
Abstract
Background
Survival and quality of life of people living with HIV (PLWH) have been improving. Understanding fertility intention among PLWH is critical in helping them accomplish their pregnancy goals while significantly lowering the risk of HIV transmission. The purpose of this study was to identify factors based on the theory of planned behavior (TPB) that may explain fertility intention among PLWH.
Methods
A survey was conducted in face-to-face interviews based on TPB, and the latent variables were devised and tested for their potential influences on fertility intentions in 487 reproductive-aged PLWH at antiretroviral treatment clinics in Kunming, China. Analysis was mainly based on the structural equation model.
Results
About 38.4% of the respondents answered that they were likely to have a/another child in the next three years. Our hypothesized factors could explain 53.7% of the total variance of fertility intention. The 20- to 35-year-old group had a higher fertility intention. Perceived partner expectations toward fertility were the strongest predictors of fertility intention followed by beliefs in the support of the two-child policy. In contrast, the three components of attitudes, subjective norm, and perceived behavioral control did not influence fertility intention.
Conclusion
In this HIV endemic area of China, fertility intended by PLWH is a matter of the couple that is also influenced by the national population fertility policy.
Background
Availability of antiretroviral treatment (ART) has a positive effect on fertility intentions among people living with HIV (PLWH).Citation1–Citation3 Reproductive-aged PLWH are critical stakeholders since they bear the threat of HIV. Furthermore, a lack of sexual health education and restricted access to sexual and reproductive health services among young adults lead to increased sexual risk behaviors and unintended births.Citation4,Citation5 Attitudes, social norms, and perceived behavioral control (PBC) responded negatively to fertility intention due to concerns about HIV transmission.Citation6–Citation8 HIV-positive status may cause PLWH to have negative fertility intentions because of uncertainty surrounding their future, childcare for an orphaned child after their death, and risk of infection to the newborn.Citation9,Citation10 Moreover, women with HIV are more reluctant than men with HIV to have a/another child despite often holding more positive reproductive attitudes.Citation11 Thus, a more thorough understanding of what motivates fertility intentions among PLWH is an important area of concern that has practical applications for creating a safe reproductive environment. Psychological, social, and cultural factors, and in particular the pressure of family members or the need to perpetuate family lineage, also play key roles in how HIV affects reproductive decisions.Citation12–Citation14
Previous researchers have shown that having a positive psychological status about an issue can be irrelevant to intention.Citation15,Citation16 Recently, fertility needs among PLWH have received attention from academia. Much research on having children has been conducted in Western countries and Africa using qualitative research methods. However, much less is known about the intention to have children among PLWH in Asian countries. Western societies stress individualism, but Eastern societies are based on interdependence or collectivism. Therefore, social norms may exert a strong effect on fertility intention in Eastern cultures.Citation17,Citation18 Previous studies in Vietnam and Thailand found that fertility intention was expressed by the interests of the family, social pressure, continuity, or heredity.Citation19–Citation21 It is not clear how psychosocial determinants of individuals influence fertility intention in China. This study aimed to test the influences of the socio-demographic characteristics, relevant beliefs, attitudes, subjective norms, PBC, and fertility intention on PLWH.
Materials and Methods
Theoretical Framework
The hypothesized model of fertility intention in this study was based on the Theory of Planned Behavior (TPB), which is a popular social and psychological model of human behavior.Citation22 The TPB model adopts attitudes, subjective norms, and perceived control as having a direct positive effect on fertility intention ().Citation23,Citation24 We included five demographic variables, namely sex, age, registered residence, employment status, and household monthly income, as having a direct effect on fertility intention and also an indirect effect through attitudes, subjective norms, and perceived control as suggested in systematic reviews of the literature.Citation25–Citation27
Figure 1 Theoretical framework for fertility intention among PLWH. Dotted line box = Behavioral beliefs; dashed line box= Normative beliefs; solid line box= Control beliefs.
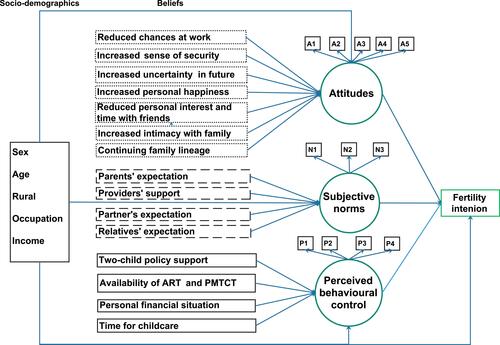
“Attitudes” were modeled as a latent variable with 5 observed variables (A1-A5). It was hypothesized to be affected by seven behavioral beliefs in the dotted frames (). This study identified salient behavioral beliefs (such as having a child could increase a person’s happiness and intimacy within their family) from a systematic review.Citation25 “Subjective norms” were included in the model as a latent variable with 3 observed variables (N1-N3). Subjective norms were influenced by four normative beliefs in the dashed frames including the expectations of important referents (partners, parents, providers, and relatives). “Perceived behavioral control” (PBC) was a latent variable with 4 observed variables (P1 through P4). PBC was modeled to be affected by four control beliefs in the solid frames. These normative beliefs and control beliefs were identified from in-depth interviews with a group of PLWH at the ART clinic.
Study Setting and Subjects
Kunming City was selected as the study site because it is one of the areas in China with a serious HIV epidemic. Data collection was performed at the Infectious Disease Department of Kunming Infectious Disease Hospital, which serves more than 10,000 clients per year. The subjects of this study were females aged 20−40 years and males aged 20−50 years who were on ART for at least 12 months and had undetectable levels of viral loads. Those who could not communicate in Mandarin, did not have stable heterosexual partners, or could not conceive for any reason were excluded. Stratified random sampling was used to select participants at a female to male ratio of 1:1. The study was approved by the Ethics Committee of Prince Songkhla University (REC-63-208-18-1) and the Research Ethics Review Committee of the Third People’s Hospital of Kunming (2020072001).
Sample Size Estimation
We determined the sample size using the Structural Equation Model Sample Size Calculator.Citation28,Citation29 In the process of data analysis, a variable with one observed variable was treated as a latent variable with a single observed variable. Therefore, there were 24 latent variables in the model including three with multiple observed variables (attitudes, subjective norms, and PBC), and 21 with a single observed variable (5 demographic factors, 7 behavioral beliefs, 4 normative beliefs, 4 control beliefs, and fertility intention). With 24 latent variables, 33 observed variables, an expected effect size of 0.3, type I error at 0.05, and the desired statistical power level of 0.8, the required sample sizes were 237 to detect an effect of one variable in the model on another and 576 to test the overall fit of the model to empirical data.
Instruments
The questionnaire collected demographic data and variables shown in . Codes and copy of the survey are in Supplemental Appendix Table 1–3.
Scales for Attitudes and Behavioral Beliefs: Questions on attitudes towards fertility intention (5 items or A1-A5 in ) measured subjective evaluation of having a/another child on a five-point Likert scale (1 = strongly disagree, 5 = strongly agree). Seven behavioral beliefs were each assessed with a question on expected outcomes of having a/another child and another on outcome evaluation (ie, the impact of the consequences). Both were rated on a five-point Likert scale (1 = not at all important, 5 = very important; 1 = not at all likely, and 5 = very likely, respectively). The product of expected outcomes and its corresponding outcome evaluation was a belief score (range from 1 to 25). Higher values implied that participants had more favorable beliefs about the particular outcomes of having a/another child.
Scales for Subjective Norms and Normative Beliefs: Questions on subjective norms contained three items (N1 to N3 in ) asking for the subjects’ perceptions of social pressure to have a/another child, for example, “Most of the people who influence me a lot hold an attitude towards fertility.” Each item was evaluated using a five-point scale (1 = strongly disagree, 5 = strongly agree). Higher scores reflected a greater perception that fertility was accepted as normal or desirable. Normative beliefs were assessed using four items of normative expectations of specific referent groups and four items of motivation to comply (with those groups) on a five-point Likert scale (1 = strongly disapprove, 5 = strongly approve and 1 = not at all important, 5 = very important, respectively). The score of each normative expectation was multiplied by its corresponding motivation to comply and became a normative belief score (ranging from 1–25). Higher scores reflected a greater perception of a particular significant other expecting participants to have a/another child.
Scales for PBC and Control Beliefs: Questions on PBC (4 items or P1 to P4 in ) measured the participants’ self-efficacy to have a/another child on a five-point Likert scale (1 = strongly disagree, 5 = strongly agree). Control beliefs were assessed by four items on participants’ beliefs on the presence of facilitating or impeding factors on having a/another child and the perceived power of these factors. Both were measured on five-point Likert scales (1 = not at all important, 5 = very important and 1 = very difficult, 5 = very easy, respectively). The score of each item on facilitating or impeding factors was multiplied by its corresponding power of control to give a weighted control belief score for a particular factor (ranging 1–25). Higher scores reflected the greater perceived presence of a particular control factor towards having a/another child.
Fertility Intention: Fertility intention was measured by a single item, “How likely am I going to have a/another child within the next three years?” on a five-point scale ranging from definitely not to definitely yes.
Socio-demographics: Five binary demographic variables were included in the model (ie, sex, age, registered residence, employment status, and household monthly income). The reference groups were being male, age >35, living in urban areas, being employed, and having a household income greater than 10,000 Chinese Yuan (CNY) per month.
Translation and Verification of the Instrument
The questionnaire was initially developed in English and independently translated into Chinese by two bilingual native Chinese speakers. A professional translator compared the two versions and corrected any discrepancies. The two translators, who were both native Chinese speakers, independently performed back translation of the Chinese version to the English version. The original and back-translated versions of the questionnaires were compared to guarantee accuracy and completeness. All translated versions were compared to the originals for semantic, idiomatic, experiential, and conceptual comparability, and the Chinese translation was finalized with consultation with an experienced team consisting of epidemiologists and doctors with extensive experience in HIV treatment and scale development in medical practice. The cognitive briefing was conducted on 35 respondents who completed the translated questionnaire and were interviewed about their thoughts on each item and the reasons behind their responses. The information was used to revise the questionnaire.
Data Collection
The principal researcher contacted the administrators of the ART clinics to obtain their consent for their clients to join this study. The researcher also asked eligible patients for their informed consent to join this study. They were informed that anonymity was assured to protect their privacy. All information that could identify the participants was kept confidential. The participants were interviewed face-to-face using a structured questionnaire. The interview took 15−30 minutes.
Statistical Analysis
Structural equation modeling (SEM) in the lavaan package of the R statistical software was used to analyze the data.Citation30,Citation31 Univariate skewness and kurtosis of all observed variables, except for binary demographic variables were within acceptable ranges (ie, less than 2 and 7, respectively).Citation32 The Robust Maximum Likelihood Estimation was used because the tested model included binary demographic variables.Citation33 We used a confirmatory factor analysis (CFA) to test the measurement model of the hypothesized model (). The fit indices in the study and their cut-off values were the Chi-squared test (p > 0.05), Comparative Fit Index (CFI > 0.90), Tucker-Lewis index (TLI > 0.90), Root Mean Square Error of Approximation (RMSEA < 0.07) and its 90% confident interval, and Standardized Root Mean Square Residual (SRMSR < 0.07).Citation34–Citation38 The measurement model was modified based on modification indices (MIs) and theoretical considerations to gain an acceptable fit.Citation39,Citation40 Subsequently, the hypothesized model according to was fitted using the same procedures as that in the measurement model. The level of significance in this study was set at a p-value <0.05.
Results
A total of 516 questionnaires were distributed. Twenty-nine questionnaires were excluded due to a large amount of incomplete data. The responses from 487 PLWH (93%) were used in the data analysis. Half of the participants were females (50.3%) with ages ranging from 20 to 50 years. Rural residents were represented by 62.8% of the participants. The percentage of unemployed participants was 63.7% while 57.1% reported a low monthly income (<10,000 CNY). Overall, 38.4% of the respondents answered that they were likely to have a/another child in the next three years.
Measurement Model
The measurement model of the hypothesized model showed an acceptable fit to the data based on CFI, RMSEA and SRMR (χ2 = 596.80, df = 240, p < 0.001; CFI = 0.948; TLI = 0.885; RMSEA = 0.059 (90% CI 0.053–0.065); SRMR = 0.031). However, TLI indicated a poor fit of the model. The model was modified by deleting two observed variables of PBC because of factor loading less than 0.50 and its redundant content. The modified model had an acceptable fit (χ2 = 271.96, df = 150, p < 0.001; CFI = 0.980; TLI = 0.941; RMSEA = 0.043 (90% CI 0.035–0.052); SRMR = 0.023). Model fit indices of this measurement model were summarized in Supplemental Appendix Table 4.
Cronbach’s alpha for multi-item variables (attitudes, subjective norm, and PBC) ranged from 0.62 to 0.80. Their composite reliabilities, based on the McDonald’s omega ranging from 0.87 to 0.88, were considered satisfactory (>0.7).Citation41 Standardized factor loadings in latent variables with multiple observed variables (attitudes, subjective norm, and PBC) were from 0.55 to 0.92 which implied convergent validity. The other variables in the model had one indicator, and their factor loadings were set to 1.0. The sizes of the factor correlations among attitudes, subjective norm, and PBC were low to moderate (range 0.39–0.42). Absolute values of the correlations among all variables in the model were between 0.010 and 0.59. The result implied divergent validity of the variables in the model.
The participants had favorable attitudes toward having a/another child (4.2 [0.68], range 1−5), and high perceived subjective norms for the behavior (4.3 [0.18] range 1−5). They perceived that it was easy to have a/another child if they intended to do so with a mean PBC of 4.2 [0.61] (out of 5).
Structural Model
The model in , following the deletion of three observed variables as mentioned in the previous section, showed an overall moderate fit to the data (χ2 = 609.49, df = 195, p < 0.001; CFI = 0.932; TLI = 0.849; RMSEA = 0.069 (90% CI 0.063–0.076); SRMR = 0.062). However, TLI was lower than 0.90 that indicated a poor fit of the model. Based on the size of the modification index and theoretical considerations, we added two paths: from perception on partner’s expectation to fertility intention and from perceived supportive effect of the two-child policy to fertility intention. The modified model showed an acceptable fit (χ2 = 417.01, df = 193, p < 0.001; CFI = 0.963; TLI = 0.917; RMSEA = 0.051 (90% CI 0.045–0.058); SRMR = 0.055). The fit parameters of structural model were summarized in Supplemental Appendix Table 4.
and Supplemental Appendix Table 5 and 6 show the modified model with significant path coefficients. The variables in the model explained 54.6, 32.4, 21.5, and 53.7% of the variance in attitudes towards having a/another child, relevant subjective norms, PBC, and fertility intention, respectively. Surprisingly, the three main concepts from the TPB (ie, attitudes towards having a/another child, relevant subjective norms, and PBC) showed no significant effects on fertility intention with the standardized coefficients (β) of 0.037, 0.080, and 0.048, respectively (p > 0.05). This implies that some important factors were not included in the model. Future studies should identify these factors to better understand the phenomena. In this study, attitudes, subjective norms, and PBC showed no direct effects on fertility intention, implying that they did not mediate the effects on other variables in the model. The strongest predictor of fertility intention among Chinese PLWH was a perception of a partner’s expectation (β = 0.442, p < 0.001), followed by perceived supportive effect of the two-child policy (β = 0.337, p < 0.001), and being younger (aged 20–35 years; β = 0.098, p < 0.003). The average score on fertility intention among the respondents aged 20–35 years (3.50 ± 1.09 out of the full score of 5) was higher than that of respondents aged >35 years (2.96 ± 1.22).
Figure 2 Psychological and socio-demographic characteristics predicting fertility intention among PLWH. ***p<0.01, **p<0.05; Squared multiple correlation, Red coefficients: Direct significant correlation between predictors and outcome.
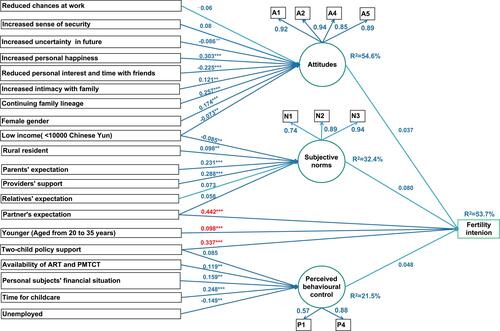
Attitudes towards having a/another child among Chinese PLWH showed significant positive relationships to perceived happiness and life satisfaction from having a/another child (β = 0.303, p < 0.001), desire to continue family lineage (β = 0.257, p < 0.001), being female (β = 0.174, p < 0.001), and belief in increased intimacy among family members (β = 0.125, p < 0.023). The mean of attitudes toward having a/another child among females (16.83 ± 2.87 out of the full score of 20) was higher than that of males (16.38 ± 2.60). Attitudes also had significant negative relationships with belief that having a/another child would jeopardize personal interest and time with friends (β = –0.225, p < 0.001), perception of increased uncertainty in life (β = –0.086, p < 0.016) and having the lower-income (β = –0.073, p < 0.039). The mean of attitudes among respondents with an income <10,000 CNY per month (16.4 ± 2.76 out of the full score of 20) was lower than that of respondents with an income >10,000 CNY per month (16.88 ± 2.71).
The strongest predictors of subjective norm on having a/another child was the expectation of health professionals (β = 0.288, p < 0.001), followed by the expectation of their parent (β = 0.231, p < 0.001), living in a rural area (β = 0.098, p < 0.025), and having the lower-income (β = –0.085, p < 0.043). Those living in rural residents reported a slightly higher level of subjective norms on having a/another child (12.84±1.71 out of the full score of 15) than those living in urban residents did (12.55 ± 1.73). The mean of subjective norms among those with less than 10,000 CNY per month (12.71 ± 1.73 out of the full score of 15) was lower than that of respondents with more than 10,000 CNY per month (13.00 ± 1.67).
PBC was influenced by four variables including time for taking care of a child (β = 0.248, p < 0.001), personal financial situation (β = 0.159, p < 0.013), being unemployed (β = –0.149, p < 0.005), and availability of HIV medications and prevention of mother-to-child HIV transmission (PMTCT) (β = 0.119, p < 0.015). The unemployed respondents reported a lower level of PBC on having a/another child (8.4 ± 1.19 out of the full score of 10) than the employed respondents did (8.61 ± 1.27).
Discussion
This study found that fertility intention among Chinese PLWH was significantly related to beliefs in the partner’s expectations, two-child policy, and being young (aged 20–35 years). The TPB-based constructs including attitudes, subjective norms, and PBC were not a significant predictor of fertility intention. This finding contradicted the findings of Laschinger et al,Citation42 the Dippel et al study on teenage pregnancy,Citation43 and the Amutah et al study on women living with HIV.Citation44 However, most female subjects in two of these studiesCitation45,Citation46 did not reveal their HIV status and hence their referents’ opinions about childbearing following HIV diagnosis could not be assessed.
Our findings suggested that the partner’s expectation was a good predictor of fertility intention. On the other hand, we found significant effects from the influences of parents and health providers on subjective norms but not on fertility intention. It was reported that family expectations are a predominant factor in having children.Citation47 However, in our PLWH sample, fertility intention was the couple’s matter that was not much influenced by social norms. Oosterhoff et alCitation48 found that, in Vietnam, parents influenced the intention of PLWH to have children, whereas the provider, partner, and other relatives did not. FeyissaCitation49 found that a provider’s support influenced fertility intention among PLWH in Western Ethiopia. Another study, however, indicated that despite a strong desire and intent to have a child, PLWH living in urban areas of Ontario, Canada were less likely to have fertility behavior due to a lack of family support.Citation50 A possible explanation for the mixed results is that the relevance of important referents might vary in different cultures.
Our findings suggested that the government’s two-child policy was associated with fertility intention. According to data from the Seventh National Census, China’s total fertility rate of reproductive-aged women in 2020 was 1.3,Citation51 which was significantly below the UN Population Division’s 2019 World Population Prospects estimate of 1.8.Citation52 Therefore, the Chinese government announced the implementation of a new three-child policy.Citation53 The belief in supportive effect of the policy on having another child showed the strongest influence on fertility intention among Chinese PLWH, compared to other factors. Since we did not have non-HIV couples in our study, whether this policy also had the same influence on the general population in the study community was not known.
Young age (≤35 years) was found to have a stronger fertility intention. This finding was consistent with that in previous studies in East Africa,Citation54 South Africa and Tanzania,Citation55 and RwandaCitation56 but not with Central BrazilCitation57 and Northwest Ethiopia.Citation58 The variation may be linked to the availability of ART among the younger age group.Citation1
Since this was a cross-sectional study, any interpretation on causality must be made with caution. Data were collected from Yunnan province, which is one of the poorest in China with diversity in ethnic groups. Generalization of the results to other PLWH in other areas must be done with caution.
Conclusions
The findings that fertility intention was strongly influenced by beliefs of partner’s expectation, support from the two-child policy, and younger age. These factors should be considered in future support of fertility intention in PLWH.
Institutional Review Board Statement
This study was approved by the Ethics Committee of Prince of Songkla University (REC-63-208-18-1) and the Research Ethics Review Committee of the Third People’s Hospital (2020072001). In this study, pseudonyms were used to protect the identity of the participants.
Data Sharing Statement
All pertinent information is contained inside the text and its accompanying information files.
Acknowledgments
This study is a part of the first author’s thesis in partial fulfillment of the requirements for a Ph.D. degree in Epidemiology at Prince of Songkla University, Songkhla, Thailand. We greatly appreciate the assistance from the staff members of the HIV treatment center who supported our study at the Third People’s Hospital in Kunming, China. The authors would like to express their gratitude to Dr. Wit Wichaidit for his assistance in developing the survey’s original questionnaire.
Disclosure
The authors declared no conflicts of interest.
Additional information
Funding
References
- Asfaw HM, Gashe FE. Fertility intentions among HIV positive women aged 18–49 years in Addis Ababa Ethiopia: a cross sectional study. Reprod Health. 2014;11(1):36. doi:10.1186/1742-4755-11-36
- Mekonnen H, Enquselassie F. Effect of antiretroviral therapy on changes in the fertility intentions of human immunodeficiency virus-positive women in Addis Ababa, Ethiopia: a prospective follow-up study. Epidemiol Health. 2017;39:e2017028. doi:10.4178/epih.e2017028
- Yan X, Du J, Ji G. Prevalence and factors associated with fertility desire among people living with HIV: a systematic review and meta-analysis. PLoS One. 2021;16(3):e0248872. doi:10.1371/journal.pone.0248872.
- Morris JL, Rushwan H. Adolescent sexual and reproductive health: the global challenges. Int J Gynaecol Obstet. 2015;131 Suppl 1:S40–42. doi:10.1016/j.ijgo.2015.02.006
- Comins CA, Rucinski KB, Baral S, Abebe SA, Mulu A, Schwartz SR. Vulnerability profiles and prevalence of HIV and other sexually transmitted infections among adolescent girls and young women in Ethiopia: a latent class analysis. PLoS One. 2020;15(5):e0232598. doi:10.1371/journal.pone.0232598
- Knippler ET, Mwamba RN, Coleman JN, et al. Attitudes toward pregnancy among women enrolled in prevention of mother-to-child transmission of HIV (PMTCT) Services in Moshi, Tanzania. AIDS Behav. 2021;25(12):4008–4017. doi:10.1007/s10461-021-03339-0
- Milford C, Beksinska M, Greener R, et al. Fertility desires of people living with HIV: does the implementation of a sexual and reproductive health and HIV integration model change healthcare providers’ attitudes and clients’ desires? BMC Health Serv Res. 2021;21(1):509. doi:10.1186/s12913-021-06487-0
- Iliyasu Z, Galadanci HS, Ibrahim YA, et al. Should they also have babies? Community attitudes toward sexual and reproductive rights of people living with HIV/AIDS in Nigeria. Ann Glob Health. 2017;83(2):320–327. doi:10.1016/j.aogh.2017.05.001
- Bankole A, Biddlecom AE, Dzekedzeke K. Women’s and men’s fertility preferences and contraceptive behaviors by HIV status in 10 sub-Saharan African countries. AIDS Educ Prev. 2011;23(4):313–328. doi:10.1521/aeap.2011.23.4.313
- Burgess A, Purssell E. What is the relationship between increased access to HAART, relationship status and fertility decisions amongst HIV-positive women? A literature review and meta-analysis. J Clin Nurs. 2017;26(23–24):3800–3810. doi:10.1111/jocn.13731
- Heard I, Sitta R, Lert F, et al. Reproductive choice in men and women living with HIV: evidence from a large representative sample of outpatients attending French hospitals (ANRS-EN12-VESPA Study). AIDS. 2007;21(Suppl 1):S77–S82. doi:10.1097/01.aids.0000255089.44297.6f
- O’shea MS, Rosenberg NE, Hosseinipour MC, et al. Effect of HIV status on fertility desire and knowledge of long-acting reversible contraception of postpartum Malawian women. AIDS Care. 2015;27(4):489–498. doi:10.1080/09540121.2014.972323
- Brahmbhatt H, Santelli J, Kaagayi J, Lutalo T, Serwadda D, Makumbi F. Pregnancy incidence and fertility desires among couples by HIV status in Rakai, Uganda. J Acquir Immune Defic Syndr. 2019;80(5):494–502. doi:10.1097/QAI.0000000000001951
- Yeatman SE. The impact of HIV status and perceived status on fertility desires in Rural Malawi. AIDS Behav. 2009;13(1):12–19. doi:10.1007/s10461-009-9534-1.
- Bandehelahi K, Khoshravesh S, Barati M, Tapak L. Psychological and sociodemographic predictors of fertility intention among childbearing-aged women in Hamadan, West of Iran: an application of the BASNEF model. Korean J Fam Med. 2019;40(3):182–187. doi:10.4082/kjfm.18.0008
- Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health. 2011;26(9):1113–1127. doi:10.1080/08870446.2011.613995
- Götmark F, Andersson M. Human fertility in relation to education, economy, religion, contraception, and family planning programs. BMC Public Health. 2020;20(1):265. doi:10.1186/s12889-020-8331-7
- Sallam H, Sallam N. Religious aspects of assisted reproduction. Facts Views Vis Obgyn. 2016;8(1):33–48.
- Tran BX, Duong HD, Nguyen AQ, Pham LD. Child desire among men and women living with HIV/AIDS in the traditional culture of Vietnam. AIDS Behav. 2018;22(9):2888–2894. doi:10.1007/s10461-018-2029-1
- Ko NY, Muecke M. Reproductive decision-making among HIV-positive couples in Taiwan. J Nurs Scholarsh. 2005;37(1):41–47. doi:10.1111/j.1547-5069.2005.00008.x
- Kaljee L, Zhang L, Li X, et al. Factors influencing fertility desire among people living with HIV in Guangxi, China; 2014.
- Ajzen I. From intentions to actions: a theory of planned behavior. Kuhl J, Beckmann J, editors. Action Control: From Cognition to Behavior. Berlin, Heidelberg:Springer; 1985:11–39. SSSP Springer Series in Social Psychology. doi: 10.1007/978-3-642-69746-3_2
- Aizen I, Klobas J. Fertility intentions: an approach based on the theory of planned behavior. DemRes. 2013;29:203–232. doi:10.4054/DemRes.2013.29.8
- Ajzen I, Kruglanski AW. Reasoned action in the service of goal pursuit. Psychol Rev. 2019;126(5):774–786. doi:10.1037/rev0000155
- Hashemzadeh M, Shariati M, Mohammad Nazari A, Keramat A. Childbearing intention and its associated factors: a systematic review. Nurs Open. 2021;8(5):2354–2368. doi:10.1002/nop2.849
- Ewemooje OS, Biney E, Amoateng AY. Determinants of fertility intentions among women of reproductive age in South Africa: evidence from the 2016 demographic and health survey. J Popul Res. 2020;37(3):265–289. doi:10.1007/s12546-020-09246-w
- Nattabi B, Li J, Thompson SC, Orach CG, Earnest J. A systematic review of factors influencing fertility desires and intentions among people living with HIV/AIDS: implications for policy and service delivery. AIDS Behav. 2009;13(5):949–968. doi:10.1007/s10461-009-9537-y
- A-priori sample size for structural equation models references - free statistics calculators [Internet]. [ cited December 24, 2021]. Available from: https://www.danielsoper.com/statcalc/references.aspx?id=89. Accessed May 16, 2022.
- Christopher Westland J. Lower bounds on sample size in structural equation modeling. Electron Commer Res Appl. 2010;9(6):476–487. doi:10.1016/j.elerap.2010.07.003
- Rosseel Y. lavaan: an R package for structural equation modeling. J Stat Softw. 2012;48:1–36. doi:10.18637/jss.v048.i02
- R: the R project for statistical computing [Internet]; [ cited January 28, 2022]. Available from: https://www.r-project.org/. Accessed May 16, 2022.
- Finney S, DiStefano C. Nonnormal and categorical data in structural equation models. Struct Equ Modeling. 2013;10:439–492.
- Miranda A, Rabe-Hesketh S. Maximum likelihood estimation of endogenous switching and sample selection models for binary, ordinal, and count variables. Stata J. 2006;6(3):285–308. doi:10.1177/1536867X0600600301
- Hooper D, Coughlan J, Mullen M. Structural equation modelling: guidelines for determining model fit; January 1, 2008. Available from: https://arrow.tudublin.ie/buschmanart/2. Accessed May 16, 2022.
- Angeles L. Evaluating cutoff criteria of model fit indices for latent variable models with binary and continuous outcomes. undefined; 2002 [ cited December 12, 2021]. Available from: https://www.semanticscholar.org/paper/Evaluating-Cutoff-Criteria-of-Model-Fit-Indices-for-Angeles/7a22ae22553f78582fc61c6cab4567d36998293b. Accessed May 16, 2022.
- Brown T. Confirmatory factor analysis for applied research; 2006.
- Funder DC, Ozer DJ. Evaluating effect size in psychological research: sense and nonsense. Adv Meth Pract Psychol Sci. 2019;2(2):156–168. doi:10.1177/2515245919847202
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
- Steiger JH. Structural model evaluation and modification: an interval estimation approach. Multivariate Behav Res. 1990;25(2):173–180. doi:10.1207/s15327906mbr2502_4
- Whittaker TA. Using the modification index and standardized expected parameter change for model modification. Int J Exp Educ. 2012;80(1):26–44. doi:10.1080/00220973.2010.531299
- Ventura-León JL, Caycho-Rodríguez T. El coeficiente Omega: un método alternativo para la estimación de la confiabilidad. Rev Latinoam Cienc Soc Ninez Juv. 2017;15(1):625–627. Danish.
- Laschinger HK, Goldenberg D. Attitudes of practicing nurses as predictors of intended care behavior with persons who are HIV positive: testing the Ajzen-Fishbein theory of reasoned action. Res Nurs Health. 1993;16(6):441–450. doi:10.1002/nur.4770160608
- Dippel EA, Hanson JD, McMahon TR, Griese ER, Kenyon DB. Applying the Theory of Reasoned Action to Understanding Teen Pregnancy with American Indian Communities. Matern Child Health J. 2017 Jul;21(7):1449–56. doi:10.1007/s10995-017-2262-7
- Amutah NN, Gifuni J, Wesley Y. Shaping the Conversation: A Secondary Analysis of Reproductive Decision-Making among Black Mothers with HIV: Supplementary Issue: Health Disparities in Women. Clinical Medicine Insights: Women’s Health. 2016 Jan;9s1:CMWH.S34671. doi:10.4137/CMWH.S34671
- Wesley Y, Smeltzer SC, Redeker NS, Walker S, Palumbo P, Whipple B. Reproductive decision making in mothers with HIV-1. Health Care Women Int. 2000;21(4):291–304. doi:10.1080/073993300245159
- Leyva-Moral JM, Palmieri PA, Feijoo-Cid M, et al. Reproductive decision-making in women living with human immunodeficiency virus: a systematic review. Int J Nurs Stud. 2018;77:207–221. doi:10.1016/j.ijnurstu.2017.10.012
- Schwank SE, Gu C, Cao Z, et al. China’s child policy shift and its impact on Shanghai and Hangzhou women’s decision-making. IJWH. 2018;10:639–648. doi:10.2147/IJWH.S172804
- Oosterhoff P, Anh NT, Hanh NT, Yen PN, Wright P, Hardon A. Holding the line: family responses to pregnancy and the desire for a child in the context of HIV in Vietnam. Cult Health Sex. 2008;10(4):403–416. doi:10.1080/13691050801915192
- Feyissa TR, Harris ML, Loxton D. Discussing reproductive plans with healthcare providers by sexually active women living with HIV in Western Ethiopia. AIDS Behav. 2020;24(10):2842–2855. doi:10.1007/s10461-020-02833-1
- Wagner AC, Ivanova EL, Hart TA, Loutfy MR. Examining the Traits-Desires-Intentions-Behavior (TDIB) model for fertility planning in women living with HIV in Ontario, Canada. AIDS Patient Care STDS. 2014;28(11):594–601. doi:10.1089/apc.2014.0075
- Times G. China’s fertility rate may become ‘world’s lowest’ without strong intervention policy, India may overtake China by 2023: demographers - Global Times [Internet] [cited 2022 May 17]. Available from: https://www.globaltimes.cn/page/202105/1223141.shtml
- United Nations, Department of Economic and Social Affairs, Population Division. World population prospects Highlights, 2019 revision Highlights, 2019 revision; 2019.
- China’s National Bureau of Statistics (NBS). China’s 2020 Fertility and Adoption of a Three-Child Policy. Population and Development Review. 2021;47(3):877–9. doi:10.1111/padr.12434
- Mujugira A, Heffron R, Celum C, Mugo N, Nakku-Joloba E, Baeten JM. Fertility intentions and interest in early antiretroviral therapy among East African HIV-1 infected individuals in serodiscordant partnerships. J Acquir Immune Defic Syndr. 2013;63(1):e33–5. doi:10.1097/QAI.0b013e318288bb32
- Rispel LC, Metcalf CA, Moody K, Cloete A, Caswell G. Sexual relations and childbearing decisions of HIV-discordant couples: an exploratory study in South Africa and Tanzania. Reprod Health Matters. 2011;19(37):184–193. doi:10.1016/S0968-8080(11)37552-0
- Niragire F, Ndikumana C, Nyirahabimana MG, Uwizeye D. Prevalence and factors associated with fertility desire among HIV-positive women in Rwanda in the context of improved life expectancy. Arch Public Health. 2021;79(1):209. doi:10.1186/s13690-021-00742-w
- Ramos de Souza M, Do Amaral WN, Alves Guimarães R, Rezza G, Brunini SM. Reproductive desire among women living with HIV/AIDS in Central Brazil: prevalence and associated factors. PLoS One. 2017;12(10). doi: 10.1371/journal.pone.0186267
- Mekonnen B, Minyihun A. Fertility desire and associated factors among HIV positive women attending ART clinics in Amhara Region referral hospitals in Northwest Ethiopia, 2017. HIV AIDS. 2019;11:247–254. doi:10.2147/HIV.S221941