
Abstract
Risk and protective processes are integrated developmental processes that directly or indirectly affect behavioral outcomes. A better understanding of these processes is needed, in order to gauge their contribution to sexual risk behaviors. This retrospective cross-sectional study modeled the ecodevelopmental chain of relationships to examine the social contexts of African-American (AA) adolescents associated with sexually transmitted disease (STD)- and HIV-risk behaviors. We used data from 1,619 AA adolescents with an average age of 16±1.8 years obtained from the first wave of the National Longitudinal Study of Adolescent Health for this study. Confirmatory factor analysis followed by structural equation modeling was conducted to identify the latent constructs that reflect the social–interactional components of the ecodevelopmental theory. Among contextual factors, findings indicated that a feeling of love from father, school, religion, and parent attitudes toward adolescent sexual behavior were all factors that played significant roles in the sexual behavior of AA adolescents. AA adolescents who reported feeling love from their father, feeling a strong negative attitude from their parents toward having sex at a very young age, and having a strong bond with school personnel were associated with better health statuses. The level of parents’ involvement in their children’s lives was reflected in the adolescents’ feeling of love from parents and moderated by their socioeconomic status. Being male, attaining increased age, and being a sexual minority were associated with higher likelihood of exhibiting risky sexual behavior. In contrast, higher socioeconomic status and fathers’ level of involvement were indirectly associated with reduced STD/HIV-related sexual risk behavior. In conclusion, our findings suggest that interventions aimed at maximal protection against STD/HIV-related risk behavior among AA adolescents should adopt both self- and context-based strategies that promote positive functioning in the family, school, and peer microsystems.
Introduction
African Americans (AAs) are disproportionately affected by HIV in the US, especially among youth in the age-group 13–24 years.Citation1 According to a Centers for Disease Control and Prevention’s HIV-surveillance report, AAs represented 44% of new HIV infections and 42% of all diagnosed persons with AIDS, while only representing 12% of the total US population in 2014.Citation1 Young people aged 13–24 years are the most vulnerable group, with the highest rate of undiagnosed HIV, and represent approximately 22% of all newly diagnosed individuals.Citation1 Indeed, among this age-group, AAs are the most threatened by HIV infection in the US, given that they account for 63% and 55% of new infections among 13- to 19- and 20- to 24-year-olds, respectively.Citation1,Citation2
Studies have shown that majority of teens engage in risky sexual behaviors that may expose them to HIV/AIDS, other sexually transmitted diseases (STDs), or unintended pregnancy.Citation1,Citation3 Several theoretical frameworks have been applied to develop intervention programs to protect young individuals from contracting HIV.Citation4,Citation5 While most intervention programs were designed to target individual-level factors, such as increasing an individual’s knowledge and ability to use a condom during sex, factors from a social context can play a significant role in behavioral change as well. For example, by applying the social cognitive theory, Jemmott et al found that AIDS knowledge, intention, and self-efficacy were associated with the target population’s condom use.Citation4 Walter et al’s school-based intervention to improve schoolchildren’s knowledge of HIV infection, guided by a health-belief model, resulted in youth having more confidence to use a condom during sex, fewer sexual partners, and lower probability of contracting other STDs.Citation5 However, Moberg and PiperCitation6 proposed that although providing school-based prevention programs benefited youth by encouraging them to stay sexually abstinent and providing adequate knowledge on HIV infection and condom use, the influence of community and family could modify the effectiveness of the prevention programs. Consequently, the natural influence of family members, peers, and the community has a large effect on a child/adolescent, and thus are essential factors to consider when providing interventions for adolescents.
Since the eighties, the Centers for Disease Control and Prevention has implemented several programs to bridge the gap between public health and education to minimize the influence of STDs/HIV on young people.Citation7 For instance, the Division of Adolescent and School Health was established in 1988 to promote a friendly learning environment that would allow students to gain health knowledge and skills.Citation7 A well-designed class-curricula program – Bringing High-Quality HIV and STD Prevention to Youth in Schools – was implemented to reduce the rate of STDs, pregnancy, and risky sexual behaviors related to substance abuse in 2010.Citation8 However, the impact of prevention programs seems to be limited, considering the fact that young people aged 13–24 years had the second-highest HIV-diagnosis rate.Citation1 The persisting high infection rate among young AAs indicates that while a majority of young people may have benefited from the intervention programs in their 13–18 years, maintaining the intervention effect and reducing HIV incidence obviously remains a challenge.Citation1
Parts of these challenges have been recognized as the unique cultural, economic, and social issues associated with AA communities. For instance, it has been reported that low socioeconomic status, drug and alcohol use, and low acceptance of homosexuality have increased the level of difficulty in lowering the high HIV-infection rate among AAs.Citation1,Citation3,Citation9–Citation12 In addition, unbalanced family structure in AA families is extremely common. This may help weaken family functions, making it difficult to provide buffers against adverse influence from teens’ social contexts.Citation13–Citation16 For example, a significant association between risky sexual behavior and youth in single-parent households has been reported.Citation14 Also, young AA girls from families with no fathers tend to have early sexual debuts; this association is even stronger for young girls living in low-income single-mother households.Citation15 These reports underscore the importance of identifying the etiological processes that place AAs at risk of engaging in HIV-related risk behaviors during their adolescence.
Because of the interference between protective and risk processes, it is important to understand the associations between the processes and adolescent behaviors. By studying risk and protective processes independently, a researcher can over- or underestimate the impact of social contexts and draw wrong assumptions from the incomplete information.Citation17,Citation18 Therefore, to reach more accurate conclusions, a study must attempt to evaluate the risk and protective processes taking place within and between these different contexts, while simultaneously addressing the influence of youth-development processes. Ecodevelopmental theory provides a useful way of integrating the multiple interacting contexts and processes that affect human development.Citation14,Citation19–Citation21 Essentially, it posits that understanding risk and protective factors for adolescent problem behaviors requires a thorough examination of the natural variants of developmental processes, as well as careful consideration of the social systems within which the risk, protection, and behaviors occur.Citation14,Citation19–Citation21
The ecodevelopmental framework has been applied in behavioral studies of adolescents on substance use, delinquent behavior, HIV-related risk behaviors, and depression, with the majority of the research focusing on young Hispanic and/or Latino populations.Citation22–Citation26 For instance, the ecodevelopmental framework has been used to develop a family-centered intervention program that helps Hispanic immigrant parents to build good parenting skills, strengthen parent–adolescent relationships, and contribute to reducing the risk of problem behaviors among second-generation Hispanic youth.Citation22 Cordova et al examined the effects of family-functioning trajectories on sexual risk behaviors and STDs among AA adolescents in a recent study.Citation26 They reported that the synergistic impact from high family conflict and low family support on adolescent trajectories disrupted adolescent sexual behavioral development and predisposed them to HIV and STD infection.Citation26 However, their study focused mainly on family functioning, and not the potential processes in adolescents’ social contexts. To our knowledge, none of the previous studiesCitation26–Citation29 considered all the social systems within which the risk, protection, and behavior occur among AA adolescents. Therefore, our current study is an attempt to address this gap by emphasizing the importance of family function and interactions among risk and protective processes from an ecodevelopmental perspective among AA adolescents.
Ecodevelopmental theory: a contextual framework for examining STD/HIV-risk behavior
Adolescence is a transition stage from childhood to adulthood when youth begin to develop stronger self-identity and self-esteem to direct their own lives and behaviors.Citation30,Citation31 During this period, while contextual domains, such as family and school, continue to exert strong influences on adolescent development, the peer domain also becomes increasingly salient.Citation21,Citation32–Citation36
The ecodevelopmental theory presented by Szapocznik and Coatsworth,Citation37,Citation38 which is an extended socioecological model that emphasizes the structure, organization, integration, and function of young adults’ social ecology over time, has been suggested as an alternative approach for studying young adult behavior from a developmental perspective. Similarly to the socioecological model, these social systems of an adolescent can be represented by a set of nested systems, including the microsystem, mesosystem, exosystem, and macrosystem. Unlike the socioecological model, however, the ecodevelopmental theory emphasizes the importance of family function and interactions among risk and protective processes from a developmental perspective.
The microsystem, the most proximal for the developing child, consists of the settings in which the child directly participates, and includes family, peers, school, and neigh-borhood systems. Among all domains of the microsystem, the most powerful social influence on adolescents is family. Previous studiesCitation20,Citation21,Citation39–Citation41 have shown that good bonding and communication between parents and young individuals delay the age of the adolescent’s sexual debut, reduce the likelihood of risky sexual behaviors, and lower the risk of contracting STDs/HIV. Other social contexts around the young individuals, such as peers and people in the neighborhood, also play an essential role in modifying the young individuals’ sexual behavior.Citation34,Citation42–Citation47 In fact, the norms created by peers and the safety of the neighborhood have increasing influence compared to family members on the adolescent’s behavioral development as the individual gets older.
The mesosystem does not include the child, but instead represents the relations among domains of a microsystem that influence the child indirectly (eg, parent–peer or parent–school relationships and interactions). The mesosystem is composed of all relationships developed in the microsystem and the sequencing effects of those relationships on adolescents. Domains of the mesosystem include parental involvement in their children’s schools and parental monitoring for their children’s peers. A stronger parent–child bond can prevent the young individual from picking up risky behaviors and lower the risk of contracting STDs/HIV.Citation33,Citation40,Citation48,Citation49
The exosystem is external, and influences the child indirectly through the effect on other family members (eg, parental social support networks, sibling, and gang involvement).Citation36,Citation50–Citation54 For example, a support system for low-income parents will help them to overcome financial difficulties and function as better parents for teenagers.Citation36,Citation50,Citation51,Citation55 The parent-support system is directly associated with parents, but the influence from the parent-support system indirectly affects adolescents through parenting functions.Citation55 Similarly, parents’ personal values can be modified by their experience and culture of the workplace, which in turn could gradually affect a child’s value. AA women’s attitudes, values, and beliefs have been reported to have significant influence on adolescents’ sexual and reproductive decision making.Citation56 For instance, among AAs, it has been reported that older generations, especially grandmothers, did not talk about contraceptives, because of the conservative environment they were raised. This indirectly influenced their daughters’ and granddaughters’ sexual and reproductive decisions.Citation56
Finally, the macrosystem is the outermost layer that envelops the microsystem, mesosystem, and exosystem. It is defined as society’s broad ideological, political, social, and cultural patterns, which may include cultural influence on behaviors and expectations, as well as political and economic impacts on individuals and families.Citation57,Citation58 The principles defined by the macrosystem have a cascading influence throughout the interactions of all other layers. For example, immigrant parents might have acculturative stress, and the acculturation differences between parents and young adults can have an adverse influence on the parenting function.Citation59,Citation60 Therefore, by implication, previous studies have proved that the ecodevelopmental framework might serve as an essential guide for researchers to appraise protective and risk processes from social contexts, and understand the direct and indirect influences on the target behavior of the youth.
Study hypotheses
This study aimed to develop an ecodevelopmental model that specifically examines the protective and STD/HIV-risk processes associated with young AAs’ social contexts. The following three hypotheses were tested in this study. The first hypothesis stated that the father and the mother have different parental influences on an adolescent’s social contexts and behaviors. The second hypothesis stated that the condition of an adolescent’s dwelling unit is determined by the parents’ socioeconomic status, which in turn significantly affects the adolescent’s health-related sexual risk behavior. The third hypothesis stated that the influence of peers and parents is bidirectional, meaning that while parental influence can reduce the influence of peers, conversely peers’ influence can also diminish the influence of parents.
Subjects and methods
Survey design and participants
The study was a retrospective data analysis conducted using data from the National Longitudinal Study of Adolescent Health (Add Health).Citation61,Citation62 The Add Health study was carried out from 1994/1995 to 2008 to survey the same group of adolescents and their parents, and comprised four waves of data covering social, emotional, physical, and health domains of each participant, who were cluster-sampled to represent the national population of the US.Citation61,Citation62 The first wave of Add Health data was used in this study, and comprised 1,619 records of AA adolescents with average age 16±1.8 years (range 12–21 years). A total of 57 variables from the respondents’ family, neighborhood, school, friendship, peer-group, and romantic relationship domains were identified from 2,799 variables and used to develop the hypothesized ecodevelopmental model. Sampling weights were applied in the data analysis as appropriate to represent all young AAs in the US.
Measures
The measures in the study included background information on the potential respondents, STD/HIV-related sexual risk behavior as the outcome, and four systems (micro-, meso-, exo-, and macrosystems) in the ecodevelopmental framework. The background information of potential respondents was comprised of the age, sex, sexual orientation, information related to biological parents, HIV test, HIV or other STD infections, and sexual behaviors (sex experience, age at sexual debut, condom/birth-control use during sex).
Reliability of constructs
The reliability of items and latent constructs were computed using McDonald’s ω-coefficients.Citation63–Citation68 The McDonald’s ω-coefficient is a measure of the reliability of a homogeneous test, computed based on the parameter estimates of a single-factor model. The coefficient has the advantage of taking into account the strength of associations between items and constructs, as well as item-specific measurement errors. The ω-coefficient is thus a composite of congeneric items measuring a common dimension (ie, factor or latent construct). The w-coefficients for the present study’s outcome measure and the social systems were computed within the factor-analysis framework.
Outcome: STD/HIV-related sexual risk behavior
The latent outcome variable for STD/HIV-related sexual risk behavior was developed using the variables early sex debut, low frequency of condom use, low HIV-test rate, and sex in exchange for money, each of which has been associated with higher risk of contracting HIV in previous studies.Citation69–Citation72 STD/HIV-related sexual risk behavior was used in this study as a measure of the adolescents’ sexual health status. The ω-estimate for AA adolescent’s STD/HIV-related sexual risk behavior was 0.923.
Microsystem
A total of six critical domains were included in the examination of the microsystem: parents’ function, religion, school, peers, parents’ attitude toward the adolescent’s sexual life, and condition of the dwelling unit. From a developmental perspective, parents are the most fundamental element in a child/adolescent’s behavioral development; therefore, parents’ functioning and attitude toward the adolescent’s sex life were both carefully examined to determine their impacts on the adolescent’s STD/HIV-related sexual risk behavior. The parents’ functions were measured through a combination of the adolescent’s feelings of love, caring, closeness, and communication from their parents. The parents’ attitudes toward the adolescent’s sex life were measured through the parents’ approval of sexual behavior. Since it was assumed that a father and mother play different roles in the development of their offspring, father and mother functioning were tested separately in this study. The ω-coefficients for father’s and mother’s love were 0.966 and 0.94, respectively. Other domains (such as school, peers, religion, and condition of dwelling unit) were also analyzed to determine their influence on the adolescent’s sexual behavior development. The ω-coefficients for the school, peer, and religion domains were 0.617, 0.773, and 0.71, respectively.
Mesosystem
Mesosystem processes were operationalized as parental involvement and influence on the adolescent’s social domains. The parents’ involvement was measured through the frequency with which they talked about school grades, projects, and expectations of educational performance with their children, and thus it tended to interfere with the social contexts of the youth. Because the foundation of the mesosystem is built from the relationships developed within it, examination of the mesosystem also includes the assessment of the influence or modification of factors therein. For example, domains in the microsystem (including the closeness of the parent–child relationship, interactions between the youth and personnel at school, the adolescent’s friends, and safe living environment) that directly interact with young people would be modified by the level of parents’ involvement. Finally, the study separately tested each parent’s degree of involvement in the adolescent’s social environment and the consequent influence on the adolescent’s STD/HIV-related sexual risk behavior. The ω-coefficients for the father’s and mother’s involvements were 0.974 and 0.816, respectively.
Exosystem
The exosystem in our study was represented by the mother’s and father’s attitudes toward the adolescent’s use of birth control. Because these were both observed variables, no latent construct or corresponding measurement model was developed, and thus an ω-coefficient was not necessary. The two variables were examined independently in our study.
Macrosystem
Macrosystem processes were operationalized as the socioeconomic status of parents, and took into consideration whether or not they received public assistance/welfare. Occupations, weekly work hours, and work location (at home or outside) of the father and the mother were examined separately. Whether or not parents received public assistance was also included in the evaluation of the socioeconomic status of parents to depict the impact of the government and policy on parents and indirect impact of parenting function and involvement on the adolescent’s behavioral development (father’s socioeconomic status, ω = 0.926; mother’s socioeconomic status, ω = 0.879).
Data analysis
Three steps were taken to study the direct and indirect protective and risk processes associated with the hypothesized model. First, a measurement model was estimated to ascertain the feasibility of collapsing multiple indicators into single latent variables alongside the observed variables using confirmatory factor analysis in Mplus package 7.3.Citation73 The final measurement model was developed from the confirmatory factor analysis, which included 57 observed variables and eleven latent variables that represented the micro-, meso-, exo-, and macrosystems.
Following this, the hypothesized structural equation model aimed at specifying the directional and nondirectional relationships among latent and observed structural variables was determined. The fit of the model was evaluated primarily in terms of the comparative fit index (CFI), which compares the hypothesized model to a null model with no paths or latent variables, the Tucker–Lewis index (TLI), which is relatively unaffected by sample size and adjusts for parsimony, and the root-mean-square error of approximation (RMSEA), which estimates the extent to which the covariance matrix specified in the model deviates from the covariance matrix observed in the dataCitation74–Citation78 CFI values of 0.9 or greater, RMSEA of 0.05 or less, and a TLI values of 0.9 or higher were indicators of good model fit. The cutoff values of the fit indices were consistent or similar to those in previous structural equation modeling studies.Citation72,Citation79
The structural equation model was finalized using the maximum-likelihood and the robust maximum-likelihood estimators.Citation67 The former provided the indices of model fitness and estimates of direct effects, while the latter was applied to accommodate departures from normality that were evident for some variables. Furthermore, to account for the clustering of respondents within schools and regions, the “TYPE = COMPLEX” command was employed in Mplus.Citation67 The bootstrapping estimation was applied to obtain accurate confidence intervals of 90% for indirect mediation effects.Citation80
Ethics statement
This study received approval from the University of Houston Committee for the Protection of Human Subjects. The study used an existing secondary data set with no identifiers linking individuals’ information to the data, and received an exempt status approval from the committee.
Results
Sample characteristics
The background information of the target population is presented in . Among the young AA respondents, 61.8% were 14–17 years old and 34.9% were 18 years and older. Females and males accounted for 49.8% and 50.2% of the target population, respectively, while 2.5% of the target population constituted a sexual minority (homosexual or bisexual). The majority of the participants (82%) lived with their biological mother compared to those that lived with their biological father (32%). Although 83% of the respondents acknowledged the importance of religion in their life, only 42.9% and 15.5% of them attended religious services with their mother and father, respectively.
Table 1 Characteristics of the study population: African-American adolescents (n = 1,619)
The HIV-infection rate in our sample population was low (0.19%). About 5.6% of the study population admitted that they had had at least one STD. Among participants who had had sex (about 55%), 60% of them reported condom use during their first sexual encounter and the same percentage of the population used condoms during recent sexual encounters. The majority of them (85%), however, used other birth-control methods. About 44.5% of the adolescents studied reported no sexual debut, but among those who reported sexual debut, 10.8% of them had their first sex at age 16–20 years, while 34.6% of the participants had their first sex at age 10–15 years.
Confirmatory factor analysis – measurement models
A summary of fitness indices for the measurement models is presented in and described in the following sections for the STD/HIV-related sexual risk-behavior outcome and each ecodevelopmental system. The corresponding factor loading for each latent variable is given in Table S1.
Table 2 Summary of fitness for measurement models
STD/HIV-related sexual risk-behavior measurement model
The measurement model of the STD/HIV-related sexual risk-behavior outcome had the following model-fitness indices: χ2 (df) = 257.959 (15) = 17.2; RMSEA = 0.1 (0.09–0.111); CFI = 0.9; and TLI = 0.859. Five of seven variables had factor loading of 0.79–0.92, while the other two variables had low factor loading: having an HIV test (−0.25) and exchanging drugs/money for sex (0.08). However, considering the importance and contribution of these two factors to STD/HIV infection, we decided to retain them in the model.
Microsystem measurement model
The measurement model of the microsystem had the following model-fitness indices: χ2 (df) = 4,530.389 (309) = 14.66; RMSEA = 0.092 (0.09–0.094); CFI = 0.756; and TLI = 0.723. Factor loading for the adolescents’ characteristics was as follows: feeling of love from mother, 0.09–0.96; feeling of love from father, 0.4–0.99; parents’ attitude toward sexual behavior, 0.4–0.85; schools’ microsystem, 0.29–0.75; religion microsystem, 0.32–0.87; and peer microsystem, 0.2–1.7.
Mesosystem measurement model
The measurement model of the mesosystem had the following model fitness indices: χ2 (df) = 2,029.69 (119) = 17.06; RMSEA = 0.1 (0.096–0.103); CFI = 0.834; and TLI = 0.81. Factor loading for mother’s involvement was 0.34–0.9, while that for father’s involvement was 0.58–0.98.
Macrosystem measurement model
The measurement model of the macrosystem had the following model-fitness indices: χ2 (df) = 807.044 (25) = 32.28; RMSEA = 0.139 (0.131–0.147); CFI = 0.811; and TLI = 0.728. Factor loading for mother’s socioeconomic status was 0.23–0.97, and that for father’s socioeconomic status was 0.54–0.98.
Final measurement model for all systems
The final measurement model for all systems had the following model-fitness indices: χ2 (df) = 4,339.069 (1,100) = 3.94; RMSEA = 0.043 (0.041–0.044); CFI = 0.924; and TLI = 0.916. This result indicates that although we did not have great model fitness for each system, the overall measurement model for all the systems showed reasonable model fitness after controlling for residual covariance associated with the different measures.
Structural equation model – hypothesized model
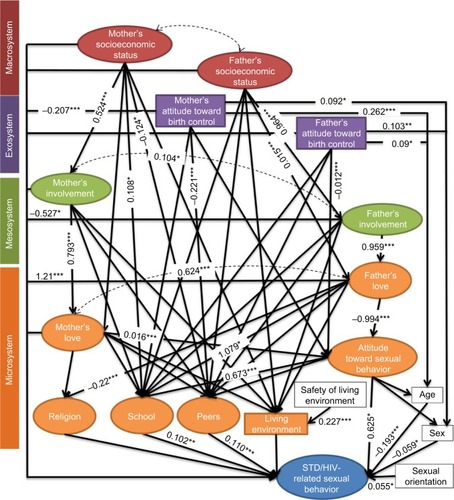
presents the hypothesized model of STD/HIV-related sexual risk behavior among young AAs. The hypothesized model-fitness indices were: χ2 (df) = 6,182.583 (1,446) = 4.28; RMSEA = 0.045 (0.044–0.046); CFI = 0.894; and TLI = 0.884.
Figure 1 Structural equation modeling of STD/HIV-related risk factors among African-American adolescents.
Abbreviations: STD, sexually transmitted disease; CFI, comparative fit index; TLI, Tucker–Lewis index; RMSEA, root-mean-square error of approximation.
Direct effects
Microsystem on STD/HIV-related sexual risk behavior
Among all domains in the microsystem, feeling of love from the father (β = 1.21, P<0.0001), school (β = 0.102, P = 0.002), and peers (β = 0.11, P = 0.001) directly influenced the adolescent’s STD/HIV-related sexual risk behavior. Their STD/HIV-related sexual risk behavior was significantly associated with age (β = −0.193, P<0.001), sex (β = −0.059, P = 0.031), and sexual orientation (β = 0.055, P = 0.047), but not with the condition of dwelling unit (β = 0.034, P = 0.202).
Mesosystem on microsystem and STD/HIV-related sexual risk behavior
The AA father’s involvement (β = −0.527, P = 0.04) had an adverse influence on the adolescent’s STD/HIV-related sexual risk behavior compared to mother’s involvement (β = 0.046, P = 0.543), which had no statistically significant impact on adolescent STD/HIV-related sexual risk behavior. The feeling of love from the father was associated with school (β = 1.079, P = 0.02) and religion in the microsystem of the adolescent (β = 0.22, P<0.0001), but the love from the mother did not have any significant impact statistically (β = 0.151, P = 0.179; β = 0.076, P = 0.063). Feeling parents’ love was majorly dependent on the level of parents’ involvement, and the influence of both father and mother involvement were highly significant (father, β = 0.959, P<0.0001; mother, β = 0.793, P<0.0001) determinants of adolescent STD/HIV-related sexual risk behavior.
Exosystem on individual characteristics and STD/HIV-related sexual risk behavior
The mother’s attitude toward the adolescent’s use of birth control (β = −0.207, P<0.001) significantly impacted the adolescent’s STD/HIV-related sexual risk behavior, while the father’s attitude did not (β = 0.014, P = 0.657). The father’s attitude toward the adolescent’s use of birth control was associated with the adolescent’s sex (β = 0.1, P = 0.002), while the mother’s attitude toward the use of birth control was mainly related to the adolescent’s age (β = 0.262, P<0.001). The parents’ attitudes toward having sex at an early age were not always influenced by their attitudes toward the adolescent’s use of birth control (father, β = −0.061, P<0.001; mother, β = 0.004, P = 0.117).
Macrosystem on microsystem, mesosystem, and STD/HIV-related sexual risk behavior
The school domain was significantly associated with the mother’s socioeconomic status (β = 0.108, P = 0.031), but not with the father’s socioeconomic status (β = −0.076, P = 0.564). Similarly, the influence of the peer domain was significantly affected by the mother’s socioeconomic status (β = −0.124, P = 0.046), but not influenced by the father’s socioeconomic status (β = 0.113, P = 0.439). The level of parents’ involvement in their children’s lives was affected by their socioeconomic status, and the associations for both father and mother were highly statistically significant (father, β = 0.964, P<0.001; mother, β = 0.524, P<0.001).
Indirect effects
The indirect influences, tested with a bootstrapping procedure (), indicated that the father plays a more important role in adolescent’s STDs/HIV-related sexual risk behavior when compared to the mother. First, higher socioeconomic status of the father tended to reduce the risk of young AAs contracting STDs/HIV by increasing the feeling of love from the father (father’s socioeconomic status, β = 0.626, P = 0.03; mother’s socioeconomic status, β = 0.022, P = 0.385). Second, more father involvement benefited the adolescent’s sexual health status through reinforcing the feeling of fatherly love (father’s involvement, β = 1.263, P<0.001; mother’s involvement, β = 0.032, P = 0.632).
Table 3 Summary of direct and indirect effects toward STDs/HIV-related sexual risk behavior among African-American adolescents
Hypotheses
The result that supports the first hypothesis showed that the father played a much more important role in the adolescent’s STD/HIV-related sexual risk behavior, both directly and indirectly, than the mother. The direct impact indicates that when an adolescent feels more love from a father, the adolescent also tends to have better sexual health status (β = 1.21, P<0.001) and thus a lower risk of contracting STDs/HIV. On the other hand, the influence of adolescent feeling of love from the mother was not statistically significant (β = 0.024, P = 0.787). Although increased father involvement directly reduced the adolescent’s sexual health status (β = −0.527, P = 0.04), the indirect processes of the father’s involvement significantly improved the adolescent’s sexual health status through increased feelings of love from the father (β = 1.263, P<0.0001). Therefore, father involvement generally resulted in better sexual health status of the adolescent (total effect, β = 0.736). In the macrosystem, while the father’s higher socioeconomic status (β = 0.626, P = 0.03) was indirectly associated with the adolescent’s better health-related sexual risk behavior, the indirect association of the mother’s socioeconomic status (β = 0.022, P = 0.385) was not statistically significant. Therefore, our study found that factors associated with the father tend to have a greater influence on the adolescent’s sexual behavior patterns than those associated with the mother.
The test for the second hypothesis indicated that the condition of a dwelling unit did not have any significant direct associations with the socioeconomic status of the parents (father, β = 0.071, P = 0.534; mother, β = 0.058, P = 0.165) or the young AA’s STD/HIV-related sexual risk behavior (β = 0.034, P = 0.202). However, the safety of the living environment was highly associated with the condition of the dwelling unit (β = 0.227, P<0.001). Therefore, the second hypothesis was rejected.
Findings from our analysis upheld the third hypothesis, which focused on the microsystem. Peers had a statistically significant direct impact on the adolescent’s STD/HIV-related sexual risk behavior (β = 0.11, P = 0.001). For instance, when peers had knowledge of the rhythm and withdrawal methods of birth control and also used condoms correctly, the adolescents were more likely to use a condom and/or birth-control measures. Secondly, the mother tended to have a more noticeable influence toward peer microsystems than a father did. It was observed that higher socioeconomic status of the mother reduced the peers’ influence more (β = −0.124, P = 0.046), but this pattern was not observed with higher socioeconomic status of the father (β = 0.113, P = 0.439). Similarly, a negative attitude toward adolescent’s birth control from the mother was associated with lower peer influence (β = −0.221, P<0.001), while the father’s negative attitude toward the adolescent’s birth-control use had no significant impact on peer influence (β = 0.029, P = 0.536). In terms of peer influence and parental functions, we found that there were tendencies for a slight weakening of parents’ functions toward adolescent health-related sexual risk behavior in the different pathways: the love of the mother, the involvement of the father, and the socioeconomic status of the father. However, these results were not statistically significant (P>0.05). Consequently, we did not find any potential mechanisms of peer–parent interactions in our study, and as such the second part of hypothesis 3 was rejected.
Discussion
This study utilized the ecodevelopmental framework, which incorporates both protective and risk processes into one model, to explore our understanding of STD/HIV-related sexual risk behavior among AA adolescents. Findings from our study support the assertion that the influence from the microsystem is salient in modifying STD/HIV-related sexual risk behavior in AA adolescents. We noted significant associations among adolescents’ misconduct behaviors and school bonding and peer influence, which support previous studies.Citation23,Citation32,Citation34,Citation42,Citation81 Specifically, not only did we find that more closeness with school personnel reduced the likelihood of adolescent STD/HIV-related behavior, but also perception about peer knowledge of contraceptive use was associated with adolescent exhibition of less risky sexual behavior and a better health status. Furthermore, adolescents’ feelings of receiving more love from their father were associated with lower odds of STD/HIV-related sexual risk behavior, implying that increased father involvement in single-parent children’s livesCitation82–Citation84 could help reduce the adolescent’s risky sexual behaviors. An adolescent’s feeling of love from the father may bring about a stronger bond with both parents, resulting in less distress, often caused by family-structure interference and subsequent development of internal or external behavioral problems with adolescents.Citation41,Citation85
The indirect influence from meso-, exo-, and macrosystems on adolescent STD/HIV-related sexual risk behavior assert that the family/parents’ function tends to modify other microsystems with no direct influence on the adolescent’s sexual behavior. It has been reported in previous studies that parent/family function is indirectly associated with risky adolescent sexual behavior through being a member of “adolescent crowds” or emotional contexts in which the adolescent is more vulnerable to influence.Citation33,Citation48 Our current study supports these assertions. For example, the socioeconomic status of the mother had significant effects on the adolescent’s school and peer domains, while the socioeconomic status of the father had insignificant influence on the adolescents’ social contexts. Moreover, our results indicated that a mother’s attitude toward an adolescent’s contraceptive adoption was significantly associated with the adolescent’s use of contraception, and thus supports one of the findings from a review conducted by Commendador.Citation49 Although the influence of a father’s attitude was not evaluated in the review, our study proved that a father’s attitude toward an adolescent’s contraceptive adoption had no significant impact on the actual use of contraceptives by the adolescent. Furthermore, we found that the mother tends to be the main support element associated with an adolescent’s living and social contexts, a situation that may be a reflection of the high prevalence of single-mother households in AA communities.
We noted a strong negative attitude toward adolescent birth-control use from the mothers in our study was associated with increases in risky adolescent sexual behavior. Although previous studiesCitation86–Citation90 have emphasized that AA fathers also show strong negative attitudes toward the use of birth control, ours did not. Therefore, an adolescent under the influence of an imbalanced family structure is more likely to be affected by a mother than a father, even if his/her attitude toward birth control is not necessarily due to behavioral involvement from the mother. Because AA girls rely more on their mothers than their peers for guidance on contraceptive use,Citation56 they tend not to adopt contraceptive use. Since the value of contraceptive use can be passed on down the generations through the mother, it is suggested that critical consideration be given to the acceptance of birth-control use among AAs when developing intervention programs to increase HIV prevention in this group.
Sexual orientation minorities (homosexuals and bisexuals) were found to be more associated with STD/HIV-related sexual risk behavior than heterosexuals. This finding supports previous reports from other research and surveillance reports.Citation3,Citation91–Citation93 Members of sexual orientation minorities suffer higher psychological distressCitation93 due to their sexual orientation and are more likely to use drugs and alcohol.Citation9,Citation10,Citation91,Citation94,Citation95 In addition, homophobiaCitation96 and discriminationCitation10 in AA communities tend to create environments less friendly to the sexual orientation minority, resulting in sexual orientation minorities delaying disclosure and being at higher risk of contracting STDs/HIV.Citation11,Citation52,Citation97 The implication of this finding is that more efforts are needed to create lesbian/gay/bisexual/transgender-friendly social environments in AA communities as a prevention/intervention strategy against STD/HIV infection and transmission.
Our current study found that the condition of the dwelling unit did not play any significant role in young AA STD/HIV-related sexual risk behavior, although several published studies have indicated that the living environmentCitation16,Citation46,Citation98,Citation99 is associated with adolescent sexual behavior development. It is possible that the inclusion of numerous variables associated with STD/HIV infection to develop an unbiased latent outcome variable may have compromised the separate associations between the condition of the dwelling unit and the main outcome variable. However, our finding tends to complement the outcomes from Bauermeister et al,Citation43 where it was reported that young AAs living in disadvantaged neighborhoods tend to have early sex debuts and use condoms consistently. They believed that young adolescents living in low-income neighborhoods were more afraid that unwanted pregnancies and STDs/HIV could put them in worse social and financial situations than their current conditions.Citation43
Finally, our study did not find peers to have any statistically significant influence on parenting functions. These findings seem to suggest that adolescents are more inclined to replace the relationships they have with their parents with those they have with their peers. This may be a reflection of the evolution of parenting behaviors over the course of their adolescence and/or a shift in response to the specifics of a young person’s peer relationships. From a developmental perspective, young individuals gradually develop independence and autonomy during adolescence while also strengthening bonds of individual–peer affiliation to replace parent–child ties.Citation31 The potential mechanism of this process is explained by Iacovetta,Citation100 indicating that adolescents undergoing new and various experiences desire higher intensity of love and belonging with their peers during the adolescence stage. On the other hand, measures of parent and peer influence have been reported to have independent effects on sexual risk-taking, but did not moderate the effects of self-regulation and risk proneness.Citation101 Our current study findings thus support the existence of multiple sources of influence on adolescents’ STD/HIV-related sexual risk and protective behaviors. They also suggest that effective intervention programs for this group should include individual-level factors and social contexts, with provisions made for the natural variations of the developmental processes.
Study limitations and strengths
The results of our study should be interpreted in light of several limitations. First, this study used retrospective cross-sectional data. The role of the ecodevelopmental processes associated with HIV-risk behaviors was not examined over time, as only one wave of the survey was used. Consequently, we were not able to examine the developmental element of the ecodevelopmental theory, and thus no causal or directional inferences can be drawn from the results. Secondly, the use of self-reported measures in our study may have led to social desirability and recall biases, with possible resultant effects on our estimates. In addition, the application of sample weights in the analysis may have contributed to reducing the selection bias and variance. The third limitation is that very specific constructs were used to assess the systemic processes associated with ecodevelopmental theory, and given the theory’s breadth, it might have been possible to choose different variables at each level; we do not know how this might have affected the results.
Despite these limitations, the strengths of our study lie in the application of the ecodevelopmental theory to test empirically the interplay of risk and protective processes associated with STD/HIV-risk behaviors among AA adolescents. Although the main data were gathered from adolescents and parents, the use of independent reports of family functioning, school bonding, academic competence, peer relationships, and antisocial or delinquent behaviors complemented these sources, and enhanced the reliability and generalizability of our findings. The pattern of results obtained in our study is consistent with the theoryCitation26,Citation37,Citation59,Citation102 and past research using well-validated measures,Citation72,Citation79 and thus provides fair tests of our study’s hypotheses.
Conclusion and practical implications
By examining the microsystem, mesosystem, exosystem, and macrosystem in the ecodevelopmental theory, we found factors that contribute to increasing or decreasing odds of adolescent participation in STD/HIV-related sexual risk behavior. The results from our study may have important implications for designing and implementing preventive interventions to prevent or reduce HIV-risk behavior and other health outcomes among AA adolescents. It is important to intervene in adolescents’ ecodevelopmental contexts to prevent problematic adolescent outcomes, because both self and context may provide maximal protection against risks of problem behaviors, depression, and their sequelae (eg, substance use, suicidal ideation).Citation3,Citation27,Citation94,Citation102–Citation106 While adolescence is a time of growing independence, our study findings suggest that parents should continue to be involved in their adolescents’ lives and monitor and guide them through the challenges of this period. Evidence from our study indicates that parents are ideal change agents who have a large influence on their children’s risk and protective processes in such contexts as school and peer domains.
Overall, any intervention aimed at maximal protection against STD/HIV-related risk among AA adolescents should adopt both self- and context-based concepts and strategies that promote positive functioning in the family, school, and peers in the microsystem.Citation107 In addition, intervention programs should generally be designed with the input of parents, adolescents, and key community members (such as school principals or teachers) who play a major role in the life of the adolescent. Our study particularly uncovers the significant roles that fathers play in the sexual behavior of AA adolescents at several levels, and thus supports the idea of developing father-specific interventions based on the potential mechanisms identified in our models.
Despite the fact that biomedical tools, including post-exposure prophylaxis, preexposure prophylaxis, and HIV self-testing kits, have been shown to be effective in reducing HIV incidence, some challenges related to access to care and HIV testing still remain. Successful HIV prevention and treatment requires evidence-based approaches that combine biomedical strategies, and structural and behavioral interventions (combination prevention) that are socially and culturally appropriate for the population or community being prioritized.Citation108,Citation109 Given that combination prevention relies on evidence-based outcomes and operates on different levels – eg, individual, relationship, community, societal – we believe that the hypothesized ecodevelopmental model in the present study will be essential in the design of effective prevention programs that examine the chain of relationships and social contexts associated with STD/HIV-risk behaviors among AA adolescents in the US.
Supplementary material
Table S1 Factor loading for each latent variable
Disclosure
This article is the full version of a study titled “Modeling ecodevelopmental context of STDs/HIV risk and protective behaviors among African American adolescents”. An excerpt of this research was initially presented as a poster with the same title at the International Society for Pharmacoeconomics and Outcome Research (ISPOR) 21st Annual International Meeting held at the Washington Hilton, Washington, DC, US, May 21–25, 2016.Citation110 The authors report no conflicts of interest in this work.
References
- Centers for Disease Control and PreventionDiagnoses of HIV Infection in the United States and Dependent Areas, 201426AtlantaCDC2015
- Centers for Disease Control and PreventionHIV surveillance – adolescents and young adults2014 Available from: https://www.cdc.gov/hiv/pdf/statistics_surveillance_adolescents.pdfAccessed April 11, 2017
- KannLMcManusTHarrisWAYouth risk behavior surveillance – United States, 2015MMWR Surveill Summ2016651174
- JemmottJBJemmottLWSpearsHHewittNCruz-CollinsMSelf-efficacy, hedonistic expectancies, and condom-use intentions among inner-city black adolescent women: a social cognitive approach to AIDS risk behaviorJ Adolesc Health1992135125191390819
- WalterHJVaughanRDAIDS risk reduction among a multiethnic sample of urban high school studentsJAMA19932707257308336374
- MobergDPPiperDLThe Healthy for Life project: sexual risk behavior outcomesAIDS Educ Prev1998101281489573435
- Centers for Disease Control and PreventionDASH – Strategic Plan for Fiscal Years 2015–2020AtlantaCDC2016
- Centers for Disease Control and PreventionBringing High-Quality HIV and STD Prevention to Youth in SchoolsAtlantaCDC2014
- D’AugelliARHershbergerSLLesbian, gay, and bisexual youth in community settings: personal challenges and mental health problemsAm J Community Psychol1993214214488192119
- FieldsELBogartLMGalvanFHWagnerGJKleinDJSchusterMAAssociation of discrimination-related trauma with sexual risk among HIV-positive African American men who have sex with menAm J Public Health201310387588023488499
- Hightow-WeidmanLBPhillipsGJonesKCOutlawAYFieldsSDSmithJCRacial and sexual identity-related maltreatment among minority YMSM: prevalence, perceptions, and the association with emotional distressAIDS Patient Care STDs201125Suppl 1S39S4521688988
- VanDevanterNDuncanABurrell-PiggottTThe influence of substance use, social sexual environment, psychosocial factors, and partner characteristics on high-risk sexual behavior among young black and Latino men who have sex with men living with HIV: a qualitative studyAIDS Patient Care STDs20112511312121235387
- AndersonSAFlemingWMLate adolescents’ identity formation: individuation from the family of originAdolescence1986217857963825661
- CicchettiDTothSLA developmental psychopathology perspective on child abuse and neglectJ Am Acad Child Adolesc Psychiatry1995345415657775351
- DodgeKAPettitGSA biopsychosocial model of the development of chronic conduct problems in adolescenceDev Psychol20033934937112661890
- McLoydVCSocioeconomic disadvantage and child developmentAm Psychol1998531852049491747
- MagnussonDCasaerPLongitudinal Research on Individual Development: Present Status and Future PerspectivesCambridgeCambridge University Press1993
- ThornberryTPLizotteAJKrohnMDFarnworthMJangSJDelinquent peers, beliefs, and delinquent behavior: a longitudinal test of interactional theoryCriminology1994324783
- CompasBEConnor-SmithJKSaltzmanHThomsenAHWadsworthMECoping with stress during childhood and adolescence: problems, progress, and potential in theory and researchPsychol Bull20011278712711271757
- BeanRABarberBKCraneDRParental support, behavioral control, and psychological control among African American youth: the relationships to academic grades, delinquency, and depressionJ Fam Issues20062713351355
- GrotevantHDCooperCRIndividuation in family relationships: a perspective on individual differences in the development of identity and role-taking skill in adolescenceHum Dev1986282100
- CoatsworthJDPantinHSzapocznikJFamilias Unidas: a family-centered ecodevelopmental intervention to reduce risk for problem behavior among Hispanic adolescentsClin Child Fam Psychol Rev2002511313212093012
- CordovaDHuangSArzonMFreitasDMalcolmSPradoGThe role of attitudes, family, peer and school on alcohol use, rule breaking and aggressive behavior in Hispanic delinquent adolescentsOpen Fam Stud J20114384522473467
- PradoGHuangSMaldonado-MolinaMAn empirical test of ecodevelopmental theory in predicting HIV risk behaviors among Hispanic youthHealth Educ Behav2010379711420130302
- CordovaDCiofuAParkKParra-CardonaJRHoltropKCervantesRThe role of intrapersonal and ecodevelopmental factors in the lives of Latino alternative high school youthJ Ethn Cult Divers Soc Work20142314816725067923
- CordovaDHeinzeJEMistryRSalas-WrightCPZimmermanMAEcodevelopmental trajectories of family functioning: links with HIV/STI risk behaviors and STI among black adolescentsDev Psychol2016521115112727253262
- PerrinoTGonzález-SoldevillaAPantinHSzapocznikJThe role of families in adolescent HIV prevention: a reviewClin Child Fam Psychol Rev20003819611227063
- LockeTFNewcombMDCorrelates and predictors of HIV risk among inner-city African American female teenagersHealth Psychol20082733734818624598
- WeineSMHoffmanYWareNSecondary migration and relocation among African refugee families in the United StatesFam Process201150274621361922
- GeXCongerRDElderGHPubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptomsDev Psychol20013740441711370915
- SteinbergLAdolescence8th edNew YorkMcGraw-Hill2007
- MaddoxSJPrinzRJSchool bonding in children and adolescents: conceptualization, assessment, and associated variablesClin Child Fam Psychol Rev20036314912659450
- BrownBBMountsNLambornSDSteinbergLParenting practices and peer group affiliation in adolescenceChild Dev1993644674828477629
- WallaceSAMillerKSForehandRPerceived peer norms and sexual intentions among African American preadolescentsAIDS Educ Prev20082036036918673068
- WeicholdKWiesnerMFSilbereisenRKChildhood predictors and mid-adolescent correlates of developmental trajectories of alcohol use among male and female youthJ Youth Adolesc20144369871624009026
- LevittMJGuacci-FrancoNLevittJLConvoys of social support in childhood and early adolescence: structure and functionDev Psychol199329811818
- SzapocznikJCoatsworthJDAn ecodevelopmental framework for organizing the influences on drug abuse: a developmental model of risk and protectionGlantzMDHartelCRDrug Abuse: Origins and InterventionsWashingtonAmerican Psychological Association1999331366
- BronfenbrennerUThe Ecology of Human Development: Experiments by Nature and DesignCambridge, MAHarvard University Press1979
- FlewellingRLBaumanKEFamily structure as a predictor of initial substance use and sexual intercourse in early adolescenceJ Marriage Fam199052171181
- NathansonMBairdAJemailJFamily functioning and the adolescent mother: a systems approachAdolescence1986218278413825665
- OmanRFVeselySFAspyCBYouth assets and sexual risk behavior: the importance of assets for youth residing in one-parent householdsPerspect Sex Reprod Health200537253115888400
- BauermeisterJAElkingtonKBrackis-CottEDolezalCMellinsCASexual behavior and perceived peer norms: comparing perinatally HIV-infected and HIV-affected youthJ Youth Adolesc2009381110112219636775
- BauermeisterJAZimmermanMACaldwellCHNeighborhood disadvantage and changes in condom use among African American adolescentsJ Urban Health201188668321161414
- CarlsonJABracyNLSallisJFSociodemographic moderators of relations of neighborhood safety to physical activityMed Sci Sports Exerc2014461554156325029166
- CubbinCSantelliJBrindisCDBravemanPNeighborhood context and sexual behaviors among adolescents: findings from the national longitudinal study of adolescent healthPerspect Sex Reprod Health20053712513416150660
- HoganDPKitagawaEMThe impact of social status, family structure, and neighborhood on the fertility of black adolescentsAm J Sociol198590825855
- LamisDAWilsonCKTarantinoNLansfordJEKaslowNJNeighborhood disorder, spiritual well-being, and parenting stress in African American womenJ Fam Psychol20142876977824707802
- SieverdingJAAdlerNWittSEllenJThe influence of parental monitoring on adolescent sexual initiationArch Pediatr Adolesc Med200515972472916061779
- CommendadorKAParental influences on adolescent decision making and contraceptive usePediatr Nurs20103614715617020687307
- BrodyGHFlorDLMaternal resources, parenting practices, and child competence in rural, single-parent African American familiesChild Dev1998698038169680686
- BrondoloEGalloLCMyersHFRace, racism and health: disparities, mechanisms, and interventionsJ Behav Med2009321819089605
- RomerDBlackMRicardoISocial influences on the sexual behavior of youth at risk for HIV exposureAm J Public Health1994849779858203696
- MontgomerySBHydeJDe RosaCJGender differences in HIV risk behaviors among young injectors and their social network membersAm J Drug Alcohol Abuse20022845347512211360
- SpohrSASuzukiSMarshallBTaxmanFSWaltersSTSocial support quality and availability affects risk behaviors in offendersHealth Justice20164227054059
- ParentJJonesDJForehandRCuellarJShoulbergEKThe role of coparents in African American single-mother families: the indirect effect of coparent identity on youth psychosocial adjustmentJ Fam Psychol20132725226223398615
- HarrisAL“I got caught up in the game”: generational influences on contraceptive decision making in African-American womenJ Am Assoc Nurse Pract20132515616524218203
- CastroFGMarsigliaFFKulisSKellisonJGLifetime segmented assimilation trajectories and health outcomes in Latino and other community residentsAm J Public Health201010066967620167890
- SimpkinsSDDelgadoMYPriceCDQuachAStarbuckESocioeconomic status, ethnicity, culture, and immigration: examining the potential mechanisms underlying Mexican-origin adolescents’ organized activity participationDev Psychol20134970672122545831
- BacioGAEstradaYHuangSMartínezMSardinasKPradoGEcodevelopmental predictors of early initiation of alcohol, tobacco, and drug use among Hispanic adolescentsJ Sch Psychol20155319520826054814
- FarrellyCCordovaDHuangSEstradaYPradoGThe role of acculturation and family functioning in predicting HIV risk behaviors among Hispanic delinquent youthJ Immigr Minor Health20131547648322532299
- HarrisKMHalpernCTWhitselEThe national longitudinal study of adolescent to adult health: research design2009 Available from: http://www.cpc.unc.edu/projects/addhealth/designAccessed April 11, 2017
- HarrisKMUdryJRNational Longitudinal Study of Adolescent Health (Add Health), 1994–2008Chapel Hill, NCCarolina Population Center2014
- McDonaldRPThe theoretical foundations of principal factor analysis, canonical factor analysis, and alpha factor analysisBr J Math Stat Psychol197023121
- McDonaldRPGeneralizability in factorable domains: “domain validity and generalizability”Educ Psychol Meas1978387579
- McDonaldRPFactor Analysis and Related MethodsNew YorkLawrence Erlbaum Associates1985
- McDonaldRPTest Theory: A Unified TreatmentNew YorkLawrence Erlbaum Associates1999
- DunnTJBaguleyTBrunsdenVFrom alpha to omega: a practical solution to the pervasive problem of internal consistency estimationBr J Psychol201410539941224844115
- Trizano-HermosillaIAlvaradoJMBest alternatives to Cronbach’s alpha reliability in realistic conditions: congeneric and asymmetrical measurementsFront Psychol2016776927303333
- CookseyECRindfussRRGuilkeyDKThe initiation of adolescent sexual and contraceptive behavior during changing timesJ Health Soc Behav19963759748820311
- KannLKinchenSShanklinSLYouth risk behavior surveillance: United States, 2013MMWR Suppl2014631168
- WhitakerDJMillerKSMayDCLevinMLTeenage partners’ communication about sexual risk and condom use: the importance of parent-teenager discussionsFam Plann Perspect19993111712110379427
- RotchfordKStrumAWWilkinsonDEffect of coinfection with STDs and of STD treatment on HIV shedding in genital-tract secretions: systematic review and data synthesisSex Transm Dis200027524324810821594
- MuthéLKMuthénBOMplus User’s Guide: Statistical Analysis with Latent Variables7th edLos AngelesMuthén and Muthén2012
- BentlerPMComparative fit indexes in structural modelsPsychol Bull19901072382462320703
- BentlerPMBonettDGSignificance tests and goodness of fit in the analysis of covariance structuresPsychol Bull198088588606
- HuLTBentlerPMCutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternativesStruct Equ Modeling19996155
- BrowneMWCudeckRAlternative ways of assessing model fitSociol Methods Res199221230258
- SteigerJHStructural model evaluation and modification: an interval estimation approachMultivariate Behav Res19902517318026794479
- ErcanIYaziciBSigirliDEdizBKanIExamining Cronbach alpha, theta, omega reliability coefficients according to sample sizeJ Mod Appl Stat Meth20076291303
- MallinckrodtBAbrahamWTWeiMRussellDWAdvances in testing the statistical significance of mediation effectsJ Couns Psychol200653372378
- LopezBWangWSchwartzSJSchool, family, and peer factors and their association with substance use in Hispanic adolescentsJ Prim Prev20093062264119949868
- ChoiJKJacksonAPFathers’ involvement and child behavior problems in poor African American single-mother familiesChild Youth Serv Rev201133689704
- EllisBJBatesJEDodgeKADoes father absence place daughters at special risk for early sexual activity and teenage pregnancy?Child Dev20037480182112795391
- LangleyCFather knows best: paternal presence and sexual debut in African-American adolescents living in povertyFam Process20165515517025582779
- SnyderARMcLaughlinDKFindeisJHousehold composition and poverty among female-headed households with children: differences by race and residenceRural Sociol200671597624
- WeisbordRGBirth control and the black American: a matter of genocide?Demography1973105715904614988
- AllenJEAn appearance of genocide: a review of governmental family-planning program policiesPerspect Biol Med197720300306846827
- BogartLMWagnerGGalvanFHBanksDConspiracy beliefs about HIV are related to antiretroviral treatment nonadherence among African American men with HIVJ Acquir Immune Defic Syndr20105364865519952767
- CaronSBirth control and the black community in the 1960s: genocide or power politics?J Soc Hist19983545569
- DarityWATurnerCBFamily planning, race consciousness and the fear of race genocideAm J Public Health197262145414595085509
- UenoKSexual orientation and psychological distress in adolescence: examining interpersonal stressors and social support processesSoc Psychol Q200568258277
- MillettGAPetersonJLWolitskiRJStallRGreater risk for HIV infection of black men who have sex with men: a critical literature reviewAm J Public Health2006961007101916670223
- RussellSTJoynerKAdolescent sexual orientation and suicide risk: evidence from a national studyAm J Public Health2001911276128111499118
- RyanCHuebnerDDiazRMSanchezJFamily rejection as a predictor of negative health outcomes in white and Latino lesbian, gay, and bisexual young adultsPediatrics200912334635219117902
- RyanCRussellSTHuebnerDDiazRSanchezJFamily acceptance in adolescence and the health of LGBT young adultsJ Child Adolesc Psychiatr Nurs20102320521321073595
- JusterRPSmithNGOuelletESindiSLupienSJSexual orientation and disclosure in relation to psychiatric symptoms, diurnal cortisol, and allostatic loadPsychosom Med20137510311623362500
- PoteatVPMereishEHDigiovanniCDKoenigBWThe effects of general and homophobic victimization on adolescents’ psychosocial and educational concerns: the importance of intersecting identities and parent supportJ Couns Psychol20115859760921859187
- AidalaACrossJEStallRHarreDSumartojoEHousing status and HIV risk behaviors: implications for prevention and policyAIDS Behav2005925126516088369
- BrookDWRubenstoneEZhangCMorojeleNKBrookJSEnvironmental stressors, low well-being, smoking, and alcohol use among South African adolescentsSoc Sci Med2011721447145321492977
- IacovettaRGAdolescent-adult interaction and peer-group involvementAdolescence1975103273361199838
- RaffaelliMCrockettLJSexual risk taking in adolescence: the role of self-regulation and attraction to riskDev Psychol2003391036104614584983
- Wilkinson-LeeAMZhangQNunoVLWilhelmMSAdolescent emotional distress: the role of family obligations and school connectednessJ Youth Adolesc20114022123020013149
- SchwartzSJCoatsworthJDPantinHPradoGSharpEHSzapocznikJThe role of ecodevelopmental context and self-concept in depressive and externalizing symptoms in Hispanic adolescentsInt J Behav Dev200630359370
- KalichmanSCCareyMPJohnsonBTPrevention of sexually transmitted HIV infection: a meta-analytic review of the behavioral outcome literatureAnn Behav Med19961861524203638
- KhanMRKaufmanJSPenceBWDepression, sexually transmitted infection, and sexual risk behavior among young adults in the United StatesArch Pediatr Adolesc Med200916364465219581548
- Ramirez-VallesJZimmermanMANewcombMDSexual risk behavior among youth: modeling the influence of prosocial activities and socioeconomic factorsJ Health Soc Behav1998392372539785696
- PradoGPantinHSchwartzSJLupeiNSSzapocznikJPredictors of engagement and retention into a parent-centered, ecodevelopmental HIV preventive intervention for Hispanic adolescents and their familiesJ Pediatr Psychol20063187489016049264
- MartinezOWuELevineECIntegration of social, cultural, and biomedical strategies into an existing couple-based behavioral HIV/STI prevention intervention: voices of Latino male couplesPLoS One2016113e015236127028873
- Rotheram-BorusMJSwendemanDChovnickGThe past, present, and future of HIV prevention: integrating behavioral, biomedical, and structural intervention strategies for the next generation of HIV preventionAnnu Rev Clin Psychol2009514316719327028
- LiYMgbereOAbughoshSChenHCuccaroPEssienEJModeling ecodevelopmental context of STDs/HIV risk and protective behaviors among African American adolescentsValue Health2016193A85