
Abstract
Several studies have validated the role of telemedicine as a new powerful screening and diagnostic tool for retinal disorders, such as diabetic retinopathy and retinopathy of prematurity. With regard to retinopathy of prematurity, bedside examination with binocular indirect ophthalmoscopy has been the gold standard technique for screening, yet with several limitations. Herein, we review the current evidence that supports the role of telemedicine for the screening of infants with retinopathy of prematurity.
Introduction
Advances in diagnostic technologies have revolutionized our understanding and treatment of retinal diseases. The advent of transferrable retinal imaging has enhanced the care of patients with retinopathies by 1) improving diagnostic accuracy, assessment, and documentation and 2) ushering in telemedicine as a new paradigm of delivering care.
With respect to retinopathy of prematurity (ROP), timely screening and early treatment remain the most crucial factors for prevention of lifelong vision-threatening sequelae. Telemedical care of infants with ROP has become a reality. Improvements have been made in image quality and software engineering, and multiple validation studies have demonstrated the efficacy of remote screening. However, bedside examinations remain the mainstay for ROP screening in most practices. This paper will review the rationale for remote photographic screening for ROP.
Current screening for ROP and limitations
According to the guidelines published jointly by the American Academy of Ophthalmology, American Academy of Pediatrics, and American Association for Pediatric Ophthalmology and Strabismus, infants with birth weight <1,500 g or gestational age ≤30 weeks, and infants with birth weight 1,500–2,000 g or gestational age >30 weeks with an unstable clinical course should receive dilated ophthalmoscopic examinations for ROP screening.Citation1 These exams are most usually performed with binocular indirect ophthalmoscopy (BIO) at the neonatal intensive care unit (NICU) bedside and require the coordination of NICU staff with the screening ophthalmologist. Scleral depression technique is commonly utilized, which can be particularly stressful for premature infants and may cause apnea, bradycardia, and aspiration.Citation2,Citation3
BIO and retinal drawings have been used since the 1950s for the screening and documentation of ROP. Undoubtedly, the development of an international classification system has allowed standardization of the disease severity, description, and location of retinal abnormalities in ROP.Citation4 However, a significant limitation of bedside examination is the subjectivity of the examiner impression of the BIO findings especially in a squirming live exam. Sometimes, a poorly dilated eye of a premature infant, corneal clouding, tunica vasculosa lentis, and vitreous haze render the exam even more challenging. In fact, several studies have shown a wide range of disagreement of ROP diagnosis and severity among health care professionals screening for ROP.Citation5,Citation6 In the pivotal CRYO-ROP trial, there was disagreement between two unmasked, certified examiners as to whether threshold disease was present in 12% of eyes.Citation7 Furthermore, the documentation of exam findings is solely based on memory using paper charts with handwritten sketches or, more recently, electronic medical records that utilize drawing tools and templates. The latter makes independent verification of disease status as well as monitoring disease progression particularly challenging.
Conversely, there is an increasing discordance between the number of premature infants requiring ROP screening and the number of ophthalmologists performing it. In 2006, a survey of 224 pediatric ophthalmologists and retinal specialists by the American Academy of Ophthalmology revealed that only 54% of retinal specialists and pediatric ophthalmologists were willing to manage ROP and 20% of them were considering stopping due to decreasing reimbursement and high medicolegal liability.Citation8
Telemedicine for ROP screening
Telemedicine refers to the use of telecommunication and information technologies in order to provide clinical health care at a distance.Citation9 With regard to “store-and-forward” telemedicine, it involves capturing of patient data usually by nonphysician providers for subsequent interpretation by a remote expert. Numerous studies have shown that photographic screening using contact wide-field cameras can detect treatment and/or referral-warranted ROP at a rate that is safe and comparable to live screening with BIO.Citation1 These results were fairly consistent even among different camera operators, who included trained ophthalmologists,Citation10–Citation12 ophthalmic photo graphers,Citation13–Citation15 or trained neonatal personnel.Citation14,Citation16,Citation17 Most of the studies have compared the gold standard for ROP screening, that is, BIO bedside exam, against wide-angle contact imaging systems (eg, RetCam; Clarity Medical Systems, Pleasanton, CA, USA). The e-ROP study was a multicenter study to test the ability of nonphysicians to recognize referral warranted-ROP or alternatively ROP at high risk of causing vision loss. In addition, 43% of severe ROP cases were identified by telemedicine before they were detected by an ophthalmologist which was on average 2 weeks earlier.Citation18,Citation19 This is likely due to being able to objectively track the progression of the fundus appearance – one of the largest advantages of photographic screening.
With >15 years of studies validating the accuracy and sensitivity of telemedicine in ROP screening, several live telemedicine programs have already demonstrated promising results.Citation20 The Stanford University Network for Diagnosis of Retinopathy of Prematurity telemedicine program has been screening five NICUs in the San Francisco Bay area since December 2005. The recently published 6-year results were highly favorable with respect to diagnostic accuracy of ROP.Citation21 Remote interpretation of images had a sensitivity of 100%, specificity of 99.8%, positive predictive value of 95.5%, and negative predictive value of 100% for the detection of treatment-warranted ROP. No adverse anatomical outcomes were observed for any infant. Similar results were demo nstrated from telemedicine programs in GermanyCitation22 and India.Citation23 In the authors’ group, remote ROP screening led to a reduction of live exams by 84% without any infant missing a treatment interval ().Citation24
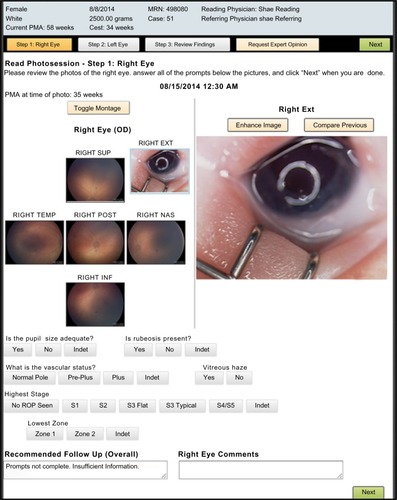
Figure 1 Computer screenshot of the interface of a telemedicine software.
Abbreviations: PMA, post-menstrual age; Cest, gestational age; SUP, superior; EXT, external; TEMP, temporal; POST, posterior pole; NAS, nasal; INF, inferior; Indet, indeterminate; S1, Stage 1; S2, Stage 2; S3 Flat, Stage 3 with flat neovascularization; S4/S5, Stage 4/Stage5.
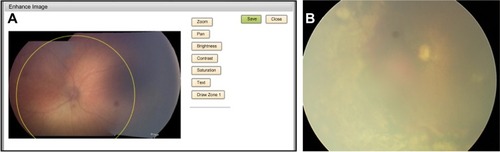
It has been shown that the clinical determination of zone 1 ROP disease and the presence of plus disease is imperfect,Citation6,Citation25 which has important implications since the majority of ROP treatment decisions are based on the presence of plus or zone 1 disease.Citation26 Photographic screening may be particularly helpful in the diagnosis of plus disease and type 1 ROP in general as several sophisticated software programs can now objectively quantify the amount of retinal vessel tortuosityCitation27–Citation29 or assist in the determination of zone 1 (). In a study performed by Abbey et al,Citation30 utilizing the ROP Tool for detecting plus disease, 93% of images were able to be processed by the tool. It is anticipated that new cameras with better image acquisition will aid in increasing this percentage even further.
Figure 2 Computerized Zone 1 determination.
Other advantages of telemedicine in ROP screening
A clear advantage of utilizing telemedicine in the screening of ROP lies in the fact that it allows improved access to health care by overcoming geographical challenges. This is especially true given that ROP screening is traditionally performed by highly specialized professionals who may not be accessible for rural NICUs.Citation31 Telemedicine allows immediate communication between local health care providers and expert consultants in a cost-effective manner.Citation32,Citation33 Scheduling conflicts are avoided and labor costs are decreased. Telemedicine examinations also require significantly less physician time than standard BIO bedside examinations.Citation34
Furthermore, the acquisition of fundus photographs aids in the education of parents. Clinical imaging illuminates the disease patterns seen in ROP for patients families, an entity otherwise abstract and difficult to comprehend. Clinical improvement would also be easier to document and convey to the patient, families, and other members of the patient care team. Fundus photographs can also serve as educational tools for less experienced ROP screeners or those in training. Sick infants are often transferred to tertiary care institutes where expert ROP treaters are accessible, but rural hospitals are often caring for less acutely ill infants, and ROP screeners in such clinical facilities may not be as familiar with the nuances of advanced ROP. Ongoing continuing education can therefore be incorporated into telemedicine screening programs.
Finally, telemedicine allows unequivocal documentation. The medicolegal climate surrounding ROP has always been complex and a deterrent for the recruitment of more screeners and treaters. While malpractice claims are, in fact, very rare, each lawsuit can be costly.Citation35 Physicians should be aware of risk management strategies, and photodocumentation is one method of demonstrating sound clinical practice and judgment, should legal action occur.
Limitations and other considerations
Image quality is an important factor for effective and reliable ROP screening. This is particularly an issue in darkly pigmented fundi or infants with small palpebral fissures, which prevent adequate contact of the camera and the corneal surface (). Vitreous or corneal haze due to extreme prematurity, vitreous hemorrhage, or motion artifacts are also additional factors that can affect image quality rendering their interpretation challenging. Uninterpretable images range from 8% to 21% in published studies.Citation10,Citation15
In addition, some may argue that the high cost of a wide-field imaging camera is prohibitive for participation in telemedicine programs. Even the smaller, more affordable retinal cameras cost ∼$90,000–$140,000, a cost difficult to absorb for smaller institutions. It is hoped that the advent of newer, cost-effective imaging technology would allow for more centers to participate in the screening of ROP via telemedicine. Of equal importance is medicolegal liability for telemedicine in ROP. Considering its relatively recent introduction in clinical practice, the legislation concerning telemedicine can be poorly defined and laws governing medical liability may differ from state to state regarding telemedicine.
Conclusion
In summary, telemedicine provides better documentation of disease severity and progression and appears to have several advantages over traditional bedside examination, which has been the gold standard for ROP screening. The future of ROP screening is to provide objective data by reducing subjectivity and potentially human error. The beauty of telemedicine lies in the fact that it provides the platform for reduction of subjectivity in ROP by providing objective data overseen by physicians thus providing high quality care.
Disclosure
AT, BT, and YY have no financial or proprietary interest in the materials presented herein. MTT is founder and equity partner of Focus ROP, partner in Pediatric Wide Angle Camera LLC, and licensed ROP Tool. DMM is director of telemedicine at Byers Eye Institute and has equity in Visunex Medical Systems. The authors report no other conflicts of interest in this work.
References
- FiersonWMAmerican Academy of Pediatrics Section on Ophthalmology, American Academy of Ophthalmology, American Association for Pediatric Ophthalmology and Strabismus, American Association of Certified OrthoptistsScreening examination of premature infants for retinopathy of prematurityPediatrics2013131118919523277315
- RushRRushSNicolauJChapmanKNaqviMSystemic manifestations in response to mydriasis and physical examination during screening for retinopathy of prematurityRetina200424224215097885
- LawsDEMortonCWeindlingMClarkDSystemic effects of screening for retinopathy of prematurityBr J Ophthalmol19968054254288695564
- An international classification of retinopathy of prematurity. The Committee for the Classification of Retinopathy of PrematurityArch Ophthalmol19841028113011346547831
- Paul ChanRVWilliamsSLYonekawaYWeissgoldDJLeeTCChiangMFAccuracy of retinopathy of prematurity diagnosis by retinal fellowsRetina (Philadelphia, Pa)2010306958965
- ChiangMFJiangLGelmanRDuYEFlynnJTInterexpert agreement of plus disease diagnosis in retinopathy of prematurityArch Ophthalmol2007125787588017620564
- Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Cryotherapy for Retinopathy of Prematurity Cooperative GroupArch Ophthalmol198810644714792895630
- CeliaFAn ophthalmology crisis: retinopathy of prematurity. Retinal Physician2006 Available from: http://www.retinalphysician.com/printarticle.aspx?articleID=100242Accessed October 27, 2015
- FieldMJGrigsbyJTelemedicine and remote patient monitoringJAMA2002288442342512132953
- Photographic Screening for Retinopathy of Prematurity (Photo-ROP) Cooperative GroupBalasubramanianMCaponeAHartnettMEPignattoSTreseMTThe Photographic Screening for Retinopathy of Prematurity Study (Photo-ROP): study design and baseline characteristics of enrolled patientsRetina2006267 SupplS4S1016946677
- SchwartzSDHarrisonSAFerronePJTreseMTTelemedical evaluation and management of retinopathy of prematurity using a fiberoptic digital fundus cameraOphthalmology20001071252810647714
- EllsALHolmesJMAstleWFTelemedicine approach to screening for severe retinopathy of prematurity: a pilot studyOphthalmology2003110112113211714597517
- ChiangMFKeenanJDStarrenJAccuracy and reliability of remote retinopathy of prematurity diagnosisArch Ophthalmol2006124332232716534051
- RothDBMoralesDFeuerWJHessDJohnsonRAFlynnJTScreening for retinopathy of prematurity employing the retcam 120: sensitivity and specificityArch Ophthalmol2001119226827211176990
- WuCPetersenRAVanderVeenDKRetCam imaging for retinopathy of prematurity screeningJ AAPOS200610210711116678743
- ChiangMFWangLBusuiocMTelemedical retinopathy of prematurity diagnosis: accuracy, reliability, and image qualityArch Ophthalmol2007125111531153817998515
- LajoieAKoreenSWangLRetinopathy of prematurity management using single-image vs multiple-image telemedicine examinationsAm J Ophthalmol2008146229830918547536
- QuinnGraham Ee-ROP Cooperative GroupTelemedicine approaches to evaluating acute-phase retinopathy of prematurity: study designOphthalmic Epidemiol201421425626724955738
- QuinnGEYingG-SDanielEValidity of a telemedicine system for the evaluation of acute-phase retinopathy of prematurityJAMA Ophthalmol2014132101178118424970095
- ChiangMFMeliaMBuffennANDetection of clinically significant retinopathy of prematurity using wide-angle digital retinal photography: a report by the American Academy of OphthalmologyOphthalmology201211961272128022541632
- WangSKCallawayNFWallensteinMBHendersonMTLengTMoshfeghiDMSUNDROP: six years of screening for retinopathy of prematurity with telemedicineCan J Ophthalmol201550210110625863848
- LorenzBSpasovskaKElfleinHSchneiderNWide-field digital imaging based telemedicine for screening for acute retinopathy of prematurity (ROP). Six-year results of a multicentre field studyGraefes Arch Clin Exp Ophthalmol200924791251126219462177
- VinekarAJayadevCMangaleshSShettyBVidyasagarDRole of tele-medicine in retinopathy of prematurity screening in rural outreach centers in India – A report of 20,214 imaging sessions in the KIDROP programSemin Fetal Neonatal Med201520533534526092301
- TreseMTDrenserKCaponeATelemedicine for ROP screeningInvest Ophthalmol Vis Sci2014551359055905
- ChiangMFThyparampilPJRabinowitzDInterexpert agreement in the identification of macular location in infants at risk for retinopathy of prematurityArch Ophthalmol201012891153115920837799
- SolarteCEAwadAHWilsonCMEllsAPlus disease: why is it important in retinopathy of prematurity?Middle East Afr J Ophthalmol201017214815520616922
- GelmanRMartinez-PerezMEVanderVeenDKMoskowitzAFultonABDiagnosis of plus disease in retinopathy of prematurity using Retinal Image multiScale AnalysisInvest Ophthalmol Vis Sci200546124734473816303973
- CheungCSYButtyZTehraniNNLamWCComputer-assisted image analysis of temporal retinal vessel width and tortuosity in retinopathy of prematurity for the assessment of disease severity and treatment outcomeJ AAPOS201115437438021907122
- KoreenSGelmanRMartinez-PerezMEEvaluation of a computer-based system for plus disease diagnosis in retinopathy of prematurityOphthalmology200711412e59e6718054630
- AbbeyAMBesirliCGMuschDCEvaluation of Screening for Retinopathy of Prematurity by ROPtool or a Lay ReaderOphthalmology201612338539026681393
- WeaverDTMurdockTJTelemedicine detection of type 1 ROP in a distant neonatal intensive care unitJ AAPOS20121622923322681938
- JacksonKMScottKEGraff ZivinJCost-utility analysis of telemedicine and ophthalmoscopy for retinopathy of prematurity managementArch Ophthalmol2008126449349918413518
- Castillo-RiquelmeMCLordJMoseleyMJFielderARHainesLCost-effectiveness of digital photographic screening for retinopathy of prematurity in the United KingdomInt J Technol Assess Health Care200420220121315209180
- RichterGMSunGLeeTCSpeed of telemedicine vs ophthalmoscopy for retinopathy of prematurity diagnosisAm J Ophthalmol20091481136142.e219376496
- DaySMenkeAMAbbottRLRetinopathy of prematurity malpractice claims: the ophthalmic mutual insurance company experienceArch Ophthalmol2009127679479819506200