
Abstract
Background
Despite the increased availability of antiretroviral therapy (ART), its success depends on a high level of adherence to a life-long antiretroviral therapy. However, the extent and factors associated with adherence to ART are not well known, especially in the current study setup. Therefore, this study aimed to assess the level of adherence and associated factors among children on ART in Northwest, Ethiopia.
Methods
A retrospective follow-up study was conducted on human immunodeficiency virus (HIV)-infected children receiving ART at South Gondar public hospitals. Children receiving ART from January 1, 2015, to November 30, 2020, were included in the study. A computer-generated simple random sampling technique was employed. The data were entered into the EpiData version 3.1 and analyzed by STATA 14 statistical software. Bivariable logistic regression was fitted for each predictor variable. Moreover, those variables having a p-value ≤0.25 in bivariate analysis were fitted into a multivariable logistic regression model. P-value <0.05 was used to declare significance.
Results
A total of 363 HIV-infected children were involved in the study. From 363 HIV-infected children, the level of adherence to ART was found to be 78.2%, 95% CI (73.6, 82.2). TB co-infection [adjusted odds ratio (AOR) = 3.8, 95% CI (1.41, 10.1)], short duration on ART (AOR = 3.4, 95% CI (1.60, 7.20)), treatment failure (AOR = 10.2, 95% CI (3.95, 26.2)), and Zidovudine containing ART regimen (AOR = 3.5, 95% CI (1.1, 10.9)) were significant predictors of poor adherence.
Conclusion
The current study showed that the level of adherence to ART was found to be low TB co-infection, short duration of ART, Zidovudine-containing ART regimen, and treatment failure were found to be significantly associated with poor adherence. Further studies on adherence rate and its determinants with multiple adherence measurements using prospective and multicenter studies were recommended.
Background
Human Immunodeficiency Virus (HIV) is an RNA virus that causes Acquired Immune Deficiency Syndrome (AIDS),Citation1 which remains the leading cause of morbidity and mortality throughout the world.Citation2 Globally, 37.7 million people were living with HIV in 2020, 1.5 million new HIV infections, and 680.000 AIDS-related deaths.Citation3 Of this, HIV infection among children constitutes 4.5% of people living with HIV and 6.87% of total HIV/AIDS deaths.Citation3
About 50% of children living with HIV/AIDS die before the age of 2 years as a result of recurrent opportunistic infections such as pneumonia, diarrhea, malnutrition, and malaria.Citation4 According to the Summary of the global HIV epidemic (2019), Africa contributes 67.6% of the total HIV-infected people and 63.7% of the total HIV/AIDS deaths.Citation5
As one of the African countries, the case in Ethiopia is not different. In 2016, there were 62.000 children aged <15 years living with HIV, 3800 newly diagnosed cases, and 2.900 deaths.Citation6 The introduction of effective antiretroviral (ART) treatment in the 1990s drastically reduced AIDS-related mortality and morbidity.Citation7 Ethiopia was among the first African countries to introduce ART in 2003 in selected health facilities following the issuance of the National Antiretroviral drugs (ARVS) supply and use policy in 2002.Citation8
Antiretroviral therapy (ART) is a treatment for HIV that combines different types of antiretroviral medications, which should be taken throughout life to increase the length and quality of life for people living with HIV by reduction of the viral load and increase of the level of CD 4 cells.Citation9 The major factor determining the success of HAART is sustainable and optimum adherence to therapyCitation10 as poor adherence increases the risk of virologic failure, viral resistance, and dangerous outcomes such as substance abuse, depression, and spread of infections such as hepatitis.Citation11–Citation14 Any patient who misses more than 3 dosages in a one-month treatment course is considered to have achieved suboptimal adherence which is less than 95%.Citation15
Despite the increased availability of ART, implementation among children 0–14 years faces major challenges due to poor adherence.Citation16,Citation17 Factors associated with pediatrics ART adherence can be related to caregivers, children themselves,Citation14,Citation18–Citation23 socioeconomic,Citation18,Citation19 socio-demographic, and socio-cultural factors,Citation24,Citation25 or service delivery issues,Citation18,Citation19 It is also affected by high pill burden, poor palatability, long-term toxicity,Citation26,Citation27 side effects of ARVs,Citation24–Citation27 ART regimes,Citation14,Citation18–Citation21,Citation25 drug dosing.Citation24,Citation25 Duration on ART,Citation28 the health of the child,Citation29 child knowledge of their HIV status,Citation30 and psychosocial factorsCitation17 have also been associated with pediatric ART adherence Unlike adults, young children rely upon their caregivers for their medicines.Citation18 Moreover, the experience of HIV-related rejections, non-acceptance, stigma, and discrimination minimize the patients’ desire to maintain their optimal levels of health.Citation14
The level of adherence to ART among HIV-infected children varied from 49% to 100% globally.Citation22 Similarly, in Ethiopia, it varied from 34.8%Citation31 to 95.5%Citation32 in Tikur Anbessa and Debre Birhan Referral Hospitals, respectively.
Ethiopia has adopted the 2014 UNAIDS 90-90-90 (90% of PLHIV know their status, 90% of PLHIV who know their status are on treatment (ART) and 90% of PLHIV on treatment have attained viral suppression by 2020) strategy.Citation33 However, only 79-71-87% have been achieved in 2018.Citation34 Although Ethiopia has been working a lot to attain the strategy since adherence is taken a lion’s share to achieve the goal, poor level of adherence was greatly challenged especially in the study area.
Moreover, the risk factors of poor adherence were varied across the countries and the regions. Fortunately, most of the risk factors of poor adherence to ART are modifiable. Result determining the risk factors of poor adherence is a crucial role for intervention to reduce its magnitude and associated complication in the study area. As a result, this study aimed to determine the level of adherence to ART and its associated factors among children receiving ART at South Gondar public Hospitals, 2020.
Materials and Methods
Study Settings and Subjects
A retrospective follow-up study was conducted on HIV-infected children receiving ART at South Gondar public Hospitals. Children receiving ART from January 1, 2015, to November 30, 2020, were included. South Gondar public hospitals are found in Debre Tabor town which is the capital of South Gondar Zone in Amhara Regional State, Northwest Ethiopia. Debre Tabor Town is located 667 and 102 km far from Addis Ababa and Bahir Dar, respectively.Citation35
South Gondar public hospital contained 05 hospitals that provide pediatric ART services. These hospitals are Debre Tabor compressive specialized hospital, Nefas Mewucha District Hospital, Mekane Eyesus District Hospital, Addis Zemen District Hospital, and Andabet District Hospital. As per the 2020 report, the total of HIV-infected children was 1312. The hospitals have a total of 71 Health care providers working at ART.
Source Populations
All HIV-positive children less than 15 years who had been taking ARV and were on follow-up from January 1, 2015, to November 30, 2020, at selected South Gondar public hospitals were the source population.
Study Population
Sampled children less than 15 years who had been taking ARV medications and were on following- from January 1, 2015, to November 30, 2020, at selected South Gondar public hospitals were the study population.
Inclusion Criteria
Children of less than 15 years who had been taking ART for a minimum of one month were included.
Exclusion Criteria
Participants who had incomplete data (that means charts without outcome variables and major explanatory variables) were excluded.
Sample Size Determination and Sampling Procedure
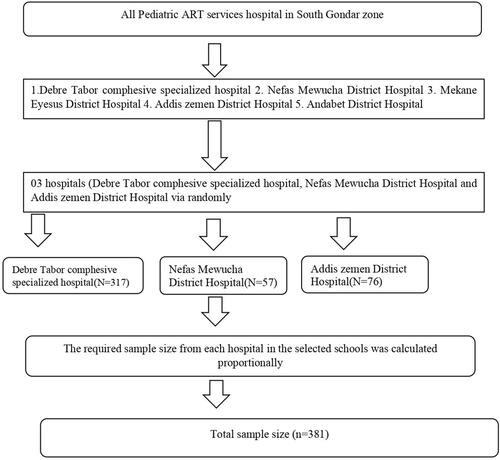
The sample size was calculated by using STATA 14 software of the two-population proportion formula taking the assumptions – 95% confidence level, 80% optimum statistical power, and taking type one error 5%. Taking male as exposure group from a previous study conducted in Mekelle Hospital, EthiopiaCitation36 denoted by q1 (0.82.0) and female non exposed group denoted by q0 (0.92.6), and then the total sample size, after adding 10% as incomplete or inconsistent data, will be 381. The hospitals were categorized into referral and district strata. Then, from the district hospitals stratum, Nefas Mewucha and Mekan Eyesus district Hospitals were selected randomly. From the referral hospital stratum, Debre Tabor specialized compressive specialized hospital was selected since it is the only specialized hospital in South Gondar Zone. Then, the sample size was allocated proportionally for each hospital. A simple random sampling technique was employed through a computer-generated system by taking the ART registration logbook as a sampling frame ().
Figure 1 Schematic presentation of the recruitment and allocation process for adherence to antiretroviral among children receiving ART at South Gondar public Hospitals, Northwest, 2020.
Operational Definitions
Poor adherence was defined as the percentage of drug dosage calculated from the total monthly doses of ART drugs <85%.Citation37
A CD4 count: CD4 below the threshold level was classified based on the age of the child (i.e infants CD4<1500/mm3, 12–35 months <750/mm3, 36–59 months <350/mm3 and ≥5 years <200/mm3).Citation38
Anemia was defined as having a hemoglobin level <10 mg/dl.Citation39
Underweight or stunting was defined as weight for age Z-score < −2 SD for under-five children and BMI for age Z-score < −2 SD for older children.Citation40
Data Collection Procedures
Data were collected using a pretested data abstraction format prepared from the national ART guidelines and by reviewing different kinds of literature. The abstraction tool was designed to collect information including socio-demographic, clinical, and treatment-related characteristics. The data were collected by three BSc nurses and supervised by two MSC pediatrics nurses. The training was given to data collectors and supervisors. The pre-test was done on 5% of the sample size in Addis Zemen district Hospital which is 57 kilometers away from Debre Tabor Town and one of the district hospitals in South Gondar.
Data Processing and Analysis
The data were entered into the EpiData version 3.1 and analyzed by STATA 14 statistical software.
Descriptive and summary statistics are explored through the table and figures. Finally, the outcome level adherence to ART was dichotomized into good or poor.
The bivariable logistic regression model was fitted for each predictor variable. Moreover, those variables having a p-value ≤0.25 in bivariate analysis were fitted into a multivariable logistic regression model. Adjusted odds ratios with 95% confidence interval and p-values were used to measure the strength of association and to identify statistically significant predictors. In multivariable analysis variables having P-value <, 0.05 were considered as significant predictors of poor adherence. The multicollinearity assumption was checked using the standard error and correlation matrix. Besides, Hosmer-Lemeshow statistics and Omnibus tests were performed, and Hosmer-Lemeshow’s test was found to be insignificant (p-value = 0.483). While Omnibus tests were significant (p≤0.01) indicating the model was fitted.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 381 medical records were reviewed among which 18 had incomplete data were excluded. Thus, a total of 363 children were included in the analysis which makes a completeness rate of 95.3%. The mean age of the study participants was 7.34 (±3.4 SD) years, and 196 (54.0%) of them were in the age group of 5–9 years. Nearly half of 186 (51.2%) were males and 184 (50.7%) of children know their HIV status. Besides, 243 (66.9%) of caregivers were married and 52 (41.9%) cannot read and write whereas 99 (27.3%) had completed secondary school ().
Table 1 Socio-Demographic Characteristics of Children Receiving ART at South Gondar Public Hospitals, Northwest, 2020 (n=363)
Clinical and Treatment-Related Characteristics of Children on ART
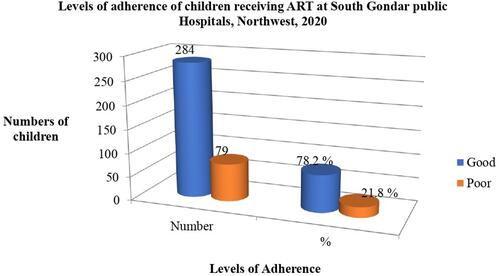
Of 363 HIV-infected children, 186 (51.2%) were underweight, and 263 (72.5%) were WHO stage (I and II). Seventy-one (19.6.3%) and 36 (9.9%) of study participants had a CD4 count below the threshold of and treatment failure, respectively. The majority (81.0%, n = 294) were on CPT users whereas 253 (69.7%) did not take IPT. Fifty-nine (16.3%) and 41 (11.3%) of the participants had anemia (<10 gm/dL) and TB, respectively. Two hundred forty (56.3%) of the study participants were on the Zidovudine-containing regimen and 231 (63.6%) were initiated ART before 2014. Regarding the duration of ART, 167 (46.0%) of study participants were taking ART > 59 months (). Finally, 79 (21.8%) of the study participants had poor adherence ().
Table 2 Clinical Characteristics of Study Participants Receiving ART at South Gondar Public Hospitals, Northwest, 2020 (n=363)
Figure 2 Levels of adherence of children receiving ART at South Gondar public Hospitals, Northwest, 2020.
Factors Associated with Poor Adherence to ART
In the bivariable logistic regression analysis residence, weight for height, hemoglobin level, WHO stages, CD4 counts, regimen type, cotrimoxazole preventive therapy (CPT), treatment failure, TB status, and duration on ART having P value less than 0.25 and fitted into a multivariable logistic regression model. In the multivariable model zidovudine regimen contained at baseline, presence treatment failure, presence of TB co-infection, and duration on ART <36 months were predictors of poor adherence.
The odds of children who were enrolled in zidovudine-containing ART regimen were (AOR=3.5, 95% CI: 1.1–10.9) three folds more likely to be poor adherent than their counterparts. The odds of being poor adherence among HIV-positive children on ART who had TB was around four higher than those who had no TB 3.8 (1.41–10.1) (OR= 3.8, 1.41–10.1). The odds of children on ART with treatment failure was around 10 times higher to be poor adherence than those who had no treatment failure (AOR= 10.2, 3.95–26.2); similarly, HIV-positive children on ART with <36 months on ART [OR = 3.4 (95% CI: 1.60, 7.20)] were more likely to poorly adhere to their ART >59 months in the follow-up period ().
Table 3 Bivariable and Multivariable Logistic Regression Analysis on Levels of Adherence Among Children Receiving ART at South Gondar Public Hospitals, Northwest, 2020 (n=363)
Discussion
This study revealed that the level of adherence to ART in south Gonder public hospitals was found to be 78.9%. Besides, TB co-infection, short duration of ART, Zidovudine containing ART regimen, and treatment failure were found to be significantly associated with poor adherence.
The finding is comparable with the study conducted in Ethiopia (78.6%), Uganda (79%), Nigeria (76.1%), and Myanmar (76.2%).Citation41–Citation44 However, this finding is higher than the studies conducted at Tikur Anbessa Hospital (34.8%) and Jimma (63.8%).Citation31,Citation45 Moreover, the level of adherence to ART is also higher than the studies conducted in Peru (41.7%), and Brazil (71.6%).Citation46,Citation47 On the other hand, this finding is lower than the studies conducted in Debre Birhan (95.5%) and Nepal (87.4%).Citation32,Citation48
The discrepancy could be explained by the difference in diagnostic procedures of adherence to ART. In addition, under-reporting due to shortage of skills of healthcare providers or caregivers is usually encounter in low-income countries than in middle countries. Socioeconomic status, the study design, methods of adherence assessment, sample size, and setting difference are also considered for this variation.
This study showed that children having TB/HIV co-infection increase the level of poor adherence by 3.80 times than children without TB co-infection (AOR=3.80, 95% CI (1.41, 10.1)) which is in line with other studies.Citation43,Citation47 This might be due to the summative effect of suffering from two chronic conditions, associated with stigma and discrimination that require clinical management for an entire life. In addition to this, medication for confection, treatment, and ART together can contribute to increased pill burden, drug–drug interactions, and more adverse drug effects, all of which are capable of hindering adherence to antiretroviral drugs.
This finding also showed that HIV-positive children on ART with <36 months on ART [AOR = 3.4 (95% CI: 1.60, 7.20)] were more likely to be poor adherents than children who were on ART > 59 months in the follow-up period Similar findings were reported from TanzaniaCitation49 and Nepal.Citation48 The duration of treatment prolongs, quality of life improves which in turn motivates the children to have good adherence and to follow every instruction and recommendation provided by the health care providers and caregivers.
The odds of children on ART with treatment failure was around 10 times higher to be poor adherent than those who had no treatment failure (AOR= 10.2, 3.95–26.2). This is a similar report from a study conducted in South Africa.Citation50
Treatment failure is the main cause of death, drug adaptability, and the development of drug-resistant viral strains which is potentiating challenge globally by reducing drug adherence. Furthermore, HIV drug resistance occurs when mutations develop frequently because of poor adherence (treatment interruptions, inadequate drug concentrations, or/and use of suboptimal drug combinations).Citation50,Citation51 Besides, Poor adherence to ART is a major factor of treatment failure, the emergence of drug-resistant viruses, disease progression, hospitalization, mortality, and health care costs.Citation52
In the current study, the odds of children who were enrolled in the Zidovudine-containing ART regimen were (AOR=3.5, 95% CI: 1.1–10.9) three folds more likely to be poor adherents than their counterparts. This was also supported by the study conducted in Kenya.Citation53 The reason behind this might be that those who were on the Zidovudine regiment were more prone to severe life-threatening anemia, severe gastro-intestinal intolerance, fatigue, congestive heart failure, and sepsis/infection which leads to poor treatment adherence. However, inconsistent with studies from Oromia EthiopiaCitation54 that showed that receiving protease inhibitors were more likely to be poor adherent. Since ART drugs most likely need to be administered throughout the patient’s life, a regimen should be chosen after considering the patient’s characteristics, the results of viral drug resistance testing, drug efficacy, and ease of administration, potential AEs, pill size, and dosing frequency.
Limitation of the Study
While this study is multi-setting, the data on adherence were collected from a chart that was recorded according to the patient’s self-report of the amount of medication taken between visits without a standardized set of questions. Being retrospective may also limit the study to evaluate the predictor’s variable of adherence to ART includes caregiver’s socioeconomic status.
Conclusion
The current study showed that the level of adherence to antiretroviral therapy was found to be low. TB co-infection, short duration of ART, Zidovudine-containing ART regimen, and treatment failure were found to be significantly associated with poor adherence. Based on our results, health care providers should provide intensive and ongoing counseling to a child and/or their caregivers before and throughout ART, training sessions are required to gain knowledge on disseminating information appropriate to a patient’s level of understanding. It will empower patients with correct knowledge about good adherence practice. Despite the earlier presentation of children to care should be motivated, more targeted adherence support should be planned for those who present at an early stage of their illness. Besides this, children or their caretakers should be provided with adequate counseling during medication change or when new medication with a different role is added and establish a system of linkage with other units in the Hospital. For instance, in the case of TB co-infection, they should be linked with the TB unit and the children should take Anti-TB medication with ART drugs. The hospital management team is also expected to provide training on ART adherence counseling to health care providers. Moreover, further studies should be conducted to evaluate and improve the quality of ART service in south Gondar public Hospitals.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; AOR, Adjusted Odds ratio; ART, Anti-Retroviral Therapy; CPT, Cotrimoxazole Preventive Therapy; HIV, Human Immunodeficiency Virus; IPT, Isoniazid Preventive Therapy; TB, Tuberculosis; WHO, World Health Organization.
Ethical Approval and Participant Consent
Ethical clearance letter was obtained from an ethical review board of Debre Tabor University. In addition, a permission letter was also obtained from each south Gondar public hospital. Since we used secondary data, we did not get informed consent from the study participants. Confidentiality was secured. This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Acknowledgments
We would like to thank the Debre Tabor university administrative bodies and south Gondar public hospitals. Moreover, our thanks also go to all individuals who participated in data collection and supervision.
Disclosure
The authors report no conflicts of interest in this work.
References
- Harrison’s Principles of Internal Medicine. 20e | accessMedicine | mcGraw-Hill Medical [Internet]; [cited March 25, 2021]. Available from: https://accessmedicine.mhmedical.com/book.aspx?bookID=2129. Accessed August 2, 2021.
- UNAIDS DATA 2017 [Internet]. [cited March 25, 2021]. Available from: https://www.unaids.org/en/resources/documents/2017/2017_data_book. Accessed August 2, 2021.
- summary-of-the-global-hiv-epidemic-2020.png (936×662) [Internet]. [cited July 21, 2021]. Available from: https://www.who.int/images/default-source/departments/hiv/summary-of-the-global-hiv-epidemic-2020.png?sfvrsn=73ac5b6a_5. Accessed August 2, 2021.
- World Health Organization. Towards the Elimination of Mother-To-Child Transmission of HIV: Report of a Technical Consultation. Geneva Switz: Rep Tech Consult; 2010.
- Global HIV statistics 2019 pdf - google search [internet]. [cited July 21, 2021]. Available from: https://www.google.com/search?sxsrf=ALeKk01-zjGwvGhnAYn7wKvFhv5VAaYYyQ:1626846819421&q=Global+HIV+statistics+2019+pdf&sa=X&ved=2ahUKEwjjx5nWvPPxAhUScBQKHenCDkEQ1QIwE3oECCIQAQ. Accessed August 2, 2021.
- World Health Organization. Ethiopia, HIV Country Profile: Spectrum Estimates (UNAIDS/WHO) and WHO HIV Country Intelligence Tool. Glob AIDS Monit UNAIDSWHOUNICEF; 2017.
- Martelli G, Antonucci R, Mukurasi A, Zepherine H, Nöstlinger C, Chemin I. Adherence to antiretroviral treatment among children and adolescents in Tanzania: comparison between pill count and viral load outcomes in a rural context of Mwanza region. PLoS One. 2019;14(3):e0214014. doi:10.1371/journal.pone.0214014
- Ethiopia F. National Guidelines for Comprehensive HIV Prevention, Care, and Treatment. AAMo Health; 2017.
- Rosen S, Fox MP, Gill CJ, Sepulveda-Amor J. Patient retention in antiretroviral therapy programs in Sub-Saharan Africa: a systematic review. PLOS Med. 2007;4(10):e298. doi:10.1371/journal.pmed.0040298
- Starace F, Massa A, Amico KR, Fisher JD. Adherence to antiretroviral therapy: an empirical test of the information-motivation-behavioral skills model. Health Psychol. 2006;25(2):153–162. doi:10.1037/0278-6133.25.2.153
- Nischal KC, Khopkar U, Saple DG. Improving adherence to antiretroviral therapy. Indian J Dermatol Venereol Leprol. 2005;71(5):316–320. doi:10.4103/0378-6323.16780
- Zoufaly A, Fillekes Q, Hammerl R, et al. Prevalence and determinants of virological failure in HIV-infected children on antiretroviral therapy in rural Cameroon: a cross-sectional study. Antivir Ther. 2013;18(5):681–690. doi:10.3851/IMP2562
- Abaasa AM, Todd J, Ekoru K, et al. Good adherence to HAART and improved survival in a community HIV/ AIDS treatment and care program: the experience of The AIDS Support Organization (TASO), Kampala, Uganda. BMC Health Serv Res. 2008;8:241. doi:10.1186/1472-6963-8-241
- Morowatisharifabad MA, Movahed E, Farokhzadian J, et al. Antiretroviral therapy adherence and its determinant factors among people living with HIV/AIDS: a case study in Iran. BMC Res Notes. 2019;12(1):162. doi:10.1186/s13104-019-4204-5
- Heyer A, Ogunbanjo GA. Adherence to HIV antiretroviral therapy part ll: which interventions are effective in improving adherence? SA Fam Pr. 2006;48:6–10. doi:10.1080/20786204.2006.10873455
- Marhefka SL, Tepper VJ, Farley JJ, Sleasman JW, Mellins CA. Brief report: assessing adherence to pediatric antiretroviral regimens using the 24-hour recall interview. J Pediatr Psychol. 2006;31(9):989–994. doi:10.1093/jpepsy/jsj107
- Biadgilign S, Deribew A, Amberbir A, Deribe K. Adherence to highly active antiretroviral therapy and its correlates among HIV infected pediatric patients in Ethiopia. BMC Pediatr. 2008;8(1):53. doi:10.1186/1471-2431-8-53
- Prendergast A, Tudor-Williams G, Jeena P, Burchett S, Goulder P. International perspectives, progress, and future challenges of pediatric HIV infection. Lancet. 2007;370(958):68–80.
- Haberer J, Mellins C. Pediatric adherence to HIV antiretroviral therapy. Curr HIVAIDS Rep. 2009;6(4):194–200. doi:10.1007/s11904-009-0026-8
- World Health Organization. Antiretroviral Therapy of HIV Infection in Infants and Children: Towards Universal Access. Switzerland: WHO; 2006.
- Ministry of health of Ethiopia and federal HIV/AIDS prevention and control office: guidel pediatr HIVAIDS care treat Ethiop Addis Ababa; 2008.
- Vreeman RC, Wiehe SE, Pearce EC, Nyandiko WM. A systematic review of pediatric adherence to antiretroviral therapy in low- and middle-income countries. Pediatr Infect Dis J. 2008;27(8):686–691. doi:10.1097/INF.0b013e31816dd325
- Simoni JM, Montgomery A, Martin E, New M, Demas PA, Rana S. Adherence to antiretroviral therapy for pediatric HIV infection: a qualitative systematic review with recommendations for research and clinical management. Pediatrics. 2007;119(6):e1371–e1383. doi:10.1542/peds.2006-1232
- Ingersoll KS, Cohen J. The impact of medication regimen factors on adherence to chronic treatment: a review of the literature. J Behav Med. 2008;31(3):213–224. doi:10.1007/s10865-007-9147-y
- Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
- World Health Organization. Underlying Causes of Child Death. Geneva, Switzerland: CHERG/WHO; 2011.
- World Health Organisation (WHO). United Nations Programme on AIDS Progress Report: Glob HIVAIDS Response. Geneva, Switzerland: WHO; 2011.
- Nozaki I, Dube C, Kakimoto K, Yamada N, Simpungwe JB. Social factors affecting ART adherence in rural settings in Zambia. AIDS Care. 2011;23(7):831–838. doi:10.1080/09540121.2010.542121
- Williams PL, Storm D, Montepiedra G, Nichols S, Kammerer B, Siros PA. Predictors of adherence to antiretroviral medications in children and adolescents with HIV infection. Pediatrics. 2006;118(6):e1745–e1757. doi:10.1542/peds.2006-0493
- Davies M-A, Boulle A, Fakir T, Nuttall J, Eley B. Adherence to antiretroviral therapy in young children in Cape Town, South Africa, measured by medication return and caregiver self-report: a prospective cohort study. BMC Pediatr. 2008;8(1):34. doi:10.1186/1471-2431-8-34
- Biressaw S, Abegaz WE, Abebe M, Taye WA, Belay M. Adherence to antiretroviral therapy and associated factors among HIV infected children in Ethiopia: unannounced home-based pill count versus caregivers’ report. BMC Pediatr. 2013;13:132. doi:10.1186/1471-2431-13-132
- Ketema AK, Shewangizaw Weret Z. Assessment of adherence to highly active antiretroviral therapy and associated factors among people living with HIV at Debrebrihan referral hospital and Health Center, Northeast Ethiopia: a cross-sectional study. HIV AIDS (Auckl). 2015;7:75–81.
- Jamieson D, Kellerman SE. The 90 90 90 strategies to end the HIV pandemic by 2030: can the supply chain handle it? J Int AIDS Soc. 2016;19(1):20917. doi:10.7448/IAS.19.1.20917
- Federal HIV/AIDS prevention and control office: HIV prevention in Ethiopia national road map 2018–2020; November, 2018.
- Debre Tabor. In: Wikipedia [internet]; 2020 [cited December 31, 2020]. Available from: https://en.wikipedia.org/w/index.php?title=Debre_Tabor&oldid=972443023. Accessed August 2, 2021.
- Gultie T. Factors affecting adherence to pediatrics antiretroviral therapy in Mekelle hospital, Tigray Ethiopia. Int J Public Health Sci. 2015;4(1):6.
- Okechukwu AA, Okechukwu OI. The clinical correlate of tuberculosis in HIV co-infected children at the University of Abuja teaching hospital, Gwagwalada, Nigeria. Niger J Clin Pract. 2011;14(2):206–211. doi:10.4103/1119-3077.84018
- Atalell KA, Birhan Tebeje N, Ekubagewargies DT, Yotebieng M. Survival and predictors of mortality among children co-infected with tuberculosis and human immunodeficiency virus at University of Gondar comprehensive specialized hospital, Northwest Ethiopia. A retrospective follow-up study. PLoS One. 2018;13(5):e0197145. doi:10.1371/journal.pone.0197145
- Melkamu MW, Gebeyehu MT, Afenigus AD, et al. Incidence of common opportunistic infections among HIV-infected children on ART at Debre Markos referral hospital, Northwest Ethiopia: a retrospective cohort study. BMC Infect Dis. 2020;20(1):50. doi:10.1186/s12879-020-4772-y
- Refera H, Wencheko E. Survival of HIV-TB co-infected adult patients under ART in Ambo Referral Hospital, Ethiopia. Ethiop J Health Dev. 2013;27(2):88–93.
- Arage G, Tessema GA, Kassa H. Adherence to antiretroviral therapy and its associated factors among children at South Wollo Zone Hospitals, Northeast Ethiopia: a cross-sectional study. BMC Public Health. 2014;14(1):365. doi:10.1186/1471-2458-14-365
- Wadunde I, Tuhebwe D, Ediau M, Okure G, Mpimbaza A, Wanyenze RK. Factors associated with adherence to antiretroviral therapy among HIV infected children in Kabale district, Uganda: a cross-sectional study. BMC Res Notes. 2018;11(1):466. doi:10.1186/s13104-018-3575-3
- Ugwu R, Eneh A. Factors influencing adherence to pediatric antiretroviral therapy in Portharcourt, South-South Nigeria. Pan Afr Med J. 2013;16:30. doi:10.11604/pamj.2013.16.30.1877
- Thandar M, Mon AS, Boonyaleepun S, Laohasiriwong W. Antiretroviral treatment adherence and associated factors among people living with HIV in a developing country, Myanmar. Int J Community Med Public Health. 2017;3(5):1318–1325.
- Abera A, Fenti B, Tesfaye T, Balcha F. Factors influencing adherence to antiretroviral therapy among people living with HIV/AIDS at ART clinic in Jimma University teaching hospital, Southwest Ethiopia. J Pharma Rep. 2015;1(101):2.
- Soares RD, Brito AM, Lima K, Lapa TM. Adherence to antiretroviral therapy among people living with HIV/AIDS in northeastern Brazil: a cross-sectional study. Sao Paulo Med J. 2019;137(6):479–485. doi:10.1590/1516-3180.2019.0212170919
- Leyva-Moral JM, Loayza-Enriquez BK, Palmieri PA, et al. Adherence to antiretroviral therapy and the associated factors among people living with HIV/AIDS in Northern Peru: a cross-sectional study. AIDS Res Ther. 2019;16(1):22. doi:10.1186/s12981-019-0238-y
- Neupane S, Dhungana GP, Ghimire HC. Adherence to antiretroviral treatment and associated factors among people living with HIV and AIDS in CHITWAN, Nepal. BMC Public Health. 2019;19(1):720. doi:10.1186/s12889-019-7051-3
- Nyogea D, Mtenga S, Henning L, et al. Determinants of antiretroviral adherence among HIV-positive children and teenagers in rural Tanzania: a mixed-methods study. BMC Infect Dis. 2015;15(1):28. doi:10.1186/s12879-015-0753-y
- Yassin S, Gebretekle GB. Magnitude and predictors of antiretroviral treatment failure among HIV-infected children in Fiche and Kuyu hospitals, Oromia region, Ethiopia: a retrospective cohort study. Pharmacol Res Perspect. 2017;5(1):e00296. doi:10.1002/prp2.296
- Endalamaw A, Mekonnen M, Geremew D, Yehualashet FA, Tesera H, Habtewold TD. HIV/AIDS treatment failure and associated factors in Ethiopia: a meta-analysis. BMC Public Health. 2020;20(1):82. doi:10.1186/s12889-020-8160-8
- Nachega JB, Marconi VC, van Zyl GU, et al. HIV treatment adherence, drug resistance, virologic failure: evolving concepts. Infect Disord Drug Targets. 2011;11(2):167–174. doi:10.2174/187152611795589663
- Ochieng W, Kitawi RC, Nzomo TJ, et al. Implementation and operational research: correlates of adherence and treatment failure among Kenyan patients on long-term highly active antiretroviral therapy. J Acquir Immune Defic Syndr. 2015;69(2):e49–e56. doi:10.1097/QAI.0000000000000580
- Biru M, Jerene D, Lundqvist P, Molla M, Abebe W, Hallström I. Caregiver-reported antiretroviral therapy non-adherence during the first week and after a month of treatment initiation among children diagnosed with HIV in Ethiopia. AIDS Care. 2017;29(4):436–440. doi:10.1080/09540121.2016.1257098