Abstract
Background
Post-poliomyelitis syndrome is a clinical condition that can affect poliomyelitis survivors with the onset of new symptoms several years after the acute disease. These symptoms include new muscular weakness, fatigue, pain, onset or aggravation of muscle atrophy, muscle cramps, onset or aggravation of pre-existing difficulties in accomplishing daily life activities, cold intolerance, sleep disorders, dysphonia or dysphagia, and respiratory deficiency. The treatment of post-poliomyelitis syndrome requires a multiprofessional health team because the rehabilitation procedures include lifestyle changes, physiotherapy, avoidance of secondary complications, and physical exercise. As physical exercise is prescribed by physical education professionals, the assessment of knowledge about post-poliomyelitis syndrome among these professionals is very relevant. The aim of this study was to evaluate poliomyelitis and post-poliomyelitis syndrome knowledge among physical education professionals in Brazil.
Methods
We invited participants with an academic degree in physical education (n = 217) to participate in this study. A self-administered survey (30 questions) was designed to probe knowledge about poliomyelitis and post-poliomyelitis syndrome. From the survey, we created a questionnaire to evaluate the performance of the professionals. The questionnaire was composed of 20 questions and a score was provided, varying from 0 (totally uninformed) to 20 (well informed).
Results
Approximately 73% of surveyed participants had never heard of post-poliomyelitis syndrome, and only 19.4% had received information about the disease. Among those surveyed, 61.8% did not know whether restriction of physical activities was warranted for people with poliomyelitis sequelae, and only 32.3% knew that physical exercise (especially intense exercise) should be limited for patients with sequelae of paralytic poliomyelitis.
Conclusion
The findings of the present study indicate a critical need for improvement of knowledge about post-poliomyelitis syndrome among Brazilian physical education professionals.
Introduction
Many people with a history of poliomyelitis report late-onset neuromuscular symptoms and a decline in their functional abilities. These late-onset symptoms are referred to as post-poliomyelitis syndrome (PPS), and include new or increased muscle weakness, fatigue, muscle and joint pain, muscle cramps, and cold intolerance.Citation1 The current pathophysiologic hypothesis is that PPS is caused by the premature metabolic exhaustion of chronically overloaded motor neurons.Citation2–Citation6 These new symptoms also cause progressively increasing difficulties with physical functions, such as walking, standing, climbing stairs, and other mobility-related activities of daily life.Citation7,Citation8
Although the number of new cases of poliomyelitis has dropped dramatically due to the introduction of an effective vaccination program, there are still approximately 20 million people with poliomyelitis sequelaeCitation9 who may develop PPS and need rehabilitation interventions. In addition, some African and Asian countries are registering new cases of poliomyelitis. According to the World Health Organization, in 2013, only three countries (Afghanistan, Nigeria, and Pakistan) remain polio-endemic and eight are affected by importations of the virus (Central African Republic, Côte d’Ivoire, Kenya, Liberia, Mali, Niger, Somalia, and Uganda).Citation10 Therefore, the future perspective is for a continued or potentially increased need for treatment of people with PPS.
Treatment of PPS requires a multiprofessional health team and is based on lifestyle changes, physiotherapy, physical exercise, and avoidance of secondary complications.Citation1 In this context, physical exercise is an important tool for rehabilitation of patients with PPS. However, physical exercise is beneficial for these patients only if an appropriate strategy is determined. Although the benefits of regular physical exercise are without question,Citation11 the prescription of exercise for people with sequelae of paralytic poliomyelitis has been the focus of an extensive debate. Health professionals believe that physical exercise in these patients, especially intense physical exercise, may be harmful because the resultant metabolic overload on motor units that physical exercise induces can precipitate development of PPS.Citation1 However, physical exercise is a useful tool for the treatment of muscle fatigue and weakness, both symptoms that are present in patients with sequelae of paralytic poliomyelitis. Therefore, current management guidelines recommend that only mild to moderate exercise should be performed to avoid metabolic overload on the giant motor units.Citation1 In Brazil, physical exercise is prescribed by physical education professionals, so evaluation of knowledge of these professionals about the disease is substantially relevant. In addition, previous studies have shown that these professionals do not have adequate knowledge about other diseases, including acquired immune deficiency syndrome (AIDS)Citation12 and epilepsy.Citation13,Citation14 Thus, in the present study, we evaluated the knowledge about poliomyelitis and PPS among Brazilian physical education professionals. We hypothesized that physical education professionals would not have knowledge related to PPS, such as physiopathology, patient care, and symptomatology.
Materials and methods
Participants
We invited participants from the community with an academic degree in physical education (n = 217, 54 females and 163 males, age 30.1 ± 7.1 years [mean ± standard deviation]) to participate in this study using different sources of advertisement (ie, Internet, local newspapers, magazine and billboards in universities, clinics, hospitals, and gymnasiums). Inclusion criteria for participation in the study were professionals with at least an undergraduate degree in physical education. All procedures involved in this study were approved by the university ethics committee and followed the principles outlined in the Declaration of Helsinki. All participants gave their written informed consent to participate in this study.
Survey
A self-administered survey was designed to probe knowledge about poliomyelitis and PPS. The survey contained 30 items (14 about poliomyelitis and 16 about PPS) with simple, closed end-type response scales. This survey was constructed according to previous recommendations.Citation15,Citation16 From the survey (composed of 30 questions), we created a questionnaire using 20 questions (see and ) in order to evaluate, in an objective manner, the performance of the professionals interviewed. Through the questionnaire, a score was provided, varying from 0 (totally uninformed) to 20 (well informed). For each of the 20 questions, there was a correct answer; the participant who correctly answered received 1 point and one who erred received 0 point. These 20 questions were chosen because they contain basic knowledge about poliomyelitis and PPS. Additionally, the subjects were divided into two groups, ie, those who answered “yes” and those who answered “no” to the question “Have you received information about PPS?” ().
Figure 1 Questionnaire result (0–20) separated by physical education professionals without (n = 175) or with (n = 42) access to information about post-poliomyelitis syndrome.
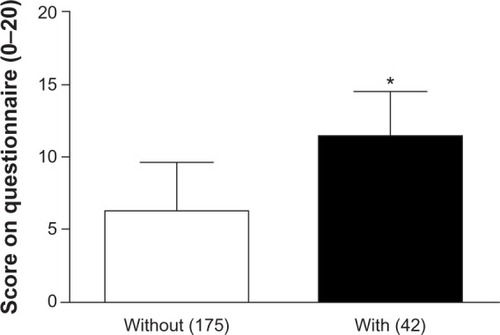
Table 1 Answers of physical educational professionals related to poliomyelitis
Table 2 Answers of physical educational professionals related to post-poliomyelitis syndrome
Statistical analysis
A descriptive statistical analysis was performed (mean, standard deviation, and absolute and relative frequencies). None of the variables presented with normal distributions according to Kolmogorov-Smirnov tests. Therefore, Mann-Whitney tests were used to compare scores obtained in the questionnaire between the two exposure (“yes” and “no”) groups. Spearman’s correlation tests were used to assess correlations between scores on the questionnaire, experience in the field, and education level. Differences were considered to be statistically significant at the level of P < 0.05.
Results
Participants’ mean time working in physical education was 6 ± 6 years. Among all participants, 4.1% (n = 9) had a doctoral degree, 3.2% (n = 7) had a master’s degree, 83.4% (n = 181) were specialized in an exercise or sports science, and 9.2% (n = 20) had an undergraduate academic degree. Areas of expertise were varied, with 0.9% (n = 2) of participants having professional experience of adapted sports for people with disabilities, 4.1% (n = 9) having academic/scientific research experience, 12.0% (n = 26) having high-performance sport experience, 43.8% (n = 95) having techniques to improve general health and quality of life experience, and 23.0% (n = 50) having experience with physical education in schools. An additional 13.4% (n = 29) did not give an area of expertise and 2.8% (n = 6) worked in a specific area of expertise not related to physical education. and show the participants’ knowledge about poliomyelitis and PPS, respectively.
With regard to our questionnaire, we found that professionals who had received previous information about PPS had significantly higher scores than those who had never received information. On average, this difference was approximately 84% () (P < 0.0001).
To demonstrate that the professional experience factor contributes to high performance levels, we correlated performance on the questionnaire and duration of professional activities. We found a statistically significant correlation between experience in the field and scores in our questionnaire (r = 0.1812, P = 0.0093). Moreover, we found a correlation between education level and scores obtained in the questionnaire (r = 0.2115, P = 0.0017).
Discussion
Investigations of the knowledge of physical education professionals about specific diseases are very rare. These types of investigations are important because physical exercise has been considered an important tool for the prevention and treatment of chronic diseases.Citation16,Citation17 This is the first study to assess knowledge among physical education professionals about poliomyelitis and PPS. We found that knowledge about poliomyelitis and PPS is low among Brazilian physical education professionals, particularly among those professionals who have had no access to previous information about PPS.
As the majority of surveyed participants had not received any formal education about PPS during their undergraduate degrees (93.5%) and 61.8% did not know about the restrictions on physical activity practice for patients with poliomyelitis sequelae, it is quite plausible that these professionals do not know how to manage a physical exercise program for patients with poliomyelitis sequelae. Thus, physical exercise prescribed by these professionals could be harmful to the health of these patients. The continued education of these professionals should be promoted by public health systems. Similar results have been found for epilepsyCitation13,Citation14 and human immunodeficiency virus-positive patients.Citation12 For example, Boyle et alCitation12 investigated the knowledge of physical education professionals about AIDS and demonstrated that only 22.2% of professionals had received formal education about AIDS.
Although most professionals had already heard about paralytic poliomyelitis (95.9%), they did not have appropriate knowledge about the characteristics of the disease (38.7% did not know the etiologic agent and 52.5% did not know the transmission mode or that a person with sequelae of paralytic poliomyelitis may develop PPS). Only 25.3% of the respondents had heard of PPS, and only 17.1% of professionals recognized that a person with sequelae of paralytic poliomyelitis may develop PPS. Consequently, the knowledge of these professionals about the clinical characteristics of PPS was low.
This is not the first study that has demonstrated a low level of knowledge among physical education professionals about a neurologic disease. Vancini et alCitation13,Citation14 showed that these professionals did not have accurate knowledge about epilepsy. According to Vancini et al,Citation13,Citation14 these results are probably a consequence of two hypotheses, ie, a considerable lack of information and any formal instruction on epilepsy during their graduate study and training, and these professionals not usually being included in a workplace of primary health care, such as health centers, clinics, and hospitals; consequently, they might have less contact with people with epilepsy when compared with physicians and nurses. Therefore, it is reasonable that similar hypotheses can be assumed in our study.
In addition to the general lack of knowledge about PPS and paralytic poliomyelitis, one of the main findings of this study was the fact that there was a positive correlation between education and knowledge of paralytic poliomyelitis and PPS. Professionals who have already obtained information about the disease have a higher level of knowledge than those who have never had access to any information about the disease. These findings can be used to sensitize the leaders of public health systems and education to two aspects of PPS education: physical education professionals demonstrate an increase in practical knowledge (at least for this disease) with an increase in education, so these professionals should be encouraged to participate in continuing education programs; and training programs, even those of short duration, may be beneficial for increasing knowledge about PPS among these professionals and most likely among other health professionals as well. Finally, we also demonstrated that more experienced professionals have a greater level of knowledge about poliomyelitis and PPS, possibly because they have already received additional sources of information during their careers, such as participation in congresses, seminars, and scientific meetings, and possibly through higher levels of education.
In conclusion, our study shows that physical education professionals do not have appropriate knowledge about poliomyelitis and PPS. Therefore, the services provided by these professionals may be compromised, and physical exercise prescribed by these professions could harm the patient. Additionally, it is possible that similarly low levels of poliomyelitis and PPS knowledge could be present among other health professionals, including nurses, physiotherapists, physicians, and nutritionists, as demonstrated by Vancini et alCitation13 for epilepsy. Therefore, further studies should be conducted to understand better the knowledge of these professionals about PPS. Public training policies should be implemented to increase knowledge about poliomyelitis and PPS and therefore to improve the services provided to patients.
Author contributions
CABL contributed to the study concept and design, data acquisition, analysis, interpretation, and manuscript preparation. TMAA, LFPP, and BSS contributed to data acquisition, data analysis, and manuscript preparation. MGS, SABR, and MSA contributed to study concept and design, data analysis, interpretation, and manuscript preparation. RLV contributed to study concept and design, data analysis, interpretation, manuscript preparation, and critical revision of the manuscript.
Acknowledgments
We would like to thank all of the participants who volunteered their time to participate in the study, which was supported by the Fundação de Amparo à Pesquisa do Estado de Goiás (FAPEG, Brazil; grant number 2009/10267000347). TMAA had a fellowship from the Conselho Nacional de Desenvolvimento Científico e Tecnológico – Programa Institucional de Bolsas de Iniciação Científica (CNPq/PIBIC, Brazil).
Disclosure
No commercial party having a direct financial interest in the results of the research presented in this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.
References
- TiffreauVRapinASerafiRPost-polio syndrome and rehabilitationAnn Phys Rehabil Med201053425020044320
- IvanyiBOngerboer de VisserBWMacro EMG follow-up study in post-poliomyelitis patientsJ Neurol199424237407897450
- StålbergEGrimbyGDynamic electromyography and muscle biopsy changes in a 4-year follow-up: study of patients with a history of polioMuscle Nerve1995186997077783759
- McComasAJQuartlyCGriggsRCEarly and late losses of motor units after poliomyelitisBrain1997120141514219278631
- RodriguezAAAgreJCCorrelation of motor units with strength and spectral characteristics in polio survivors and controlsMuscle Nerve1991144294341870634
- WiechersDOHubbellSLLate changes in the motor unit after acute poliomyelitisMuscle Nerve198145245286273721
- IvanyiBNolletFRedekopWKLate onset polio sequelae: disabilities and handicaps in a population-based cohort of the 1956 poliomyelitis outbreak in The NetherlandsArch Phys Med Rehabil19998068769010378496
- NolletFBeelenAPrinsMHDisability and functional assessment in former polio patients with and without postpolio syndromeArch Phys Med Rehabil19998013614310025486
- AylwardRBHullHFCochiSLDisease eradication as a public health strategy: a case study of poliomyelitis eradicationBull World Health Organ20007828529710812724
- World Health OrganizationPoliomyelitis. Fact sheet 114 Available from: http://www.who.int/mediacentre/factsheets/fs114/en/Accessed June 21, 2013
- GarberCEBlissmerBDeschenesMRAmerican College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exerciseMed Sci Sports Exerc2011431334135921694556
- BoyleMSitlerMKimuraIKnowledge and attitudes of certified athletic trainers in Pennsylvania toward HIV/AIDS and treating HIV-positive athletesJ Athl Train199732404416558431
- VanciniRLBenedito-SilvaAASousaBSKnowledge about epilepsy among health professionals: a cross-sectional survey in Sao Paulo, BrazilBMJ Open20122e000919
- VanciniRLLiraCAGomes da SilvaSEvaluation of physical educators’ knowledge about epilepsyArq Neuropsiquiatr20106836737120602037
- KelleyKClarkBBrownVGood practice in the conduct and reporting of survey researchInt J Qual Health Care20031526126612803354
- BurnsKEDuffettMKhoMEA guide for the design and conduct of self-administered surveys of cliniciansCMAJ200817924525218663204
- ChomistekAKCookNRFlintAJVigorous-intensity leisure-time physical activity and risk of major chronic disease in menMed Sci Sports Exerc2012441898190522543741
- MorrisPJPhysical activity recommendations for children and adolescents with chronic diseaseCurr Sports Med Rep2008735335819005359