
Abstract
Background
HIV-related chronic pain has emerged as a major symptom burden among people living with HIV (PLHIV). Physical therapy (PT) has been shown to be effective as a non-pharmacological method of chronic pain management in the general population; however, there is a gap in research examining the role of PT for chronic pain among PLHIV.
Materials and methods
This study examined the effect of PT on self-reported pain scores and pain medication usage in PLHIV enrolled in a multidisciplinary HIV clinic. Data were collected via reviews of patient medical records within a certain timeframe. Data were gathered from patient charts for two points: initial PT encounter (Time 1) and PT discharge or visit ≤4 months after initial visit (Time 2).
Results
Subjects who received PT during this timeframe reported decreased pain (65.2%), elimination of pain (28.3%), no change in pain (15.2%), and increased pain (6.5%). Three-quarters of the subjects reported a minimal clinically important difference (MCID) in pain score, and more than half reported a decrease in pain score over the MCID. Subjects showed a trend of decreasing pain medication prescription and usage during the study period.
Conclusion
Results of the current study indicate that in this sample, PT intervention appears to be an effective, cost-effective, non-pharmacological method to decrease chronic pain in PLHIV.
Keywords:
Introduction
HIV-related chronic pain has emerged as a major symptom burden among people living with HIV (PLHIV): recent research indicates that chronic pain prevalence among PLHIV may be as high as 85%.Citation1–Citation3 It is well documented in the literature that PLHIV have increased rates of chronic pain, which causes considerable disability and negatively affects quality of life.Citation4–Citation6 Pain in this patient population has been associated with up to ten times greater odds of functional impairment and with decreased patient retention in HIV primary care.Citation7 Pain is undertreated and more complex to manage in the HIV patient population for a number of reasons, including complex antiretroviral drug regimens, contraindications for commonly used analgesics, and higher rates of comorbid psychiatric illness and substance abuse.Citation7,Citation8 PLHIV are at greater risk for addiction and misuse of opioids than HIV-negative peers; PLHIV are often exposed to opiates during their HIV care, and drug overdose is a common cause of non-AIDS death among PLHIV.Citation8
Research shows that even when PLHIV receive pharmaceutical pain treatment, they are still likely to persistently report high levels of pain, suggesting that current strategies to manage pain among PLHIV are inadequate.Citation9 Physical therapy (PT) has been widely shown to be a safe, effective approach to chronic pain management in the general population, and preliminary research suggests that PT can be an effective part of the medical management of PLHIV when addressing impairments such as musculoskeletal and neurological issues and deconditioning.Citation10–Citation14 However, there is a gap in research specifically examining PT’s role in pain management for PLHIV. Given the significant need for effective, nonnarcotic pain management for PLHIV, a multidisciplinary approach to HIV management must be utilized, with an increasing role for PT in the continuum of care for PLHIV as well as those with AIDS-related impairments.Citation15 Identification of cost-effective, safe approaches to pain for PLHIV will aid in the development of improved therapeutic options to treat chronic pain in this patient population.
Studies in the area of HIV and chronic pain have suggested non-opioid analgesics and psychosocial therapies as alternatives to opioids; however, there is a gap in research examining pain outcomes of PLHIV in a cohort treated by PT for pain-related diagnoses. This study examined pain outcomes – measured by self-reported pain scores and analgesic use – of PLHIV who had received PT for pain management in an HIV clinic. The study aimed to address PT as a viable primary alternative to pharmacological pain therapy among PLHIV with chronic pain diagnoses.
Materials and methods
This project investigated the role of PT – specifically progressive exercise and manual therapy – in pain outcomes of PLHIV enrolled at the Ponce de Leon Center – a large, multidisciplinary HIV clinic located in metropolitan Atlanta, GA, USA. The Ponce de Leon Center is one of the largest and most comprehensive HIV clinics in the US and serves the most vulnerable and at-risk populations in Atlanta. Metropolitan Atlanta was an ideal location for this study, as the burden of HIV disease is high: Atlanta currently ranks fifth in the nation for total number of adults and adolescents living with HIV.Citation16 The Ponce de Leon Center has approximately 6,000 enrolled HIV-positive patients, and approximately 90% of these patients pertain to ethnic or racial minority groups. It is home to several NIH-funded clinical trials and studies and is a study site for the NIH Center for AIDS Research (CFAR). The NIH Center for AIDS Research has been open since the early 1990s; however, PT has only been available since 2014. Weekly PT is onsite, and patients who are enrolled at the NIH Center for AIDS Research may be referred for services. PT is also part of the multidisciplinary Palliative Care Program, where patients see various disciplines within one visit.
Inclusion criteria for this study included: 1) HIV-positive adults’ age ≥18 years, enrolled at the Ponce de Leon Center; 2) patients who received PT services at the Ponce de Leon Center between June 1, 2014 and December 31, 2015; and 3) patients who had a pain diagnosis in their PT referral.
PT interventions comprised individually tailored progressive exercise, manual therapy, therapeutic taping, and patient education. Subjects were seen weekly during the timeframe by a single provider, with an average of eight visits. PT charts at the Ponce de Leon Center are paper records kept within a secure filing system. Charts were reviewed at the clinic in a private room and selected based on the abovementioned inclusion criteria. Charts were selected only if the patient was referred to PT for a pain diagnosis.
Subjects’ pain scores were recorded upon two points in time: initial PT evaluation (Time 1) and PT discharge date or a visit at least 4 months from Time 1 (Time 2). PT treatment course was based on a patient’s individual rehabilitation needs. The timeframe of June 1, 2014 – December 31, 2015 was chosen because PT services at the Ponce de Leon Center have been available on a weekly basis since May 2014.
The study is a secondary data analysis with data from the Center for AIDS Research (CFAR) HIV Data Registry at the Grady Health System’s Ponce de Leon Center. The Registry contains data from the electronic medical records (EMR) of patients who received medical treatment at the Ponce de Leon Center. Pain scores were gathered from charts using the numerical rating scale (NRS), a standard, 0–10 pain self-reporting scale that is the most widely implemented clinical scale for pain screening and has been shown to provide sufficient discriminative power for patients to describe their pain intensity.Citation17 In this study, pain scores were obtained from the PT at the beginning and end of each PT treatment session. Pain medication prescription and usage were also recorded. Data were recorded for pain medications that were prescribed to patients and that patients took with or without a prescription. Patients were queried at each PT visit whether or not they were taking pain medications and whether or not these medications were prescribed. Analgesic prescriptions were verified through electronic charts where all prescriptions were recorded. The classes of medications collected were opiate analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), and acetaminophen-based medications. PT interventions described in charts were categorized into the following categories: progressive strengthening, manual therapies such as soft tissue massage and mobilization, passive stretching, gait training, and patient education. Data collected at Time 1 (initial encounter) included birth date, gender, body mass index (BMI), CD4 count, viral load, pain score, ICD-9 diagnoses, pain medication prescriptions, and usage. Pain diagnoses and their corresponding ICD-9 codes consisted of generalized pain, neck pain, pain in joint, shoulder pain, ankle pain, hip pain, lumbago, thoracic pain, pain in limb, headache, osteoarthritis, and unspecified idiopathic peripheral neuropathy. These specific diagnoses and ICD-9 codes were chosen based upon discussion with medical providers at this clinic about the most common pain diagnoses that would warrant a PT referral in this patient population. Data collected at Time 2 were BMI, CD4 count, viral load, pain score, ICD-9 diagnoses, pain medication prescriptions, and usage. Data from Time 1 and Time 2 were compared for change in all abovementioned listed areas. This study was approved by the Emory University Institutional Review Board, who ensures that ethical standards of the responsible committee on human experimentation are adhered to. The IRB deemed that consents were not required, as data collection was performed by retrospective chart review only, with identifying characteristics and personal health information removed.
Results
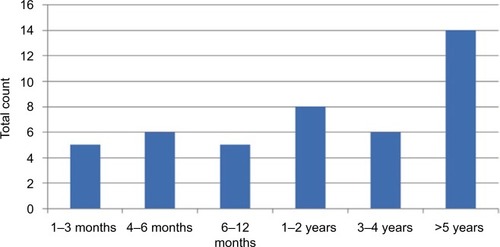
A total of 46 patient charts met all inclusion criteria. Among the subjects, 60.9% were male (n=28) and 39.1% were female (n=18). None of the subjects were identified as transgender. The majority (73.3%, n=33) of patients were identified as Black/African American, 22.2% (n=10) were identified as White, 2.2% (n=1) were identified as Hispanic/Latino, and one subject’s race was not identified. Subjects’ ages ranged from 22 to 67 years, with a median age of 51 years and an average age of 47 years. Subjects’ BMI ranged from 16.9 to 55.26 kg/m2. BMI categories are defined in the following range: <18.5= underweight to ≥30.0= obese. Referring PT diagnoses are listed in . The pain diagnoses referred to PT included the following: low back pain (32.6%, n=15), lower extremity pain (23.9%, n=11), upper extremity pain (23.9%, n=11), cervical pain (15.2%, n=7), hip pain (10.9%, n=5), deconditioning (10.9%, n=5), generalized pain (4.3%, n=2), and neurological pain (2.2%, n=1). Deconditioning – while not a pain diagnosis – was included as it is often concurrent with pain/weakness and is a frequent reason for PT referral. At the time of initial PT evaluation (Time 1), the most commonly reported duration of pain was >5 years (30.4%, n=14). Duration of pain reported by subjects is detailed in .
Figure 1 PT diagnosis.
Abbreviation: PT, physical therapy.
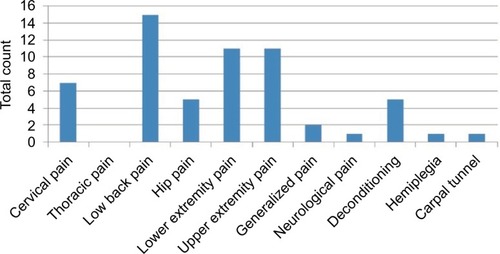
Figure 2 Duration of pain.
Abbreviation: PT, physical therapy.
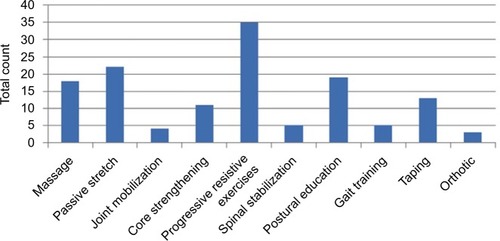
Over the duration of treatment, the most commonly applied intervention was progressive resistive exercises (77.8%, n=35), followed by passive stretch (48.9%, n=22), postural education (42.2%, n=19), massage (40.0%, n=18), therapeutic taping (28.9%, n=13), and core strengthening (24.4%, n=11). Other treatments included gait training (11.1%, n=5), spinal stabilization (11.1%, n=5), joint mobilization (8.9%, n=4), and usage of orthotics (6.7%, n=3; ).
Figure 3 PT interventions provided.
Abbreviation: PT, physical therapy.
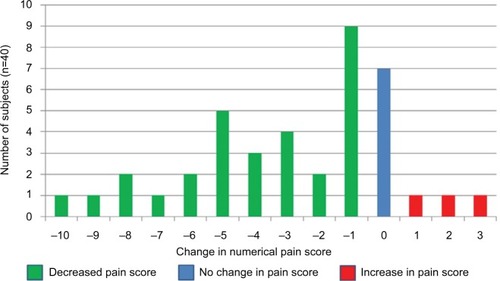
During the study period, the majority of study subjects reported a decrease in pain (65.2%, n=30), followed by becoming completely pain free (28.3%, n=13). A smaller percentage reported no change (15.2%, n=7) or an increase in pain (6.5%, n=3) after the intervention. The majority of subjects reported a decrease in pain score over the minimal clinically important difference (MCID), with a decrease in pain of >15% or ≥1 point ().
Figure 4 Change in pain score (Time 1–Time 2).
Study subjects reported an overall trend of decreased pain medication usage in all pain medication categories. Patients were queried about medication usage at each PT visit, and medication usage was compared at Time 1 and Time 2. shows the numbers of patients taking pain medications and the change in pain medication usage during the study period. Change in pain medication was defined as an increase or decrease in analgesic use from Time 1 to Time 2. Of subjects who were prescribed opioids at Time 1, 5.3% of subjects did not take their medication, 24.4% took it regularly/as prescribed, and none took it only as needed. Out of all subjects who were prescribed NSAIDs at Time 1, 48.7% of subjects did not take their medication, 24.4% took it regularly, and 11.4% took it only as needed. Out of all subjects who were prescribed acetaminophen at Time 1, 80.0% of subjects did not take their medication, 4.4% took it regularly, and 2.2% took it as needed. Out of all subjects who were prescribed neuropathic medications at Time 1, 66.7% of subjects did not take their medication, 17.8% took it regularly, and none took it as needed.
Figure 5 Percentage of patients on pain medications.
Abbreviation: NSAIDs, nonsteroidal anti-inflammatory drugs.
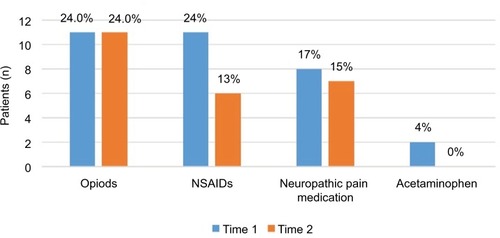
Pain medication prescription was also recorded for patients during Time 2, with overall decreased pain medication prescription and usage compared to Time 1 with the exception of opioids. Out of all subjects who were prescribed opioids at Time 2, 5.3% of subjects did not take their medication, 23.9% took it regularly, and none took it as needed. At Time 2, subjects reported the exact same numbers of opioid usage as in Time 1. Out of all subjects who were prescribed NSAIDs at Time 2, 56.5% of subjects did not take their medication, 13.0% took it regularly, and none took it as needed. Out of all subjects who were prescribed acetaminophen at Time 2, 73.9% of subjects did not take their medication, none took it regularly, and 2.2% took it as needed. Out of all subjects who were prescribed neuropathic medications at Time 2, 63.0% of subjects did not take their medication, 15.2% took it regularly, and none took it as needed ().
Discussion
Research shows that even when PLHIV receive pharmaceutical pain treatment, they are still likely to persistently report high levels of pain. This suggests that current strategies to manage pain in the HIV patient population are inadequate. Given the multi-morbidities experienced frequently among PLHIV, pain management must be included within the overall plan of care for this population. Pain management is a major tenet in the scope of PT practice; however, there is a lack of published research regarding pain management through PT within the HIV-positive patient population. This study reviewed PT patient charts in a large, urban HIV clinic to assess the change over time in self-reported MCID pain scores and pain medication usage. Results reveal that more than half (52.5%) of subjects reported a decrease in pain score over the MCID, with a change of ≥2 points. In all pain medication categories except opioids, subjects reported a decrease in medication usage during and after their PT intervention period. It is noteworthy, however, that opioid usage did not increase during the study period, but rather remained the same at 24% of subjects taking opioids both at Time 1 and Time 2. Given the highly addictive qualities of opioid analgesics, more research is warranted specifically examining opioid usage in a larger cohort of PLHIV with chronic pain.
Our results reveal that in this sample, PT interventions appear to correlate with decreased self-reported pain scores within a sample of PLHIV with pain diagnosis. As the increased chronicity of HIV leads to increased life expectancies, it is inevitable that PLHIV will increasingly present clinically with chronic pain. The decreased pain reports and decrease in analgesic use among subjects who received PT in this study indicate that HIV providers should consider PT to treat pain within this patient population.
This study was conducted via chart review of subjects in an HIV clinic situated in an urban, low-income region in the Southeastern US. This study should be repeated using a larger sample of PLHIV in different settings, in different geographical regions. In this sample of patients enrolled at a multidisciplinary HIV clinic, PT interventions appeared to be an effective, non-pharmacological method to decrease chronic pain in PLHIV. Given the small sample size and the fact that the cohort had positive access and compliance to antiretroviral drugs, these conclusions may be taken modestly. However, our results reveal that PT may have a solid role within a multidisciplinary HIV clinic and should be considered in the overall pain management of this patient population.
As the national opioid epidemic continues to present a major public health threat, it is crucial to consider non-pharmacological methods of pain control. As PLHIV continue to present clinically with both age and HIV-related comorbidities, physical therapy will occupy a key role in decreasing pain and improving the quality of life of this patient population.
Acknowledgments
The author would like to acknowledge Grady Health System and the Ponce de Leon Center. This study received support from the Emory Center for AIDS Research (P30 AI050409).
Disclosure
The authors report no conflicts of interest in this work.
References
- ParkerRSteinDJJelsmaJPain in people living with HIV: a systematic reviewJ Int AIDS Soc20141711879
- MerlinJSWestfallAORaperJLPain, mood, and substance abuse in HIV: implications for clinic visit utilization, ART adherence, and virologic failureJ Acquir Immune Defic Syndr201261216417022766967
- LeeKAGayCPortilloCJSymptom experience in HIV-infected adults: a function of demographic and clinical characteristicsJ Pain Symptom Manage200938688289319811886
- MerlinJSCenLPraestgaardAPain and physical and psychological symptoms in ambulatory HIV patients in the current treatment eraJ Pain Symptom Manage201243363864522115794
- MiaskowskiCPenkoJMGuzmanDMattsonJEBangsbergDRKushelMBOccurrence and characteristics of chronic pain in a community-based cohort of indigent adults living with HIV infectionJ Pain20111291004101621684218
- MerlinJSWestfallAOChamotEPain is independently associated with impaired physical function in HIV-infected patientsPain Med201314121985199324119077
- MerlinJSWestfallAOChamotEQuantitative evaluation of an instrument to identify chronic pain in HIV-infected individualsAIDS Res Hum Retroviruses201531662362725693683
- GreenTCMcGowanSKYokellMAPougetERRichJDHIV infection and risk of overdose: a systematic review and meta-analysisAIDS201226440341722112599
- TsaoJSteinJDobalianAPain, problem drug use history, and aberrant analgesic use behaviors in persons living with HIVPain20071331–312813717449182
- HanadaEYEfficacy of rehabilitative therapy in regional musculoskeletal conditionsBest Pract Res Clin Rheumatol200317115116612659826
- WrightASlukaKANonpharmacological treatments for musculoskeletal painClin J Pain2001171334611289087
- PullenSPakJPietonCSaundersMShelusMWebsterLPhysical therapy as an adjunct treatment for people living with HIV/AIDS: a provider needs assessment-phase IIJ Allied Health2014433e45e5225194067
- PullenSGilmanKHuntKPhysical therapy as an adjunct treatment for people living with HIV/AIDS: an allied health perspectiveJ Allied Health2014432e11e1724925040
- PullenSDChigboNNNwigweECChukwukaCJAmahCCIduSCPhysiotherapy Intervention as a complementary treatment for people living with HIV/AIDSHIV AIDS (Auckl)201469910724936132
- RockstrohJGuaraldiGDerayGHIV and the body: a review of multidisciplinary managementHIV Med201011suppl 218
- Centers for Disease Control and Prevention [webpage on the Internet]HIV Surveillance Report, 2013252015 Available from: http://www.cdc.gov/hiv/library/reports/surveillance/Accessed October 29, 2015
- JensenMPTurnerJARomanoJMWhat is the maximum number of levels needed in pain intensity measurement?Pain19945833873927838588