
Abstract
Molluscum contagiosum (MC) is an infectious disease caused by the MC virus. In human immunodeficiency virus (HIV) patients, MC has an atypical predilection and prominence, sometimes measuring more than 1 cm in diameter, known as giant MC. Giant MC lesions on the eyelids are rare. There is no standardized therapy for eyelids MC in HIV patients. Antiretroviral (ARV) administration is recommended as the primary treatment for MC in HIV patients along with other treatment modalities, such as potassium hydroxide (KOH). The 20% KOH solution is a keratolytic agent with good efficacy as MC therapy. Two cases of giant MC on the eyelids of stage 2 HIV patients with respective CD4+ of 31 cells/μL and 46 cells/μL were reported. The lesions consisted of multiple confluent papules with central umbilication, and Tzanck smear revealed Henderson–Patterson bodies. Both patients were treated with ARV and self-applied 20% KOH solution once daily. The lesions improved after four weeks of therapy in both patients with most of the lesions diminished. The successful treatment with 20% KOH solution for giant MC on the eyelids of HIV patients observed in the current study provides evidence that treatment with this solution yielded prompt results, is non-toxic, and can be self-applied.
Introduction
Approximately 5–18% immunocompromised patients with human immunodeficiency virus (HIV) experienced molluscum contagiosum (MC),Citation1,Citation2 with lesions occurring in up to one-third of patients with CD4+ level of less than 100 cells/μL.Citation2 The classic MC lesions consists of pearl-like, dome-shaped, centrally-umbilicated discrete papules, measuring 3–5 mm in diameter, that usually resolve spontaneously.Citation1–Citation3 MC in HIV patients can occur in atypical predilection sites including the eyelids, and tend to be prominent, measuring more than 1 cm in diameter, known as giant MC.Citation1–Citation4 To date, antiretroviral drugs (ARV) is the only standardized therapy allowed for MC in HIV patients.Citation2,Citation5 In these patients, MC rarely resolves spontaneously, and adjuvant therapy is needed to accelerate resolution.Citation5 Treatment for MC is also indicated for aesthetically-disturbing lesions.Citation2 Potassium hydroxide (KOH) solution is a keratolytic, destructive agent which can be used as MC therapy with high effectiveness. It is also relatively easy to use, and inexpensive.Citation6,Citation7 This case report aims to present two cases of giant MC on the eyelids of HIV patients successfully treated with ARV and adjuvant self-administered topical 20% KOH solution.
Case 1
A 36-year-old male presented with multiple papules on the upper and lower right and left eyelids. Seven months prior to consult, acne-like, pin-point sized, mildly pruritic papules appeared on the patient’s right cheek. The papules multiplied and appeared on the right upper eyelid within a month. Patient often rubbed the papules on the right upper eyelids, which then increases in number and size, became confluence, and spread to the right lower eyelid measuring more than 1 cm in diameter ( and ). The complaint is occasionally followed by eye redness and discharge with no blurred vision or pain. Difficulty in opening the eye was more prominent in the last two weeks. The patient was diagnosed with HIV in 2012 and started ARV therapy in 2017. CD4+ value was 31 cells/μL. Tzanck smear from skin lesion on the forehead revealed Henderson–Paterson bodies as round hyperbasophilic mass (). The patient was diagnosed with giant MC on the eyelids and stage 2 HIV. We consulted the patient to an ophthalmologist who suggested excisional surgery, but the patient refused the option. The patient was then treated with self-administered 20% KOH solution applied once daily at night. The application methods were as follows: the surrounding healthy skin was covered with vaseline album, the upper and lower eyelids covered with wet gauze to prevent the solution from dripping or irritating the eye, then the 20% KOH solution was spread evenly using a cotton tip on the skin lesions. Follow up visit one week later revealed superficial ulceration with crusts on most papules on the right eyelids. The patient’s complaint of red eyes remained, but with no blurred vision or pain (). The patient was again referred to an ophthalmologist who suggested using artificial tears and discontinuing the 20% KOH solution, followed with the application of an open wet dressing using saline solution twice daily for a week. The patient then resumed treatment with 20% KOH solution once daily at night, three times a week. Clinical improvement was observed after four weeks of therapy, all lesions on right eyelids disappeared and no new lesions were observed (). The burning sensation side effect was well tolerated by the patient, who was satisfied and willing to redo the treatment if new lesion appears.
Figure 1 (A and B) Clinical manifestation of day-1 prior to therapy, (C) molluscum bodies found in cytological examination.
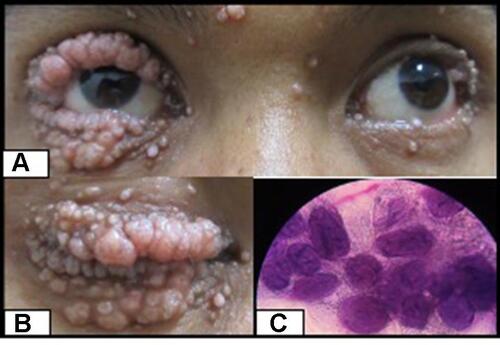
Figure 2 (A) One-week follow up after topical therapy with 20% KOH solution, (B) resolution of the lesions at 4 weeks after therapy.

Case 2
A 26-year-old female presented with multiple papules on the upper and lower left eyelid with occasional itch. The first lesion appeared as a single pin-sized papule on the left eyelid six months prior to consult, which multiplied and spread quickly within one month to the upper and lower left eyelids. Patient admitted to being in the habit of rubbing the eye. The pre-existing papules increased in number in the past month and became confluent with a diameter of 1 cm (). The patient was diagnosed with HIV in 2016 and consumed ARV routinely. CD4+ value was 46 cells/μL. Tzanck smear from the skin lesion revealed Henderson–Paterson bodies (). Other physical examination was within normal limits. The patient was diagnosed with giant MC on the eyelid and stage 2 HIV. The patient was treated with 20% KOH solution applied once daily at night. The application methods were as follows: the surrounding healthy skin was covered with vaseline album, the upper and lower eyelids covered with wet gauze to prevent the solution from dripping or irritating the eye. Then, the 20% KOH solution was spread evenly using a cotton tip on the skin lesions. Follow up visit three weeks later revealed slight erythema and edema on the right eyelids and smaller lesion (). All the lesions were cleared completely four weeks after therapy (). Side effects reported by the patient include stinging and burning sensation immediately after application, but these symptoms improved after one to five minutes without any additional treatment. The patient was satisfied with the final result.
Figure 3 (A) Clinical manifestation of day-1 prior to therapy, (B) molluscum bodies found in cytological examination.
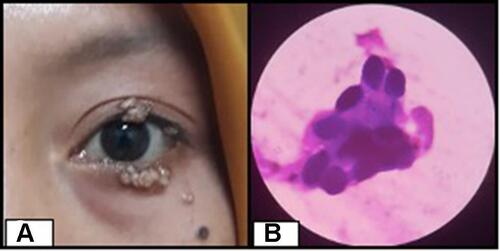
Figure 4 (A) Two-weeks follow up after topical therapy with 20% KOH solution, (B) resolution of the lesions at 4 weeks after therapy.

Discussion
In HIV patients, MC tends to occur during the advanced stage with more severe immunodeficiency.Citation2,Citation5 Stage 2 HIV can be established upon finding of prominent and giant MC lesions in HIV patients.Citation8 Perez-Blazquez et al reported 10 advanced stage HIV patients with CD4+ values below 80 cells/μL having lesions on the eyelids.Citation9 There was no significant differences in terms of MC incidence in male or female.Citation3 Our first case was a 36-year-old-male with CD4+ level of 31 cells/μL and the second case was a 26 year-old-female with CD4+ level of 46 cells/μL. Both patients were diagnosed with stage 2 HIV. The occurrence of MC on the eyelids can be a sign of a patient having HIV or that the HIV is in an advanced stage.Citation2,Citation5
The MC virus can be transmitted through direct contact to skin with previous history of trauma or micro abrasion, through sexual or nonsexual routes including through contact with contaminated objects (fomites).Citation1,Citation2 The lesions then spread to other locations due to autoinoculation.Citation1,Citation2 The typical predilection in children include exposed sites such as the face, extremities, or intertriginous areas, whereas in adults, lesions typically develop in the genital area.Citation1,Citation2 Immunosuppressed patients typically have more severe and extensive disease with atypical predilections including oral mucosa, lips, palms, soles, and eyelids.Citation2,Citation3 Although the exact pathogenesis of giant MC lesions and atypical morphology in HIV patients remains unknown, several factors were thought to play role, including decreased in T cell counts, impaired natural killer cell function, and decreased number of Langerhans cells in the epidermis.Citation10 In this case report, MC lesions were found only on the face and eyelids. Both patients have a history of repeated scratching on their lesions, which may play role in spreading the lesion through autoinoculation.
Immunocompromised patients may have other opportunistic infections resembling MC, such as penicilliosis, cryptococcosis, and histoplasmosis.Citation2,Citation5 Using direct cytological examination with Giemsa staining on samples taken from the skin lesion (Tzanck smear), MC can be differentiated from other lesions with the discovery of molluscum bodies, also known as Henderson–Paterson bodies, as its pathognomonic finding.Citation2,Citation3 In our cases the findings of molluscum bodies from cytological examination exclude other differential diagnoses.
MC is generally self-limiting, and can last several months to several years.Citation1,Citation2 However, in HIV patients, these lesions often do not resolve spontaneously and can be widespread.Citation5 Therapy of MC in HIV patients is indicated to minimize the risk of autoinoculation, prevent secondary infections, prevent transmission, and for aesthetic purposes.Citation2,Citation11 Considerations for treatment options include therapeutic effectiveness, the patient’s physical and psychological endurance during treatment, the patient’s individual choice, treatment cost, availability of materials or therapeutic devices, and practicality.Citation11
There is no standard treatment for MC in HIV patients, since the lesions tend to be recalcitrant and recurring.Citation5 In HIV patients, MC will resolve spontaneously as the CD4+ count increases. Therefore, administration of ARV is recommended for HIV patients along with other therapies.Citation2,Citation9,Citation12 There was one case report of MC on the eyelids in children with HIV treated with ARV, without any additional therapy. The lesion was resolved after six months of ARV.Citation13
Destructive therapy works by damaging the intracytoplasmic sacs containing viral particles and stimulating the immune response to clear the infection.Citation2 Destructive modalities include physical and chemical therapy. Physical therapy effective for MC cases include curettage and cryotherapy,Citation1 but the lesion predilections in our cases made it difficult to perform. Chemical therapy using KOH solution provides keratolytic effect that lyses protein and lipid. The advantages of KOH solution for MC therapy stems from the fact that it was effective, easy to apply, can be self-administered, has minimal side effects, and was cost-effective.Citation14 KOH is an alkaline substance that can cause ocular burns and may do harm if not used properly.Citation15,Citation16 Therefore, our patient was trained to safely use KOH solution to prevent ocular injury. The most important intervention in chemical injuries is timely irrigation of the eye using normal saline or water to reduce the severity of chemical burns.Citation15
Chemical therapy using KOH solution with various concentrations (2.5 to 20%) in MC have resulted in various outcomes.Citation6,Citation15 A study in Pakistan on 120 patients with MC found that 10% KOH solution had the same effectiveness compared to cryotherapy. However, the pain was less prominent in the 10% KOH group.Citation14 A study of 24 cases of MC in children treated using 20% KOH solution found that all patients had resolution within an average of 17 days.Citation17 A serial case of MC lesions treated using 20% KOH solution reported that twice-daily application reduced facial lesions at day 7 and genital lesions at day 20 after therapy. Meanwhile, once-daily application of 20% KOH solution required longer time (day 25–31 after therapy) to reduce genital MC lesions.Citation7 Common side effects such as stinging pain within 1–2 minutes after use, inflammation for 5–7 days, and post-inflammatory hypopigmentation were reported.Citation7,Citation17 Other side effects reported in a study using 20% KOH solution in 18 adult MC patients include pain (55%), burning sensation (20%), and secondary infections (10%).Citation6 Our patients were treated with ARV and adjuvant topical 20% KOH solution once daily at night. In the first case, superficial inflammation, ulceration, and crusted lesions were noted one week after therapy, with all the lesions resolved within four weeks. Side effects of burning and stinging sensations were mild and well-tolerated by the patient. In the second case, there were mild side effects of stinging and burning sensations and the lesions resolved within four weeks of therapy.
Conclusion
Giant MC lesions on the eyelids of HIV patients pose a challenge in treatment. Successful treatment with 20% KOH solution on giant MC lesions on the eyelids of HIV patients observed in this study provides evidence that treatment with 20% KOH solution yielded prompt results, is non-toxic, and can be self-applied.
Abbreviations
MC, molluscum contagiosum; HIV, human immunodeficiency virus; ARV, antiretroviral; KOH, potassium hydroxide; CD, cluster of differentiation.
Ethical Approval
This study was conducted in compliance with the Declaration of Helsinki, Good Clinical Practices, local regulatory requirements, and was approved by the Medical Ethics Committee of Hasan Sadikin General Hospital Bandung (approval number: LB.02.01/X.6.5/230/2021).
Consent for Publication
Both patients signed informed consent forms. They also signed forms giving consent for the use of cases details and images for publication and for scientific purposes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the staff of Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Haddock ES, Friedlander SF, et al. Poxvirus infection. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, editors. Fitzpatrick Dermatology, 9th. New York: McGraw-Hill; 2019:3086–3091.
- Douglas JM. Molluscum contagiosum. In: Holmes KK, Sparling PF, Stamm WE, Piot P, Wasserheit JN, Corey L, editors. Sexually Transmitted Diseases. 4th ed. New York: McGraw-Hill; 2008:545–552.
- Meza-Romero R, Navarrete-Dechent C, Downey C. Molluscum contagiosum: an update and review of new perspectives in etiology, diagnosis, and treatment. Clin Cosmet Investig Dermatol. 2019;12:373. doi:10.2147/CCID.S187224
- Rosner M, Zloto O. Periocular molluscum contagiosum: six different clinical presentations. Acta Ophthalmol Scand. 2018;96(5):e600–5. doi:10.1111/aos.13717
- Schwartz JJ, Myskowski PL. Molluscum contagiosum in patients with human immunodeficiency virus infection: a review of twenty-seven patients. J Am Acad Dermatol. 1992;27(4):583–588. doi:10.1016/0190-9622(92)70226-6
- Maluki A, Kadhum QJ. Treatment of molluscum contagiosum by potassium hydroxide solution 20% with and without pricking and by pricking alone: a comparative study with review of literature. Int J Dermatol Clin Res. 2015;1(2):031–041. doi:10.17352/2455-8605.000011
- Achdiat PA, Rowawi R, Fatmasari D, et al. A case series: experience of using 20% potassium hydroxide solution to treat adult sexually transmitted molluscum contagiosum. Clin Cosmet Investig Dermatol. 2020;13:671. doi:10.2147/CCID.S270380
- World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. 2nd edition: World Health Organization; 2016. Available from http://www.who.int/hiv/pub/guidelines/HIVstaging150307.pdf. Accessed November 9, 2021.
- Pérez-Blázquez E, Villafruela I, Madero S. Eyelid molluscum contagiosum in patients with human immunodeficiency virus infection. Orbit. 1999;18(2):75–81. doi:10.1076/orbi.18.2.75.2712
- Vora RV, Pilani AP, Kota RK. Extensive giant molluscum contagiosum in a HIV positive patient. J Clin Diagn Res. 2015;9(11):WD01.
- Mahdi MA, Mukheilf TA. Topical Retinoid In Treatment of Molluscum Contagiosum in Iraqi patients in Khalis City (Placebo Control Study). Diyala Journal of Medicine. 2017;13(1):17–21. doi:10.26505/DJM.13013272003
- Martin P. Interventions for molluscum contagiosum in people infected with human immunodeficiency virus: a systematic review. Int J Dermatol. 2016;55(9):956–966. doi:10.1111/ijd.13267
- Averbuch D, Jaouni T, Pe’er J, Engelhard D. Confluent molluscum contagiosum covering the eyelids of an HIV-positive child. Clin Exp Ophthalmol. 2009;37(5):525–527.
- Qureshi A, Zeb M, Jalal-ud-din M, et al. Comparison of efficacy of 10% potassium hydroxide solution versus cryotherapy in treatment of molluscum contagiosum. J Ayub Med Coll Abbottabad. 2016;28(2):382–385.
- Al-Sudany NK, Abdulkareem DR. A comparative study of topical 10% KOH solution and topical 25% podophyllin solution as home-base treatments of molluscum contagiosum. J Dermatol Dermatosurg. 2016;20:107–114.
- Bizrah M, Yusuf A, Ahmad S. An update on chemical eye burns. Eye. 2019;33(9):1362–1377. doi:10.1038/s41433-019-0456-5
- Mahajan BB, Pall A, Gupta RR. Topical 20% KOH an effective therapeutic modality for molluscum contagiosum in children. Indian J Dermatol Venereol Leprol. 2003;69(2):175–177.