb study June 72008Accessed March 28, 2009 Available from: http://se.sanofi-aventis.com/live/se/sv/layout.jsp?cnt=A920FF21-6EA2-42A0-80BE-E242E4D1E088
- Merrion PharmaceuticalsMerrion announces license agreement with Novo Nordisk to develop oral formulation of GLP-1 receptor agonist(s) January 162009Accessed January 16, 2009 Available from: http://www.merrionpharma.com/archive/Merrion_NN_GLP-1.pdf
- NauckMADuranSKimDA comparison of twice-daily exenatide and biphasic insulin aspart in patients with type 2 diabetes who were suboptimally controlled with sulfonylurea and metformin: a non-inferiority studyDiabetologia200750225926717160407